
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 45(2); 2020 > Article
- Research Article A micro-computed tomographic evaluation of root canal filling with a single gutta-percha cone and calcium silicate sealer
-
Jong Cheon Kim1
 , Maung Maung Kyaw Moe2, Sung Kyo Kim1
, Maung Maung Kyaw Moe2, Sung Kyo Kim1 -
Restor Dent Endod 2020;45(2):e18.
DOI: https://doi.org/10.5395/rde.2020.45.e18
Published online: February 12, 2020
1Department of Conservative Dentistry, School of Dentistry, Kyungpook National University, Daegu, Korea.
2Department of Conservative Dentistry, University of Dental Medicine, Mandalay, Myanmar.
- Correspondence to Sung Kyo Kim, DDS, MSD, PhD. Professor, Department of Conservative Dentistry, School of Dentistry, Kyungpook National University, 2177 Dalgubeol-daero, Jung-gu, Daegu 41940, Korea. skykim@knu.ac.kr
• Received: September 25, 2019 • Revised: December 15, 2019 • Accepted: December 19, 2019
Copyright © 2020. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,215 Views
- 27 Download
- 11 Crossref
Abstract
-
Objectives The purpose of this study was to evaluate the void of root canal filling over time when a calcium silicate sealer was used in the single gutta-percha cone technique.
-
Materials and Methods Twenty-four J-shaped simulated root canals and twenty-four palatal root canals from extracted human maxillary molars were instrumented with ProFile Ni-Ti rotary instruments up to size 35/0.06 or size 40/0.06, respectively. Half of the canals were filled with Endoseal MTA and the other half were with AH Plus Jet using the single gutta-percha cone technique. Immediately after and 4 weeks after the root canal filling, the samples were scanned using micro-computed tomography at a resolution of 12.8 μm. The scanned images were reconstructed using the NRecon software and the void percentages were calculated using the CTan software, and statistically analyzed by 1-way analysis of variance, paired t-test and Tukey post hoc test.
-
Results After 4 weeks, there were no significant changes in the void percentages at all levels in both material groups (p > 0.05), except at the apical level of the AH Plus Jet group (p < 0.05) in the simulated root canal showing more void percentage compared to other groups. Immediately after filling the extracted human root canals, the Endoseal MTA group showed significantly less void percentage compared to the AH Plus Jet group (p < 0.05).
-
Conclusions Under the limitations of this study, the Endoseal MTA does not seem to reduce the voids over time.
INTRODUCTION
Canal obturation reduces coronal leakage, bacterial contamination, and seals the apex from periapical tissue fluids and entombs the remaining irritants in the canal [1]. However, the available materials and techniques using for obturation cannot create an impervious seal in the canal system and may result in a leak to some extent [2].
Materials for conventional root canal fillings, which are composed of core material, usually gutta-percha, and a sealer, have some limitations. First, gutta-percha acts only as a filler and does not seal the canal. Furthermore, it shrinks when cooled after being heated [3]. Second, traditional sealers generally shrink on the setting and can be washed out in the presence of tissue fluids [4]. Third, since the sealers do not bond to gutta-percha, shrinkage of the gutta-percha and the sealer results in a gap, which may lead to micro-leakages [5]. In order to minimize the shortcomings of the sealer, it should be as thin as possible, which can be difficult because most canals are not simple and round [6].
Recently, calcium silicate sealers including mineral trioxide aggregate (MTA) sealers have been introduced, and they have some advantages. MTA is hydrophilic and can use the natural moisture in the root canal, has a high pH, which can be advantageous in managing inflammation, does not shrink but expands slightly, which can aid in making a tight seal and is insoluble in tissue fluids [6].
In a systematic review, calcium silicate sealer was reported to have similar physicochemical properties compared to other conventional sealers, better biological properties, and a bioactive potential [7]. Endoseal MTA (Maruchi, Wonju, Korea) is one of the recently introduced calcium silicate sealers. A study reported that Endoseal MTA expands significantly compared to other sealers [8]. Even though the slight expansion may contribute to a tight seal, excessive expansion may trigger a crack in the root dentin. Endoseal MTA was recommended for use with the single gutta-percha cone technique since it maximizes convenience, is considered to be less technique-sensitive and may exert less damage to the root canal wall [9].
To evaluate the filling quality, including the tightness of the seal, conventional leakage studies were performed, which have the shortcomings of being time-consuming, hard to standardize, non-reproducible, and an inability to simulate clinical conditions. For a more accurate and 3-dimensional (3D) evaluation, micro-computed tomography (micro-CT) technology with its non-destructive and objective characteristics has been applied [10]. Micro-CT presents the area concentration including empty space in an object. The voids in a canal filling may weaken the filling quality, serve as a hub for microbes, and make tunnels and transport contaminants along the canal [11].
