
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 42(4); 2017 > Article
- Research Article Smear layer removal by different chemical solutions used with or without ultrasonic activation after post preparation
-
Daniel Poletto1
 , Ana Claudia Poletto2, Andressa Cavalaro3, Ricardo Machado4, Leopoldo Cosme-Silva5, Cássia Cilene Dezan Garbelini6, Márcio Grama Hoeppner1
, Ana Claudia Poletto2, Andressa Cavalaro3, Ricardo Machado4, Leopoldo Cosme-Silva5, Cássia Cilene Dezan Garbelini6, Márcio Grama Hoeppner1 -
2017;42(4):-331.
DOI: https://doi.org/10.5395/rde.2017.42.4.324
Published online: November 1, 2017
1Department of Restorative Dentistry, Londrina State University (UEL), Londrina, PR, Brazil.
2Dentistry Course, Paranaense University, Cascavel, PR, Brazil.
3Clinical Practice Limited to Esthetic Dentistry, Campo Grande, MS, Brazil.
4Clinical Practice Limited to Endodontics, Navegantes, SC, Brazil.
5Department of Endodontics, São Paulo State University (UNESP) School of Dentistry, Araçatuba, SP, Brazil.
6Department of Oral Medicine and Pediatric Dentistry, Londrina State University (UEL), Londrina, PR, Brazil.
- Correspondence to Ricardo Machado, DDS, MSc, PhD. Clinical Practice Limited to Endodontics, Rua Brasilia, n. 300, Centro, Navegantes, SC 88.370-100, Brazil. Tel:+55-47-98409-1561, Fax: +55-47-3319-1625, ricardo.machado.endo@gmail.com
• Received: July 8, 2017 • Accepted: October 7, 2017
Copyright © 2017. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,515 Views
- 21 Download
- 12 Crossref
Abstract
-
Objectives This study evaluated smear layer removal by different chemical solutions used with or without ultrasonic activation after post preparation.
-
Materials and Methods Forty-five extracted uniradicular human mandibular premolars with single canals were treated endodontically. The cervical and middle thirds of the fillings were then removed, and the specimens were divided into 9 groups: G1, saline solution (NaCl); G2, 2.5% sodium hypochlorite (NaOCl); G3, 2% chlorhexidine (CHX); G4, 11.5% polyacrylic acid (PAA); G5, 17% ethylenediaminetetraacetic acid (EDTA). For the groups 6, 7, 8, and 9, the same solutions used in the groups 2, 3, 4, and 5 were used, respectively, but activated with ultrasonic activation. Afterwards, the roots were analyzed by a score considering the images obtained from a scanning electron microscope.
-
Results EDTA achieved the best performance compared with the other solutions evaluated regardless of the irrigation method (p < 0.05).
-
Conclusions Ultrasonic activation did not significantly influence smear layer removal.
INTRODUCTION
The success of endodontic treatment depends on both good apical and coronal sealing. This sealing prevents residual bacteria and their endotoxins from reaching the root apex, otherwise possibly leading to treatment failure [1,2]. For this reason, different techniques and materials have been extensively studied to enhance the performance of fillings and restorations of endodontically treated teeth [3,4,5].
Considering the extensive coronal destruction of most teeth requiring endodontic treatment, intraradicular glass fiber posts have frequently been used to keep these teeth in the oral cavity for a longer time. This type of post has been found to be a viable alternative in meeting today's greater aesthetic demands, especially because of its properties, such as modulus of elasticity similar to dentin [6], flexibility [7], and translucency [8].
The most widely used material for cementation of fiberglass posts is resin cement. Considering that this is an adhesive material, the retention of fiberglass posts when cemented with this material depends both on the characteristics of the cementing agent [9] and on the morphological characteristics of the intraradicular dentin [10,11].
The smear layer is a substrate of nonhomogeneous structure loosely adherent to the root canal walls composed of organic and inorganic particles, coagulated proteins, pulp tissue, blood cells, bacteria, and fungi [12]. The smear layer may be a factor supporting the persistence of infection, because of the organic and inorganic substrates in its composition. Therefore, it can compromise the intratubular penetration of endodontic sealers [13] and the adhesiveness of luting cements [14]. For these reasons, its removal with chemical substances has been advocated.
