
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 44(3); 2019 > Article
- Case Report A new minimally invasive guided endodontic microsurgery by cone beam computed tomography and 3-dimensional printing technology
-
Jong-Eun Kim1
 , June-Sung Shim1, Yooseok Shin2
, June-Sung Shim1, Yooseok Shin2 -
Restor Dent Endod 2019;44(3):e29.
DOI: https://doi.org/10.5395/rde.2019.44.e29
Published online: July 25, 2019
1Department of Prosthodontics, College of Dentistry, Yonsei University, Seoul, Korea.
2Department of Conservative Dentistry, Oral Science Research Center and Microscope Center, College of Dentistry, Yonsei University, Seoul, Korea.
- Correspondence to Yooseok Shin, DDS, PhD. Associate Professor, Department of Conservative Dentistry, Oral Science Research Center and Microscope Center, College of Dentistry, Yonsei University, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea. densys@yuhs.ac
• Received: July 13, 2019 • Revised: July 18, 2019 • Accepted: July 18, 2019
Copyright © 2019. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,358 Views
- 42 Download
- 24 Crossref
Abstract
- Endodontic microsurgery is defined as the treatment performed on the root apices of an infected tooth, which was unresolved with conventional root canal therapy. Recently, the advanced technology in 3-dimensional model reconstruction based on computed tomography such as cone beam computed tomography has opened a new avenue in application of personalized, accurate diagnosis and has been increasingly used in the field of dentistry. Nevertheless, direct intra-oral localization of root apex based on the 3-dimensional information is extremely difficult and significant amount of bone removal is inevitable when freehand surgical procedure was employed. Moreover, gingival flap and alveolar bone fenestration are usually required, which leads to prolonged time of surgery, thereby increasing the chance of trauma as well as the risk of infection. The purpose of this case report is to present endodontic microsurgery using the guide template that can accurately target the position of apex for the treatment of an anterior tooth with calcified canal which was untreatable with conventional root canal therapy and unable to track the position of the apex due to the absence of fistula.
INTRODUCTION
Endodontic microsurgery is, in its broadest sense, defined as the treatment performed on the root apices of an infected tooth, which was unresolved with conventional root canal therapy. Generally, procedure for endodontic microsurgery encompasses the removal of the buccal bone in order to accurately locate the root apices of an infected tooth, which may include the removal of intact bone. Then, surgical debridement of pathological peri-radicular tissue is performed, followed by the removal of root-end resection. A minimum of 3 mm preparation depth is required to effectively seal the accessory canals that may be present. Finally, a root-end cavity is obturated with Mineral Trioxide Aggregate (MTA) and the surgical site is sutured [1].
Unless there is a presence of fistula, which allows tracking the origin of the apical pathology, initial root tip localization and assessment for access site have been limited to the use of traditional 2-dimensional radiography such as periapical or panoramic radiograph. More recently, the advanced technology in 3-dimensional (3D) model reconstruction based on computed tomography such as cone beam computed tomography (CBCT) has opened a new avenue in application of personalized, accurate diagnosis and has been increasingly used in the field of dentistry [2]. Nevertheless, direct intra-oral localization of root apex based on the 3D information is extremely difficult and significant amount of bone removal is inevitable when freehand surgical procedure was employed. Moreover, gingival flap and alveolar bone fenestration are usually required, which leads to prolonged time of surgery, thereby increasing the chance of trauma as well as the risk of infection [3].
Indeed, CBCT has been widely used in contemporary implant dentistry for 3D pre-surgical planning and fabrication of surgical guide. Consequently, the use of guide template has become an emerging gold standard [4,5] for it allows patient-specific treatment, which is still being developed by advancement and refinement of computer-aided design and computer-aided manufacturing (CAD/CAM) technology and auxiliary devices including intra oral scanner, CAD software and 3D printer. Pre-surgical implant planning using 3D software offers prevention of disrupting adjacent root or anatomically vital structures and precise implant placement in correct position and angulation depending on the residual bone volume. It was also reported that the use of guided implantation is more accurate than freehand insertion [6].
