
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 44(1); 2019 > Article
- Research Article Discoloration of teeth due to different intracanal medicaments
-
Farzaneh Afkhami1
 , Sadaf Elahy2, Alireza Mahmoudi Nahavandi3, Mohamad Javad Kharazifard4, Aidin Sooratgar1
, Sadaf Elahy2, Alireza Mahmoudi Nahavandi3, Mohamad Javad Kharazifard4, Aidin Sooratgar1 -
Restor Dent Endod 2019;44(1):e10.
DOI: https://doi.org/10.5395/rde.2019.44.e10
Published online: February 12, 2019
1Department of Endodontics, Faculty of Dentistry, Tehran University of Medical Sciences, International Campus, Tehran, Iran.
2General Dentist, Private Practice, Tehran, Iran.
3Color Imaging and Color Image Processing Department, Institute for Color Science and Technology (ICST), Tehran, Iran.
4Department of Epidemiology and Biostatistics, Faculty of Public Health, Tehran University of Medical Sciences, Tehran, Iran.
- Correspondence to Aidin Sooratgar, DDS, MS. Assistant Professor, Department of Endodontics, Faculty of Dentistry, Tehran University of Medical Sciences, International Campus, Baradaran Mozaffar Street, Tehran 1856714984, Iran. a-sooratgar@sina.tums.ac.ir, aidin_s66@yahoo.com, f-afkhami@tums.ac.ir
• Received: June 30, 2018 • Revised: October 10, 2018 • Accepted: October 30, 2018
Copyright © 2019. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,362 Views
- 70 Download
- 13 Crossref
Abstract
-
Objectives The objective of this study was to assess coronal discoloration induced by the following intracanal medicaments: calcium hydroxide (CH), a mixture of CH paste and chlorhexidine gel (CH/CHX), and triple antibiotic paste (3Mix).
-
Materials and Methods Seventy extracted single-canal teeth were selected. Access cavities were prepared and each canal was instrumented with a rotary ProTaper system. The specimens were randomly assigned to CH, CH/CHX, and 3Mix paste experimental groups (n = 20 each) or a control group (n = 10). Each experimental group was randomly divided into 2 subgroups (A and B). In subgroup A, medicaments were only applied to the root canals, while in subgroup B, the root canals were completely filled with medicaments and a cotton pellet dipped in medicament was also placed in the pulp chamber. Spectrophotometric readings were obtained from the mid-buccal surface of the tooth crowns immediately after placing the medicaments (T1) and at 1 week (T2), 1 month (T3), and 3 months (T4) after filling. The ∆E was then calculated. Data were analyzed using 2-way analysis of variance (ANOVA), 3-way ANOVA, and the Scheffé post hoc test.
-
Results The greatest color change (ΔE) was observed at 3 months (p < 0.0001) and in 3Mix subgroup B (p = 0.0057). No significant color change occurred in the CH (p = 0.7865) or CH/CHX (p = 0.1367) groups over time, but the 3Mix group showed a significant ΔE (p = 0.0164).
-
Conclusion Intracanal medicaments may induce tooth discoloration. Use of 3Mix must be short and it must be carefully applied only to the root canals; the access cavity should be thoroughly cleaned afterwards.
INTRODUCTION
Endodontic treatment aims to prevent or control pulp and periapical infections. Due to the role of microorganisms in the pathogenesis of periradicular lesions, it is obvious that endodontic treatment outcomes depend on the reduction or elimination of microorganisms [1]. Bacteria invading the root canal system are responsible for the initiation and persistence of periapical diseases. Thus, elimination of bacteria from the root canal system is among the main goals of endodontic treatment [1,2,3]. The microbial count can be decreased by cleaning and shaping the root canal system, but cleaning and shaping cannot completely eliminate the bacteria lodged in the accessory canals. Thus, intracanal medicaments are recommended for use between treatment sessions to decrease the bacterial count in the root canal system [4,5,6]. Intracanal medicaments have several clinical applications, including management of traumatized teeth, treatment of teeth with extensive periapical lesions or inflammatory root resorption, and apexification and revascularization of permanent immature teeth [7]. Many intracanal medicaments cause tooth discoloration, especially when they remain in the tooth crown for a long period of time [8]. Tooth discoloration primarily occurs due to the penetration of materials into the dentinal tubules. Furthermore, it was shown that materials placed in the pulp chamber for long periods of time darkened the teeth over time [9]. Tooth discoloration due to the use of endodontic materials compromises esthetics. Therefore, endodontic treatment should not only focus on biological and practical aspects, but also take esthetics into account because tooth discoloration results in patient dissatisfaction [10].
Calcium hydroxide (CH) is extensively used as an intracanal material. This material has several favorable biological properties, such as antimicrobial activity, tissue-dissolving ability, prevention of tooth resorption, and induction of hard tissue barrier formation. Due to these characteristics, CH has several clinical applications. At present, this chemical agent is believed to be the most effective intracanal medicament for endodontic treatment [8,9]. Some studies have reported tooth discoloration, although insignificant, due to the application of CH [8,10,11,12]. Some additional materials have been incorporated into the formulation of CH to confer antibacterial properties or radiopacity; it has been suggested that these materials may result in tooth discoloration following the application of CH [10,13].
