
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 42(1); 2017 > Article
- Research Article Retreatability of two endodontic sealers, EndoSequence BC Sealer and AH Plus: a micro-computed tomographic comparison
- Enrique Oltra1, Timothy C. Cox2,3,4, Matthew R. LaCourse3, James D. Johnson1, Avina Paranjpe1
-
2016;42(1):-26.
DOI: https://doi.org/10.5395/rde.2017.42.1.19
Published online: December 8, 2016
1Department of Endodontics, University of Washington, Seattle, WA, USA.
2Department of Pediatrics (Craniofacial Medicine), University of Washington, Seattle, WA, USA.
3Center for Developmental Biology and Regenerative Medicine, Seattle Children's Research Institute, Seattle, WA, USA.
4Department of Anatomy and Developmental Biology, Monash University, Clayton, Victoria, Australia.
- Correspondence to Avina Paranjpe, BDS, MS, MSD, PhD. Associate Professor, Department of Endodontics, University of Washington School of Dentistry, 1959 NE Pacific Street, D-669 Health Science Center, Box 357448 Seattle, WA, USA 98195. TEL, +1-206-685-7517; FAX, +1-206-616-9085; avina@uw.edu
• Received: August 9, 2016 • Accepted: October 13, 2016
©Copyrights 2017. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 5,182 Views
- 75 Download
- 93 Crossref
Abstract
-
Objectives Recently, bioceramic sealers like EndoSequence BC Sealer (BC Sealer) have been introduced and are being used in endodontic practice. However, this sealer has limited research related to its retreatability. Hence, the aim of this study was to evaluate the retreatability of two sealers, BC Sealer as compared with AH Plus using micro-computed tomographic (micro-CT) analysis.
-
Materials and Methods Fifty-six extracted human maxillary incisors were instrumented and randomly divided into 4 groups of 14 teeth: 1A, gutta-percha, AH Plus retreated with chloroform; 1B, gutta-percha, AH Plus retreated without chloroform; 2A, gutta-percha, EndoSequence BC Sealer retreated with chloroform; 2B, gutta-percha, EndoSequence BC Sealer retreated without chloroform. Micro-CT scans were taken before and after obturation and retreatment and analyzed for the volume of residual material. The specimens were longitudinally sectioned and digitized images were taken with the dental operating microscope. Data was analyzed using an ANOVA and a post-hoc Tukey test. Fisher exact tests were performed to analyze the ability to regain patency.
-
Results There was significantly less residual root canal filling material in the AH Plus groups retreated with chloroform as compared to the others. The BC Sealer samples retreated with chloroform had better results than those retreated without chloroform. Furthermore, patency could be re-established in only 14% of teeth in the BC Sealer without chloroform group.
-
Conclusion The results of this study demonstrate that the BC Sealer group had significantly more residual filling material than the AH Plus group regardless of whether or not both sealers were retreated with chloroform.
Introduction
The success of nonsurgical endodontic therapy depends on the removal of necrotic and inflamed tissue, microorganisms, and debris from the root canal system and the prevention of recontamination.1 Four conditions which include pre-operative absence of periapical radiolucency, root filling with no voids, root filling extending to 2 mm within the radiographic apex, and satisfactory coronal restoration, were found to significantly improve the outcome of primary root canal treatment.2 However, endodontic failures do occur and the percentages of cases that fail to heal can range from 15 - 22%.3 Nonsurgical retreatment is the principal treatment of choice to manage post-treatment disease.4 Retreatment consists of the removal of existing obturation material to allow disinfection of the root canal system in order to provide an environment satisfactory for periradicular healing.5 Nevertheless, the myriad of retreatment techniques and studies consistently find residual root canal filling after removal is accomplished.6 Removing filling material from root canal systems is necessary because this material could potentially cause a mechanical barrier that hinders contact of irrigating solutions and intracanal dressings to the root canal walls.7 Furthermore, there maybe bacteria present in these areas that could be responsible for post treatment pathosis.8 For this purpose, it is imperative that the obturation material be completely removed in order to improve chances of success.
