
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 43(1); 2018 > Article
- Research Article Influence of size and insertion depth of irrigation needle on debris extrusion and sealer penetration
-
Emel Uzunoglu-Özyürek1
 , Hakan Karaaslan1, Sevinç Aktemur Türker2, Bahar Özçelik1
, Hakan Karaaslan1, Sevinç Aktemur Türker2, Bahar Özçelik1 -
Restor Dent Endod 2017;43(1):e2.
DOI: https://doi.org/10.5395/rde.2018.43.e2
Published online: December 22, 2017
1Department of Endodontics, Hacettepe University Faculty of Dentistry, Ankara, Turkey.
2Department of Endodontics, Bülent Ecevit University Faculty of Dentistry, Zonguldak, Turkey.
- Correspondence to Emel Uzunoglu-Özyürek, DDS, PhD. Research Assistant, Department of Endodontics, Hacettepe University Faculty of Dentistry, Sihhiye, Ankara 06100, Turkey. emel_dt@hotmail.com
• Received: September 23, 2017 • Accepted: November 8, 2017
Copyright © 2018. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,589 Views
- 25 Download
- 10 Crossref
Abstract
-
Objectives To determine the effect of size and insertion depth of irrigation needle on the amount of apical extruded debris and the amount of penetration depth of sealer using a confocal laser scanning microscope (CLSM).
-
Materials and Methods Twenty maxillary premolars were assigned to 2 groups (n = 10), according to the size of needle tip, 28 G or 30 G. Buccal roots of samples were irrigated with respective needle type inserted 1 mm short of the working length (WL), while palatal roots were irrigated with respective needle type inserted 3 mm short of the WL. Prepared teeth were removed from the pre-weighed Eppendorf tubes. Canals were filled with F3 gutta-percha cone and rhodamine B dye-labeled AH 26 sealer. Teeth were transversally sectioned at 1 and 3 mm levels from the apex and observed under a CLSM. Eppendorf tubes were incubated to evaporate the irrigant and were weighed again. The difference between pre- and post-weights was calculated, and statistical evaluation was performed.
-
Results Inserting needles closer to the apex and using needles with wider diameters were associated with significantly more debris extrusion (p < 0.05). The position of needles and level of sections had statistically significant effects on sealer penetration depth (p < 0.05 for both).
-
Conclusions Following preparation, inserting narrower needles compatible with the final apical diameter of the prepared root canal at 3 mm short of WL during final irrigation might prevent debris extrusion and improve sealer penetration in the apical third.
INTRODUCTION
Root canal irrigation has an essential role in endodontic treatment aiming to remove any pulpal remnants and microorganisms within the root canal system adjunct to instrumentation [1]. In recent years, its perceived importance has grown considerably [2,3], in view of the finding that a significant part of the root canal wall is left untouched by contemporary instrumentation techniques [4,5]. The effectiveness of the irrigating solution during chemo-mechanical preparation relies on many variables, such as the root canal anatomy, the delivery system, volume, flow and the type of the irrigant [6,7,8]. In addition to preparing the root canal chemo-mechanically, hermetic 3-dimensional filling of the root canal with the core material and root canal sealer is also considered a key factor in successful endodontic therapy [9]. During filling of the root canal, penetration of root canal sealer into the dentinal tubule is necessary because it increases the connection between the core material and dentine, thereby helping to optimize the adaptability and sealing capability of the root canal filling [10,11].
Several different commercial irrigant delivery systems have been developed for improving the cleanliness of root canal as well as penetrability of sealers into the dentinal tubules [8,12,13,14]. However, there are controversial results regarding the efficiency of these devices compared to a syringe and a needle (SN); which still remains the most commonly used method, with the solution being injected under positive pressure into the depths of the root canal [15,16]. Various factors, which affect success of SN in removing debris and bacteria from root canal, such as volume of irrigation, the type, size, and insertion depth of the irrigation needle were investigated [2,17,18,19,20,21,22,23]. Syringe delivery of the irrigant allows control of the depth of needle penetration in the canal and the volume of irrigant flushed through the canal [22]. Positioning the needle close to the working length (WL) has been advocated to effectively clean the apical part of the root canal with SN [6,17,23,24]; because the irrigant seldom flows beyond 1-mm of the tip of the needle [17,25]. On the other hand, this might increase the possibility of irrigant extrusion to the periapical area [26,27,28,29]. According to the authors' knowledge there is no current study that evaluates the effect of needle size and insertion depth simultaneously on sealer penetration in apical third and apically extruded debris. Therefore, the aim of this study was to determine the effect of: 1) the size and 2) the insertion depth of the needle on the amount of apically extruded debris and penetration depth of resin-based sealer in apical third of root canal. The null hypothesis tested was that there would be no differences in the amount of apical extrusion of debris and penetration depth of resin-based sealer in the apical third of the root canal, with respective of the size, or the insertion depth of used needle.
MATERIALS AND METHODS
After the approval of Non-interventional Clinical Researches Ethics Board of Hacettepe University (Approval number: GO17/251), 20 freshly extracted, human permanent maxillary first premolar teeth with fully formed 2 roots and 2 canals were included in this study. Curvatures of roots were ranged between 0° and 5°. Teeth with caries, cracks, fractures, resorptions, open apexes, and previous root canal treatment were excluded. The specimens were collected from patients aged 18–40 years.