Chlorhexidine (CHX) has long been suggested for use as an intracanal medicament due to its broad-spectrum antimicrobial activity and substantivity. Previous studies have found that a mixture of CH and CHX had greater antibacterial efficacy than CH alone [14,15]. Enamel discoloration has been reported following the use of CHX mouthwash [16,17,18]; however, no study has evaluated tooth discoloration following the application of CHX combined with CH as an intracanal medicament.
Triple antibiotic paste (3Mix) (metronidazole, ciprofloxacin, and minocycline) has recently been used as an intracanal medicament for disinfection of root canals during endodontic treatment [9,10]. Studies on tooth discoloration following the use of 3Mix are scarce, but tooth discoloration following the use of this paste has been reported. Minocycline has also been found to cause significant discoloration in the tooth crown [9,19].
This study aimed to compare tooth discoloration following the application of different intracanal medicaments. Additionally, the effect of the location of intracanal medicament placement on coronal discoloration was evaluated.
MATERIALS AND METHODS
This study protocol was approved by the Institutional Ethical Committee (IRB No. IR.TUMS.IC.1392/1804). Human anterior maxillary teeth extracted for periodontal treatment were used in this study. The teeth were immersed in 0.5% sodium hypochlorite (NaOCl) solution for 30 minutes to eliminate the soft tissue debris and to disinfect the teeth. The teeth were then immersed in 0.5% chloramine-T solution (Merck, Darmstadt, Germany) and stored in dark conditions until the experiment.
Seventy single-rooted teeth with straight roots, no caries, no cracks or fractures, no resorption, a closed apex, and no cervical wear were included in this study. The calculus and debris were removed by a scaler and pumice paste and polishing cups. The teeth were inspected for cracks and resorption under a stereomicroscope (SM X800, Nikon Co., Melville, NY, USA). Radiographs were taken to ensure that the teeth had a single root canal. Standard access cavities were prepared using a round bur (Dentsply Maillefer, Ballaigues, Switzerland) and a fissure bur (d&z, Wiesbaden, Germany). A size 15 K-file (Mani Inc., Tochigi, Japan) was used for to determine the working length. The file was introduced into the canal until its tip was visible at the apex. One millimeter was subtracted from this length to yield the working length. Each canal was prepared with ProTaper rotary instrument (Dentsply Maillefer,) according to the manufacturer's instructions (S1, S2, F1, F2, F3, F4, and F5, respectively). RC-Prep (Premier Dental, Plymouth Meeting, PA, USA) was used as a lubricant and 10 mL of 2.5% NaOCl was used as an irrigant. The smear layer was eliminated using 1 mL of 17% ethylenediaminetetraacetic acid (Aria Dent, Tehran, Iran) and 1 mL of 5.25% NaOCl each for 3 minutes at the end of root canal preparation. The final rinse was done using 10 mL of normal saline. The apical foramen of each tooth was sealed with self-cured glass ionomer (Fuji Corporation, Tokyo, Japan). The teeth were then mounted in clear acrylic blocks (Acropars, Tehran, Iran) measuring 2 cm in length, 1 cm in width, and 4 cm in height in such a way that the apical two-thirds of the roots was embedded in acrylic resin (Figure 1). Tiny squares measuring 1.5 × 1.5 mm were prepared at the mid-buccal surface of all teeth by a fissure bur (Dentsply Maillefer) to be used as a reference for repeated measurements.
Next, the teeth were randomly divided into 3 experimental groups (n = 20 each) and 1 control group (n = 10). The groups are shown in Table 1. In the control group, the canals were filled with saline and a cotton pellet was placed in the pulp chamber. Each experimental group was randomly divided into 2 subgroups of 10 (A and B). In subgroup A, we tried our best to apply the medicaments only to the root canals (below the cementoenamel junction), and a small cotton pellet was placed in the pulp chamber. In subgroup B, the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber. The access cavity in all specimens was then restored with Cavit (3M ESPE, Seefeld, Germany). During the experiment, the teeth were in an upright position to prevent the flow of the medicaments in the root canal system towards the coronal portion of the teeth. All the teeth were kept in a dark glass jar, completely covered with a piece of cotton, and stored in an incubator at 37°C and 100% humidity.
Table 1
Medicaments in the experimental and control groups
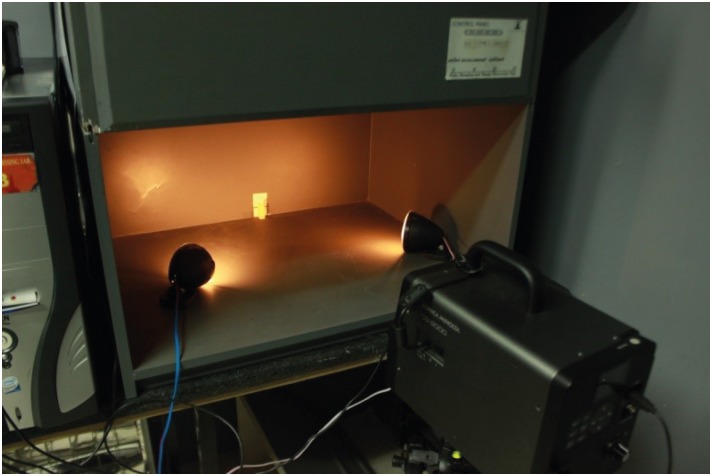
Color assessments were done immediately after the placement of medicaments in the root canals (baseline=T0) and at 1 week (T1), 1 month (T2), and 3 months (T3) using the CIELAB color space. Spectral reflectance measurements were made using a spectrophotometer (CS-2000, Konica Minolta, Tokyo, Japan) and the obtained data were converted to color coordinates in D65/20 geometry using Konica Minolta CS-S10w Professional Edition software (Konica Minolta Sensing Americas, Inc., Ramsey, NJ, USA). At each time of evaluation, the specimens were fixed on a jig, and color measurements were made at 20°C. Before each set of measurements, the spectrophotometer was calibrated according to the manufacturer's instructions. At each time point, 3 measurements were made of each specimen against a white background and the mean of the measurements was calculated. The light source illuminated the specimen surface at a 45° angle relative to the sample's perpendicular axis. The spectrophotoradiometer was adjusted at an angle of 0° relative to the sample's perpendicular axis at a distance of 70 cm from the specimens (Figure 2). The viewing angle of the device was adjusted to 0.1°, yielding a circular measurement area with a 1.2 mm diameter at the center of the specimens' crown.