Gutta-percha (GP) in conjunction with sealers is the most common root canal filling material.9 Currently, many different sealers are being used in endodontics.10,11 More recently, bioceramic sealers like EndoSequence BC Sealer (BC Sealer, Brasseler USA, Savannah, GA, USA) have been introduced and are being used in endodontic practice. BC Sealer is a premixed bioceramic endodontic sealer that is composed of zirconium oxide, calcium silicates, calcium phosphate (monobasic), calcium hydroxide, filler, and thickening agents.12 However, this sealer has a short history of use and limited research related to its retreatability. Previous studies on bioceramic sealers have evaluated their bond strength, sealing ability, root fracture resistance, setting properties, cytotoxicity, and antibacterial effects.13,14,15,16,17 However, there are limited studies related to the retreatability of these sealers.18 On the contrary, AH Plus (Dentsply International Inc., York, PA, USA), an epoxy-resin-based endodontic sealer, has an extensive history of use and research studies13,14,17,19 which is why it has been used for many comparative studies.19,20,21
The efficacy of removing the root filling materials during retreatment has been assessed by many different methods. However, most methodologies destroy the specimens. These methodologies include horizontal or vertical splitting of the examined teeth or clearing to render the teeth transparent.22,23 Another method involves micro-computed tomography (micro-CT) analysis.8 This method has been used previously and provides detailed imaging of the root canal system without destroying the specimen.
It is important to understand if these newer sealers are retreatable, especially since these materials are being used routinely in endodontics and could affect periapical healing.24 Hence, the aim of this study was to evaluate the retreatability of BC Sealer as compared with AH Plus sealer using micro-CT analysis. The null hypothesis tested was that there were no differences in the retreatability of BC Sealer and AH Plus sealer.
Materials and Methods
Fifty-six extracted human single-rooted maxillary anterior teeth with straight roots were selected. Roots with curvatures higher than twenty degrees were excluded. Only fully formed apices with a single root canal and a single apical foramen were included. The presence of a single canal was verified with buccal and proximal radiographs. Teeth were divided into 4 groups of 14 teeth each:
Group 1A: Canals obturated with GP/AH Plus and retreated using chloroform.
Group 1B: Canals obturated with GP/AH Plus and retreated without chloroform.
Group 2A: Canals obturated with GP/BC Sealer and retreated using chloroform.
Group 2B: Canals obturated with GP/BC Sealer and retreated without chloroform.
Teeth that had an initial apical file size of more than a size 25 were discarded. Teeth were decoronated with a diamond disk (Keystone industries, Gibbstown, NJ, USA) to standardize the lengths to 17 mm with the aid of calipers. After access, cavity preparation patency and working length were determined by introducing a size 10 Flexofile (Dentsply Maillefer, Tulsa, OK, USA) in the canal until it was visible at the apical foramen and by subtracting 1 mm from this measurement for a working length (WL) of 16 mm.
Instrumentation of teeth was performed by using a crown-down technique with Vortex Blue (Dentsply, Tulsa Dental Specialties, Tulsa, OK, USA) nickel titanium rotary instruments at 500 rpm to master apical file of size size 45/0.04 taper. Files were used to instrument 5 canals and then replaced. Each canal was filled with irrigant during instrumentation. Three mL of 6% NaOCl was used for irrigation after each file. A size 10 Flexofile was used to reconfirm patency. As a final rinse each canal was irrigated with 2 mL 17% EDTA, 2 mL NaOCl, followed by 2 mL of sterile saline, and then dried with paper points. All irrigating solutions were delivered with a 30 G Max-i-Probe irrigating needle (Dentsply-Rinn, Elgin, IL, USA) placed 1 mm short of the WL.
Specimens were numbered and scanned with a micro-CT (Skyscan 1076, Bruker microCT, Antwerp, Belgium). Each specimen was scanned three times: once following instrumentation to enable calculation of the root canal volume, once to confirm the homogeneity of root canal obturation, and the final time to determine the volume of remaining material. The scanning parameters for each scan were kept constant: 65 kV (10 W, 154 µA), a 0.5 mm aluminum filter, a 160 milllisecond exposure time and 0.70° rotation step, and isotropic voxel size of 35 µm. Raw scan data were reconstructed into multiplanar slice data using the computer program, NRecon V1.6.1.0 (Bruker microCT).
After reconstruction of the initial scan dataset, the degree of curvature of the root canals was re-evaluated from images rendered with the 3D volume exploration software, Drishti V2.4 (http://sf.anu.edu.au/Vizlab/drishti) and compared with the original determinations from the 2D radiographs. The curvatures were checked once again to ensure none had curvatures greater than 20 degrees. For calculation of the root canal volume following instrumentation, the canal was reverse filled by inverting the rendering settings (ie. transfer function) and using the getvolume function in Drishti.