Following access cavity preparation, the WL was determined using a size 10 K-file until it was visible at the apical foramen and was recorded as the length 1 mm short of this length. Specimens were adjusted into the apparatus as previously described [30] to collect extruded debris. Stoppers were separated from the Eppendorf tubes. An analytical balance (Radwag, Radom, Poland) with an accuracy of 10−4 g was used to measure the initial weight of the tubes. Three consecutive weights were obtained for each tube, and the mean value was calculated. A hole was created on each stopper. Each tooth was inserted up to the cementoenamel junction, and a 27-gauge needle (Ultradent, South Jordan, UT, USA) was placed alongside the stopper. This acted as a drainage cannula and helped to balance the air pressure inside and outside the tubes. Then, each stopper with the tooth and the needle was attached to its Eppendorf tube, and the tubes were fitted into vials with cyanoacrylate (Figure 1A). A rubber-dam sheet was used to prevent leakage of overflowing irrigant and also shielded the root apex from operator during the instrumentation procedure.
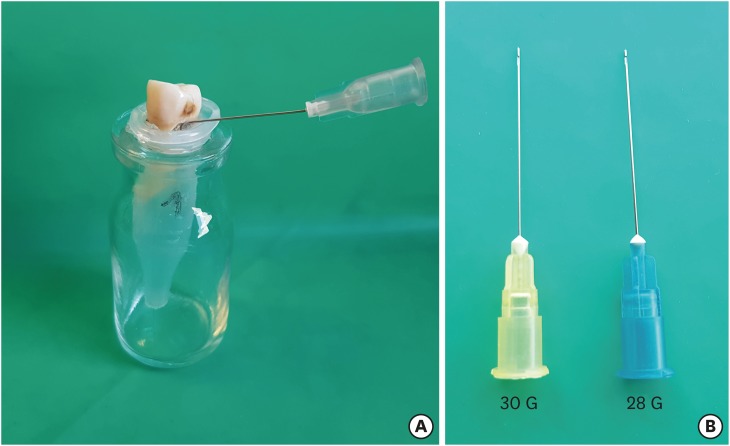
Samples were randomly divided into 2 groups (n = 10) according to the needles that were used during irrigation as follows: 28 G (0.36 × 25 mm) and 30 G (0.30 × 25 mm) (Steri Irrigation Tips, Diadent, Cheongju, Korea). During the final irrigation, the side-vented, closed-ended needles (Figure 1B) were positioned 1 mm short of the WL in buccal (B) canals of both groups and 3 mm short of the WL in palatal (P) canals. Each canal was prepared separately and the debris extruded from B or P root was collected in different tubes (total n = 40). B canal orifices were sealed with composite material (Dentonics Chemical Composite, Dentonics, Monroe, NC, USA) while instrumenting the P canal or vice versa. All of the canals were prepared using ProTaper Universal rotary files (Dentsply Maillefer, Ballaigues, Switzerland) up to F3 [21]. Root canals were irrigated with 2 mL of 2.5% sodium hypochlorite (NaOCl) after each file. In the early stage of preparation, irrigation was made at the farthest possible length, but needle depth was maintained according to the study criteria, especially 3 mm short of the WL was always maintained in P canals. Totally, 12 mL of 2.5% NaOCl was used per root canal. Following preparation, the specimens were removed from their tubes and irrigated using 3 mL of 17% ethylenediaminetetraacetic acid (EDTA) for 1 minute for smear layer removal. Final irrigation was done with 3 mL of 2.5% NaOCl and 3 mL of saline, respectively. During irrigation, needles were avoided from binding into the root canal walls and irrigation was done at a constant speed of 0.26 mL/s to avoid pushing material into the periapex as previous studies [31,32]. Vials were stored at 37°C for 21 days for to evaporate NaOCl. After the incubation period, the tubes were weighed again for 3 times. The average of these measurements was considered to be the weight of the tube plus the debris.
The specimens were detached from the plastic vials and obturated using single cone technique with F3 gutta-percha (Dentsply Sirona Endodontics, Tulsa, OK, USA) and AH 26 root canal sealer (Dentsply Sirona Endodontics) mixed with 0.1% Rhodamin-B (Sigma-Aldrich, Darmstadt, Germany). Composite material (Dentonics Chemical Composite, Dentonics) was used to restore the access cavities. The specimens were then stored at 37°C in 100% humidity for 1 week, for the sealer to set. At the end of the week, the specimens were embedded into resin blocks and then sectioned at 1 mm and 3 mm levels from the apex with an Isomet precision saw (IsoMet Low Speed Precision Cutter, Buehler, Lake Bluff, IL, USA). These sections were photographed under confocal laser scanning microscope (CLSM Pascal, Carl Zeiss, Oberkochen, Germany) and the images were analysed in CLSM Image Browser (Carl Zeiss) to measure the sealer penetration depth and percentage into the dentinal tubules [13,14]. The percentage of penetrated sealer was calculated as follows: amount of sealer penetrated in the canal perimeter (green line in Figure 2) divided by the total canal perimeter (white line in Figure 2) × 100 (%). The longest penetration depth of sealer was also measured as microns (yellow line in Figure 2) via CLSM Image Browser.
Figure 2
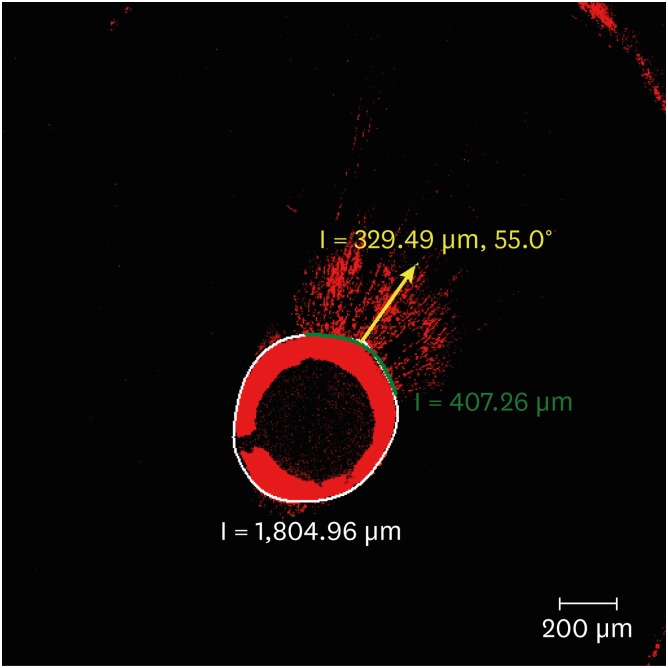
Calculation of the amount of penetrated sealer into the dentinal tubules using a formula as follows: amount of sealer penetrated in the canal perimeter (green line) divided by the total canal perimeter (white line) × 100 (%). The longest penetration depth of sealer was also measured as microns (yellow line) via confocal laser scanning microscope (CLSM) image browser.