The color change between different time points was calculated using the formula below [20]:
Where L* indicates lightness-darkness, a* indicates redness-greenness, and b* indicates yellowness-blueness of the samples [21].
The L*, b*, and a* parameters of the samples were measured and compared to the baseline values. In the experimental groups, ΔE*, ΔL*, Δb*, and Δa* were compared at different time points using 2-way analysis of variance (ANOVA). To compare the mean values of appearance changes caused by different medicaments, three-way ANOVA was performed on the ΔE*,ΔL*,Δb*, and Δa* parameters. The causes of differences were analyzed by post hoc ANOVA using the Scheffé method, and p-values < 0.05 were considered to indicate statistical significance.
RESULTS
The treatment groups did not have significant differences at baseline in the L* (p = 0.05), a* (p = 0.59), or b* (p = 0.32) parameters. At 3 months, the 3Mix group showed the highest ΔE* compared to other time points and medicaments. The ΔE*, ΔL*, Δa*, and Δb* values of different groups and subgroups (based on where the medicament was placed) at different time points are shown in Tables 2, 3, 4, 5.
Table 2
Mean ΔE* values ± standard deviation of tooth samples from the different groups and at different time points
The same uppercase letters in a row and the lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Table 3
Mean ΔL* values ± standard deviation of tooth samples from the different groups and at different time points
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Table 4
Mean Δa* values ± standard deviation of tooth samples from the different groups and at different time points
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Table 5
Mean Δb* values ± standard deviation of tooth samples from the different groups at different time points
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
The CH group showed no significant differences in ΔE* at different time points (p = 0.7865). Furthermore, no difference with regard to where the medicament was placed was noted in the CH group (p = 0.2906). However, the ΔL* values of the specimens showed significant differences across different time points (p = 0.0015), and also depending on the location of medicament placement (p = 0.0278). The ΔE* in the group treated with a CH/CHX mixture showed no significant difference at different time points (p = 0.1367). However, when the medicament was placed in the pulp chamber, ΔE was significantly higher than when it was only applied to the root canal (p = 0.0377). Two-way ANOVA showed significant differences in ΔL* among different time points (p = 0.0001), and the specimens became lighter over time; however, no significant difference in ΔL* was found based on the location of medicament placement (p = 0.7132).
Analysis of the ΔE* and ΔL* values of the specimens treated with 3Mix showed significant differences across different time points (p = 0.0164 and p = 0.0044, respectively) and depending on the location of medicament placement (p = 0.0057 and p = 0.0380, respectively).
Three-way ANOVA showed significant differences among groups in terms of ΔE* (p < 0.0001). Post hoc analysis revealed that the 3Mix group had significant differences from other groups; but the difference in this regard between the CH and CH/CHX groups was not significant. Similar results were obtained with regard to the ΔL* parameter among different medicaments, with the 3Mix group being much darker than the other 2 groups (p < 0.0001).
DISCUSSION
Misshapen or discolored teeth are among the main concerns for which adults, especially female patients and young individuals, seek esthetic dental treatments. Tooth discoloration can affect individuals' self-confidence and social activities. In children, tooth discoloration can result in being mocked or bullied. Many patients undergoing root canal treatment are worried about the appearance of their teeth and possible postoperative discoloration [10].
Intracanal medicaments are used in many different ways in endodontics. For instance, in a necrotic tooth, CH is used as an intracanal medicament at a 1-week interval between treatment sessions for its antibacterial effects. CH is also used for apexification of immature teeth and during the monitoring of traumatized teeth for several weeks to months [22]. Other medicaments, such as 3Mix, are used in the root canal system for long periods of time in treatments such as revascularization [23]. Thus, tooth color assessments were done in the current study at multiple time intervals.
Colorimetry can be done visually or instrumentally. Visual colorimetry is performed using shade guides; which are extensively used by dentists. This analysis is influenced by the operator and the environment [10]. In contrast, spectrophotometry provides reliable, documented, high-quality, and reproducible colorimetric data [24]. Since the tooth surface is convex, not straight, a tele-spectrophotometer is preferred for color assessment. We used a CS2000 Konica Minolta spectrophotometer in the current study. This device is capable of making reproducible measurements from a non-straight surface [10,24].