The most commonly used irrigating solutions for endodontic treatment are sodium hypochlorite (NaOCl) and chlorhexidine (CHX) [12]. These are used more specifically because of their antimicrobial properties; however, neither can remove the smear layer effectively. The solution most frequently used to remove the smear layer is ethylenediaminetetraacetic acid (EDTA) [12]. However, the vast majority of studies have demonstrated the inability of any of these solutions to completely remove the smear layer, especially when used passively (without any type of activation) [15]. For this reason, ultrasonic activation has been proposed to remove the smear layer. This technique is based on the premise that the energy released by the instrument improves the physicochemical properties of the irrigation solutions by cavitation and transmission of acoustic waves [16,17].
Considering that only a few studies, to date, have evaluated smear layer removal after preparation for cementation of intraradicular posts, the objective of this paper was to evaluate this variable, comparing different chemical solutions used with or without ultrasonic activation.
MATERIALS AND METHODS
After approval by the Research Ethics Committee of the Londrina State University (310.888/2013), 45 human lower premolars with a single canal and a completely formed apex, without previous endodontic treatment or anatomical complexities, were selected. These teeth were extracted for periodontal reasons or by orthodontic indication, from patients with ages ranging from 20–40 years. After extraction, the specimens were kept in 0.1% thymol solution until the moment of use. Before performing the instrumentation, the crowns were removed using a low-speed steel cutting disc (Isomet, Buehler, Lake Bluff, IL, USA), standardizing all roots at 15 mm in length.
Initially, the entrance orifice of the canal and the cervical and middle thirds were prepared using Largo No. 2 (Dentsply Maillefer, Rio de Janeiro, RJ, Brazil) and No. 4, 3, and 2 Gates Glidden drills (Dentsply-Maillefer, Ballaigues, Switzerland), respectively, according to the crown-down technique. The working length was determined by inserting a size 15 Flexo-File (Dentsply-Maillefer) up to the apical foramen, and subtracting 1 mm from this measurement.
The K3 system (SybronEndo, Scafati, Italy) was used for instrumentation, with a file of size 55/0.04 as the final instrument. An amount of 2.5 mL of 2.5% NaOCl (Formula e Ação, São Paulo, SP, Brazil) was used at change of each file, using disposable syringes and 30 G NaviTip needles (Ultradent, South Jordan, UT, USA) calibrated at 1 mm short of the working length. The root canals were dried with absorbent paper cones (Tanari, São Paulo, SP, Brazil), and filled using the lateral condensation technique and Fillapex sealer (Angelus, Londrina, PR, Brazil). Next, the specimens were stored at 37°C and 100% humidity for 7 days to allow the sealer to set.
The filling material was removed from the cervical and middle thirds using No. 2 Largo drills (Dentsply Maillefer, Brazil) calibrated at 10 mm. The canal was then prepared using a drill compatible with the diameter of the No. 2 fiberglass post from the Exacto system (Angelus), and the specimens were radiographed.
Afterwards, the root canals were irrigated according to the experimental groups (Table 1), using disposable syringes and 30 G NaviTip needles (Ultradent). In the groups where ultrasonic activation was performed, a 0.20 mm cylindrical insert (Irrisonic, Helse, São Paulo, SP, Brazil) was coupled to the device (Profi Class, Dabi Atlante, São Paulo, SP, Brazil) and activated at a power of 20% for 60 seconds, except on the G8 specimens where the activation was performed for only 20 seconds. The final irrigation was performed with 5 mL of 0.9% saline solution (NaCl) in all the groups except for the G1 specimens. Afterwards, the canals were dried again using absorbent paper points (Tanari).
Table 1
Experimental groups according to chemical solution and irrigation method
NaCl, saline solution; NaOCl, sodium hypochlorite; CHX, chlorhexidine; PAA, polyacrylic acid; EDTA, ethylenediaminetetraacetic acid; PUI, passive ultrasonic irrigation.
*Halex Istar Indústria Farmacêutica Ltda, Goiânia, GO, Brazil; †Asfer Ind. Quim. Ltda, São Caetano do Sul, SP, Brazil; ‡FGM Produtos Odontológicos, Joinville, SC, Brazil; §DFL Indústria e Comércio Ltda, Rio de Janeiro, RJ, Brazil; ∥Biodinâmica Química e Farmecêutica Ltda, Ibiporá, PR, Brazil.
