
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 43(4); 2018 > Article
- Research Article Improved dentin disinfection by combining different-geometry rotary nickel-titanium files in preparing root canals
-
Marwa M. Bedier1
 , Ahmed Abdel Rahman Hashem2, Yosra M. Hassan3
, Ahmed Abdel Rahman Hashem2, Yosra M. Hassan3 -
Restor Dent Endod 2018;43(4):e46.
DOI: https://doi.org/10.5395/rde.2018.43.e46
Published online: November 1, 2018
1Department of Endodontics, Faculty of Dentistry, Cairo University, Cairo, Egypt.
2Department of Endodontics, Faculty of Dentistry, Ain Shams University, Cairo, Egypt.
3Department of Clinical Pathology, Cairo University, Cairo, Egypt.
- Correspondence to Marwa M. Bedier BDS, MSc, MD. Lecturer, Department of Endodontics, Faculty of Dentistry, Cairo University, 12 El Saraya Street, Manial ElRoda, 11451 Cairo, Egypt. m.bedier81@gmail.com
• Received: June 19, 2018 • Accepted: September 11, 2018
Copyright © 2018. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,462 Views
- 14 Download
- 15 Crossref
Abstract
-
Objectives This study was to evaluate the antibacterial effect of different instrumentation and irrigation techniques using confocal laser scanning microscopy (CLSM) after root canal inoculation with Enterococcus faecalis (E. faecalis).
-
Materials and Methods Mesiobuccal and mesiolingual canals of extracted mandibular molars were apically enlarged up to a size 25 hand K-file, then autoclaved and inoculated with E. faecalis. The samples were randomly divided into 4 main groups according to the system of instrumentation and irrigation: an XP-endo Shaper (XPS) combined with conventional irrigation (XPS/C) or an XP-endo Finisher (XPF) (XPS/XPF), and iRaCe combined with conventional irrigation (iRaCe/C) or combined with an XPF (iRaCe/XPF). A middle-third sample was taken from each group, and then the bacterial reduction was evaluated using CLSM at a depth of 50 µm inside the dentinal tubules. The ratio of red fluorescence (dead cells) to green-and-red fluorescence (live and dead cells) represented the percentage of bacterial reduction. The data were then statistically analyzed using the Kruskal-Wallis test for comparisons across the groups and the Dunn test was used for pairwise comparisons.
-
Results The instrumentation and irrigation techniques had a significant effect on bacterial reduction (p < 0.05). The iRaCe/XPF group showed the strongest effect, followed by the XPS/XPF and XPS/C group, while the iRaCe/C group had the weakest effect.
-
Conclusions Combining iRaCe with XPF improved its bacterial reduction effect, while combining XPS with XPF did not yield a significant improvement in its ability to reduce bacteria at a depth of 50 µm in the dentinal tubules.
INTRODUCTION
The success of endodontic treatment depends on elimination of the inflamed pulp tissue from the pulp space, prevention of the microbial challenge to the surrounding periodontal structures, and provision of a suitable environment for periapical healing [1,2]. The eradication of bacteria from the root canal is difficult to achieve due to the anatomical complexities of root canal systems [3], which favor the presence of bacteria and the retention of residual infected tissues [4,5] and hinder root canal disinfection.
Enterococcus faecalis (E. faecalis) was observed in 38% of failed root canal treatments [6], while Pinheiro et al. [7] reported its presence in 52.94% of infected canals. This microorganism can invade the dentinal tubules, form biofilms, and survive in an environment with scarce nutrients, hindering its complete elimination by chemo-mechanical instrumentation and intracanal medication [6,8].
Several attempts have been made to develop rotary nickel-titanium (NiTi) instruments with advanced designs, different cross-sections, and variable tapers to provide more efficient systems for reaching the root canal dentinal walls [9,10]. Recently, a new approach for root canal shaping and cleaning has emerged, using a shape-memory NiTi instrument to improve root canal shaping and disinfection.
The XP-endo Shaper (XPS, FKG Dentaire, La Chaux-de-Fonds, Switzerland), a snake-shaped rotary NiTi file manufactured by NiTi MaxWire (Martensite-Austenite Electropolish-FleX), has been introduced. The XPS has an initial 0.01 taper in its martensite phase, but upon exposure to body temperature, the taper changes to 0.04 according to the molecular memory of the austenite phase, achieving final canal preparation with a size of 30 and a taper of 0.04 when used alone [11]. It has been claimed that XPS applies minimal stress on the dentin walls, thereby minimizing the risk of micro-crack formation in dentin and enabling it to easily adapt to canal irregularities with excellent resistance to cyclic fatigue [11,12,13,14,15].
Moreover, the XP-endo Finisher (XPF, FKG Dentaire), a new non-tapered NiTi instrument made of MaxWire. which gives the instrument its high flexibility, helps to remove packed debris from the complex anatomy of the root canal system. It can be used as an adjunctive approach to improve the effectiveness of irrigation in endodontics through agitation of the irrigant for root canal disinfection [13,16,17,18].