Lenherr et al. [10] used extracted human teeth to assess color changes due to the application of endodontic materials. Similarly, we used extracted human teeth, since these teeth show the same patterns of color change as natural teeth in the oral cavity and better simulate clinical circumstances [10]. Similar to previous studies, a proper access cavity was prepared to allow placement of an adequate amount of material in the pulp chamber for a long period of time (3 months). The cavity was completely sealed to prevent extrusion of material through the access cavity [9].
Smear layer removal can affect the permeability of dentin, consequently influencing color change [9]. Kim et al. [9] reported that smear layer removal increased the color change of teeth. However, since recent disinfection protocols recommend smear layer removal to more efficiently clean the root canal system [9], the smear layer was removed in the current study.
The CIE L*a*b* system was used for color assessment in the present study. According to this system, the L* parameter indicates lightness; +a* indicates redness and –a* indicates greenness. The +b* values indicate yellowness and −b* values indicate blueness. Finally, ΔE* shows the overall color change perceivable by the human eye [21].
CH as an intracanal medicament is marketed with different formulations, which can affect its discoloration potential [25,26]. Lenherr et al. [10], demonstrated that CH (ProduitsDentaires, SA, Vevey, Switzerland) alone and UltracalXS did not cause tooth discoloration after 12 weeks of application, and the changes in tooth color were not perceivable by the human eye. Moreover, Kim et al. [9], indicated that CH did not cause significant changes in tooth color compared to the control group, although CH resulted in yellowness and lightening of specimens. To explain this phenomenon, it has been proposed that the penetration of calcium ions into the dentinal tubules and their reaction with the hydroxyapatite crystals in the tubules result in lightening and yellowness of teeth medicated with CH [10,27]. In the present study, overall changes in tooth color did not occur and the color of teeth did not significantly change along the yellowness-blueness axis, but changes were noted in lightness. Similarly, Day et al. [28] reported an increase in the lightness of specimens. Changes in lightness may occur because a cotton pellet dipped in CH is darker than a plain cotton pellet, may help explain why lower lightness changes were observed after treatment with CH in subgroup B (crown) than in subgroup A (root). Considering the significant effect of time on the greenness-redness parameter, the change in the mean values in the groups responsible for the significant differences (T1 and T4) was only 0.6 units, which is lower than the perceivable color change by the human eye (3.7). In the present study, CH was used in the Metapex formulation, which has been shown not to cause significant discoloration as an intracanal medicament. Furthermore, this product is premixed and has a homogenous consistency, making it possible to place the CH paste in the same amount and density in all specimens [29,30].
In general, CH as a medicament did not cause any color change, in contrast to the 3Mix group, and the color change in this group was similar to that in the CH/CHX group.
In dentistry, CHX mouthwash is used for plaque control. Studies have shown that continuous use of CHX mouthwash results in tooth staining [31,32]. However, no study has shown that application of CHX gel as an intracanal medicament leads to tooth discoloration. In the present study, color changes occurred in the CH/CHX group both when a cotton pellet dipped in medicament was placed in the crown in subgroup B and when a cotton pellet without the medicament was used in subgroup A. The presence of a red tint in the specimens over time may have been due to the pink color of the CHX medicament, which shifts the color change towards redness in the red-green axis. This medicament was not significantly different from CH alone in terms of color change, but, it was significantly different from 3Mix [33].
Considering the increase in the reported cases of revascularization in the literature, 3Mix is often used for disinfection of root canals in these teeth. The greatest color change among the experimental groups in this study occurred in the 3Mix group; this color change in different studies has been attributed to the presence of minocycline in the composition of 3Mix [19]. Minocycline, a bacteriostatic agent, is derived from tetracycline [34]. When in direct contact with the tooth surface, it bonds to the calcium ions in dentin and forms an insoluble compound that results in tooth surface discoloration [28]. Discoloration starts in the first week and gradually increases with further penetration of the medicament until the tooth becomes completely dark. Similarly, Lenherr et al. [10], showed that the greatest color change occurred at 12 weeks. In another study, Kim et al. [27] demonstrated that 3Mix containing minocycline showed a greater color change than other 3Mix formulations, in which minocycline had been replaced with another antibiotic.
In a study by Kim et al. [9], color change due to the application of Ledermix as an intracanal medicament was evaluated. The results showed that its application led to tooth discoloration, and greater discoloration was found in the group where the medicament was placed in the pulp chamber than in the group where the medicament was placed only in the root canals [35]. The reason for this may be that coronal dentin is more permeable than root dentin. The antibiotic in Ledermix infiltrates into the dentinal tubules and bonds to dentin, resulting in tooth discoloration. In the current study, the cause of severe discoloration was the reaction of 3Mix with dentin, which led to tooth darkening following the use of this medicament. Its further penetration into the tubules over time is why the greatest discoloration was found after 3 months of treatment. The significant differences depending on where 3Mix was placed may have been due to the effect of direct placement of the medicament in the access cavity.
CONCLUSIONS
The 3Mix medicament must be used for a short period of time to minimize tooth discoloration. It would also be better not to use 3Mix in teeth visible in the smile line. If 3Mix must be used in these teeth, care must be taken to limit its application to the root canal system, and the remaining paste in the pulp chamber must be thoroughly cleaned. Long-term use of a mixture of CH and CHX as an intracanal medicament does not compromise esthetics, but its application must be limited to the root canals.