The 3D software used for pre-surgical implant planning can be utilized in root-end resection, for it allows to avoid damage of adjacent tooth and to accurately determine the position of the affected area. Since 3D software for pre-surgical implant planning has been used successfully, its accuracy can be equally adapted to root-end resection, giving significantly improved control over drilling position as well as the depth of drilling. In the field of endodontics, the use of surgical template that reproduced the root canal morphology was attempted for the treatment of challenging tooth anomaly, which was untreatable with conventional freehand procedure [7]. Previous ex vivo study conducted with extracted human teeth also indicated that ‘guided endodontic technique’ allowed an accurate access cavity preparation and showed negligible influence of the operator, reducing operator dependent ‘technique sensitivity’ [8]. It was also reported that guide template was successfully employed into root-end resections, showing improved accuracy and reduced patient discomfort and surgery time by 30% [3]. However, this study used the guide template made by reverse engineering software, which may be limited for utilizing in daily-based clinical settings.
In this case report, we present endodontic microsurgery using the guide template that can accurately target the position of apex for the treatment of an anterior tooth with calcified canal which was untreatable with conventional root canal therapy and unable to track the position of the apex due to the absence of fistula.
CASE REPORT
A male patient, 25 years old, attended Yonsei University College of Dental Hospital complaining of pain in the maxillary right central incisor (tooth #21), which presented a history of trauma on tooth #21. After clinical and radiological examination, calcified canal was observed to be significant. Under a surgical microscope, localization of root canals was attempted twice but failed as patient continued to show clinical symptoms. Therefore, endodontic microsurgery was suggested, and patient consent was obtained. A CBCT scan was taken and apical radiolucency and completely blocked root canal with intact buccal bone were identified. Alginate impression was taken and poured up in yellow stone to obtain study cast. With conventional root-end resection, vast amount of buccal bone removal was inevitable and therefore, the use of minimally invasive guided endodontic microsurgery by using surgical template, cone-beam computed tomography and 3D printing technology was suggested as an alternative.
The study cast made by alginate impression was scanned and transformed to the digital data using tabletop scanner (Identica Blue; Medit Co., Seoul, Korea). Both CBCT data and digital data obtained from patient's study cast were imported to implant planning software (In2Guide; Cybermed Co., Seoul, Korea). Two sets of data were merged for the tooth image, so the surgical template was designed accordingly.
The guide template was designed to cover 5 teeth with maxillary left central incisor placed in the middle. Among various guide drills with different diameter contained within In2Guid Universal implant kit (Cybermed Co.), which is compatible with the guide template, anchor pin drill with 1.5 mm in diameter was selected for targeting root apex and sleeves to accommodate anchor pin drill was designed inside the template. The position and direction of sleeve were determined in consideration of approachable drill angulation as well as accessibility for minimum of 3 mm preparation depth. Finally, it was once more confirmed if the drill accurately aims for target root without damaging the adjacent root or surrounding vital structures. (Figure 1) Designed guide template was exported in forms of STereoLithography (STL) file and printed with 3D printer (Objet 260; Stratasys Co., MN, USA).
Figure 1
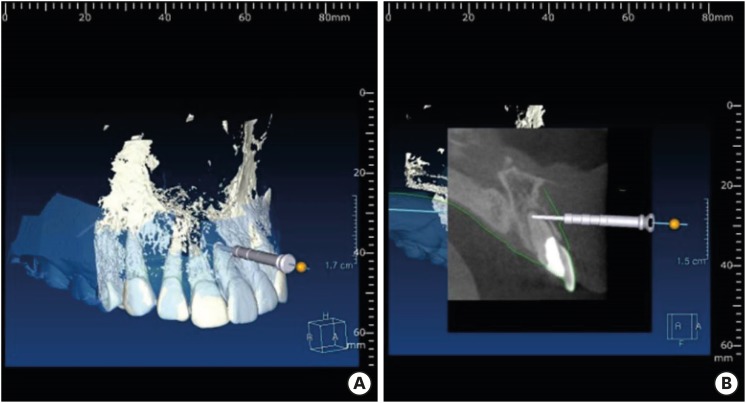
This figure demonstrates cone beam computed tomography (CBCT) data merged with STereoLithography (STL) data obtained from scanning dental cast on implant planning software. (A) Merging of CBCT (white) and STL (blue transparency) data with the area of targeting indicated. (B) Cross-sectional view of CBCT. Depth and angulation of drill can be determined.