The difference between pre- and post-weights of the tubes were calculated, and the statistical evaluation was performed using SPSS version 22 (IBM Corporation, Armonk, NY, USA). Normality distribution of data was determined by Shapiro-Wilk test. The weight measurements of apically extruded debris were compared using 2-way analysis of variance (ANOVA) and sealer penetration depths were compared using repeated measures ANOVA with Bonferroni post hoc test (p = 0.05). Sealer penetration percentages were not distributed normally and were compared with Kruskal-Wallis and Wilcoxon signed rank sum tests (p = 0.05).
RESULTS
Table 1 shows the amount of extruded debris for each group. A 28 G needle was related to more extrusion than a 30 G needle (p < 0.001) for both insertion depths. Positioning the needle at 1 mm short of WL led to a larger volume of extruded debris than at 3 mm short of WL (p < 0.001) for both needle diameters.
Table 1
The amount of extruded debris for each group of 28 G and 30 G needles according to the needle insertion depths of 1 mm and 3 mm short of working length (WL)
| Group | 28 G | 30 G |
|---|---|---|
| 1 mm short of WL (buccal roots) | 0.1090 ± 0.0268a | 0.0665 ± 0.0251c |
| 3 mm short of WL (palatal roots) | 0.0708 ± 0.0244b | 0.0296 ± 0.0138d |
The values are means and standard deviations (n = 10). In the group 1 mm short of WL, needles were inserted into buccal roots; in the group 3 mm short of WL, needles were inserted into palatal roots.
Different superscript letters mean statistical significant difference for each rows and columns (p < 0.001).
Figure 3 shows the depth of sealer penetration measured at different levels of needle insertion depth within each experimental group with different needle diameter. Diameter of needle did not affect the sealer penetration depth statistically (p > 0.05). Position of needle and level of sections had statistically significant effects on sealer penetration depth (p < 0.05 for needle position; p < 0.001 for section level). Depth of penetrated sealer was always statistically higher at 3 mm level compared to 1 mm level at both needle positions and sizes (p < 0.001). Positioning a 30 G needle at 1 mm short of WL resulted in statistically lower sealer penetration depth than positioning the 30 G needle at 3 mm short of WL at 3 mm level (p < 0.001). Figure 4 shows an overview of representative CLSM images from each experimental group at 1 mm and 3 mm levels of sections.
Figure 3
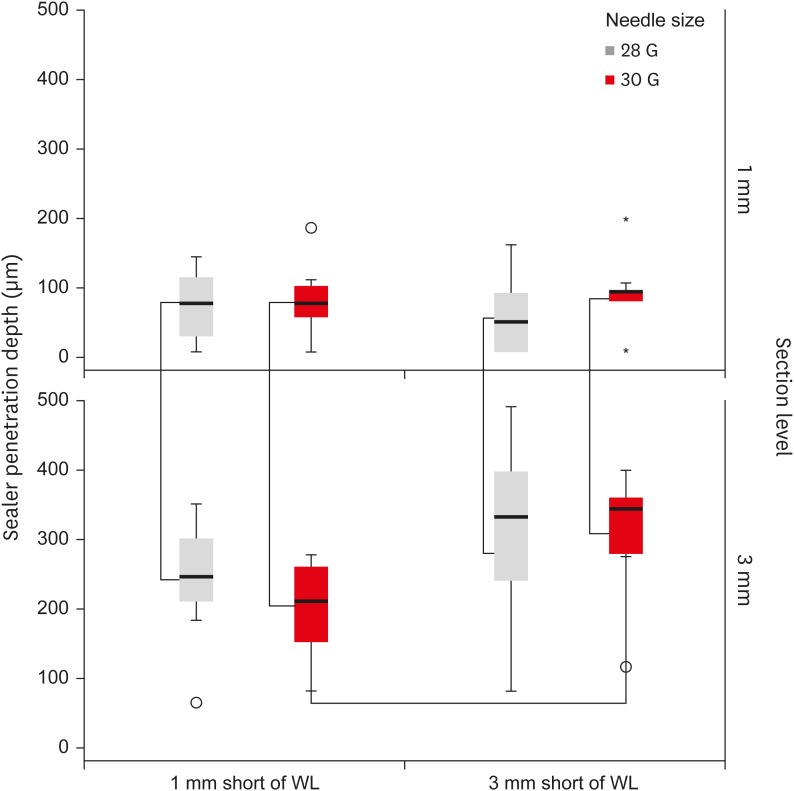
Depth of sealer penetration (µm) measured at different levels of needle insertion within each experimental group. In each box plot, the median value (line inside the box), the interquartile range (IQR; length of the box), and the minimum and maximum values (extreme lines) are reported. Values more than 1.5 IQRs but < 3 IQRs are labelled as outliers (o); values ≥ 3 IQRs are labelled as extreme cases (*). Brackets are connected between statistically different groups (p < 0.001).
WL, working length.