-
Funding: This research was supported by Tehran University of Medical Sciences, International Campus (grant No. 92-02-168-22998). The authors report no conflicts of interest.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Afkhami F.
Data curation: Kharazifard MJ.
Formal analysis: Kharazifard MJ.
Funding acquisition: Elahy S.
Investigation: Elahy S.
Methodology: Afkhami F, Mahmoudi Nahavandi A.
Project administration: Afkhami F, Elahy S.
Resources: Elahy S.
Software: Sooratgar A.
Supervision: Mahmoudi Nahavandi A.
Validation: Afkhami F.
Visualization: Elahy S.
Writing - original draft: Afkhmi F.
Writing - review & editing: Sooratgar A.
- 1. DaSilva L, Finer Y, Friedman S, Basrani B, Kishen A. Biofilm formation within the interface of bovine root dentin treated with conjugated chitosan and sealer containing chitosan nanoparticles. J Endod 2013;39:249-253.ArticlePubMed
- 2. Shrestha A, Shi Z, Neoh KG, Kishen A. Nanoparticulates for antibiofilm treatment and effect of aging on its antibacterial activity. J Endod 2010;36:1030-1035.ArticlePubMed
- 3. Kishen A, Shi Z, Shrestha A, Neoh KG. An investigation on the antibacterial and antibiofilm efficacy of cationic nanoparticulates for root canal disinfection. J Endod 2008;34:1515-1520.ArticlePubMed
- 4. Safavi K, Nakayama TA. Influence of mixing vehicle on dissociation of calcium hydroxide in solution. J Endod 2000;26:649-651.ArticlePubMed
- 5. Ballal V, Kundabala M, Acharya S, Ballal M. Antimicrobial action of calcium hydroxide, chlorhexidine and their combination on endodontic pathogens. Aust Dent J 2007;52:118-121.ArticlePubMed
- 6. Valera MC, Silva KC, Maekawa LE, Carvalho CA, Koga-Ito CY, Camargo CH, Lima RS. Antimicrobial activity of sodium hypochlorite associated with intracanal medication for Candida albicans and Enterococcus faecalis inoculated in root canals. J Appl Oral Sci 2009;17:555-559.ArticlePubMedPMC
- 7. Ahmed HM, Abbott PV. Discolouration potential of endodontic procedures and materials: a review. Int Endod J 2012;45:883-897.ArticlePubMed
- 8. Thomson AD, Athanassiadis B, Kahler B, Walsh L. Tooth discolouration: staining effects of various sealers and medicaments. Aust Endod J 2012;38:2-9.ArticlePubMed
- 9. Kim ST, Abbott PV, McGinley P. The effects of Ledermix paste on discolouration of immature teeth. Int Endod J 2000;33:233-237.ArticlePubMed
- 10. Lenherr P, Allgayer N, Weiger R, Filippi A, Attin T, Krastl G. Tooth discoloration induced by endodontic materials: a laboratory study. Int Endod J 2012;45:942-949.ArticlePubMed
- 11. Ordinola-Zapata R, Bramante CM, Minotti PG, Cavenago BC, Garcia RB, Bernardineli N, Jaramillo DE, Hungaro Duarte MA. Antimicrobial activity of triantibiotic paste, 2% chlorhexidine gel, and calcium hydroxide on an intraoral-infected dentin biofilm model. J Endod 2013;39:115-118.ArticlePubMed
- 12. Rahimi S, Janani M, Lotfi M, Shahi S, Aghbali A, Vahid Pakdel M, Salem Milani A, Ghasemi N. A review of antibacterial agents in endodontic treatment. Iran Endod J 2014;9:161-168.PubMedPMC
- 13. Almyroudi A, Mackenzie D, McHugh S, Saunders WP. The effectiveness of various disinfectants used as endodontic intracanal medications: an in vitro study. J Endod 2002;28:163-167.ArticlePubMed
- 14. Javidi M, Afkhami F, Zarei M, Ghazvini K, Rajabi O. Efficacy of a combined nanoparticulate/calcium hydroxide root canal medication on elimination of Enterococcus faecalis . Aust Endod J 2014;40:61-65.PubMed
- 15. Wu D, Fan W, Kishen A, Gutmann JL, Fan B. Evaluation of the antibacterial efficacy of silver nanoparticles against Enterococcus faecalis biofilm. J Endod 2014;40:285-290.PubMed
- 16. Hennessey TS. Some antibacterial properties of chlorhexidine. J Periodontal Res Suppl 1973;12:61-67.ArticlePubMed