Initially, longitudinal grooves were made in the buccolingual direction with a double-faced flexible diamond disc (KG Sorensen, Barueri, SP, Brazil), and the final cleavage was achieved using a pair of cutting pliers to expose the root canal. Afterwards, the hemisections were fixed in circular metal stubs to perform the metallization process. At this stage, the specimens received a surface layer of gold, about 30 nanometers thick, using the Quorum Q150R ES device (Quorum Technologies, Ashford, Kent, England).
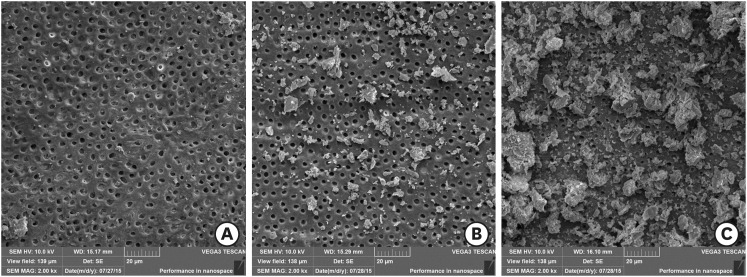
Three SEM images at × 2,000 magnification were obtained for each radicular hemisection, using a SEM (VEGA 3, Tescan, Brno, Czech Republic). These high magnification SEM images corresponded to the apical, middle and cervical portion of the prepared canal, 2, 5 and 8 mm short of the remainder of the filling material, respectively. The images were evaluated by a previously calibrated endodontist blinded to the research objectives. Only one score for the amount of smear layer was assigned to each image of each third (Table 2 and Figure 1) [18]. For each specimen, 3 images and 3 scores were obtained totaling 15 scores per group and 135 scores in total.
Table 2
Criteria for scoring the presence or absence of smear layer on the surface of the root canal or in the dentinal tubules
All data were analyzed by using Kruskal-Wallis and Mann-Whitney U tests with a significance level of 5% (SPSS software, SPSS, Chicago, IL, USA).
RESULTS
EDTA was found to have the highest smear layer removal ability, regardless of the irrigation method (with or without ultrasonic activation) (p < 0.05). In addition, the use of ultrasonic activation did not significantly influence smear layer removal when the same solution was used (G2 = G5, G3 = G6, G4 = G7, and G5 = G9, Table 3).
Table 3
Absolute and relative frequency of assigned scores in different groups
DISCUSSION
When fiber posts and resin cements are used to restore endodontically treated teeth, dentin adhesion results from the micromechanical retention created by the demineralized dentin surface associated with the formation of resinous tags [19]. Therefore, the cleaning of the root canal wall is a critical procedure to ensure successful treatment [20]. The objective of the present study was to evaluate the removal of the smear layer after preparation for cementation of intraradicular posts, comparing different chemical substances used with or without ultrasonic activation.
SEM has been the most widely used methods to evaluate the removal of the smear layer [10,15,17,18,21,22]. However, one of the main drawbacks related to this methodology is that the SEM allows the evaluation of only reduced areas, without considering the entire area of the root canal. Nevertheless, in the present study, the evaluation focused only on the area corresponding to the cervical and middle thirds. This area was divided into three segments (apical, medial, and cervical) and, because of the dimensions of the instrument used to prepare the intraradicular post, the total area for analysis of each segment was kept to about 1.1, 1.4 and 1.4 mm2, respectively. For this reason, we believe that it was possible to obtain representative images of the general context. Even so, we believe that further studies with similar methodological designs are needed using more complete analysis tools, such as microcomputed tomography.
Just like the results obtained in previous studies, those of the present study also showed that EDTA performed better than NaOCl [21,23] and CHX [22,24]. Although NaOCl is effective in dissolving the organic matter of the smear layer, it does not act effectively on the inorganic portion of this layer [12]. On the other hand, CHX is unable to dissolve organic matter, thus also compromising its smear layer removal ability [12,22,24,25].