Although the calcium silicate sealers have been reported to have good biological properties, they are used to attain a fluid-proof seal [12], since they are known to expand when setting [6,8,12,13]. However, more studies are needed on the amount of sealer expansion in the root canal and its relationship with the change in void volume percentage. Therefore, the purpose of this study was to evaluate the quality of the root canal filling over time when a calcium silicate sealer was used in the single gutta-percha cone technique. The null hypothesis was that there would be no difference in the void percentage of the canal filling over time when the root canal was filled with the single gutta-percha cone technique with a calcium silicate-based sealer.
MATERIALS AND METHODS
This study protocol was approved by the Institutional Review Board (IRB) of Kyungpook National University Dental Hospital (IRB No. KNUDH-2019-11-05-00). Twenty-four simulated root canals in clear resin blocks and twenty-four root canals in extracted human teeth were used for this study.
Simulated root canals in the resin blocks of SCS-SP181 (SCS, Foshan, China) have a J-shaped curve and with a mean canal length of 18.0 mm. The palatal roots of the extracted human maxillary first molars were found to have a root curvature of 10˚–20˚ by the Schneider method and an apical canal size comparable to the 20–40 hand K file, without any canal obstruction or any previous history of root canal treatment. The palatal roots were cut at the level of 11.0 mm from the apex with a high-speed diamond bur.
The working length was determined at 0.5 mm from the file length that was seen from the apical foramen. The root canals were enlarged up to size 35/0.06 in the resin blocks and up to size 40/0.06 in the extracted human teeth with ProFile Ni-Ti rotary files (Dentsply Maillefer, Ballaigues, Switzerland) by using VDW silver endo engine (VDW, Munich, Germany) under copious irrigation with 2.5% sodium hypochlorite.
The twenty-four simulated root canals and twenty-four root canals of extracted human teeth were randomly distributed into 2 groups of control and experimental. The control group used a resin sealer and the experimental group used a calcium silicate sealer.
After canal preparation, a size 35/0.06 gutta-percha cone (Diadent, Cheongju, Korea) was fitted in the canal and confirmed by eye in the simulated root canals and a size 40/0.06 gutta-percha cone was fitted in the root canals of the extracted human teeth and confirmed by digital radiographs (Vatech, Hwasung, Korea).
After irrigation with saline and drying with paper points (Diadent), the root canals were filled with a single gutta-percha cone technique. A resin sealer, AH Plus Jet (Dentsply DeTrey, Konstanz, Germany), was used in the control group and a calcium silicate sealer, Endoseal MTA was used in the experimental group. The excess material above the canal orifice was passively cut with a GP cone cutter (A Blade, Azdent, Clujnapoca, Romania).
After cleaning, the access cavity was filled with composite resin for coronal sealing. The access cavities in the resin block specimens were treated with a resin adhesive, Adper Single Bond 2 (3M ESPE, Saint Paul, MN, USA) and filled with a flowable resin (Filtek Z350, 3M ESPE) followed by an acrylic adhesive coating. In the extracted teeth specimens, the access cavities were treated with a resin adhesive, Clearfil SE Bond 2 (Kuraray, Okayama, Japan), and filled with a flowable resin in the same way as the resin block.
The specimens were scanned immediately after the root canal filling and 4 weeks later using a micro-CT scanner, Skyscan 1272 (Bruker, Kontich, Belgium) at a resolution of 12.8 μm, the source voltage of 80 kV, source current of 125 μA, and filter of Al 1 mm. After the first micro-CT scan, the samples were immersed in a tube that contained 5 mL of phosphate buffer saline (PBS) and stored in a 37˚C water-bath for 4 weeks for the second scan [13].
The raw-images were reconstructed by using the NRecon ver. 1.7.3.0 (Bruker) software. The reconstructed images showed a cross-sectional view of each sample and were analyzed by CTan ver. 1.14.4.1 (Bruker). The volume of interest (VOI) was selected from the upper plane of minor constriction to 9 mm above of apical plane. A round region of interest (ROI) was set to exclude dentin and artifacts. The ROI was automatically stacked to make VOI. To make each file lighter and the image processing faster, this VOI was saved with a new dataset and reloaded for custom processing.
The thresholding process was performed to make image binarization of black and white to get a filling material image. The threshold level for the filling material in the simulated canals was 100–255, while for the filling material in the extracted teeth was 140–255. After imaging the filling material, it was copied to the ROI by the bitwise operation. The morphological operation processing, including closing, ROI, 2D space, round, radius 100, was carried out to set the ROI to a round canal shape.