- 17. Dametto FR, Ferraz CC, Gomes BP, Zaia AA, Teixeira FB, de Souza-Filho FJ. In vitro assessment of the immediate and prolonged antimicrobial action of chlorhexidine gel as an endodontic irrigant against Enterococcus faecalis . Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:768-772.ArticlePubMed
- 18. Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod 2004;30:196-200.ArticlePubMed
- 19. Akcay M, Arslan H, Yasa B, Kavrık F, Yasa E. Spectrophotometric analysis of crown discoloration induced by various antibiotic pastes used in revascularization. J Endod 2014;40:845-848.ArticlePubMed
- 20. Agahian F, Amirshahi SA, Amirshahi SH. Reconstruction of reflectance spectra using weighted principal component analysis. Color Res Appl 2008;33:360-371.Article
- 21. Lee YK, Lim BS, Powers JM. Color changes of dental resin composites by a salivary enzyme. J Biomed Mater Res B Appl Biomater 2004;70:66-72.ArticlePubMed
- 22. Sjögren U, Figdor D, Spångberg L, Sundqvist G. The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int Endod J 1991;24:119-125.ArticlePubMed
- 23. Garcia-Godoy F, Murray PE. Recommendations for using regenerative endodontic procedures in permanent immature traumatized teeth. Dent Traumatol 2012;28:33-41.ArticlePubMed
- 24. Feiz A, Barekatain B, Khalesi S, Khalighinejad N, Badrian H, Swift EJ. Effect of several bleaching agents on teeth stained with a resin-based sealer. Int Endod J 2014;47:3-9.ArticlePubMed
- 25. Jung IY, Lee SJ, Hargreaves KM. Biologically based treatment of immature permanent teeth with pulpal necrosis: a case series. J Endod 2008;34:876-887.ArticlePubMed
- 26. Gomes-Filho JE, Duarte PC, de Oliveira CB, Watanabe S, Lodi CS, Cintra LT, Bernabé PF. Tissue reaction to a triantibiotic paste used for endodontic tissue self-regeneration of nonvital immature permanent teeth. J Endod 2012;38:91-94.ArticlePubMed
- 27. Kim JH, Kim Y, Shin SJ, Park JW, Jung IY. Tooth discoloration of immature permanent incisor associated with triple antibiotic therapy: a case report. J Endod 2010;36:1086-1091.ArticlePubMed
- 28. Day PF, Duggal MS, High AS, Robertson A, Gregg TA, Ashley PF, Welbury RR, Cole BO, Westland S. Discoloration of teeth after avulsion and replantation: results from a multicenter randomized controlled trial. J Endod 2011;37:1052-1057.ArticlePubMed
- 29. Afkhami F, Elahy S, Mahmoudi-Nahavandi A. Spectrophotometric analysis of crown discoloration following the use of silver nanoparticles combined with calcium hydroxide as intracanal medicament. J Clin Exp Dent 2017;9:e842-e847.ArticlePubMedPMC
- 30. Kabaktchieva R, Gateva N, Gusiyska A, Stanimirov P, Milcheva N. Dental care for children after replantation of avulsed permanent incisors. J IMAB 2016;22:1392-1402.Article
- 31. van Maanen-Schakel NW, Slot DE, Bakker EW, Van der Weijden GA. The effect of an oxygenating agent on chlorhexidine-induced extrinsic tooth staining: a systematic review. Int J Dent Hyg 2012;10:198-208.ArticlePubMedPDF
- 32. Gomes BP, Souza SF, Ferraz CC, Teixeira FB, Zaia AA, Valdrighi L, Souza-Filho FJ. Effectiveness of 2% chlorhexidine gel and calcium hydroxide against Enterococcus faecalis in bovine root dentine in vitro. Int Endod J 2003;36:267-275.ArticlePubMedPDF
- 33. Wang CS, Arnold RR, Trope M, Teixeira FB. Clinical efficiency of 2% chlorhexidine gel in reducing intracanal bacteria. J Endod 2007;33:1283-1289.ArticlePubMed
- 34. Windley W 3rd, Teixeira F, Levin L, Sigurdsson A, Trope M. Disinfection of immature teeth with a triple antibiotic paste. J Endod 2005;31:439-443.ArticlePubMed
- 35. Jang JH, Kang M, Ahn S, Kim S, Kim W, Kim Y, Kim E. Tooth discoloration after the use of new pozzolan cement (Endocem) and mineral trioxide aggregate and the effects of internal bleaching. J Endod 2013;39:1598-1602.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Time-dependent Tooth Color Changes Following Conventional, Silver-based, and Photodynamic Root Canal Irrigants: An In Vitro Study