Figure 4
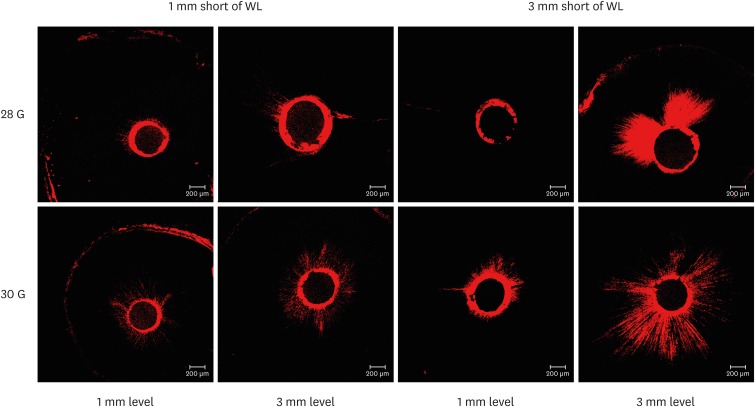
Representative confocal laser scanning microscope (CLSM) images from each experimental group at 1 mm and 3 mm levels.
WL, working length.
The percentage of sealer penetration into dentinal tubules was not significantly different (Kruskal-Wallis test, p > 0.05) among groups when the overall distribution of values was compared (Figure 5). Within each group, an increase in the percentage of sealer penetration was observed from 1 mm to 3 mm levels from the apex. Percentages of penetration measured at 1 mm level always appeared significantly lower than those recorded at 3 mm levels (Wilcoxon signed rank sum tests, p < 0.05), regardless of needle gauges and positions. Neither needle positions nor their sizes affected the penetration percentage of sealer (Wilcoxon signed rank sum tests, p > 0.05).
Figure 5
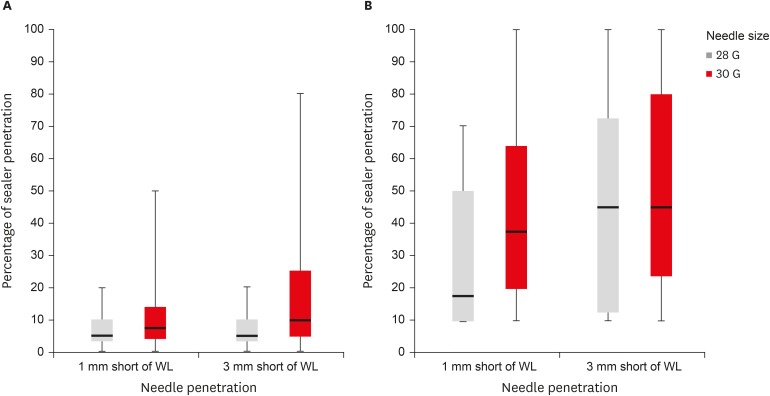
Percentage of sealer penetration measured at (A) 1 mm and (B) 3 mm levels from the apex within each experimental group. In each box plot, the median value (line inside the box), the interquartile range (IQR; length of the box), and the minimum and maximum values (extreme lines) are reported (Wilcoxon signed rank sum tests, p > 0.05).
WL, working length.
DISCUSSION
One of the limitations of in vitro studies is to obtain standardized tooth samples. The morphology, and age of tooth are the examples of some parameters that might affect the amount of extruded debris as well as the penetration depth of the sealer. It is difficult to standardize the amount and distribution of sclerotic dentine and irregular secondary dentine, which may have influence on the sealer penetration or smear layer patterns. Even a careful sample selection does not guarantee a homogeneous dentine pattern among the specimens. Because of these reasons maxillary premolar teeth with fully formed 2 separate roots were used to overcome this limitation. Needles were inserted 1 mm short of the WL in B roots, while it was inserted 3 mm short of the WL in P roots. According to authors' knowledge, this is the first study using maxillary premolar for the evaluation of debris extrusion. A previously described method was modified for debris collection [30]. No attempt was made to simulate the presence of vital pulp or periapical tissues. Current results could change in an in vivo model because of periapical tissues, which act as a natural barrier to prevent debris extrusion. Thus, the results should not be directly extrapolated to the clinical situation.
Root canal preparation was done up to F3 ProTaper rotary file (size 30/0.09) in the present study and the diameter of needles were 0.36 mm (28 G) and 0.30 mm (30 G). Previous studies reported that the minimum instrumentation size needed for penetration of irrigants to the apical third of the root canal is a size 30 file [17,21]. In the present study, NaOCl was used to simulate clinical conditions as previous extrusion studies [29,32]. However, it is also important to consider that using NaOCl in extrusion studies could cause to greater amount of debris because it is impossible to separate sodium crystals from debris [33]. NaOCl has been used as the irrigant of choice for cleaning root canals in endodontic therapy, because of its antimicrobial properties and tissue-dissolving capabilities [3]. When confined to the root canal system, these properties enable thorough disinfection. NaOCl extrusion during root canal treatment is commonly referred to as ‘the hypochlorite accident’; it causes acute immediate symptoms and potentially serious sequelae [34]. Syringe irrigation was employed in all the reported accidents in a recent systematic review [35]. However, this finding may be attributed to the wider use of SN compared to other irrigation methods and systems [16].
Different-sized needles (28 G and 30 G) were used at 1 mm and 3 mm short of the WL and sealer penetration was evaluated in the sections that were obtained 1 mm and 3 mm levels from the apex to represent apical third. Several studies reported that needle placement closer to the WL resulted in more efficient irrigant replacement and debridement [17,18,19,20,23,24,27]. Furthermore, Munoz and Camacho-Cuadra [25] showed that the irrigant only penetrated 0–1.1 mm deeper than the tip of the needle. For an effective cleaning, irrigation system is needed to penetrate deeply into the apical third [6,17,23,24], but at the same time it should not cause extrusion of irrigants beyond the apex [26,27,28,29]. The space available around the needle is important for the reverse flow of the irrigant towards the canal orifice [27]. For this purpose, it has been reported that needle should be positioned at 2 or 3 mm short of the WL [27,35]. Because of this dilemma, 2 different insertion depths were used in the present study. Needle size as well as needle insertion depth have a significant effect on apically extruded debris in the current study. Using 30 G needle caused less amount of apically extruded debris in both insertion depths compared to 28 G. Furthermore, inserting needle 3 mm short of the WL resulted in less extrusion with both sizes as previous studies [26,29], especially with 30 G needles.