The 3D analysis that includes porosity of additional value was performed to obtain the void percentage. VOIs of the coronal/middle/apical levels were obtained by dividing the long axis into 3 mm spans. The void percentage of each portion was calculated in the same way [14].
To statistically compare the void percentage of each level in the simulated root canal or the human root canal, 1-way analysis of variance (ANOVA) and paired t-test were used under 95% significance and Tukey was used as post hoc (SPSS, SPSS Inc., Chicago, IL, USA).
RESULTS
Distribution of the void percentage in the simulated root canals is shown in Table 1 and the human root canal is shown in Table 2.
Table 1
Void percentage after root canal filling in the simulated root canals
Data are presented as mean ± standard deviation. Statistical analysis was performed by 1-way ANOVA (p < 0.05) with the Tukey post hoc test. Different letters mean statistical differences in the same row. Four weeks later, there is a significant increase at the apical third of AH Plus Jet in comparison to immediately after the filling.
Table 2
Void percentage after root canal filling in the extracted teeth
Data are presented as mean ± standard deviation. Statistical analysis was performed by 1-way ANOVA (p < 0.05) with the Tukey post hoc test. Different letters mean statistical differences in the same row. Four weeks later, there is no significant difference in comparison to immediately after the filling.
Micro-CT scans taken immediately after the canal filling showed no significant differences in the void percentage at all levels between the Endoseal MTA and the AH Plus Jet groups in the simulated root canals (p > 0.05). The void percentage was not significantly changed after 4 weeks at all levels of both material groups (p > 0.05; Figure 1 and Table 1), except at the apical level of the AH Plus Jet group (p < 0.05) in the simulated root canals.
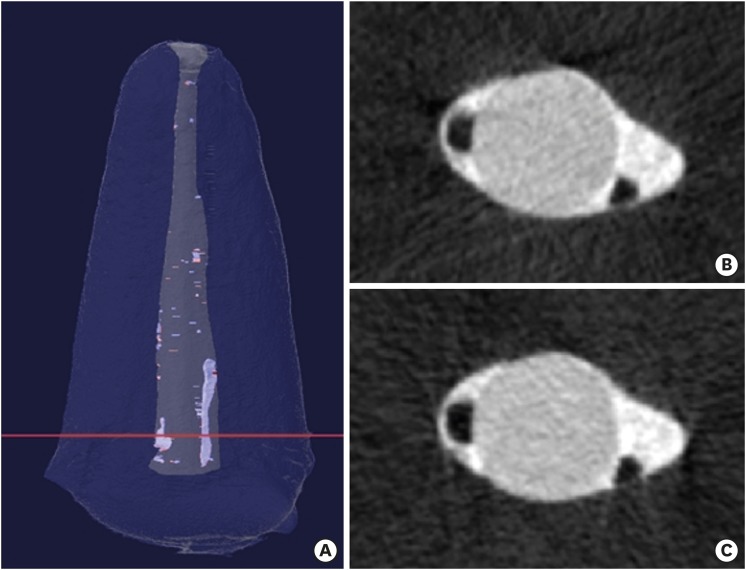
Figure 1

A sample of simulated root canal filled with Endoseal MTA sealer and single gutta-percha cone (A). Scanned images at the red line level of the left sample immediately after (B) and 4 weeks after (C) canal filling. Void of the first scan (B) is seen as blue, and void of the second scan (C) is seen as red in the left 3-dimensional modeling image.
Micro-CT scans taken immediately after the canal filling showed no significant differences in the void percentage at all levels between the Endoseal MTA and the AH Plus Jet groups in the extracted human root canals (p > 0.05; Table 2), except at the coronal level in which the Endoseal MTA group showed significantly less void percentage than in the AH Plus Jet group (p < 0.05). However, after 4 weeks, the void percentage was not significantly changed at all levels of both material groups (p > 0.05; Figure 2 and Table 2) in the extracted human root canals.