Like conventional oral surgery, patient was prescribed amoxicillin (250 mg) and Ibuprofen (400 mg) 1 hour before surgery. Before starting microsurgery, surgical guide was applied to upper anterior area for checking its adaptation. Incisal opening of guide was helpful for fully adaptation between tooth and guide (Figure 2). The Leubke-Oschenbein flap design was applied after 1 ample local anesthesia (2% lidocaine with epinephrine 1:80,000; Huons, Seongnam, Korea) for minimal invasion. All surgical procedures were performed with an operating microscope (OPMI PICO; Carl Zeiss, Göttingen, Germany) (Supplemental Video 1).
Figure 2
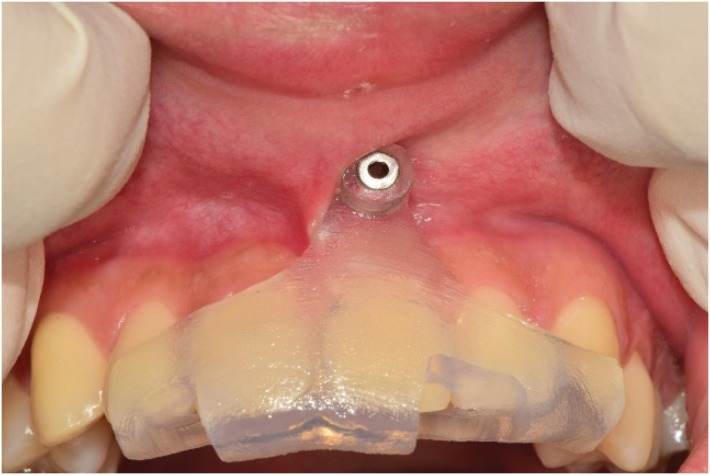
Clinical photograph showing intraoral guide template in situ. Windows made on the guide template indicates the fitness of the guide template.
Under the application of guide, surgical site was punched 3 mm depth with 2 mm straight rotary instrument (Figure 3A and 3B). After removing guide template, punched buccal bone was checked. Only apical buccal bone was prepared again with a No.6 round rotary straight instrument (No. 6; Prima Classic Prima Dental Group, Gloucester, UK) under distilled irrigation (Figure 3C). Exposed root tip was confirmed with methylene blue. And then root tip was finally prepared and removed with diamond high speed bur (Figure 3D). After removing of all inflammatory tissues, the resected root surfaces were then stained with methylene blue and inspected with micro-mirrors (Obtura Spartan, Fenton, MO, USA) under ×20 magnification to detect the canal space. The root-end preparation was made with KIS ultrasonic tips (Obtura Spartan). ProRoot MTA (Dentsply Tulsa Dental, Tulsa, OK, USA) used with the root-end filling material. ProRoot MTA was incrementally placed under the bleeding control, after that, the wound site was closed and sutured with 5 × 0 monofilament sutures. A post-operative radiograph was taken and compared with pre-operative radiograph (Figure 4). Only 30 minutes was taken for entire operation.
Figure 3

(A) Drilling with guide template placed. (B) After initial drilling, the position of targeting area can be identified. (C) Removal of adjacent labial bone using tooth #6 round bur after initial drilling. (D) Root resection as indicated by guide drilling after confirming the contour of root apex using methylene blue dye.