In addition, no significant statistical differences were found between groups 5 and 9; that is, the use of ultrasonic activation did not potentiate the effects of EDTA. These results differ from those found in other studies [15,21]. Kuah et al. [15] evaluated smear layer removal promoted by 17% EDTA with or without ultrasonic activation for 1 and 3 minutes, and observed that the use of ultrasonic activation was able to potentiate the action of this solution. Lui et al. [21] evaluated smear layer removal by comparing Smear Clear (17% EDTA and surfactants) and 17% EDTA used with or without ultrasonic activation. According to the authors, the addition of surfactants to EDTA did not potentiate the removal of the smear layer. However, ultrasonic activation provided more favorable results, especially when 17% EDTA was used. However, 2 main points need to be taken into consideration. In both of the studies cited [12,14], removal of the smear layer was evaluated after instrumentation, whereas, in our study, removal followed preparation for cementation of the intraradicular posts [26,27]. In addition, Lui et al. [21] used 75 specimens divided into 5 groups (n = 15), and Kuah et al. [15] used 105 specimens divided into 7 groups (n = 15). In the present study, only 45 specimens were used and divided into 9 groups (n = 5). The use of fewer specimens per group may have influenced the results obtained, and this represents a limitation of this study.
Although polyacrylic acid (PAA) was not used conventionally in the intraradicular space, it was included in this study, considering its indication in dentin conditioning to potentiate adhesiveness [28,29]. The results showed that PAA was less effective than EDTA in removing the smear layer. Because PAA is a weak acid with high molecular weight, it only managed to disorganize the smear layer and not remove it effectively [30]. In addition, the action of PAA was not enhanced by the use of ultrasonic activation. This result was already expected, due to its consistency in gel form. However, PAA was used for 20 seconds in this study, according to the manufacturer's recommendations for restorations with glass ionomer cement. Therefore, we believe that further studies are needed to analyze the removal of the smear layer using the PAA for a longer period, considering that root dentin is more mineralized and sclerotic than the coronary dentin [31,32], for which this material has presented satisfactory results [28,29].
As mentioned previously, considering the particular characteristics of each substance used in the experimental groups of the present study, ultrasonic activation overall, failed to potentiate removal of the smear layer. Another point to consider is the activation method used. In the present study, ultrasonic activation was used for 20 seconds on G8 specimens and for 60 seconds on the specimens from the other groups. Ultrasonic activation at faster cycles produces a cumulative effect on debris removal [33] and facilitates keeping the tip of the activated instrument in a centralized position in the root canal, thus avoiding its contact with lateral root walls [34]. Therefore, in this study, the use of continuous activations may have led to not observing any advantages to using ultrasonic activation for smear layer removal in all the groups.
CONCLUSIONS
Considering the limitations of the present study, EDTA showed the best results for removal of the smear layer, compared with the other solutions evaluated. Use of ultrasonic activation showed no benefit in relation to removal of the smear layer.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Poletto D, Hoeppner MG.
Data curation: Poletto D, Poletto AC, Cavalaro A.
Formal analysis: Garbelini CCD, Hoeppner MG.
Funding acquisition: Poletto D, Poletto AC.
Investigation: Poletto D, Poletto AC, Cavalaro A.
Methodology: Poletto D, Hoeppner MG.
Project administration: Hoeppner MG.
Resources: Poletto D, Poletto AC.
Software: Garbelini CCD, Hoeppner MG.
Supervision: Garbelini CCD, Hoeppner MG.
Validation: Garbelini CCD, Hoeppner MG.
Visualization: Garbelini CCD, Hoeppner MG.
Writing - original draft: Poletto D, Hoeppner MG.
Writing - review & editing: Machado R, Cosme-Silva L.