To enable calculation of total remaining sealer after retreatment, rendering settings were applied that readily detected the radiopaque sealer (Figure 1). The same rendering settings were applied to both the second (obturated) and third (retreated) scan datasets and the volumes of sealer determined again using the getvolume function. For visualization purposes, the 3D renderings of each tooth was manually aligned and oriented in the same multi-dimensional space and different transfer functions applied to show both the surface of the root and the sealer (Figure 1, root, black; obturation material, orange). For subdivision of the root canal into thirds (apical, middle, and coronal), the rendered datasets were virtually cut in the horizontal plane such that each third consisted of the exact number of rendered slices. The volume of sealer remaining in each third was then determined using the getvolume function of Drishti as described above.
The teeth were randomly divided into 2 groups (Groups 1 and 2) of 28 each. All canals were obturated by the continuous wave compaction technique. In Group 1, twenty-eight canals were obturated by coating EndoSequence gutta-percha (Brasseler USA) of size 45/0.04 with AH Plus sealer (Dentsply Maillefer) following the manufacturer's protocol. In Group 2, 28 canals were obturated with EndoSequence gutta-percha points and EndoSequence BC Sealer again following the manufacturer's protocol. The access preparations were sealed with Cavit (3M ESPE, St. Paul, MN, USA). The same volumes of sealer were used for both groups of teeth. The specimens were scanned a second time with the micro-CT using the same scanning parameters to confirm the homogeneity of root canal obturation. All samples were stored at 37℃ in 100% humidity for 30 days to allow the sealers to set completely. A single operator performed all the procedures.
Each group was divided into two subgroups: Groups 1A and 2A were retreated using chloroform; Groups 1B and 2B were retreated without chloroform. Briefly, for Groups 1A and 2A, Cavit was removed and a total of 0.2 mL of chloroform was used for each tooth. Two drops of chloroform were introduced in the access preparations. ProFile ISO Rotary Files (Dentsply Maillefer) of size 45/0.04 taper at 300 rpm were used until WL was reached or resistance was met. If the WL was reached, crown-down instrumentation was performed using Vortex Blue size 45/0.04 at 500 rpm to WL to remove the remaining obturation material. If the WL was not reached, small hand files (C+ Files, and Flexofile sizes 6, 8, and 10) were used to reach WL. When WL was reached, the canal was instrumented to length with Vortex Blue size 50/0.04. The remaining volume of chloroform was introduced in the canals and any remaining gutta-percha was removed with paper points. As a final rinse, each canal was irrigated with 5 mL of 6% NaOCl, 5 mL of 17% EDTA, followed by 2 mL of sterile saline, and then dried with paper points. Files were used to instrument 5 canals and then replaced.
For Groups 1B and Group 2B, retreatment was done as stated above in the methods section with the similar rotary files but without chloroform. After retreatment of all samples, a third micro-CT scan was performed using the same parameters as the first two scans.
The specimens were longitudinally sectioned and observed under the dental operating microscope (×20 magnification, Global Surgical Corp., St. Louis, MO, USA).14 Digitized images were taken for correlation with the results from the micro-CT imaging.
SigmaPlot 11.0 (Systat Software Inc., San Jose, CA, USA) was used for the statistical testing. The required sample size was calculated to be 14 samples per group. This gave at least 95% power to detect a maximum difference between group means. Data from the experiments were analyzed using an analysis of variance (ANOVA) to determine differences among the groups, with further pairwise multiple comparisons with a post hoc Tukey test. Fisher exact tests were performed to analyze the ability to regain patency. Differences with p < 0.05 were considered significant.
Results
The percentages of residual filling material was calculated based on an equation stated in a previous study.8 Analysis of the rendered micro-CT images showed significantly less residual root filling material in Group 1A when compared to Groups 1B, 2A, and 2B when the entire length of the root canal was analyzed (Figure 1). The BC Sealer group retreated with chloroform (Group 2A) showed significantly less sealer than the BC Sealer Group 2B (Figure 2). These results were verified and related closely with the longitudinal sections of the teeth (Figure 1). Group 1B showed less residual material compared to Group 2B, however, these results were not statistically significant. All teeth were scanned using micro-CT but only representative images have been shown in Figure 1.