Several techniques have been introduced to evaluate the root canal flora. Histological sections show the distribution of bacteria in the infected dentin, but do not give any information about their viability; in addition, the field of analysis that is possible using scanning electron microscopy is very small due to its high magnification [19,20]. Recently, confocal laser scanning microscopy (CLSM) has been used to evaluate bacterial viability, as the use of fluorescence dye enables live and dead bacteria to be distinguished inside the dentinal tubules according to cytoplasmic membrane permeability [21,22].
CLSM has the ability to penetrate deep into the specimen and capture a series of image scans, meaning that it is a more accurate and convenient approach for evaluating bacterial viability than the bacterial culturing method [23], Therefore, the aim of this study was to quantitatively assess the effect of XPS combined with conventional irrigation (XPS/C) or XPF (XPS/XPF) on bacterial reduction in the dentinal tubules of the root canal after inoculation with E. faecalis by using CLSM. Additionally, the reduction of E. faecalis following root canal preparation using a conventional austenitic NiTi instrument, iRaCe (reamer with alternating cutting edges; FKG Dentaire), with conventional irrigation (iRaCe/C) or combined with an XPF (iRaCe/XPF) was evaluated. The null hypothesis was that there would be a no statistically significant difference in the removal of E. faecalis between the use of an XPS/C or with an XPF and the use of iRaCe/C or with an XPF.
MATERIALS AND METHODS
The sample size calculation was based on the results of Azim et al. [24], utilizing the percentage reduction of bacteria as the primary outcome. The effect size for the differences among the 4 groups was found to be (0.66), using an alpha (α) level of (5%) and a beta (β) level of (20%) (i.e., a power of 80%); the minimum estimated sample size was 8 samples per group for a total of 32 samples. The sample size calculation was performed using G*Power version 3.1.9.2 (Heinrich-Heine-University Düsseldorf, Düsseldorf, Germany).
The present study was performed following the guidelines of the institutional review board of the Faculty of Dentistry, Cairo University. Intact recently-extracted mandibular molars due to prosthodontic or periodontal disease with fully-formed apices were collected from the clinic of the Department of Oral and Maxillofacial Surgery.
All the teeth were examined to exclude those with previous root canal treatment, root caries, fractures, and root resorption. Preoperative radiographs in the buccolingual and mesiodistal directions were taken to ensure that no calcification was present. Forty teeth with mild root curvature (15°–20°) in both the mesiodistal and buccolingual directions [25] and a tooth length of 20 ± 1 mm was chosen and included in the study. The teeth were then immersed in 5.25% NaOCl for 30 minutes to remove the soft tissue.
All the crowns were flattened with a diamond disc at a level of 18 mm to obtain a reproducible flat reference point. The access cavity was prepared with a diamond round bur followed by an Endo-Z bur (Endo-Z bur, Dentsply, Tulsa Dental, Dentsply Maillefer, Tulsa, OK, USA), and canal patency was then checked by placing a size 15 K-file (Mani, Tochigi, Japan) into each canal until it was visible at the apical foramen. Canals that did not allow the placement of a size 15 K-file into the apex or those wider than a size 20 K-file at the apex were excluded.
The teeth were vertically split into mesial and distal roots using a water-cooled low-speed diamond disc (Eastwind Diamond Abrasives, Windsor, Canada). The mesiobuccal and mesiolingual canals were apically enlarged up to a size 25 hand K-file, and then each specimen was autoclaved in a single-glass tube containing phosphate-buffered saline (PBS) at 121°C for 20 minutes.
E. faecalis was grown aerobically from frozen stock cultures (ATCC 29212) in brain heart infusion (BHI) broth (BHI broth, OXOID, Basingstoke, Hants, England) at 37°C. A standard suspension (1 × 108 cells/mL) was prepared from cultures grown for 18 to 20 hours. Cells were harvested by centrifugation and resuspended in fresh BHI broth. An E. faecalis suspension was placed in each root to the orifice level, using a sterile 1-mL insulin syringe with a 30-gauge needle inside a laminar flow hood (Thermo Fisher Scientific Inc, Waltham, MA, USA). Each sample was then placed into a 15-mL sterile Falcon tube containing 10 mL of BHI broth and incubated at 37°C for 21 days in 100% humidity to allow colonization of the bacteria on the canal wall and into the dentinal tubules. The growth medium was replenished every 2 days to ensure the culture viability [26], and after the final replenishment of the medium, a sample was streaked onto BHI agar and incubated for 18 hours to confirm the purity of the culture.
The root canals were disinfected using the 4 different root canal preparation/irrigation methods described below (n = 10).
Group (XPS/C): An XPS was placed in an X Smart Plus Motor (Dentsply Maillefer, Ballaigues, Switzerland), and rotated at a speed of 800 rpm and a torque of 1 Ncm with a gentle and slow in-and-out motion until reaching the full working length. During instrumentation, the root canals were irrigated with 5 mL of 2.6% NaOCl using a 30-gauge side-vented needle (NaviTip, Ultradent South Jordan, UT, USA) that was placed within 2 mm of the working length. At the end of the preparation, 3 mL of 17% ethylenediaminetetraacetic acid (EDTA) was used for 1 minute to remove the smear layer, followed by 10 mL of distilled water as a final flush.