Figure 4
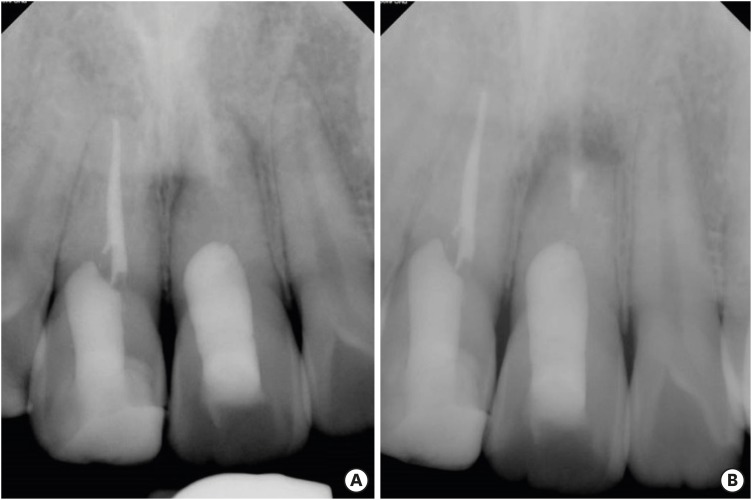
(A) Pre- and (B) post-operative periapical radiograph showing root-end fillings with Mineral Trioxide Aggregate (MTA).
After 1 month follow up, clinical symptom was completely resolved. No other signs of adverse effects around surrounding soft tissues were identified.
DISCUSSION
Endodontic microsurgery using the guide template has demonstrated improved accuracy over a free hand operation. Moreover, the guide template itself may act as soft tissue retractor, helping to avoid iatrogenic soft tissue damage. It is generally accepted that it is more advantageous to use the guide template for the clinical cases in which there is an apical pathology with clinical symptom but untreatable with conventional root canal therapy due to canal calcification and absence of fistula, which otherwise helps to identify the position of root apex.
Compared to the conventional approach, endodontic microsurgery using the guide template has many advantages: 1) root apex can be more accurately located through the provision of drilling hole, which will result in the minimal invasive preparation, 2) Surgical time and the volume of bone preparation can be significantly reduced, 3) Post-operative healing is more favorable and reduced risk of infection leads to better prognosis [9], and 4) more predictable and less-technique sensitive results can be expected regardless of clinician's experience. Therefore, it can also be used for educational purpose.
One of the most critical disadvantages of conventional root-end resection include the damage to anatomically vital structures such as inferior dental nerve, mental nerve, adjacent root and maxillary sinus. In contrast, endodontic microsurgery using the guide template significantly reduces these damages [10,11]. Pinsky et al. [2] confirmed in their in vitro study that the greater accuracy and consistency was achieved during endodontic surgery with surgical guidance without damaging vital structures. An error greater than 3 mm occurred over 22% of the time with freehand whereas none of errors occurred with surgical guidance [2].
Despite the aforementioned advantages, the limitations of guided endodontic microsurgery still do exist. Scattering artifact of CBCT caused by metal prosthesis may negatively affect the accuracy of diagnosis as accuracy of template is largely dependent on the process of merging CBCT data (DICOM) with digitalized intra oral data (STL). When there is much scattering artifact, the merging process cannot be accurately performed, leading to reduced accuracy of the template. Also, when the template is in situ, surgical access and vision may be disturbed by lips and cheeks for anterior and posterior region, respectively. Technically, the guide template and associated surgical kit were designed for implant placement not for the root-end resection and therefore, may have inappropriate length of metal sleeve or drills, which may restrict the use of surgical template for root-end resection.
In addition, accuracy of impression process may have a significant effect on the accuracy of guide template. Bubbles formed on impression material or gypsum model may reduce the accuracy. Consequently, in situ intraoral fitting of the guide template will be of great importance in determining the reliability and accuracy of root-end resection. Such was likewise this case in which guide template has to play both roles in accurately targeting the area 3 mm above the root apex as well as removal of such amount. In this sense, therefore, high-precision impression material such as rubber impression materials may better help to improve the accuracy of the guide template rather than using alginate impression.