The teeth were further analyzed after micro-CT analysis for residual filling material in the coronal, middle, and apical thirds of the canal. There was significantly less residual root canal filling material in all the areas of Group 1A compared to those one-thirds of Groups 1B, 2A, and 2B (Figure 3). Furthermore, the BC Sealer group that was retreated without chloroform (Group 2B) showed significantly more sealer in the coronal 1/3 of the root as compared to those teeth that were retreated with chloroform (Group 2A).
Establishing patency and WL in retreatment cases has been shown to significantly improve periapical healing rates.24 Hence these two factors were considered in this study when evaluating all the groups. Patency and WL were reestablished in all the teeth (100%) in the AH Plus groups (Groups 1A and 1B). WL and patency were re-established in 93% of teeth in Group 2A. In contrast, although WL was re-established in 93% of Group 2B teeth, patency could only be re-established in 14% of the cases, which was significantly different from the other groups (p < 0.0001, Table 1).
Discussion
Root canal failures occur due to persistent periapical disease after treatment.24 There are a number of causes that could lead to failure to heal which include necrotic tissue, bacterial biofilms, coronal leakage, recurrent caries, and tooth fractures.25,26 In order to establish adequate periapical healing, these etiological factors must be removed. Hence, it is imperative that the root canal system be adequately cleaned which would entail removing the entire existing root canal filling. Furthermore, establishing patency and WL in retreatment cases has been shown to significantly improve periapical healing rates.24 However, this is not always possible due to various factors, which include root canal anatomy.27
Many new sealers have been introduced in the market; however, the retreatability of some of these sealers is still unknown. Hence, this study evaluated the retreatability of the relatively new BC Sealer compared to the more commonly used AH Plus sealer. Previous studies have shown that AH Plus is soluble in chloroform to about 99% which is why it was used for this comparative study.28,29 Our results demonstrate that BC Sealer left significantly more residual filling material in the root canal as compared to AH Plus whether or not they were retreated with chloroform, although when treatment was performed with chloroform the differences were even more marked. Nevertheless, when treated with chloroform, the BC Sealer group left less residual material when compared to the group without chloroform (Figure 2). This notable difference between the sealers could be attributed to the fact that BC Sealer has the potential to adhere to the dentin.20 Another explanation for this finding could be related to the tag-like structures that were of calcium and phosphate materials, suggesting intratubular precipitation and this may be responsible for the sealing ability and dentine bonding of this material.30,31 Some previous studies have inferred that BC Sealer and AH Plus had comparable remaining filling material.18,32 However, retreatment methods and the techniques used in these studies were different and so firm conclusions are not possible. In this study, we employed non-destructive, quantitative high resolution micro-CT-based imaging to assess the percentage of residual filling material of EndoSequence BC Sealer compared to AH Plus with or without the use of chloroform. This methodology, which has been successfully used in other studies, allows stepwise assessment by repeated scans of the same root specimen.11,33
Analysis of the apical, middle, and coronal one-thirds of the canals of retreated teeth indicated that AH Plus with the use chloroform had significantly less residual filling material compared to all one-thirds from all the other groups (Figure 3). The longitudinal sections of the teeth corroborated the findings from the micro-CT scans (Figure 1). An interesting observation was the coronal 1/3 of both the Groups 1B and 2B, which demonstrated more filling material remaining. This could be attributed to tooth anatomy and the fact that no chloroform was used in these groups and maybe a solvent is necessary to clean the coronal 1/3 of the canal more efficiently. Most sections showed only residual sealer, however, there were a few specimens in all the groups that did show some residual gutta percha with sealer (Figure 1). This is an important finding as it correlates to some earlier studies that mention that no technique or solvent was effective in completely cleaning the root canal system during retreatment procedures.18,34
Another important factor to consider is the concern related to the toxicity of chloroform. In 1976, the U.S. Food and Drug Administration (FDA) banned the use of chloroform in drugs and cosmetics due to toxicity concerns.35 However, there is no available data related to the toxicity of chloroform in endodontics and previous studies have demonstrated that chloroform is safe to be used in endodontics.36,37,38 Furthermore, chloroform has been shown to efficiently soften gutta percha along with having some antimicrobial activity against E. faecalis during retreatment procedures.39,40 Hence, based on previous research chloroform was used in this study.
Our study focused on single rooted teeth based on previous studies and the fact that we wanted to demonstrate differences in less complex anatomy.33 It is a possibility that more complex anatomy like mesial roots of mandibular molars could demonstrate even more significant differences between the two sealer groups. Another important aspect that was taken into consideration was the volume of sealer and the quantity of chloroform used in the study. The quantity of chloroform was standardized between Groups 1A and 2A, and the same volume of sealer was used for all the groups. Both these aspects of this study are important as these could have been potential variables when analyzing the results of the study.