Group (XPS/XPF): Root canal preparation was done using an XPS file, and the root canals were irrigated with 5 mL of 2.6% NaOCl. The XPF file was cooled by spraying ENDO Frost (RSA, Colten, Whaledent GmBH, Langenau, Germany) through the plastic tube and then inserted through the entire working length of the root canal, operated at 800 rpm and 1 Ncm of torque for 1 minute with a slow and gentle vertical motion of 7–8 mm. Thereafter, 3 mL of EDTA was used for 1 minute followed by 10 mL of distilled water as a final flush.
Group (iRaCe/C): Root canal preparation was done using iRaCe at 600 rpm and 1.5 Ncm according to the manufacturer's instructions. Sizes 15/0.06, 25/0.04, and 30/0.04 were used for the entire working length. Two milliliters of freshly prepared 2.6% NaOCl was used after each rotary instrument. Two milliliters of freshly prepared 2.6% NaOCl was used after each rotary file, using a 30-gauge needle NaviTip at 2 mm short of the working length, and then finally 3 mL of 17% EDTA was used, followed by 10 mL of distilled water.
Group (iRaCe/XPF): Root canal preparation was performed following the protocol used for the iRaCe/C group described above. Between the use of each instrument, the root canals were irrigated with 2 mL of 2.6% NaOCl. Then, an XPF file was applied according to the manufacturer's instruction. Thereafter, 3 mL of EDTA was used for 1 minute, followed by 10 mL of distilled water as a final flush.
After root canal preparation and disinfection, the roots were sectioned horizontally under constant irrigation with sterile saline, a middle-third sample measuring 2 × 2 × 4 mm in thickness was obtained, and the sample was then stained using the Syto-9/propidium iodide technique (Live/Dead, Backlight; Invitrogen, Eugene, OR, USA). The working solution was prepared by adding 1 μL of each dye to 1 mL of distilled water to improve the contrast between the biofilm cells and dentin, and then 200 μL was added to the dentin samples and incubated in a dark environment for 20 minutes at room temperature.
Samples were gently washed in PBS for 1 minute, and then immediately mounted on a cover slip for examination under CLSM (Figure 1). The excitation/emission wavelengths were set at 480/500 nm for Syto-9 and 490/635 nm for propidium iodide to inspect the tooth samples. Four confocal images of random areas were obtained for each specimen using a using a ×40 oil lens and a step size of 1 µm. CLSM images were acquired by the Zen V. 2 software (Carl Zeiss Ltd., Jena, Germany) at a resolution of 1,024 × 1,024 pixels. For each image, the intensity of the red (dead bacteria) and the green fluorescence (live bacteria) at a depth of 50 µm was measured and the percentage of the dead bacteria was calculated.
The ratio of the red fluorescence (dead cells) to the green-and-red fluorescence (live and dead cells) indicated the percentage of the bacterial reduction. Data were statistically analyzed using SPSS version 20 (IBM Corp., Armonk, NY, USA). The Kolmogorov-Smirnov and Shapiro-Wilk tests were used to explore the normality of the data by checking the distribution. The data showed a non-parametric distribution; the Kruskal-Wallis test was therefore used to make comparisons across groups, and the Dunn test was used for pairwise comparisons. The significance level was set at p ≤ 0.05.
RESULTS
The percentages of E. faecalis reduction in the dentinal tubules at a depth of 50 µm and the statistical analysis of all groups are summarized in Table 1 and presented in Figures 2 and 3. The Kruskal-Wallis test showed statistically significant differences among the different groups (p = 0.001, p < 0.05). The XPS/XPF group showed no statistically significant difference in bacterial reduction compared to the XPS/C group. However, the iRaCe/XPF group showed a significantly greater bacterial reduction than the iRaCe/C group, and statistically significant differences were found in the percentage of bacterial reduction between the XPS/C and iRaCe/C, XPS/C and iRaCe/XPF, XPS/XPF and iRaCe/C, and XPS/XPF and iRaCe/XPF groups (p < 0.05). The greatest bacterial reduction was found in the iRaCe/XPF group (62.91% ± 16.96%), followed by the XPS/XPF group (45.17% ± 10.25%), the XPS/C group (33.28% ± 17.01%), and finally the iRaCe/C group (11.81% ± 5.13%).
Table 1
The mean and standard deviation (SD) values of the percentage of bacterial reduction after root canal preparation and disinfection in the groups
Different superscripts in the same column indicate statistically significant differences.
CI, confidence interval; XPS/C, XP-endo Shaper combined with conventional irrigation; XPS/XPF, XP-endo Shaper combined with XP-endo Finisher; iRaCe/C, iRaCe combined with conventional irrigation; iRaCe/XPF, iRaCe combined with an XP-endo Finisher.
*Significant at p ≤ 0.05.