A significant reduction in the volume of hard-tissue debris and more effective ex vivo removal of bioluminescent bacteria from root canals were observed when the needle tip was placed 1 mm short of the WL compared to 5 mm [20,23]. Improving cleanliness of apical third might enhance the depth of sealer penetration [8]. On the other hand, Mandorah [36] reported that no difference was found in the cleanliness of rotary prepared canals between placements of the irrigation needle tip at full or half WL. In the present study, insertion depth did not cause significant differences in sealer penetration depth and penetration percentage with 28 G needle. Vapor lock effect, which prevents the irrigant from effectively reaching the WL, could be one of the reasons for this result [37]. On the other hand, inserting 30 G needle at 3 mm short of the WL resulted in higher sealer penetration at 1 mm and 3 mm from the apex compared to 1 mm. It has been reported that gauge irrigation needles with narrower outer diameter (larger gauge number) than the diameter of the prepared canal was more effective than needles with wider outer diameter (smaller gauge number) for deeper penetration and consequently removing more smear layer from the apical part [6]. This could be the one explanation of the present data. Chow [17] reported that the type and size of needle used for endodontic irrigation of the root canal affect the degree of cleanliness in the apical third of the canal. However, in the present study, sealer penetration depths were not significantly different in needle sizes. This difference could be resulted from different needle sizes that were used in the studies. The needles of 28 G and 30 G were used in the present study, while 23 G and 25 G were used in the previous one [17].
In the present study, the results showed that in all experimental groups the sealer penetration depth and percentage of penetration were significantly greater at 3 mm from the apex than 1 mm as in previous studies [8,13,14]. The presence of sclerotic dentine [7], the small number of dentinal tubules relative to the cervical and middle thirds, and the difficulties in delivering irrigation solutions, as well as removing the smear layer from the apical third constitute possible reasons that could explain ascending levels of penetration depth of sealer from apical to coronal levels [10].
CONCLUSIONS
Both size and insertion depth of needles affected the amount of extruded debris as well as the amount of penetrated sealer into dentinal tubules. As a conclusion, inserting needles 3 mm short of WL for final irrigation, which have narrower diameters than final apical diameter of the prepared root canal, might prevent debris extrusion and improve sealer penetration at apical third.
ACKNOWLEDGEMENT
Authors are grateful to Sevilay Karahan for statistical assistance.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B.
Data curation: Uzunoglu-Özyürek E.
Formal analysis: Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B.
Funding acquisition: Uzunoglu-Özyürek E.
Investigation: Uzunoglu-Özyürek E, Karaaslan H, Türker SA.
Methodology: Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B.
Project administration: Uzunoglu-Özyürek E, Karaaslan H.
Resources: Karaaslan H, Türker SA.
Software: Uzunoglu-Özyürek E, Karaaslan H, Türker SA.
Supervision: Özçelik B; Validation: Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B.
Visualization: Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B.
Writing - original draft: Uzunoglu-Özyürek E.
Writing - review & editing: Karaaslan H, Türker SA, Özçelik B.
- 1. Haapasalo M, Endal U, Zandi H, Coil JM. Eradication of endodontic infection by instrumentation and irrigation solutions. Endod Topics 2005;10:77-102.Article
- 2. Gulabivala K, Patel B, Evans G, Ng YL. Effects of mechanical and chemical procedures on root canal surfaces. Endod Topics 2005;10:103-122.Article