Further clinical study may be required regarding surgical procedure for endodontic microsurgery using the guide template to improve the accuracy or to reduce the surgical time. Evaluation of accuracy depending on surgical site (anterior or posterior) may also be utilized to construct new treatment modality for the root-end resection. For easy application, it is also worth considering constructing guide template in ‘modeless’ manner using intraoral scanner.
CONCLUSIONS
Endodontic microsurgery using the guide template could be useful method in calcified canal which was untreatable with conventional root canal therapy and unable to track the position of the apex due to the absence of fistula.
-
Funding: This study was supported by a faculty research grant of Yonsei University new faculty research fund (6-2018-0025).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Shin Y.
Data curation: Kim JE.
Formal analysis: Kim JE.
Funding acquisition: Shin Y.
Investigation: Shim JS.
Methodology: Shin Y.
Project administration: Shin Y.
Resources: Shin Y.
Software: Kim JE.
Supervision: Shim JS.
Validation: Shim JS.
Visualization: Shin Y.
Writing - original draft: Kim JE.
Writing - review & editing: Shim JS.
SUPPLEMENTARY MATERIAL
- 1. von Arx T, Walker WA 3rd. Microsurgical instruments for root-end cavity preparation following apicoectomy: a literature review. Endod Dent Traumatol 2000;16:47-62.ArticlePubMedPDF
- 2. Pinsky HM, Champleboux G, Sarment DP. Periapical surgery using CAD/CAM guidance: preclinical results. J Endod 2007;33:148-151.ArticlePubMed
- 3. Liu Y, Liao W, Jin G, Yang Q, Peng W. Additive manufacturing and digital design assisted precise apicoectomy: a case study. Rapid Prototyping J 2014;20:33-40.Article
- 4. Yatzkair G, Cheng A, Brodie S, Raviv E, Boyan BD, Schwartz Z. Accuracy of computer-guided implantation in a human cadaver model. Clin Oral Implants Res 2015;26:1143-1149.ArticlePubMedPDF
- 5. D’Souza KM, Aras MA. Types of implant surgical guides in dentistry: a review. J Oral Implantol 2012;38:643-652.ArticlePubMedPDF
- 6. Arisan V, Karabuda ZC, Ozdemir T. Accuracy of two stereolithographic guide systems for computer-aided implant placement: a computed tomography-based clinical comparative study. J Periodontol 2010;81:43-51.ArticlePubMed
- 7. Byun C, Kim C, Cho S, Baek SH, Kim G, Kim SG, Kim SY. Endodontic treatment of an anomalous anterior tooth with the aid of a 3-dimensional printed physical tooth model. J Endod 2015;41:961-965.ArticlePubMed
- 8. Zehnder MS, Connert T, Weiger R, Krastl G, Kühl S. Guided endodontics: accuracy of a novel method for guided access cavity preparation and root canal location. Int Endod J 2016;49:966-972.ArticlePubMed