Laila Mohamed Mohamed Kenawi, Mohamed Fattouh, Khaled Abid Althaqafi, Abla Arafa
The Open Dentistry Journal.2026;[Epub] CrossRef - Comparative analysis of tooth discoloration induced by different intracanal medicaments in regenerative endodontics: A systematic review and network meta-analysis
Ashlesha Nageshwar Madankar, Sulabha Radke, Shanmuga Priya, Darshan Dakshindas
Endodontology.2026; 38(1): 8. CrossRef - Effects of Intra-canal Medicaments on Infrared Light Energy Transmission Through Enamel and Dentin During Photobiomodulation: An In Vitro Study
Sachin Kulkarni, Laurence J. Walsh, Yash Bhurani, Roy George
Journal of Endodontics.2025; 51(5): 616. CrossRef - Tooth discoloration caused by nanographene oxide as an irrigant and intracanal medicament in the endodontic treatment of extracted single-rooted teeth: An ex-vivo study
Abbas Abbaszadegan, Zeinab Rafiee, Bahar Asheghi, Ahmad Gholami, Mohmed Isaqali Karobari
PLOS One.2025; 20(6): e0325430. CrossRef - Investigation of Discoloration of Anterior Teeth With Three Types of Substances Used in Endodontic Treatment
Sahar Soltani, Eshagh Ali Saberi, Nazanin Shahradnia, Pedram Abdollahzade Sangrodi, Elham Majidi
Clinical and Experimental Dental Research.2025;[Epub] CrossRef - A New Disinfection Approach Using a Chitosan-Based Endodontic Irrigant
Alejandra Itzel Lopez-Flores, Ulises Velazquez-Enriquez, Rogelio Jose Scougall-Vilchis, Laura Susana Acosta-Torres, Laura Emma Rodriguez-Vilchis, Rosalía Contreras-Bulnes, Paloma Netzayeli Serrano-Diaz, Rene Garcia-Contreras
Materials.2025; 18(24): 5552. CrossRef - Spectrophotometric Analysis of Intracoronal Bleaching on Crown Discoloration Induced by Various Antibiotic Pastes: An In Vitro Study
Avneet Kaur, Dileep Soni, Poorva R Sharma
International Journal of Clinical Pediatric Dentistry.2025; 18(12): 1443. CrossRef - Effect of Calcium Hydroxide Versus Double Antibiotic Paste on Endodontic Treatment Outcomes in Teeth With Large Periapical Lesions: A Triple‐Blind Randomized Clinical Trial
Afsaneh Rahmati, Farshad Seyedein, Omid Dianat, Sara Saedi, Golriz Rostami, Alireza Akbarzadeh Baghban, Shima Sabertahan, Majid Kazem, Kee Y. Kum
International Journal of Dentistry.2024;[Epub] CrossRef - The effect of different intracanal irrigants on the push-out bond strength of dentin in damaged anterior primary teeth
Leila Bassir, Shirin Taravati, Farzad Nouri, Saeide Rahimi
Journal of Medicine and Life.2024; 17(5): 536. CrossRef - In Vıtro Evaluatıon of Dıscoloratıon Caused by Root Canal Sealers and Color Changes after Bleachıng
Emre Bodrumlu, Esma Dinger
Annals of Dental Specialty.2024; 12(1): 77. CrossRef - Assessment of Discoloration Induced by Root Canal Sealers and Color Alterations Post-Bleaching
T.P. Van der Burgt, T.P. Mullaney, A.J.M. Plasschaert
International Journal of Dental Research and Allied Sciences.2024; 4(1): 1. CrossRef - The effect of four different intracanal medicaments on the push-out bond strength of root canal sealers
Shalu Maan, Vijaya Dhar Bhatt, Rohit Singh, Sayak Gupta, Syed Alay Noorain, Aashna Gill, Pradeep Kumar, Sushil Yadav, Preeti Sharma
Journal of Medicine and Life.2022; 15(4): 448. CrossRef - Effect of hydrogel-based antibiotic intracanal medicaments on crown discoloration
Rayan B. Yaghmoor, Jeffrey A. Platt, Kenneth J. Spolnik, Tien Min Gabriel Chu, Ghaeth H. Yassen
Restorative Dentistry & Endodontics.2021;[Epub] CrossRef
 ePub Link
ePub Link Cite
CiteDiscoloration of teeth due to different intracanal medicaments

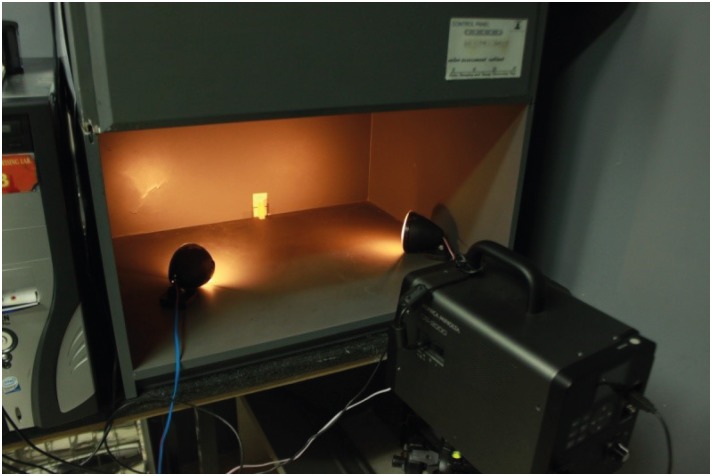
Figure 1 Specimen mounted in acrylic block.
Figure 2 Positioning of the specimen, light source, and spectrophotometer.