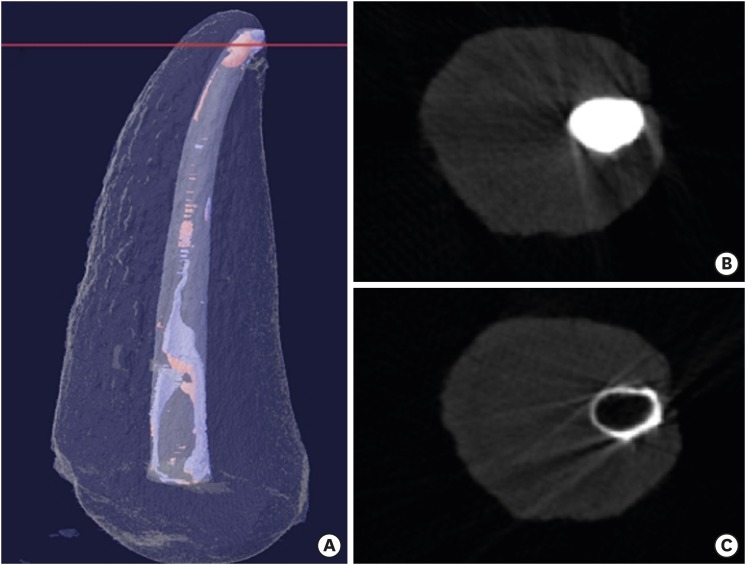
Figure 2
A sample of extracted human root canal filled with Endoseal MTA sealer and a single gutta-percha cone (A). Scanned images at the red line level of the left sample immediately after (B) and 4 weeks after (C) canal filling. Void of the first scan (B) is seen as blue, and void of the second scan (C) is seen as red in the left 3-dimensional modeling image.
DISCUSSION
The results of this study support the null hypothesis due to the insignificant differences in the void percentage immediately after canal filling in comparison with 4 weeks later. In this study, Endoseal MTA showed no significant changes in the void percentage. However, AH Plus Jet showed a slight increase of void percentage in the simulated root canal over time. Analysis of the void percentage distribution in each area indicated that the main cause of this change was the significant increase in the void percentage in the apical area of the AH Plus Jet sealer. One of the factors for this increase may be the solubility of the sealer. Since the canal-filled apex was immersed in PBS solution after 30 minutes of canal filling, the uncured resin sealer could be dissolved [13] (Figure 3). The probable cause for the void percentage changes in the AH Plus Jet group seemed to mainly be the sealer dissolution and not sealer expansion or shrinkage. These are the limitations of this study and more studies on the methodology will be needed to simulate clinical conditions.
Figure 3
A sample of extracted human root canal filled with AH Plus Jet sealer and single gutta-percha cone. (A). Scanned images at the red line level of the left sample immediately after (B) and 4 weeks after (C) canal filling. Void of the first scan (B) is seen as blue, and void of the second scan (C) is seen as red in the left 3-dimensional modeling image. The increase of void at apical area and loss of sealer can be seen at the right image a second scan (C). It is also seen at the red lines on the upper side of this image (shadow projection).
In addition to the significant void increases in the apical area of the simulated root canal, a void increasing tendency in the coronal area of extracted teeth canal was also observed in the AH plus Jet group in the present study. This is assumed to be caused by artifacts. Since the sealers are radio-opaque, some artifacts appeared in the coronal and apical areas, which were filled with a larger amount of sealer. Furthermore, AH Plus Jet is more radiopaque than Endoseal MTA [8,12]. The artifacts were more prominent in the second scan of the AH Plus Jet sealer group, in which large amounts of voids were calculated. More studies are needed to understand why some artifacts are more prominent in certain scans.
Among similar studies to the present study, one study reported a significant dimensional increase of the extruded calcium silicate sealer, MTA Fillapex (Angelus, Londrina, PR, Brazil), filled with the single gutta-percha cone technique after storage in PBS solution for 7 days [13]. In another study, a calcium silicate sealer, MTA Flow (University of Bologna, Bologna, Italy) filled with Thermafil (Dentsply Maillefer) was stored in Hank's Balanced Salt Solution for 6 months, and there was a trend of void percentage decrease over time with no significance [15].
According to a previous study, Endoseal MTA showed an expansion of more than 2% up to 3 weeks [8]. In another study, Endoseal MTA showed a 0.21% expansion 30 days later [12]. Although the present study did not examine the amount of expansion, some samples showed that the extruded sealer had developed cracks over time, which is thought to be related to the expansion of Endoseal MTA. However, in the present study, neither the expansion of Endoseal MTA nor the reduction in the percentage of voids could be confirmed over 4 weeks.
Nowadays, sealing ability tests are focused on visual assessment instead of the conventional leakage test. Visual assessment tests can be classified as micro-CT or microscope study. Micro-CT shows the whole canal system 3-dimensionally, but the resolution may not be sufficient to detect small voids because the filling materials are too radio-opaque. Although the microscope is more sensitive, it shows only part of the canal system and a loss of material can occur during sectioning [9]. It is hard to evaluate the sealing ability in an objective and reproducible manner with a microscope. The micro-CT method is increasingly being used, but there is no clearly defined and comprehensive analysis protocol [11].