Figure 2
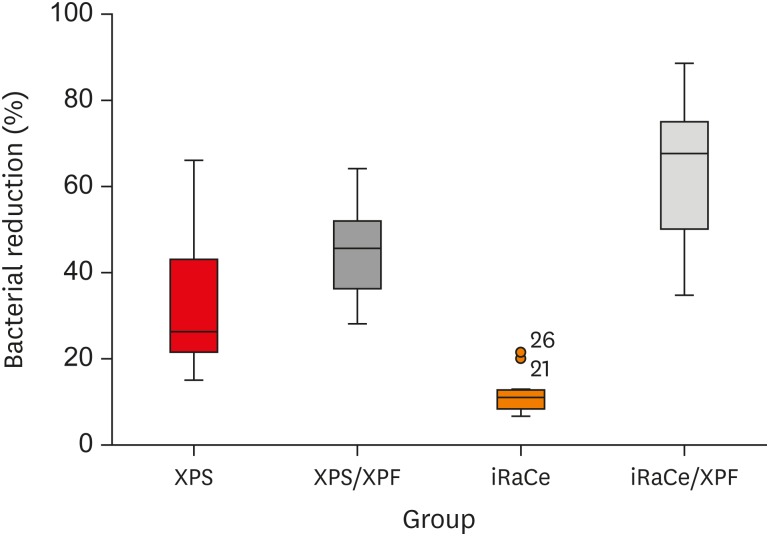
Box and whisker plot representing the percentage of bacterial reduction in the 4 groups (circles represent outliers).
XPS, XP-endo Shaper; XPS/XPF, XP-endo Shaper combined with an XP-endo Finisher, iRaCe/XPF, iRaCe combined with an XP-endo Finisher.
Figure 3

Confocal laser scanning microscopy (CLSM) images after root canal preparation and disinfection in the (A) XP-endo Shaper combined with conventional irrigation (XPS/C), (B) XP-endo Shaper combined with an XP-endo Finisher (XPS/XPF), (C) iRaCe combined with conventional irrigation (iRaCe/C), and (D) iRaCe combined with an XP-endo Finisher (iRaCe/XPF) groups at a depth of 50 µm in the dentinal tubules. The red color denotes dead bacteria, while the green color denotes living bacteria.
DISCUSSION
The primary aim of endodontic treatment is the eradication of bacteria and their byproducts from the root canal system, followed by 3-dimensional sealing of the root canals [27]. The removal of bacteria from the root canal is difficult to achieve due to biofilm formation on the dentin walls [28]; thus, the field of modern clinical microbiology is attempting to develop new strategies capable of eliminating the bacterial biofilm [29].
It has been reported that in a bacterial invasion model, bacteria penetrated into dentinal tubules up to 500 µm from the main root canal [30], and the time needed for biofilm formation may range from 15 minutes to 60 days [26,31]. E. faecalis has been used for its role in persistent endodontic infections because of its high virulence and its ability to form a resistant biofilm [31,32], and samples were incubated for 21 days to ensure bacterial colonization of the dentinal tubules [21,33]. The roots were then sectioned horizontally, and a middle-third sample measuring 2 × 2 mm in thickness was used to evaluate the amount of live and dead bacteria at a depth of 50 µm inside the dentinal tubules, as the middle third showed greater dentinal tubule invasion by bacteria than was observed in the apical region. In addition, the apical third of the canal has fewer dentinal tubules, more peritubular dentin, and a high possibility of sclerotic dentin formation [33,34,35].
The results of this study showed that XPS/C was superior to iRace/C in bacterial reduction, which is consistent with the results of Paqué et al. [36], who reported limited cleanliness of the root canal when using RaCe and ProTaper rotary NiTi instruments, and agrees with the findings of Azim et al. [37], who reported that XPS left fewer untouched walls (38.6%) than Vortex Blue (58.8%), and the results of Lacerda et al. [38], who reported that the proportion of untouched areas in the full canal length after preparation with SAF, TRUShape, and XPS was 10.92%, 17.45%, and 17.31%, respectively, with no significant difference.
This result may be attributed to the difference in the alloy used for manufacturing the files; the iRaCe is manufactured from a conventional austenitic NiTi alloy with an electropolished surface [39], while the innovative XPS with the MaxWire Technology allows the file to change from its M-phase at room temperature to the A-phase. This enables it to expand from its original size to adapt to the canal morphology and to enlarge the canal to at least size 30/0.04, as well as provides it with a greater ability to contact and clean areas that are difficult to reach with regular instrumentation techniques [40].
The use of XPF for irrigant agitation after the use of iRaCe improved its bacterial reduction; this is supported by the findings of Alves et al. [41], who found that XPF yielded improvements in bacterial reduction when used after chemomechanical preparation. Likewise, Azim et al. [24] reported that XPF was efficient for disinfecting the main canal space up to 50 µm deep into the dentinal tubules, and Bao et al. [17] found improvements in biofilm removal from the root canal system when XPF was used for irrigant agitation, and this finding supported by the superior ability of XPF to remove the smear layer and to reduce hard tissue debris [18,42,43].
This property of XPF may be related to its special manufacturing process from a proprietary alloy with a shape-memory based design, allowing this single file with a size 25 diameter and zero taper to change from the M-phase to the A-phase within the root canal during the rotation mode. Its unique spoon shape, with a length of 10 mm from the tip and a depth of 1.5 mm, allows the file to expand to 6 mm in diameter, or 100-fold compared to an equivalent-sized file, which enables the file to adapt to the canal, to clean canal irregularities, and to detach biofilm [13]. Thus, the null hypothesis was rejected.