- 1. Kirkevang LL, Ørstavik D, Hörsted-Bindslev P, Wenzel A. Periapical status and quality of root fillings and coronal restorations in a Danish population. Int Endod J 2000;33:509-515.ArticlePubMed
- 2. Hommez GM, Coppens CR, De Moor RJ. Periapical health related to the quality of coronal restorations and root fillings. Int Endod J 2002;35:680-689.ArticlePubMed
- 3. Mohammadi Z, Jafarzadeh H, Shalavi S, Bhandi S, Kinoshita J. Resilon: Review of a new material for obturation of the canal. J Contemp Dent Pract 2015;16:407-414.ArticlePubMed
- 4. Souza LC, Yadlapati M, Dorn SO, Silva R, Letra A. Analysis of radiopacity, pH and cytotoxicity of a new bioceramic material. J Appl Oral Sci 2015;23:383-389.ArticlePubMedPMC
- 5. Carvalho AO, Bruzi G, Anderson RE, Maia HP, Giannini M, Magne P. Influence of adhesive core buildup designs on the resistance of endodontically treated molars restored with lithium disilicate CAD/CAM crowns. Oper Dent 2016;41:76-82.ArticlePubMedPDF
- 6. Veríssimo C, Simamoto Júnior PC, Soares CJ, Noritomi PY, Santos-Filho PC. Effect of the crown, post, and remaining coronal dentin on the biomechanical behavior of endodontically treated maxillary central incisors. J Prosthet Dent 2014;111:234-246.ArticlePubMed
- 7. Freedman GA. Esthetic post-and-core treatment. Dent Clin North Am 2001;45:103-116.ArticlePubMed
- 8. Goracci C, Ferrari M. Current perspectives on post systems: a literature review. Aust Dent J 2011;56:77-83.ArticlePubMed
- 9. Calixto LR, Bandéca MC, Clavijo V, Andrade MF, Vaz LG, Campos EA. Effect of resin cement system and root region on the push-out bond strength of a translucent fiber post. Oper Dent 2012;37:80-86.ArticlePubMedPDF
- 10. Serafino C, Gallina G, Cumbo E, Ferrari M. Surface debris of canal walls after post space preparation in endodontically treated teeth: a scanning electron microscopic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:381-387.ArticlePubMed
- 11. Baena E, Flores A, Ceballos L. Influence of root dentin treatment on the push-out bond strength of fiber posts. Odontology 2017;105:170-177.ArticlePubMedPDF
- 12. Violich DR, Chandler NP. The smear layer in endodontics - a review. Int Endod J 2010;43:2-15.ArticlePubMed
- 13. Kuçi A, Alaçam T, Yavaş O, Ergul-Ulger Z, Kayaoglu G. Sealer penetration into dentinal tubules in the presence or absence of smear layer: a confocal laser scanning microscopic study. J Endod 2014;40:1627-1631.ArticlePubMed
- 14. Scotti N, Rota R, Scansetti M, Migliaretti G, Pasqualini D, Berutti E. Fiber post adhesion to radicular dentin: The use of acid etching prior to a one-step self-etching adhesive. Quintessence Int 2012;43:615-623.PubMed
- 15. Kuah HG, Lui JN, Tseng PS, Chen NN. The effect of EDTA with and without ultrasonics on removal of the smear layer. J Endod 2009;35:393-396.ArticlePubMed
- 16. Roy RA, Ahmad M, Crum LA. Physical mechanisms governing the hydrodynamic response of an oscillating ultrasonic file. Int Endod J 1994;27:197-207.ArticlePubMed
- 17. Kato AS, Cunha RS, da Silveira Bueno CE, Pelegrine RA, Fontana CE, de Martin AS. Investigation of the efficacy of passive ultrasonic irrigation versus irrigation with reciprocating activation: An environmental scanning electron microscopic study. J Endod 2016;42:659-663.ArticlePubMed
- 18. Torabinejad M, Cho Y, Khademi AA, Bakland LK, Shabahang S. The effect of various concentrations of sodium hypochlorite on the ability of MTAD to remove the smear layer. J Endod 2003;29:233-239.ArticlePubMed