- 3. Zehnder M. Root canal irrigants. J Endod 2006;32:389-398.ArticlePubMed
- 4. Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod 2010;36:703-707.ArticlePubMed
- 5. Paqué F, Zehnder M, De-Deus G. Microtomography-based comparison of reciprocating single-file F2 ProTaper technique versus rotary full sequence. J Endod 2011;37:1394-1397.ArticlePubMed
- 6. Abou-Rass M, Piccinino MV. The effectiveness of four clinical irrigation methods on the removal of root canal debris. Oral Surg Oral Med Oral Pathol 1982;54:323-328.ArticlePubMed
- 7. Carrigan PJ, Morse DR, Furst ML, Sinai IH. A scanning electron microscopic evaluation of human dentinal tubules according to age and location. J Endod 1984;10:359-363.ArticlePubMed
- 8. Gu Y, Perinpanayagam H, Kum DJ, Yoo YJ, Jeong JS, Lim SM, Chang SW, Baek SH, Zhu Q, Kum KY. Effect of different agitation techniques on the penetration of irrigant and sealer into dentinal tubules. Photomed Laser Surg 2017;35:71-77.ArticlePubMed
- 9. Ørstavik D. Endodontic filling materials. Endod Topics 2014;31:53-67.Article
- 10. Mamootil K, Messer HH. Penetration of dentinal tubules by endodontic sealer cements in extracted teeth and in vivo . Int Endod J 2007;40:873-881.ArticlePubMed
- 11. Sadr S, Golmoradizadeh A, Raoof M, Tabanfar MJ. Microleakage of single-cone gutta-percha obturation technique in combination with different types of sealers. Iran Endod J 2015;10:199-203.PubMedPMC
- 12. Bolles JA, He J, Svoboda KK, Schneiderman E, Glickman GN. Comparison of Vibringe, EndoActivator, and needle irrigation on sealer penetration in extracted human teeth. J Endod 2013;39:708-711.ArticlePubMed
- 13. Kara Tuncer A, Unal B. Comparison of sealer penetration using the EndoVac irrigation system and conventional needle root canal irrigation. J Endod 2014;40:613-617.ArticlePubMed
- 14. Generali L, Cavani F, Serena V, Pettenati C, Righi E, Bertoldi C. Effect of different irrigation systems on sealer penetration into dentinal tubules. J Endod 2017;43:652-656.ArticlePubMed
- 15. Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod 2004;30:559-567.ArticlePubMed
- 16. Dutner J, Mines P, Anderson A. Irrigation trends among American Association of Endodontists members: a web-based survey. J Endod 2012;38:37-40.ArticlePubMed
- 17. Chow TW. Mechanical effectiveness of root canal irrigation. J Endod 1983;9:475-479.ArticlePubMed
- 18. Usman N, Baumgartner JC, Marshall JG. Influence of instrument size on root canal debridement. J Endod 2004;30:110-112.ArticlePubMed
- 19. Falk KW, Sedgley CM. The influence of preparation size on the mechanical efficacy of root canal irrigation in vitro . J Endod 2005;31:742-745.ArticlePubMed
- 20. Sedgley CM, Nagel AC, Hall D, Applegate B. Influence of irrigant needle depth in removing bioluminescent bacteria inoculated into instrumented root canals using real-time imaging in vitro . Int Endod J 2005;38:97-104.ArticlePubMed
- 21. Khademi A, Yazdizadeh M, Feizianfard M. Determination of the minimum instrumentation size for penetration of irrigants to the apical third of root canal systems. J Endod 2006;32:417-420.ArticlePubMed
- 22. van der Sluis LW, Gambarini G, Wu MK, Wesselink PR. The influence of volume, type of irrigant and flushing method on removing artificially placed dentine debris from the apical root canal during passive ultrasonic irrigation. Int Endod J 2006;39:472-476.ArticlePubMed
- 23. Perez R, Neves AA, Belladonna FG, Silva EJ, Souza EM, Fidel S, Versiani MA, Lima I, Carvalho C, De-Deus G. Impact of needle insertion depth on the removal of hard-tissue debris. Int Endod J 2017;50:560-568.ArticlePubMedPDF
- 24. Boutsioukis C, Lambrianidis T, Kastrinakis E. Irrigant flow within a prepared root canal using various flow rates: a computational fluid dynamics study. Int Endod J 2009;42:144-155.ArticlePubMed
- 25. Munoz HR, Camacho-Cuadra K. In vivo efficacy of three different endodontic irrigation systems for irrigant delivery to working length of mesial canals of mandibular molars. J Endod 2012;38:445-448.ArticlePubMed