In micro-CT studies, the materials are distinguished using threshold [9,10,11,16], and the threshold settings can be subjective. In addition, it is difficult to differentiate the canal wall from the filling material. However, it was relatively easy to distinguish the filling material alone in the present study. To overcome these difficulties, in previous studies, another micro-CT scan was taken before canal filling [11,12] or a manual ROI setting was taken on each section plane [9]. The first method is time-consuming and expensive, while the second method can be subjective and inaccurate. In order to obtain an objective and reproducible process, the present study established an ROI slightly greater than the filling material and used the images of the filling material to create a round canal shape using the morphological operation of CTan. This operation may not create an image that exactly matches the true canal shape in non-circular canals [14]. However, it could be applied to examine the differences between the first and the second scanned images of the same sample. It may have some advantages of being easier and reproducible.
A previous void percentage study using micro-CT reported that the void volume percentage of the single-cone technique was similar to that of the continuous wave of condensation technique, except for in the coronal portion of the canal [16]. This exception is probably because the single-cone technique is not suitable for the large coronal area. Previous reports indicate that the void percentages of the apical area were variable [10,11,15,16]. These void percentage variations of the filled root canals are thought to be due to the anatomical differences rather than the materials or technology [10].
Due to the large deviations in the results from the root canals of extracted human teeth in this study, it was difficult to verify the statistical significance. The average and deviation in the void percentages of the simulated root canals in the resin blocks were much less compared to those of human root canals. However, the changes in the void percentage were not much different in the simulated root canals or the human root canals.
In the extracted human root canals, the micro-CT scan taken immediately after canal filling showed significant differences in the void percentage at the coronal level, in which the Endoseal MTA group showed significantly less void percentage than the AH Plus Jet group. This difference also seemed to be due to the anatomical deviations rather than the materials. The micro-CT scan taken immediately after canal filling showed no significant difference in the simulated root canal. It could also be seen that the coronal area of the extracted human root canals had a large deviation in size.
CONCLUSIONS
Under the limitations of this study, it can be concluded that Endoseal MTA does not seem to reduce the voids over time when it was used with a single gutta-percha cone technique. Further studies are required to investigate the expansion of Endoseal MTA and the quality of canal filling over a longer time compared to other types of sealers.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Kim SK.
Data curation: Kim JC, Kim SK.
Formal analysis: Kim JC, Kim SK.
Funding acquisition: Kim JC.
Investigation: Kim JC.
Methodology: Kim JC, Moe MMK.