- 9. Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod 2006;32:601-623.ArticlePubMed
- 10. Wesson CM, Gale TM. Molar apicectomy with amalgam root-end filling: results of a prospective study in two district general hospitals. Br Dent J 2003;195:707-714.ArticlePubMedPDF
- 11. Phillips JL, Weller RN, Kulild JC. The mental foramen: 2. Radiographic position in relation to the mandibular second premolar. J Endod 1992;18:271-274.PubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Accuracy of Guided Drilling, Partially Guided Trephination, and Fully Guided Trephination Within a Static Surgical Guide for Apicoectomy in Hard Bone: An In Vitro Study
Fatima Jasim Humaid Alzaabi, Eszter Nagy, Dániel Gerhard Gryschka, Shishir Ram Shetty, Tarek Elsewify, Gábor Braunitzer, Hatem M. El-Damanhoury, Mark Adam Antal
Dentistry Journal.2026; 14(3): 155. CrossRef - Guided endodontic microsurgery using a simplified surgical guide for mandibular first molars with intact buccal cortical bone
Hyoung-Hoon Jo, Joo-Hun Song
Oral Biology Research.2026;[Epub] CrossRef - Effectiveness of guided endodontic microsurgery using a trephine bur in critical anatomical regions: a randomized controlled clinical trial
Rami Kaddoura, Thuraya Lazkani, Yasser Alsayed Tolibah
BDJ Open.2026;[Epub] CrossRef - A narrative review of papilla preservation techniques in clinical dentistry
Yinghua Fu, Zhixin Zhang, Xiaoping Tang, Jiangling Su
Medicine.2025; 104(3): e41033. CrossRef - Segmentation algorithms of dental CT images: A comprehensive review from classical to deep learning trend
Dianhao Wu, Jingang Jiang, Jinke Wang, Zhuming Bi, Guang Yu
Expert Systems with Applications.2025; 275: 126853. CrossRef - Endodontic Microsurgery of Mandibular Molars with an Autonomous Robotic System
Haiying Zhang, Zi Yang, Mangnan Liu, Yaoxin Wang, Mei Fu, Benxiang Hou, Chen Zhang
Journal of Endodontics.2025; 51(12): 1830. CrossRef - Removal of Extraradicular Separated Instrument by Targeted Endodontic Microsurgery Using the 3D‐Printed Guide and Trephine: A Case Report
Lin Yang, Liang Chen
Clinical Case Reports.2025;[Epub] CrossRef - Augmented Reality-Assisted Micro-Invasive Apicectomy with Markerless Visual–Inertial Odometry: An In Vivo Pilot Study
Marco Farronato, Davide Farronato, Federico Michelini, Giulio Rasperini
Applied Sciences.2025; 15(23): 12588. CrossRef - 3D finite element analysis of stress distribution on the shape of resected root-end or with/without bone graft of a maxillary premolar during endodontic microsurgery
Aein Mon, Mi-El Kim, Kee-Yeon Kum, Ho-Beom Kwon