- 19. Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, Vijay P, Van Landuyt K, Lambrechts P, Vanherle G. Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent 2003;28:215-235.PubMed
- 20. Boone KJ, Murchison DF, Schindler WG, Walker WA. Post retention: the effect of sequence of post-space preparation, cementation time, and different sealers. J Endod 2001;27:768-771.ArticlePubMed
- 21. Lui JN, Kuah HG, Chen NN. Effect of EDTA with and without surfactants or ultrasonics on removal of smear layer. J Endod 2007;33:472-475.ArticlePubMed
- 22. Poggio C, Dagna A, Chiesa M, Bianchi S, Arciola CR, Visai L, Giardino L. SEM evaluation of the root canal walls after treatment with Tetraclean. Int J Artif Organs 2010;33:660-666.ArticlePubMedPDF
- 23. Gu XH, Mao CY, Kern M. Effect of different irrigation on smear layer removal after post space preparation. J Endod 2009;35:583-586.ArticlePubMed
- 24. de Vasconcelos BC, Luna-Cruz SM, De-Deus G, de Moraes IG, Maniglia-Ferreira C, Gurgel-Filho ED. Cleaning ability of chlorhexidine gel and sodium hypochlorite associated or not with EDTA as root canal irrigants: a scanning electron microscopy study. J Appl Oral Sci 2007;15:387-391.PubMedPMC
- 25. Haapasalo M, Shen Y, Qian W, Gao Y. Irrigation in endodontics. Dent Clin North Am 2010;54:291-312.ArticlePubMed
- 26. Lo Giudice G, Lizio A, Giudice RL, Centofanti A, Rizzo G, Runci M, Alibrandi A, Cicciù M. The effect of different cleaning protocols on post space: a SEM study. Int J Dent 2016;2016:1907124.PubMedPMC
- 27. Mirseifinejad R, Tabrizizade M, Davari A, Mehravar F. Efficacy of different root canal irrigants on smear layer removal after post space preparation: a scanning electron microscopy evaluation. Iran Endod J 2017;12:185-190.PubMedPMC
- 28. Choudhary K, Nandlal B. Comparative evaluation of shear bond strength of nano-hydroxyapatite incorporated glass ionomer cement and conventional glass ionomer cement on dense synthetic hydroxyapatite disk: An in vitro study. Indian J Dent Res 2015;26:170-175.ArticlePubMed
- 29. Youm SH, Jung KH, Son SA, Kwon YH, Park JK. Effect of dentin pretreatment and curing mode on the microtensile bond strength of self-adhesive resin cements. J Adv Prosthodont 2015;7:317-322.ArticlePubMedPMC
- 30. Mount GJ. Buonocore Memorial Lecture. Glass-ionomer cements: past, present and future. Oper Dent 1994;19:82-90.PubMed
- 31. Vasiliadis L, Darling AI, Levers BG. The amount and distribution of sclerotic human root dentine. Arch Oral Biol 1983;28:645-649.ArticlePubMed
- 32. Vasiliadis L, Darling AI, Levers BG. The histology of sclerotic human root dentine. Arch Oral Biol 1983;28:693-700.PubMed
- 33. van der Sluis LW, Vogels MP, Verhaagen B, Macedo R, Wesselink PR. Study on the influence of refreshment/activation cycles and irrigants on mechanical cleaning efficiency during ultrasonic activation of the irrigant. J Endod 2010;36:737-740.ArticlePubMed
- 34. Sabins RA, Johnson JD, Hellstein JW. A comparison of the cleaning efficacy of short-term sonic and ultrasonic passive irrigation after hand instrumentation in molar root canals. J Endod 2003;29:674-678.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Cerium Oxide Nanoparticle Loaded with Toluidine Blue as Cavity Disinfectant Activated via Light-Emitting Diode on the Shear Bond Strength and Resin Tag Length of Universal Adhesive: A Scanning Electron Microscope-EDX Study
Amer M. Alanazi, Syed Hussain Askary, Ibrahim Warsi, Aamir Afzal, Muhammad Omar Niaz, Ambrina Qureshi
Photobiomodulation, Photomedicine, and Laser Surgery.2026;[Epub] CrossRef - O papel do ultrassom no tratamento e retratamento de canais radiculares: Revisão de literatura