Project administration: Kim SK.
Resources: Kim JC.
Software: Moe MMK.
Supervision: Kim SK.
Validation: Kim SK.
Visualization: Kim JC.
Writing - original draft: Kim JC.
Writing - review & editing: Kim SK, Moe MMK.
- 1. Whitworth J. Methods of filling root canals: principles and practices. Endod Topics 2005;12:2-24.Article
- 2. Yanpiset K, Banomyong D, Chotvorrarak K, Srisatjaluk RL. Bacterial leakage and micro-computed tomography evaluation in round-shaped canals obturated with bioceramic cone and sealer using matched single cone technique. Restor Dent Endod 2018;43:e30.ArticlePubMedPMCPDF
- 3. Tsukada G, Tanaka T, Torii M, Inoue K. Shear modulus and thermal properties of gutta percha for root canal filling. J Oral Rehabil 2004;31:1139-1144.ArticlePubMed
- 4. Ørstavik D, Nordahl I, Tibballs JE. Dimensional change following setting of root canal sealer materials. Dent Mater 2001;17:512-519.ArticlePubMed
- 5. Ørstavik D. Endodontic filling materials. Endod Topics 2014;31:53-67.Article
- 6. Trope M, Bunes A, Debelian G. Root filling materials and techniques: bioceramics a new hope? Endod Topics 2015;32:86-96.Article
- 7. Silva Almeida LH, Moraes RR, Morgental RD, Pappen FG. Are premixed calcium silicate-based endodontic sealers comparable to conventional materials? A systematic review of in vitro studies. J Endod 2017;43:527-535.ArticlePubMed
- 8. Lim ES, Park YB, Kwon YS, Shon WJ, Lee KW, Min KS. Physical properties and biocompatibility of an injectable calcium-silicate-based root canal sealer: in vitro and in vivo study. BMC Oral Health 2015;15:129.ArticlePubMedPMCPDF
- 9. Kim JA, Hwang YC, Rosa V, Yu MK, Lee KW, Min KS. Root canal filling quality of a premixed calcium silicate endodontic sealer applied using gutta-percha cone-mediated ultrasonic activation. J Endod 2018;44:133-138.ArticlePubMed
- 10. Celikten B, Uzuntas CF, Orhan AI, Orhan K, Tufenkci P, Kursun S, Demiralp KÖ. Evaluation of root canal sealer filling quality using a single-cone technique in oval shaped canals: an in vitro micro-CT study. Scanning 2016;38:133-140.ArticlePubMedPDF
- 11. Moinzadeh AT, Zerbst W, Boutsioukis C, Shemesh H, Zaslansky P. Porosity distribution in root canals filled with gutta percha and calcium silicate cement. Dent Mater 2015;31:1100-1108.ArticlePubMed
- 12. Lee JK, Kwak SW, Ha JH, Lee W, Kim HC. Physicochemical properties of epoxy resin-based and bioceramic-based root canal sealers. Bioinorg Chem Appl 2017;2017:2582849.ArticlePubMedPMCPDF
- 13. Silva EJ, Perez R, Valentim RM, Belladonna FG, De-Deus GA, Lima IC, Neves AA. Dissolution, dislocation and dimensional changes of endodontic sealers after a solubility challenge: a micro-CT approach. Int Endod J 2017;50:407-414.PubMed
- 14. Salmon P. Bruker MicroCT Tutorial [Internet]. c2013;updated 2013 Apr 19]. cited 2018 Sep 10]. Available from: https://www.youtube.com/watch?v=wpWo55LBsNk.
- 15. Gandolfi MG, Parrilli AP, Fini M, Prati C, Dummer PM. 3D micro-CT analysis of the interface voids associated with Thermafil root fillings used with AH Plus or a flowable MTA sealer. Int Endod J 2013;46:253-263.PubMed
- 16. Iglecias EF, Freire LG, de Miranda Candeiro GT, Dos Santos M, Antoniazzi JH, Gavini G. Presence of voids after continuous wave of condensation and single-cone obturation in mandibular molars: a micro-computed tomography analysis. J Endod 2017;43:638-642.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Comparative analysis between resin-based root canal sealer and recent bioceramic-based root canal sealers using MicroCT, film thickness, and solubility