The XPS/XPF group showed no statistically significant difference in bacterial reduction from the XPS/C group, which may be attributed to the similarity of the technique of manufacturing of both files from NiTi MaxWire (Martensite-Austenite Electropolish-FleX), with its unique molecular memory that allows the file to expand when inserted in the canal at body temperature, which enables it to adapt to canal walls and to reach areas that conventional instruments cannot access [13]. Thus, the null hypothesis was accepted.
CONCLUSIONS
In conclusion, within the limitations of this study, XPF improved the effectiveness of iRaCe for bacterial reduction up to a depth of 50 µm in the dentinal tubules, whereas combining XPS with XPF did not show any significant difference compared to XPS alone.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Bedier MM.
Data curation: Hashem AR.
Formal analysis: Hashem AR.
Methodology: Bedier MM, Hassan YM.
Project administration: Bedier MM.
Supervision: Hashem AR.
Validation: Hashem AR, Bedier MM.
Visualization: Bedier MM.
Writing - original draft: Bedier MM, Hassan YM.
Writing - review & editing: Hashem AR.
- 1. Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997;30:297-306.ArticlePubMed
- 2. Siqueira JF Jr, Lima KC, Magalhães FA, Lopes HP, de Uzeda M. Mechanical reduction of the bacterial population in the root canal by three instrumentation techniques. J Endod 1999;25:332-335.ArticlePubMed
- 3. Schäfer E, Zapke K. A comparative scanning electron microscopic investigation of the efficacy of manual and automated instrumentation of root canals. J Endod 2000;26:660-664.ArticlePubMed
- 4. Paqué F, Ganahl D, Peters OA. Effects of root canal preparation on apical geometry assessed by micro-computed tomography. J Endod 2009;35:1056-1059.ArticlePubMed
- 5. Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod 2010;36:703-707.ArticlePubMed
- 6. Sundqvist G, Figdor D, Persson S, Sjögren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:86-93.ArticlePubMed
- 7. Pinheiro ET, Gomes BP, Ferraz CC, Sousa EL, Teixeira FB, Souza-Filho FJ. Microorganisms from canals of root-filled teeth with periapical lesions. Int Endod J 2003;36:1-11.ArticlePubMedPDF
- 8. Ørstavik D, Haapasalo M. Disinfection by endodontic irrigants and dressings of experimentally infected dentinal tubules. Endod Dent Traumatol 1990;6:142-149.ArticlePubMed
- 9. Peters OA, Arias A, Paqué F. A micro-computed tomographic assessment of root canal preparation with a novel instrument, TRUShape, in mesial roots of mandibular molars. J Endod 2015;41:1545-1550.ArticlePubMed
- 10. Versiani MA, Pécora JD, de Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37:1002-1007.ArticlePubMed
- 11. Bayram HM, Bayram E, Ocak M, Uygun AD, Celik HH. Effect of ProTaper Gold, self-adjusting File, and XP-endo Shaper instruments on dentinal microcrack formation: a micro-computed tomographic study. J Endod 2017;43:1166-1169.ArticlePubMed
- 12. Elnaghy AM, Elsaka SE. Torsional resistance of XP-endo Shaper at body temperature compared with several nickel-titanium rotary instruments. Int Endod J 2018;51:572-576.ArticlePubMedPDF
- 13. FKG Dentaire SA. The XP-endo Finisher file brochure [Internet]. La Chaux-de-Fonds: FKG Dentaire SA; c2014. updated 2018 Oct 29]. cited 2018 Aug 5]. Available from: https://www.fkg.ch/products/endodontics/canal-shaping-and-cleaning/xp-endo-finisher.
- 14. Silva EJ, Vieira VT, Belladonna FG, Zuolo AS, Antunes HD, Cavalcante DM, Elias CN, De-Deus G. Cyclic and torsional fatigue resistance of XP-endo Shaper and TRUShape instruments. J Endod 2018;44:168-172.ArticlePubMed
- 15. Elnaghy A, Elsaka S. Cyclic fatigue resistance of XP-endo Shaper compared with different nickel-titanium alloy instruments. Clin Oral Investig 2018;22:1433-1437.ArticlePubMedPDF
- 16. Trope M, Debelian G. XP-3D Finisher™ file—the next step in restorative endodontics. Endod Pract US 2015;8:22-24.
- 17. Bao P, Shen Y, Lin J, Haapasalo M. In vitro efficacy of XP-endo Finisher with 2 different protocols on biofilm removal from apical root canals. J Endod 2017;43:321-325.ArticlePubMed
- 18. Leoni GB, Versiani MA, Silva-Sousa YT, Bruniera JF, Pécora JD, Sousa-Neto MD. Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int Endod J 2017;50:398-406.ArticlePubMedPDF
- 19. Ozdemir HO, Buzoglu HD, Calt S, Stabholz A, Steinberg D. Effect of ethylenediaminetetraacetic acid and sodium hypochlorite irrigation on Enterococcus faecalis biofilm colonization in young and old human root canal dentin: in vitro study. J Endod 2010;36:842-846.ArticlePubMed
- 20. Wong DT, Cheung GS. Extension of bactericidal effect of sodium hypochlorite into dentinal tubules. J Endod 2014;40:825-829.ArticlePubMed
- 21. Shen Y, Qian W, Chung C, Olsen I, Haapasalo M. Evaluation of the effect of two chlorhexidine preparations on biofilm bacteria in vitro: a three-dimensional quantitative analysis. J Endod 2009;35:981-985.ArticlePubMed
- 22. Ordinola-Zapata R, Bramante CM, de Moraes IG, Bernardineli N, Porto CV, Campanelli AP, Garcia RB, Duarte MH. The use of confocal laser scanning microscopy for the study of dentin infection. In: Mendez-Vilas A, Diaz J, editors. Microscopy: science, technology, applications and education. Badajoz: Formatex; 2010. p. 583-589.