Carlos Roberto Souza Hipp, Joaquim Carlos Fest da Silveira, Luiz Felipe Gilson de Oliveira Rangel, Tatiana Federici de Souza Fest da Silveira, Carla Minozzo Mello, Rodrigo Simões de Oliveira
Research, Society and Development.2025; 14(8): e1314849323. CrossRef - Effect of sodium hypochlorite, ethylenediaminetetraacetic acid, and dual-rinse irrigation on dentin adhesion using an etch-and-rinse or self-etch approach
Matej Par, Tobias Steffen, Selinay Dogan, Noah Walser, Tobias T. Tauböck
Scientific Reports.2024;[Epub] CrossRef - Evaluation of Effect of Poloxamer on Smear Layer Removal Using Apical Negative Pressure: An In Vitro Scanning Electron Microscopy Study
Chandra Prabha, Chitharanjan Shetty, Aditya Shetty
Journal of International Oral Health.2024; 16(6): 498. CrossRef - Laboratory Assessment of Antibacterial Efficacy of Five Different Herbal-based Potential Endodontic Irrigants
Anjali A Oak, Kailash Attur, Kamal Bagda, Nitish Mathur, Lubna Mohammad, Nikhat M Attar
Advances in Human Biology.2023; 13(4): 350. CrossRef - Dental Surface Conditioning Techniques to Increase the Micromechanical Retention to Fiberglass Posts: A Literature Review
Paulina Leticia Moreno-Sánchez, Maricela Ramírez-Álvarez, Alfredo del Rosario Ayala-Ham, Erika de Lourdes Silva-Benítez, Miguel Ángel Casillas-Santana, Diana Leyva del Rio, León Francisco Espinosa-Cristóbal, Erik Lizárraga-Verdugo, Mariana Melisa Avendaño
Applied Sciences.2023; 13(14): 8083. CrossRef - Effect of irrigation protocols on smear layer removal, bond strength and nanoleakage of fiber posts using a self-adhesive resin cement
Rodrigo Stadler Alessi, Renata Terumi Jitumori, Bruna Fortes Bittencourt, Giovana Mongruel Gomes, João Carlos Gomes
Restorative Dentistry & Endodontics.2023;[Epub] CrossRef - Effects of using different root canal sealers and protocols for cleaning intraradicular dentin on the bond strength of a composite resin used to reinforce weakened roots
Luiz Pascoal Vansan, Ricardo Machado, Celso Bernardes de Souza, Ricardo Gariba, Antônio Miranda da Cruz, Cinara Muniz, Jardel FranciscoX Jardel Francisco Mazzi-Chaves, Lucas da Fonseca Roberti Garcia
Journal of Oral Research.2022; 11(6): 1. CrossRef - Influence of the use of chelating agents as final irrigant on the push‐out bond strength of epoxy resin‐based root canal sealers: A systematic review
Carla M. Augusto, Miguel A. Cunha Neto, Karem P. Pinto, Ana Flavia A. Barbosa, Emmanuel J. N. L. Silva, Ana Paula P. dos Santos, Luciana M. Sassone
Australian Endodontic Journal.2022; 48(2): 347. CrossRef - Adhesion and whitening efficacy of P11-4 self-assembling peptide and HAP suspension after using NaOCl as a pre-treatment agent
Niloofar Hojabri, Karl-Heinz Kunzelmann
BMC Oral Health.2022;[Epub] CrossRef - Influence of resin cements and root canal disinfection techniques on the adhesive bond strength of fibre reinforced composite post to radicular dentin
Zaid A. Al Jeaidi
Photodiagnosis and Photodynamic Therapy.2021; 33: 102108. CrossRef - The Antibacterial Efficacy and In Vivo Toxicity of Sodium Hypochlorite and Electrolyzed Oxidizing (EO) Water-Based Endodontic Irrigating Solutions
Sung-Chih Hsieh, Nai-Chia Teng, Chia Chun Chu, You-Tai Chu, Chung-He Chen, Liang-Yu Chang, Chieh-Yun Hsu, Ching-Shuan Huang, Grace Ying-Wen Hsiao, Jen-Chang Yang
Materials.2020; 13(2): 260. CrossRef
 ePub Link
ePub Link Cite
CiteSmear layer removal by different chemical solutions used with or without ultrasonic activation after post preparation
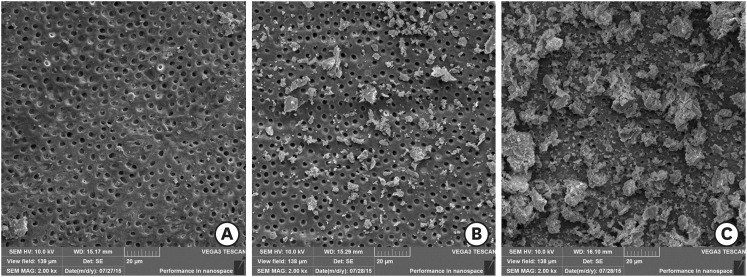
Figure 1 Representative images: (A) score 1; (B) score 2; (C) score 3.