- 26. Aksel H, Askerbeyli S, Canbazoglu C, Serper A. Effect of needle insertion depth and apical diameter on irrigant extrusion in simulated immature permanent teeth. Braz Oral Res 2014;28:1-6.Article
- 27. Boutsioukis C, Lambrianidis T, Verhaagen B, Versluis M, Kastrinakis E, Wesselink PR, van der Sluis LW. The effect of needle-insertion depth on the irrigant flow in the root canal: evaluation using an unsteady computational fluid dynamics model. J Endod 2010;36:1664-1668.ArticlePubMed
- 28. Malentacca A, Uccioli U, Zangari D, Lajolo C, Fabiani C. Efficacy and safety of various active irrigation devices when used with either positive or negative pressure: an in vitro study. J Endod 2012;38:1622-1626.ArticlePubMed
- 29. Psimma Z, Boutsioukis C, Kastrinakis E, Vasiliadis L. Effect of needle insertion depth and root canal curvature on irrigant extrusion ex vivo. J Endod 2013;39:521-524.ArticlePubMed
- 30. Myers GL, Montgomery S. A comparison of weights of debris extruded apically by conventional filing and Canal Master techniques. J Endod 1991;17:275-279.ArticlePubMed
- 31. Boutsioukis C, Gogos C, Verhaagen B, Versluis M, Kastrinakis E, Van der Sluis LW. The effect of root canal taper on the irrigant flow: evaluation using an unsteady Computational Fluid Dynamics model. Int Endod J 2010;43:909-916.ArticlePubMed
- 32. Silva PB, Krolow AM, Pilownic KJ, Casarin RP, Lima RK, Leonardo RT, Pappen FG. Apical extrusion of debris and irrigants using different irrigation needles. Braz Dent J 2016;27:192-195.ArticlePubMed
- 33. Tanalp J, Güngör T. Apical extrusion of debris: a literature review of an inherent occurrence during root canal treatment. Int Endod J 2014;47:211-221.ArticlePubMed
- 34. Farook SA, Shah V, Lenouvel D, Sheikh O, Sadiq Z, Cascarini L, Webb R. Guidelines for management of sodium hypochlorite extrusion injuries. Br Dent J 2014;217:679-684.ArticlePubMedPDF
- 35. Boutsioukis C, Psimma Z, van der Sluis LW. Factors affecting irrigant extrusion during root canal irrigation: a systematic review. Int Endod J 2013;46:599-618.ArticlePubMed
- 36. Mandorah A. Effect of irrigation needle depth in smear layer removal: scanning electron microscope study. Saudi Endod J 2013;3:114-119.Article
- 37. Tay FR, Gu LS, Schoeffel GJ, Wimmer C, Susin L, Zhang K, Arun SN, Kim J, Looney SW, Pashley DH. Effect of vapor lock on root canal debridement by using a side-vented needle for positive-pressure irrigant delivery. J Endod 2010;36:745-750.ArticlePubMedPMC
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Effect of laser-induced pulpal anesthesia of single-rooted teeth with irreversible pulpitis treated by single-visit root canal therapy - A randomized clinical trial
Geeta Asthana, Dhwani Morakhia, Ravina Parmar, Rajashree Tamuli
Endodontology.2025; 37(3): 244. CrossRef - Efficacy of different irrigation needles used in endodontics: an in silico and an in vitro investigation
Maulee Sheth, Ankit Arora, Sonali Kapoor, Balraj Shukla
Biomaterial Investigations in Dentistry.2025; 12: 264. CrossRef - Preliminary insights: exploring irrigation practices during endodontic treatment among general dental practitioners in Malaysia
Kai Qi Chiew, Xin Ni Lim, Shekhar Bhatia, Naveen Chhabra
British Dental Journal.2024;[Epub] CrossRef - Efficiency of diode laser in control of post-endodontic pain: a randomized controlled trial
Hend H. Ismail, Maram Obeid, Ehab Hassanien
Clinical Oral Investigations.2023; 27(6): 2797. CrossRef - Endodontic management of an aberrant germinated composite odontome: A case report
Ankit Arora, Kavina Desai, Sonali Kapoor, Seema Gajera
Australian Endodontic Journal.2023; 49(3): 684. CrossRef - Potentials of 3D-Modeling in the Preclinical Stage of Root Needle Research
Aleksandr V. Kuligin, Larisa N. Kazakova, Oksana S. Tereshchuk, Vadim V. Bokov
I.P. Pavlov Russian Medical Biological Herald.2022; 30(1): 95. CrossRef - Effect of root canal geometry and needle type on apical extrusion of irrigant: an ex vivo study