- 23. Silva EJ, Belladonna FG, Zuolo AS, Rodrigues E, Ehrhardt IC, Souza EM, De-Deus G. Effectiveness of XP-endo Finisher and XP-endo Finisher R in removing root filling remnants: a micro-CT study. Int Endod J 2018;51:86-91.ArticlePubMedPDF
- 24. Azim AA, Aksel H, Zhuang T, Mashtare T, Babu JP, Huang GT. Efficacy of 4 irrigation protocols in killing bacteria colonized in dentinal tubules examined by a novel confocal laser scanning microscope analysis. J Endod 2016;42:928-934.ArticlePubMedPMC
- 25. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971;32:271-275.ArticlePubMed
- 26. George S, Kishen A, Song KP. The role of environmental changes on monospecies biofilm formation on root canal wall by Enterococcus faecalis . J Endod 2005;31:867-872.ArticlePubMed
- 27. Siqueira JF Jr. Endodontic infections: concepts, paradigms, and perspectives. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:281-293.ArticlePubMed
- 28. Nakamura VC, Candeiro GT, Cai S, Gavini G. Ex vivo evaluation of three instrumentation techniques on E. faecalis biofilm within oval shaped root canals. Braz Oral Res 2015;29:1-7.Article
- 29. Stewart PS. New ways to stop biofilm infections. Lancet 2003;361:97.Article
- 30. Haapasalo M, Orstavik D. In vitro infection and disinfection of dentinal tubules. J Dent Res 1987;66:1375-1379.ArticlePubMedPDF
- 31. Nair PN, Henry S, Cano V, Vera J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after “one-visit” endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:231-252.ArticlePubMed
- 32. Spratt DA, Pratten J, Wilson M, Gulabivala K. An in vitro evaluation of the antimicrobial efficacy of irrigants on biofilms of root canal isolates. Int Endod J 2001;34:300-307.ArticlePubMedPDF
- 33. Ma J, Wang Z, Shen Y, Haapasalo M. A new noninvasive model to study the effectiveness of dentin disinfection by using confocal laser scanning microscopy. J Endod 2011;37:1380-1385.ArticlePubMed
- 34. Love RM. Regional variation in root dentinal tubule infection by Streptococcus gordonii . J Endod 1996;22:290-293.ArticlePubMed
- 35. Carrigan PJ, Morse DR, Furst ML, Sinai IH. A scanning electron microscopic evaluation of human dentinal tubules according to age and location. J Endod 1984;10:359-363.ArticlePubMed
- 36. Paqué F, Musch U, Hülsmann M. Comparison of root canal preparation using RaCe and ProTaper rotary Ni-Ti instruments. Int Endod J 2005;38:8-16.ArticlePubMed
- 37. Azim AA, Piasecki L, da Silva Neto UX, Cruz AT, Azim KA. XP Shaper, a novel adaptive core rotary instrument: micro-computed tomographic analysis of its shaping abilities. J Endod 2017;43:1532-1538.ArticlePubMed
- 38. Lacerda MF, Marceliano-Alves MF, Pérez AR, Provenzano JC, Neves MA, Pires FR, Gonçalves LS, Rôças IN, Siqueira JF Jr. Cleaning and shaping oval canals with 3 instrumentation systems: a correlative microcomputed tomographic and histoligical study. J Endod 2017;43:1878-1884.PubMed
- 39. Zupanc J, Vahdat-Pajouh N, Schäfer E. New thermomechanically treated NiTi alloys - a review. Int Endod J 2018;51:1088-1103.ArticlePubMedPDF
- 40. FKG Dentaire SA. FKG XP-endo Shaper brochure [Internet]. La Chaux-de-Fonds: FKG Dentaire SA; c2014. updated 2018 Oct 29]. cited 2018 Aug 5]. Available from: https://www.fkg.ch/sites/default/files/201704_fkg_xp_endo_shaper_brochure_v4_fr_web.pdf.
- 41. Alves FR, Andrade-Junior CV, Marceliano-Alves MF, Pérez AR, Rôças IN, Versiani MA, Sousa-Neto MD, Provenzano JC, Siqueira JF Jr. Adjunctive steps for disinfection of the mandibular molar root canal system: a correlative bacteriologic, micro-computed tomography, and cryopulverization approach. J Endod 2016;42:1667-1672.ArticlePubMed
- 42. Elnaghy AM, Mandorah A, Elsaka SE. Effectiveness of XP-endo Finisher, EndoActivator, and File agitation on debris and smear layer removal in curved root canals: a comparative study. Odontology 2017;105:178-183.ArticlePubMedPDF
- 43. Sanabria-Liviac D, Moldauer BI, Garcia-Godoy F, Antonio-Campos A, Casaretto M, Torres-Navarro J, Scalercio JM. Comparison of the XP-Endo Finisher file system and passive ultrasonic irrigation (PUI) on smear layer removal after root canal instrumentation. J Dent Oral Health 2017;4:1-7.