Journal of Dental Sciences.2024; 19(2): 837. CrossRef - TREATMENT OF YATROGENIC POST-TRAUMATIC NEUROPATHY ASSOCIATED WITH
ENDODONTIC THERAPY USING 3D TECHNOLOGIES
Karen Sevterteryan, Vladislav Tarasenok, Lyudmila Tatintsyan
BULLETIN OF STOMATOLOGY AND MAXILLOFACIAL SURGERY.2024; : 73. CrossRef - Advancements in guided surgical endodontics: A scoping review of case report and case series and research implications
Giusy Rita Maria La Rosa, Matteo Peditto, Andrea Venticinque, Antonia Marcianò, Alberto Bianchi, Eugenio Pedullà
Australian Endodontic Journal.2024; 50(2): 397. CrossRef - Comparison of a Novel Static Computer-aided Surgical and Freehand Techniques for Osteotomy and Root-end Resection
Kyle Westbrook, Corey Rollor, Sara A. Aldahmash, Guadalupe G. Fay, Elias Rivera, Jeffery B. Price, Ina Griffin, Patricia A. Tordik, Frederico C. Martinho
Journal of Endodontics.2023; 49(5): 528. CrossRef - Comparison of the Three-Dimensional Accuracy of Guided Apicoectomy Performed with a Drill or a Trephine: An In Vitro Study
Ramóna Kiscsatári, Eszter Nagy, Máté Szabó, Gábor Braunitzer, József Piffkó, Márk Fráter, Márk Ádám Antal
Applied Sciences.2023; 13(17): 9642. CrossRef - Review of “Outcome of Endodontic Surgery: A Meta- Analysis of the Literature—Part 1: Comparison
of Traditional Root-End Surgery and Endodontic Microsurgery” by Setzer and Colleagues in J Endod 36(11):1757-1765, 2010
Oleksandr Nozhenko
Journal of Endodontic Microsurgery.2023; 2: 41. CrossRef - The Impact of the Preferred Reporting Items for Case Reports in Endodontics (PRICE) 2020 Guidelines on the Reporting of Endodontic Case Reports
Sofian Youssef, Phillip Tomson, Amir Reza Akbari, Natalie Archer, Fayjel Shah, Jasmeet Heran, Sunmeet Kandhari, Sandeep Pai, Shivakar Mehrotra, Joanna M Batt
Cureus.2023;[Epub] CrossRef - New-designed 3D printed surgical guide promotes the accuracy of endodontic microsurgery: a study of 14 upper anterior teeth
Dan Zhao, Weige Xie, Tianguo Li, Anqi Wang, Li Wu, Wen Kang, Lu Wang, Shiliang Guo, Xuna Tang, Sijing Xie
Scientific Reports.2023;[Epub] CrossRef - An Exploratory In Vitro Microcomputed Tomographic Investigation of the Efficacy of Semicircular Apicoectomy Performed with Trephine Bur
Eszter Nagy, Brigitta Vőneki, Lívia Vásárhelyi, Imre Szenti, Márk Fráter, Ákos Kukovecz, Márk Ádám Antal
Applied Sciences.2023; 13(16): 9431. CrossRef - The Time Has Come: Journal of Endodontic Microsurgery: A First Peer-Reviewed Open Access Publication Focused on Microsurgery in Endodontics
Ievgen Fesenko
Journal of Endodontic Microsurgery.2022;[Epub] CrossRef - Prefabricated Grid-guided Endodontic Microsurgery: A Pilot Study