Amira Galal Ismail, Manar M. Galal, Tamer M. Hamdy
Journal of Oral Biology and Craniofacial Research.2026; 16(2): 101400. CrossRef - Evaluation of various obturation techniques with bioceramic sealers in 3D-printed C-shaped canals
Maryam Gharechahi, Melika Hoseinzadeh, Saeed Moradi, Mina Mehrjouei
BMC Oral Health.2024;[Epub] CrossRef - Comparison of obturation quality in natural and replica teeth root-filled using different sealers and techniques
Chuta Kooanantkul, Richard M Shelton, Josette Camilleri
Clinical Oral Investigations.2023; 27(5): 2407. CrossRef - Obturation canalaire
N. Linas, M.-L. Munoz-Sanchez, N. Decerle, P.-Y. Cousson
EMC - Médecine buccale.2023; 16(5): 1. CrossRef - The Effect of Sealer Application Methods on Voids Volume after Aging of Three Calcium Silicate-Based Sealers: A Micro-Computed Tomography Study
Amre R. Atmeh, Rakan Alharbi, Ibrahim Aljamaan, Abdulrahman Alahmari, Ashwin C. Shetty, Ahmed Jamleh, Imran Farooq
Tomography.2022; 8(2): 778. CrossRef - Clinical Efficacy of Sealer-based Obturation Using Calcium Silicate Sealers: A Randomized Clinical Trial
Ji-hyung Kim, Sin-Yeon Cho, Yoonwoo Choi, Do-hyun Kim, Su-Jung Shin, Il-Young Jung
Journal of Endodontics.2022; 48(2): 144. CrossRef - A critical analysis of research methods and experimental models to study root canal fillings
Gustavo De‐Deus, Erick Miranda Souza, Emmanuel João Nogueira Leal Silva, Felipe Gonçalves Belladonna, Marco Simões‐Carvalho, Daniele Moreira Cavalcante, Marco Aurélio Versiani
International Endodontic Journal.2022; 55(S2): 384. CrossRef - Calcium Silicate Cements vs. Epoxy Resin Based Cements: Narrative Review
Mario Dioguardi, Cristian Quarta, Diego Sovereto, Giuseppe Troiano, Khrystyna Zhurakivska, Maria Bizzoca, Lorenzo Lo Muzio, Lucio Lo Russo
Oral.2021; 1(1): 23. CrossRef - Physico-Chemical Properties of Calcium-Silicate vs. Resin Based Sealers—A Systematic Review and Meta-Analysis of Laboratory-Based Studies
Viresh Chopra, Graham Davis, Aylin Baysan
Materials.2021; 15(1): 229. CrossRef - Micro-computed tomography in preventive and restorative dental research: A review
Mehrsima Ghavami-Lahiji, Reza Tayefeh Davalloo, Gelareh Tajziehchi, Paria Shams
Imaging Science in Dentistry.2021; 51(4): 341. CrossRef - Main and Accessory Canal Filling Quality of a Premixed Calcium Silicate Endodontic Sealer According to Different Obturation Techniques
Su-Yeon Ko, Hae Won Choi, E-Deun Jeong, Vinicius Rosa, Yun-Chan Hwang, Mi-Kyung Yu, Kyung-San Min
Materials.2020; 13(19): 4389. CrossRef
 ePub Link
ePub Link Cite
CiteA micro-computed tomographic evaluation of root canal filling with a single gutta-percha cone and calcium silicate sealer
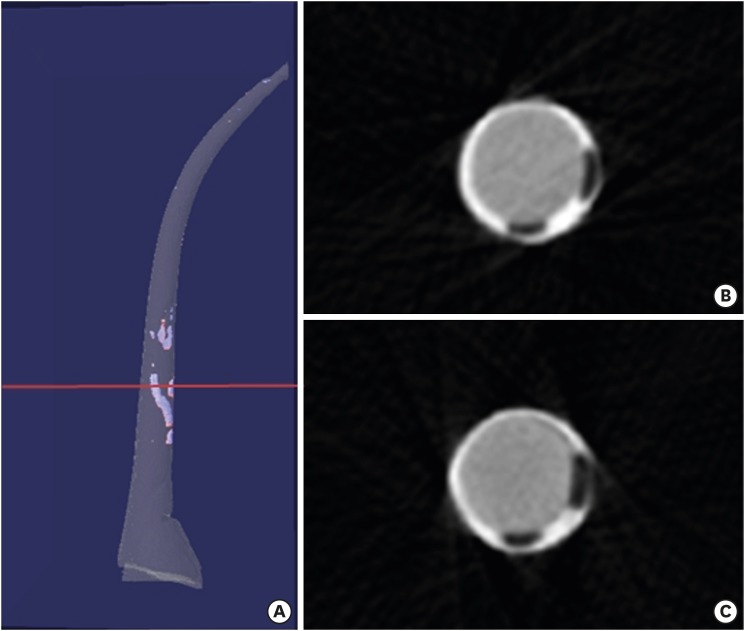
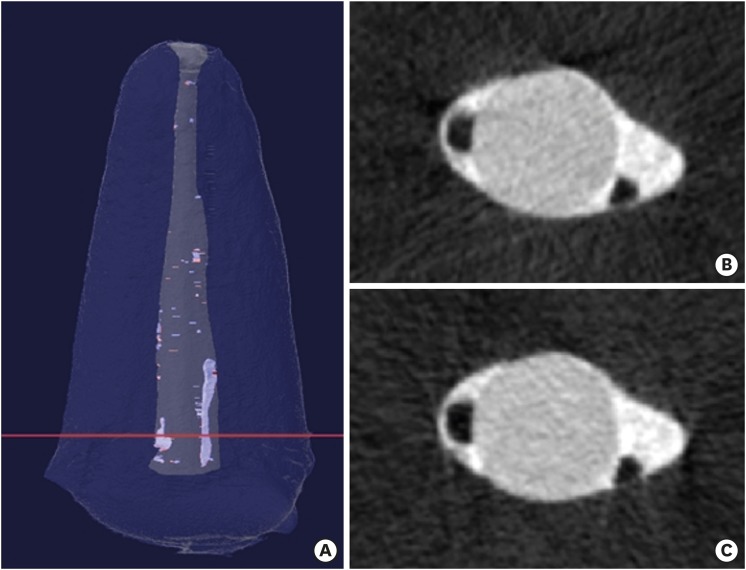
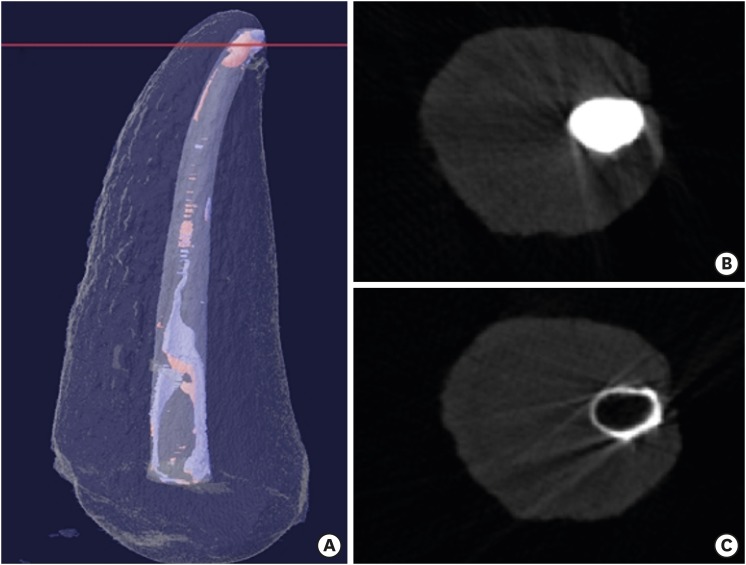
Figure 1 A sample of simulated root canal filled with Endoseal MTA sealer and single gutta-percha cone (A). Scanned images at the red line level of the left sample immediately after (B) and 4 weeks after (C) canal filling. Void of the first scan (B) is seen as blue, and void of the second scan (C) is seen as red in the left 3-dimensional modeling image.