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Evaluation of bacterial reduction by contemporary irrigation activation methods against Enterococcus faecalis biofilm in root canals
Tuğçe Özdemir Sakin, Fatoş Albayrak, Tutku Tunç
Scientific Reports.2026;[Epub] CrossRef - Biofilm-forming activity of Enterococcus faecalis on basic materials of removable dental prosthetic bases
Oksana A. Shuliatnikova, Mikhail V. Yakovlev, Anatoliy P. Godovalov
HERALD of North-Western State Medical University named after I.I. Mechnikov.2025; 17(2): 89. CrossRef - A Short Report on the Effectiveness of Edge Taper Platinum and XP-3D Shaper for the Reduction of Enterococcus faecalis Count in the Root Canal System: An Ex Vivo Study
Hanie Moaveni, Parastou Ghahari, Samira Behrad, Majid Mirmohammadkhani, Sobhan Rashmee, Somayeh Teimoori
Avicenna Journal of Dental Research.2024; 16(2): 77. CrossRef - Shaping ability of non‐adaptive and adaptive core nickel–titanium single‐file systems with supplementary file in ribbon‐shaped canals analysed by micro‐computed tomography
Parichat Chinchiyanont, Kallaya Yanpiset, Danuchit Banomyong, Nathamon Thongbai‐On
Australian Endodontic Journal.2023; 49(1): 38. CrossRef - Impact XP-endo finisher on the 1-year follow-up success of posterior root canal treatments: a randomized clinical trial
Ludmila Smith de Jesus Oliveira, Fabricio Eneas Diniz de Figueiredo, Janaina Araújo Dantas, Maria Amália Gonzaga Ribeiro, Carlos Estrela, Manoel Damião Sousa-Neto, André Luis Faria-e-Silva
Clinical Oral Investigations.2023; 27(12): 7595. CrossRef - In vitro reduction in Enterococcus faecalis count following root canal preparation with Neolix and XP shaper rotary files
Mina Mehrjouei, Somayeh Teimoori, Majid Mirmohammadkhani, Seyed Majed Mortazavi, Maryam Khorasanchi
Saudi Endodontic Journal.2023; 13(3): 236. CrossRef - Antibacterial efficacy of sodium hypochlorite versus apple cider vinegar against Enterococcus faecalis in contracted endodontic cavity
Kaur Supreet, Karkala Venkappa Kishan, Nimisha Chinmay Shah
Endodontology.2022; 34(4): 254. CrossRef - Ex vivo evaluation of the effectiveness of XP-endo Finisher on the removal of smear layer from the root canal
Sângela Maria PEREIRA, Ceci Nunes CARVALHO, Rudys Rodolfo TAVAREZ, Paulo NELSON-FILHO, Léa Assed Bezerra DA SILVA, Etevaldo Matos MAIA FILHO
RGO - Revista Gaúcha de Odontologia.2022;[Epub] CrossRef - Biofilm elimination from infected root canals using four different single files
Sarah A. Hamed, Sarah Shabayek, Hayam Y. Hassan
BMC Oral Health.2022;[Epub] CrossRef - The effectiveness of the supplementary use of the XP-endo Finisher on bacteria content reduction: a systematic review and meta-analysis
Ludmila Smith de Jesus Oliveira, Rafaella Mariana Fontes de Bragança, Rafael Sarkis-Onofre, André Luis Faria-e-Silva
Restorative Dentistry & Endodontics.2021;[Epub] CrossRef - Combination of a new ultrasonic tip with rotary systems for the preparation of flattened root canals
Karina Ines Medina Carita Tavares, Jáder Camilo Pinto, Airton Oliveira Santos-Junior, Fernanda Ferrari Esteves Torres, Juliane Maria Guerreiro-Tanomaru, Mario Tanomaru-Filho
Restorative Dentistry & Endodontics.2021;[Epub] CrossRef - Effect of Adaptive, Rotary, and Manual Root Canal Instrumentation in Primary Molars: A Triple-Armed, Randomized Controlled Clinical Trial
Bhaggyashri A. Pawar, Ajinkya M. Pawar, Anuj Bhardwaj, Dian Agustin Wahjuningrum, Amelia Kristanti Rahardjo, Alexander Maniangat Luke, Zvi Metzger, Anda Kfir