Büşra SERÇE FİKİRLİ, Bülent ALTUNKAYNAK, Güven KAYAOĞLU
Acta Odontologica Turcica.2022; 39(3): 58. CrossRef - An in vitro radiological evaluation of irrigant penetration in the root canals using three different irrigation systems: Waterpik WP-100 device, passive irrigation, and manual dynamic irrigation systems
Suragani Hemalatha, Archana Srinivasan, A Srirekha, Lekha Santhosh, C Champa, Ashwija Shetty
Journal of Conservative Dentistry.2022; 25(4): 403. CrossRef - Preparation Ability of ProTaper Next and XP-endo Shaper Instruments in Isthmus-containing Root Canal System
Mustafa Sarıkahya, Tayfun Alaçam
Conservative Dentistry and Endodontic Journal.2021; 5(2): 28. CrossRef - Penetration depth of irrigants into root dentine after sonic, ultrasonic and photoacoustic activation
K. M. Galler, V. Grubmüller, R. Schlichting, M. Widbiller, A. Eidt, C. Schuller, M. Wölflick, K.‐A. Hiller, W. Buchalla
International Endodontic Journal.2019; 52(8): 1210. CrossRef
 ePub Link
ePub Link Cite
CiteInfluence of size and insertion depth of irrigation needle on debris extrusion and sealer penetration
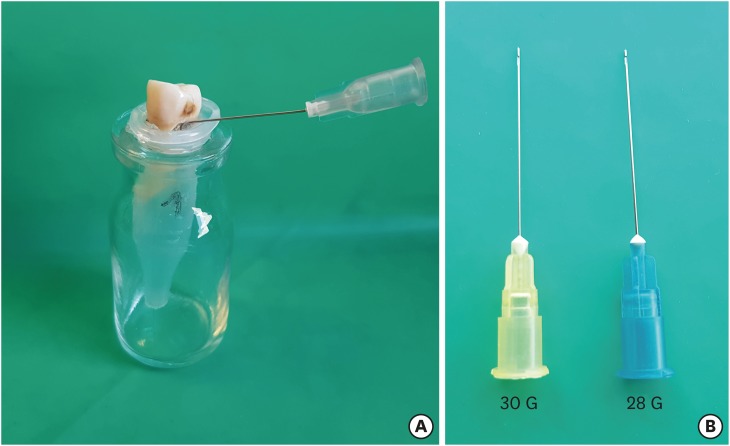
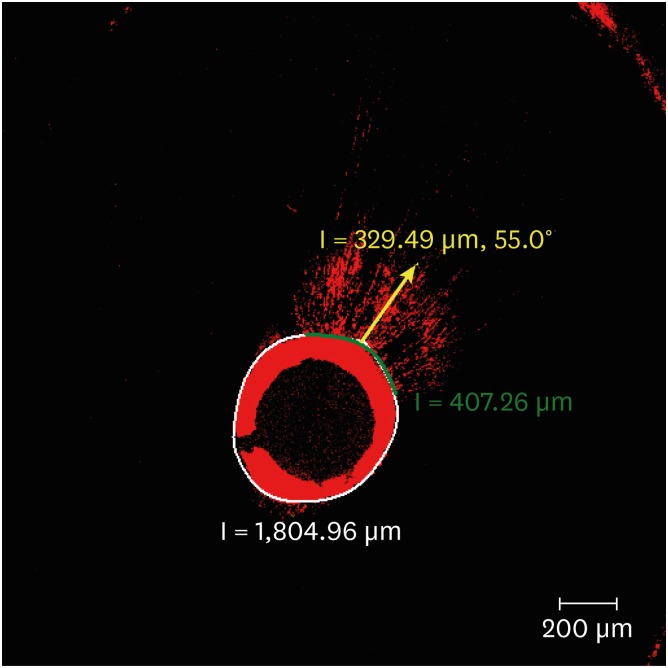
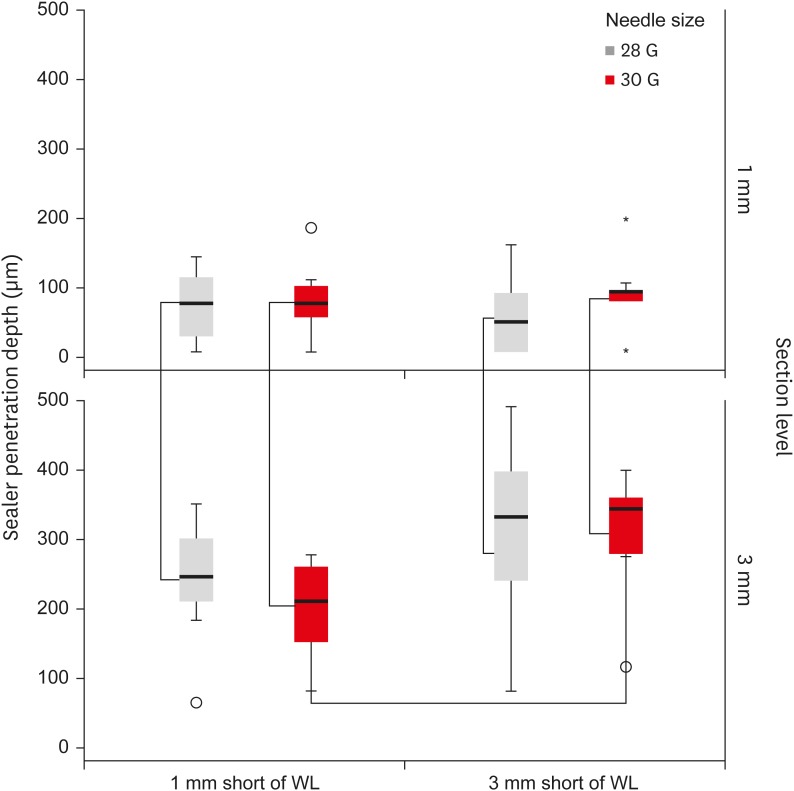
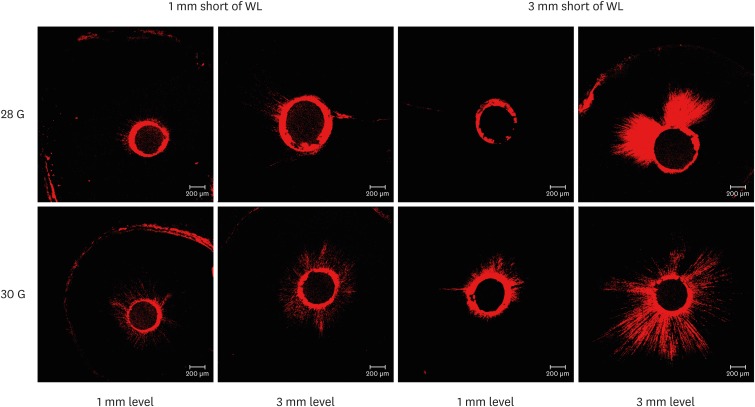
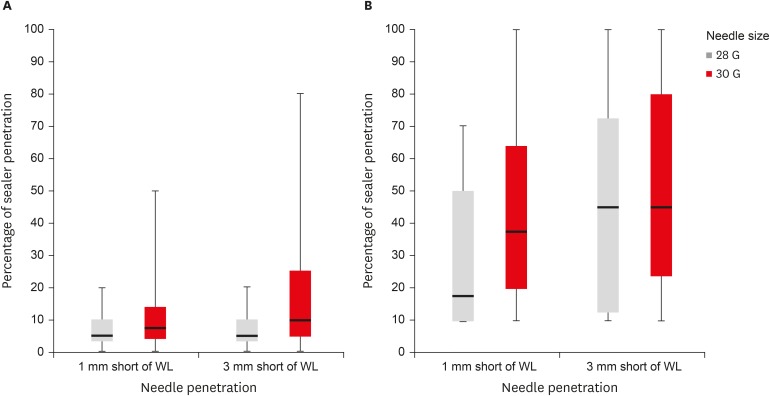
Figure 1 (A) Experimental set-up. (B) Image of needles used in this study.
Figure 2 Calculation of the amount of penetrated sealer into the dentinal tubules using a formula as follows: amount of sealer penetrated in the canal perimeter (green line) divided by the total canal perimeter (white line) × 100 (%). The longest penetration depth of sealer was also measured as microns (yellow line) via confocal laser scanning microscope (CLSM) image browser.
Figure 3 Depth of sealer penetration (µm) measured at different levels of needle insertion within each experimental group. In each box plot, the median value (line inside the box), the interquartile range (IQR; length of the box), and the minimum and maximum values (extreme lines) are reported. Values more than 1.5 IQRs but < 3 IQRs are labelled as outliers (o); values ≥ 3 IQRs are labelled as extreme cases (*). Brackets are connected between statistically different groups (p < 0.001).WL, working length.
Figure 4 Representative confocal laser scanning microscope (CLSM) images from each experimental group at 1 mm and 3 mm levels.WL, working length.
Figure 5 Percentage of sealer penetration measured at (A) 1 mm and (B) 3 mm levels from the apex within each experimental group. In each box plot, the median value (line inside the box), the interquartile range (IQR; length of the box), and the minimum and maximum values (extreme lines) are reported (Wilcoxon signed rank sum tests, p > 0.05).WL, working length.
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Influence of size and insertion depth of irrigation needle on debris extrusion and sealer penetration
The amount of extruded debris for each group of 28 G and 30 G needles according to the needle insertion depths of 1 mm and 3 mm short of working length (WL)
| Group | 28 G | 30 G |
|---|---|---|
| 1 mm short of WL (buccal roots) | 0.1090 ± 0.0268a | 0.0665 ± 0.0251c |
| 3 mm short of WL (palatal roots) | 0.0708 ± 0.0244b | 0.0296 ± 0.0138d |
The values are means and standard deviations (n = 10). In the group 1 mm short of WL, needles were inserted into buccal roots; in the group 3 mm short of WL, needles were inserted into palatal roots.
Different superscript letters mean statistical significant difference for each rows and columns (p < 0.001).
Table 1 The amount of extruded debris for each group of 28 G and 30 G needles according to the needle insertion depths of 1 mm and 3 mm short of working length (WL)
The values are means and standard deviations (
Different superscript letters mean statistical significant difference for each rows and columns (