Cruz Nishanthine, Manali Ramakrishnan Srinivasan, Ravi Devi, Kadhar Begam Farjana, Dasarathan Duraivel
Journal of Operative Dentistry & Endodontics.2022; 6(2): 58. CrossRef - Guided osteotomy
Saini Rashmi, Saini V Kr
Tanta Dental Journal.2022; 19(3): 172. CrossRef - Accuracy of digitally planned, guided apicoectomy with a conventional trephine and a custom-made endodontic trephine: An in vitro comparative study
Eszter Nagy, Gábor Braunitzer, Dániel Gerhard Gryschka, Ibrahim Barrak, Mark Adam Antal
Journal of Stomatology, Oral and Maxillofacial Surgery.2022; 123(4): 388. CrossRef - Stress Distribution on Trephine-Resected Root-end in Targeted Endodontic Microsurgery: A Finite Element Analysis
Yeon-Jee Yoo, Hiran Perinpanayagam, Miel Kim, Qiang Zhu, Seung-Ho Baek, Ho-Beom Kwon, Kee-Yeon Kum
Journal of Endodontics.2022; 48(12): 1517. CrossRef - An Update on Endodontic Microsurgery of Mandibular Molars: A Focused Review
Sun Mi Jang, Euiseong Kim, Kyung-San Min
Medicina.2021; 57(3): 270. CrossRef - When to consider the use of CBCT in endodontic treatment planning in adults
Nisha Patel, Andrew Gemmell, David Edwards
Dental Update.2021; 48(11): 932. CrossRef
 ePub Link
ePub Link Cite
CiteA new minimally invasive guided endodontic microsurgery by cone beam computed tomography and 3-dimensional printing technology
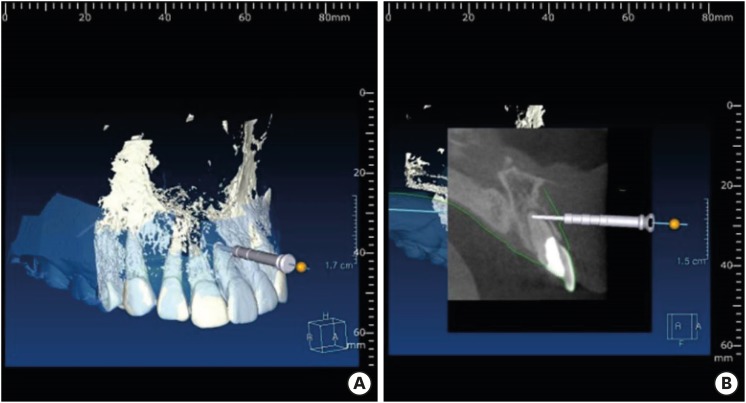

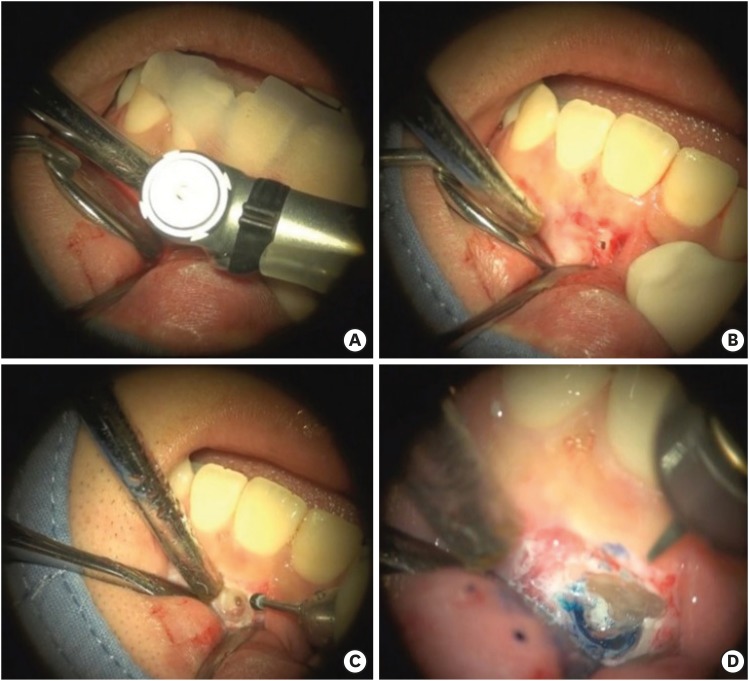
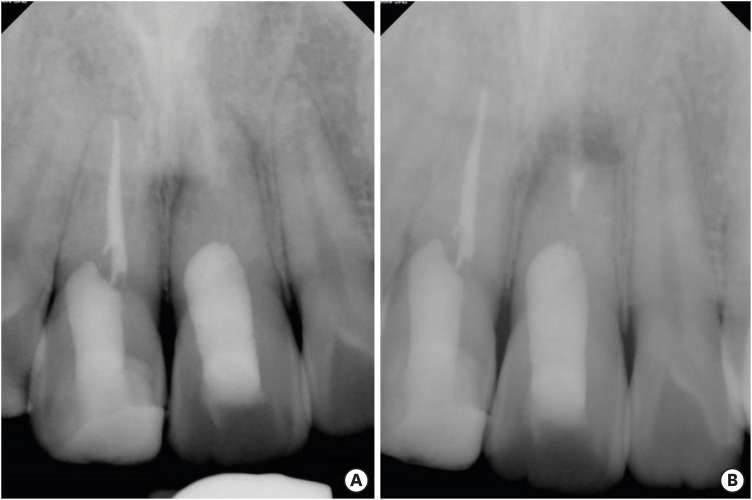
Figure 1 This figure demonstrates cone beam computed tomography (CBCT) data merged with STereoLithography (STL) data obtained from scanning dental cast on implant planning software. (A) Merging of CBCT (white) and STL (blue transparency) data with the area of targeting indicated. (B) Cross-sectional view of CBCT. Depth and angulation of drill can be determined.
Figure 2 Clinical photograph showing intraoral guide template in situ. Windows made on the guide template indicates the fitness of the guide template.
Figure 3 (A) Drilling with guide template placed. (B) After initial drilling, the position of targeting area can be identified. (C) Removal of adjacent labial bone using tooth #6 round bur after initial drilling. (D) Root resection as indicated by guide drilling after confirming the contour of root apex using methylene blue dye.
Figure 4 (A) Pre- and (B) post-operative periapical radiograph showing root-end fillings with Mineral Trioxide Aggregate (MTA).
Figure 1
Figure 2
Figure 3
Figure 4
A new minimally invasive guided endodontic microsurgery by cone beam computed tomography and 3-dimensional printing technology