Figure 1
Smear layer removal by different chemical solutions used with or without ultrasonic activation after post preparation
Experimental groups according to chemical solution and irrigation method
| Group | Chemical substance (volume) | Irrigation method |
|---|---|---|
| G1 | 0.09% NaCl (5 mL)* | Conventional |
| G2 | 2.5% NaOCl (5 mL)† | Conventional |
| G3 | 2% CHX (5 mL)‡ | Conventional |
| G4 | 11.5% PAA (1 mL)§ | Conventional |
| G5 | 17% EDTA (5 mL)∥ | Conventional |
| G6 | 2.5% NaOCl (5 mL)† | PUI |
| G7 | 2% CHX (5 mL)‡ | PUI |
| G8 | 11.5% PAA (5 mL)§ | PUI |
| G9 | 17% EDTA (5 mL)∥ | PUI |
NaCl, saline solution; NaOCl, sodium hypochlorite; CHX, chlorhexidine; PAA, polyacrylic acid; EDTA, ethylenediaminetetraacetic acid; PUI, passive ultrasonic irrigation.
*Halex Istar Indústria Farmacêutica Ltda, Goiânia, GO, Brazil; †Asfer Ind. Quim. Ltda, São Caetano do Sul, SP, Brazil; ‡FGM Produtos Odontológicos, Joinville, SC, Brazil; §DFL Indústria e Comércio Ltda, Rio de Janeiro, RJ, Brazil; ∥Biodinâmica Química e Farmecêutica Ltda, Ibiporá, PR, Brazil.
Criteria for scoring the presence or absence of smear layer on the surface of the root canal or in the dentinal tubules
| Score | Criterion |
|---|---|
| 1 | No smear layer - No smear layer on the surface of the root canals; all tubules were clean and open. |
| 2 | Moderate smear layer - No smear layer on the surface of root canal, but tubules contained debris. |
| 3 | Heavy smear layer - Smear layer covered the root canal surfasse and the tubules. |
Absolute and relative frequency of assigned scores in different groups
| Group | Score 1 | Score 2 | Score 3 | Total | ||||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | No. | % | |
| G1a,b | 2 | 13.3 | 4 | 26.7 | 9 | 60.0 | 15 | 100 |
| G2c,d | 0 | 0.0 | 9 | 69.0 | 6 | 40.0 | 15 | 100 |
| G3e,f | 1 | 6.7 | 8 | 53.3 | 6 | 40.0 | 15 | 100 |
| G4g,h | 2 | 13.3 | 10 | 66.7 | 3 | 20.0 | 15 | 100 |
| G5a,c,e,g,i,j,k | 8 | 53.3 | 7 | 46.7 | 0 | 0.0 | 15 | 100 |
| G6i,l | 2 | 13.3 | 10 | 66.7 | 3 | 20.0 | 15 | 100 |
| G7j,m | 1 | 6.7 | 8 | 53.3 | 6 | 40.0 | 15 | 100 |
| G8k,n | 1 | 6.7 | 9 | 60.0 | 5 | 33.3 | 15 | 100 |
| G9b,d,f,h,l,m,n | 11 | 73.3 | 4 | 26.7 | 0 | 0.0 | 15 | 100 |
| Total | 28 | 20.7 | 69 | 51.1 | 38 | 28.2 | 135 | 100 |
a–nThe same superscript letters indicate statistically significant difference among the groups (Mann-Whitney U test; p < 0.05).
Table 1 Experimental groups according to chemical solution and irrigation method
NaCl, saline solution; NaOCl, sodium hypochlorite; CHX, chlorhexidine; PAA, polyacrylic acid; EDTA, ethylenediaminetetraacetic acid; PUI, passive ultrasonic irrigation.
*Halex Istar Indústria Farmacêutica Ltda, Goiânia, GO, Brazil; †Asfer Ind. Quim. Ltda, São Caetano do Sul, SP, Brazil; ‡FGM Produtos Odontológicos, Joinville, SC, Brazil; §DFL Indústria e Comércio Ltda, Rio de Janeiro, RJ, Brazil; ∥Biodinâmica Química e Farmecêutica Ltda, Ibiporá, PR, Brazil.
Table 2 Criteria for scoring the presence or absence of smear layer on the surface of the root canal or in the dentinal tubules
Table 3 Absolute and relative frequency of assigned scores in different groups
a–nThe same superscript letters indicate statistically significant difference among the groups (Mann-Whitney