Figure 2 A sample of extracted human root canal filled with Endoseal MTA sealer and a single gutta-percha cone (A). Scanned images at the red line level of the left sample immediately after (B) and 4 weeks after (C) canal filling. Void of the first scan (B) is seen as blue, and void of the second scan (C) is seen as red in the left 3-dimensional modeling image.
Figure 3 A sample of extracted human root canal filled with AH Plus Jet sealer and single gutta-percha cone. (A). Scanned images at the red line level of the left sample immediately after (B) and 4 weeks after (C) canal filling. Void of the first scan (B) is seen as blue, and void of the second scan (C) is seen as red in the left 3-dimensional modeling image. The increase of void at apical area and loss of sealer can be seen at the right image a second scan (C). It is also seen at the red lines on the upper side of this image (shadow projection).
Figure 1
Figure 2
Figure 3
A micro-computed tomographic evaluation of root canal filling with a single gutta-percha cone and calcium silicate sealer
Void percentage after root canal filling in the simulated root canals
| Void (%) of Endoseal MTA | Void (%) of AH Plus Jet | |||
|---|---|---|---|---|
| Immediately | 4 weeks later | Immediately | 4 weeks later | |
| Coronal | 0.18 ± 0.59a | 0.24 ± 0.80a | 0.09 ± 0.09a | 0.46 ± 0.50ab |
| Middle | 0.03 ± 0.04a | 0.02 ± 0.02a | 0.10 ± 0.15a | 0.22 ± 0.24a |
| Apical | 0.20 ± 0.10a | 0.33 ± 0.39a | 0.38 ± 0.48a | 0.96 ± 0.64b |
| Total | 0.13 ± 0.30a | 0.19 ± 0.40a | 0.15 ± 0.13a | 0.48 ± 0.35ab |
Data are presented as mean ± standard deviation. Statistical analysis was performed by 1-way ANOVA (p < 0.05) with the Tukey post hoc test. Different letters mean statistical differences in the same row. Four weeks later, there is a significant increase at the apical third of AH Plus Jet in comparison to immediately after the filling.
Void percentage after root canal filling in the extracted teeth
| Void (%) of Endoseal MTA | Void (%) of AH Plus Jet | |||
|---|---|---|---|---|
| Immediately | 4 weeks later | Immediately | 4 weeks later | |
| Coronal | 1.52 ± 1.62a | 1.39 ± 1.49a | 8.69 ± 7.24cd | 8.90 ± 7.24d |
| Middle | 1.40 ± 1.74a | 1.32 ± 1.63a | 6.58 ± 5.03abcd | 6.48 ± 5.01abcd |
| Apical | 1.38 ± 0.87a | 1.20 ± 0.68a | 3.10 ± 3.48ab | 3.42 ± 2.34abc |
| Total | 1.49 ± 1.29a | 1.37 ± 1.17a | 7.19 ± 4.87bcd | 7.24 ± 5.02bcd |
Data are presented as mean ± standard deviation. Statistical analysis was performed by 1-way ANOVA (p < 0.05) with the Tukey post hoc test. Different letters mean statistical differences in the same row. Four weeks later, there is no significant difference in comparison to immediately after the filling.
Table 1 Void percentage after root canal filling in the simulated root canals
Data are presented as mean ± standard deviation. Statistical analysis was performed by 1-way ANOVA (
Table 2 Void percentage after root canal filling in the extracted teeth
Data are presented as mean ± standard deviation. Statistical analysis was performed by 1-way ANOVA (