Hess et al. evaluated the retreatability of BC Sealer and AH Plus related to patency and loss of WL using the scanning electron microscope.41 This study reported that BC Sealer was impenetrable to small hand files when it remained in the apical foramen. In this study, we had similar results. We demonstrated that while WL and patency could be re-established in 100% of AH Plus samples, these could not be re-established in every tooth in the BC Sealer groups. With the use of chloroform, WL and patency was regained in 93% of BC Sealer samples. Without the use of chloroform WL was re-established in 93% of cases, with patency in only 14% of the BC Sealer samples, which was significantly different from the other groups (Table 1). This is an important factor to consider especially during retreatments as this could affect periapical healing.24
Koch and Brave published a series of three review articles that included retreatment techniques for the removal of gutta-percha and EndoSequence BC Sealer.42 In the reviews, they recommended that retreatment techniques include the use of rotary, hand files, ultrasonics, and solvents (i.e. chloroform), which is why rotary files were used this study. A recent study suggested the use of solvents during retreatments as this technique reduced the amount of debris extruded apically and also reduced the time taken to retreat teeth.43 Furthermore, chloroform has been shown to have a superior ability over other solvents in dissolving canal sealing materials.44 Chloroform did prove to be effective when used with BC Sealer as it increased the likelihood of regaining patency in these samples (Table 1). However, we believe that it may be necessary to develop a solvent that has superior effect on bioceramic sealers to improve its retreatability.
Conclusion
The results of this in vitro study show that conventional retreatment techniques are not always able to fully remove all the filling material from the canal; however, the AH Plus group retreated with chloroform had significantly less material remaining than BC Sealer whether or not chloroform was used. Moreover, the use of chloroform increased the likelihood of regaining patency in a few of the BC Sealer samples but could not be achieved in 100% of the cases. We believe this information is important for practitioners especially when they are retreating teeth that have been previously obturated with BC Sealer.
Acknowledgement
This research was supported by the AAE Foundation Resident Research Grant.
- 1. Haapasalo M, Shen Y, Qian W, Gao Y. Irrigation in endodontics. Dent Clin North Am 2010;54:291-312.ArticlePubMed
- 2. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - part 2. influence of clinical factors. Int Endod J 2008;41:6-31.ArticlePubMed
- 3. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - part 1. effects of study characteristics on probability of success. Int Endod J 2007;40:921-939.ArticlePubMed
- 4. Friedman S. Prognosis of initial endodontic therapy. Endod Topics 2002;2:59-88.ArticlePDF
- 5. Stabholz A, Friedman S. Endodontic retreatment-case selection and technique. Part 2: treatment planning for retreatment. J Endod 1988;14:607-614.ArticlePubMed
- 6. Yadav P, Bharath MJ, Sahadev CK, Makonahalli Ramachandra PK, Rao Y, Ali A, Mohamed S. An in vitro CT comparison of gutta-percha removal with two rotary systems and hedstrom files. Iran Endod J 2013;8:59-64.PubMedPMC
- 7. Barletta FB, Rahde Nde M, Limongi O, Moura AA, Zanesco C, Mazocatto G. In vitro comparative analysis of 2 mechanical techniques for removing gutta-percha during retreatment. J Can Dent Assoc 2007;73:65.PubMed
- 8. Hammad M, Qualtrough A, Silikas N. Three-dimensional evaluation of effectiveness of hand and rotary instrumentation for retreatment of canals filled with different materials. J Endod 2008;34:1370-1373.ArticlePubMed
- 9. Kratchman SI. Obturation of the root canal system. Dent Clin North Am 2004;48:203-215.ArticlePubMed
- 10. Flores DS, Rached FJ Jr, Versiani MA, Guedes DF, Sousa-Neto MD, Pécora JD. Evaluation of physicochemical properties of four root canal sealers. Int Endod J 2011;44:126-135.ArticlePubMed