Biology.2021; 10(1): 42. CrossRef - Complete Obturation—Cold Lateral Condensation vs. Thermoplastic Techniques: A Systematic Review of Micro-CT Studies
Shilpa Bhandi, Mohammed Mashyakhy, Abdulaziz S. Abumelha, Mazen F. Alkahtany, Mohamed Jamal, Hitesh Chohan, A. Thirumal Raj, Luca Testarelli, Rodolfo Reda, Shankargouda Patil
Materials.2021; 14(14): 4013. CrossRef - The Effects of Different Endodontic Access Cavity Design and Using XP-endo Finisher on the Reduction of Enterococcus faecalis in the Root Canal System
Pelin Tüfenkçi, Koray Yılmaz
Journal of Endodontics.2020; 46(3): 419. CrossRef - Irrigation in Endodontics: a Review
Sarah Bukhari, Alaa Babaeer
Current Oral Health Reports.2019; 6(4): 367. CrossRef
 ePub Link
ePub Link Cite
CiteImproved dentin disinfection by combining different-geometry rotary nickel-titanium files in preparing root canals
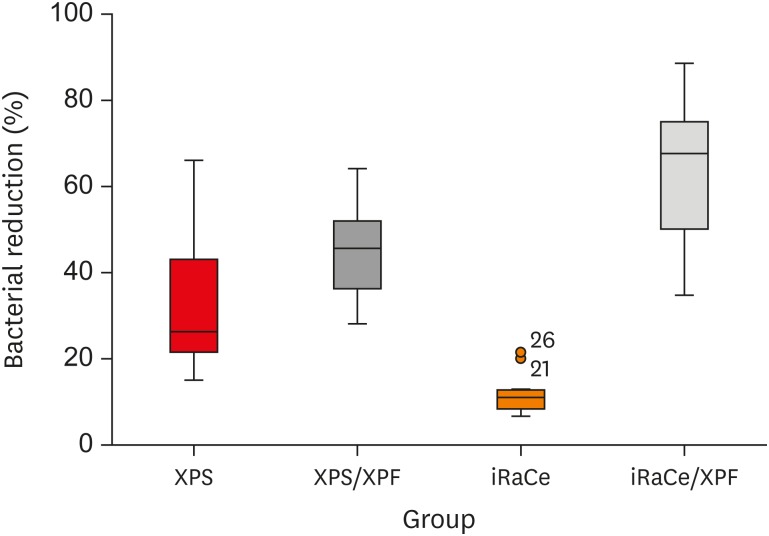
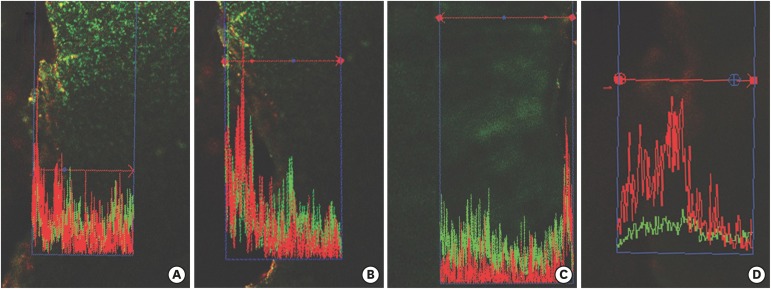
Figure 1 A Zeiss LSM 710 confocal laser scanning microscope.
Figure 2 Box and whisker plot representing the percentage of bacterial reduction in the 4 groups (circles represent outliers).XPS, XP-endo Shaper; XPS/XPF, XP-endo Shaper combined with an XP-endo Finisher, iRaCe/XPF, iRaCe combined with an XP-endo Finisher.
Figure 3 Confocal laser scanning microscopy (CLSM) images after root canal preparation and disinfection in the (A) XP-endo Shaper combined with conventional irrigation (XPS/C), (B) XP-endo Shaper combined with an XP-endo Finisher (XPS/XPF), (C) iRaCe combined with conventional irrigation (iRaCe/C), and (D) iRaCe combined with an XP-endo Finisher (iRaCe/XPF) groups at a depth of 50 µm in the dentinal tubules. The red color denotes dead bacteria, while the green color denotes living bacteria.
Figure 1
Figure 2
Figure 3
Improved dentin disinfection by combining different-geometry rotary nickel-titanium files in preparing root canals
The mean and standard deviation (SD) values of the percentage of bacterial reduction after root canal preparation and disinfection in the groups
| Group | Mean | SD | Median | Minimum | Maximum | 95% CI | p value | |
|---|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | |||||||
| XPS/C | 33.28B | 17.01 | 26.25 | 15.00 | 66.00 | 21.11 | 45.45 | < 0.001* |
| XPS/XPF | 45.17B | 10.25 | 45.58 | 28.00 | 64.08 | 37.83 | 52.50 | |
| IRaCe/C | 11.81C | 5.13 | 10.96 | 6.60 | 21.43 | 8.14 | 15.48 | |
| iRaCe/XPF | 62.91A | 16.96 | 67.58 | 34.78 | 88.57 | 50.78 | 75.04 | |
Different superscripts in the same column indicate statistically significant differences.
CI, confidence interval; XPS/C, XP-endo Shaper combined with conventional irrigation; XPS/XPF, XP-endo Shaper combined with XP-endo Finisher; iRaCe/C, iRaCe combined with conventional irrigation; iRaCe/XPF, iRaCe combined with an XP-endo Finisher.
*Significant at p ≤ 0.05.
Table 1 The mean and standard deviation (SD) values of the percentage of bacterial reduction after root canal preparation and disinfection in the groups
Different superscripts in the same column indicate statistically significant differences.
CI, confidence interval; XPS/C, XP-endo Shaper combined with conventional irrigation; XPS/XPF, XP-endo Shaper combined with XP-endo Finisher; iRaCe/C, iRaCe combined with conventional irrigation; iRaCe/XPF, iRaCe combined with an XP-endo Finisher.
*Significant at