Figure 1
Figure 2
Discoloration of teeth due to different intracanal medicaments
Medicaments in the experimental and control groups
| Group | Material | Composition | Manufacturer |
|---|---|---|---|
| Control (n = 10) | Normal saline | 0.9% sodium chloride | Shahid Ghazi Pharmaceutical Co., Tabriz, Iran |
| CH (n = 20) | Calcium hydroxide | Calcium hydroxide–iodoform | Metapex; Meta Biomed Co., Cheongju, Korea |
| CH/CHX (n = 20) | Calcium hydroxide paste and chlorhexidine gel | Calcium hydroxide was mixed with 2% chlorhexidine gel at a proportion of 1:1 | Metapex; Meta Biomed Co., Cheongju, Korea |
| Gluco-Chex 2% gel; PPH Cerkamed, StalowaWola, Poland | |||
| 3Mix (n = 20) | Ciprofloxacin | Equal portions of metronidazole, ciprofloxacin, and minocycline mixed with distilled water (at a powder/liquid ratio of 3:1) | Bayer, Leverkusen, Germany |
| Metronidazole | Braun, Melsungen, Germany | ||
| Minocycline | Ratiopharm, Ulm, Germany |
Mean ΔE* values ± standard deviation of tooth samples from the different groups and at different time points
| Group (subgroup) | 1 week | 1 month | 3 months |
|---|---|---|---|
| CH (B) | 1.8 ± 0.33aA | 1.6 ± 0.30aA | 2.1 ± 0.34aA |
| CH (A) | 1.9 ± 0.36aA | 2.4 ± 0.54aA | 2.3 ± 0.89aA |
| CH/CHX (B) | 1.8 ± 0.33aA | 2.6 ± 0.68aA | 3.2 ± 0.63aA |
| CH/CHX (A) | 1.4 ± 0.22aA | 1.9 ± 0.43aA | 1.8 ± 0.33aA |
| 3Mix (B) | 5.0 ± 1.40bA | 6.0 ± 1.40bA | 12.0 ± 2.90bA |
| 3Mix (A) | 3.1 ± 0.97aA | 2.5 ± 0.83aA | 5.3 ± 1.50aA |
| Control | 3.9 ± 0.65aA | 5.0 ± 0.72aA | 3.4 ± 0.63aA |
The same uppercase letters in a row and the lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Mean ΔL* values ± standard deviation of tooth samples from the different groups and at different time points
| Group (subgroup) | 1 week | 1 month | 3 months |
|---|---|---|---|
| CH (B) | −0.29 ± 0.50aA | 0.79 ± 0.25aA | −1.50 ± 0.35aA |
| CH (A) | 0.23 ± 0.36aA | 0.98 ± 0.42aA | 0.09 ± 0.52aA |
| CH/CHX (B) | −0.024 ± 0.27aA | 1.20 ± 0.58aA | −1.70 ± 0.65aB |
| CH/CHX (A) | −0.05 ± 0.36aA | 0.78 ± 0.51aA | −0.83 ± 0.50aA |
| 3Mix (B) | −0.81 ± 1.70aA | −3.40 ± 1.70bA | −8.90 ± 2.60bB |
| 3Mix (A) | −0.42 ± 1.20aA | −0.24 ± 1.00aA | −3.50 ± 1.60aA |
| Control | 3.30 ± 0.64aA | 4.50 ± 0.61aA | 1.50 ± 0.60aA |
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Mean Δa* values ± standard deviation of tooth samples from the different groups and at different time points
| Group (subgroup) | 1 week | 1 month | 3 months |
|---|---|---|---|
| CH (B) | −0.21 ± 0.16aA | 0.35 ± 0.09aB | 0.20 ± 0.12aA |
| CH (A) | −0.55 ± 0.19aA | 0.15 ± 0.19aA | −0.05 ± 0.32aA |
| CH/CHX (B) | −0.46 ± 0.08aA | 0.24 ± 0.16aB | 0.12 ± 0.21aA |
| CH/CHX (A) | −0.47 ± 0.09aA | 0.56 ± 0.35aB | 0.35 ± 0.09aB |
| 3Mix (B) | −1.10 ± 0.09bA | −0.031 ± 0.37aA | −0.32 ± 0.45aA |
| 3Mix (A) | −0.52 ± 0.22aA | −0.14 ± 0.26aA | −0.26 ± 0.42aA |
| Control | −0.20 ± 0.09aA | 0.43 ± 0.23aB | 0.71 ± 0.23aB |
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Mean Δb* values ± standard deviation of tooth samples from the different groups at different time points
| Group (subgroup) | 1 week | 1 month | 3 months |
|---|---|---|---|
| CH (B) | −0.21 ± 0.16aA | 0.35 ± 0.09aA | 0.20 ± 0.12aA |
| CH (A) | −0.55 ± 0.19aA | 0.15 ± 0.19aA | −0.05 ± 0.32aA |
| CH/CHX (B) | −0.46 ± 0.08aA | 0.24 ± 0.16aA | 0.12 ± 0.21aA |
| CH/CHX (A) | −0.47 ± 0.09aA | 0.56 ± 0.35aA | 0.35 ± 0.09aA |
| 3Mix (B) | −1.10 ± 0.09aA | −0.03 ± 0.37aA | −0.32 ± 0.45bA |
| 3Mix (A) | −0.52 ± 0.22aA | −0.14 ± 0.26aA | −0.26 ± 0.42aA |
| Control | −0.20 ± 0.09aA | 0.43 ± 0.23aA | 0.71 ± 0.23aA |
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Table 1 Medicaments in the experimental and control groups
Table 2 Mean ΔE* values ± standard deviation of tooth samples from the different groups and at different time points
The same uppercase letters in a row and the lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Table 3 Mean ΔL* values ± standard deviation of tooth samples from the different groups and at different time points
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Table 4 Mean Δa* values ± standard deviation of tooth samples from the different groups and at different time points
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.
Table 5 Mean Δb* values ± standard deviation of tooth samples from the different groups at different time points
The same uppercase letters in a row and the same lowercase letters in a column indicate statistically similar groups (α = 0.05).
CH, alcium hydroxide; CHX, hlorhexidine; 3Mix, triple antibiotic paste (metronidazole, ciprofloxacin, and minocycline); A, subgroup in which medicaments were filled only into the canal (below the cementoenamel junction); B, subgroup in which the canals were completely filled with the materials, and a cotton pellet was dipped in the medicaments and placed in the pulp chamber.