- 11. Marin-Bauza GA, Silva-Sousa YT, da Cunha SA, Rached-Junior FJ, Bonetti-Filho I, Sousa-Neto MD, Miranda CE. Physicochemical properties of endodontic sealers of different bases. J Appl Oral Sci 2012;20:455-461.ArticlePubMedPMC
- 12. Hess D, Solomon E, Spears R, He J. Retreatability of a bioceramic root canal sealing material. J Endod 2011;37:1547-1549.ArticlePubMed
- 13. Ozkocak I, Sonat B. Evaluation of effects on the adhesion of various root canal sealers after Er:YAG laser and irrigants are used on the dentin surface. J Endod 2015;41:1331-1336.ArticlePubMed
- 14. Pawar SS, Pujar MA, Makandar SD. Evaluation of the apical sealing ability of bioceramic sealer, AH plus & epiphany: an in vitro study. J Conserv Dent 2014;17:579-582.PubMedPMC
- 15. Topçuoğlu HS, Tuncay Ö, Karataş E, Arslan H, Yeter K. In vitro fracture resistance of roots obturated with epoxy resin-based, mineral trioxide aggregate-based, and bioceramic root canal sealers. J Endod 2013;39:1630-1633.ArticlePubMed
- 16. Loushine BA, Bryan TE, Looney SW, Gillen BM, Loushine RJ, Weller RN, Pashley DH, Tay FR. Setting properties and cytotoxicity evaluation of a premixed bioceramic root canal sealer. J Endod 2011;37:673-677.ArticlePubMed
- 17. Candeiro GT, Moura-Netto C, D'Almeida-Couto RS, Azambuja-Júnior N, Marques MM, Cai S, Gavini G. Cytotoxicity, genotoxicity and antibacterial effectiveness of a bioceramic endodontic sealer. Int Endod J 2015 8 17 [Epub ahead of print].ArticlePDF
- 18. Uzunoglu E, Yilmaz Z, Sungur DD, Altundasar E. Retreatability of root canals obturated using gutta-percha with bioceramic, MTA and resin-based sealers. Iran Endod J 2015;10:93-98.PubMedPMC
- 19. Du T, Wang Z, Shen Y, Ma J, Cao Y, Haapasalo M. Combined antibacterial effect of sodium hypochlorite and root canal sealers against Enterococcus faecalis biofilms in dentin canals. J Endod 2015;41:1294-1298.ArticlePubMed
- 20. Candeiro GT, Correia FC, Duarte MA, Ribeiro-Siqueira DC, Gavini G. Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J Endod 2012;38:842-845.ArticlePubMed
- 21. Gade VJ, Belsare LD, Patil S, Bhede R, Gade JR. Evaluation of push-out bond strength of endosequence BC sealer with lateral condensation and thermoplasticized technique: an in vitro study. J Conserv Dent 2015;18:124-127.ArticlePubMedPMC
- 22. Wolcott JF, Himel VT, Hicks ML. Thermafil retreatment using a new ‘System B’ technique or a solvent. J Endod 1999;25:761-764.ArticlePubMed
- 23. Zmener O, Pameijer CH, Banegas G. Retreatment efficacy of hand versus automated instrumentation in oval-shaped root canals: an ex vivo study. Int Endod J 2006;39:521-526.ArticlePubMed
- 24. Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J 2011;44:583-609.ArticlePubMed
- 25. Stabholz A, Friedman S. Endodontic retreatment-case selection and technique. Part 2: treatment planning for retreatment. J Endod 1988;14:607-614.ArticlePubMed
- 26. Friedman S, Stabholz A. Endodontic retreatment-case selection and technique. Part 1: criteria for case selection. J Endod 1986;12:28-33.ArticlePubMed
- 27. Rechenberg DK, Paqué F. Impact of cross-sectional root canal shape on filled canal volume and remaining root filling material after retreatment. Int Endod J 2013;46:547-555.ArticlePubMed
- 28. Schäfer E, Zandbiglari T. A comparison of the effectiveness of chloroform and eucalyptus oil in dissolving root canal sealers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:611-616.ArticlePubMed
- 29. Bodrumlu E, Er O, Kayaoglu G. Solubility of root canal sealers with different organic solvents. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:e67-e69.ArticlePubMed
- 30. Han L, Okiji T. Bioactivity evaluation of three calcium silicate-based endodontic materials. Int Endod J 2013;46:808-814.ArticlePubMed
- 31. Han L, Okiji T. Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J 2011;44:1081-1087.ArticlePubMed
- 32. Ersev H, Yilmaz B, Dinçol ME, Dağlaroğlu R. The efficacy of ProTaper Universal rotary retreatment instrumentation to remove single gutta-percha cones cemented with several endodontic sealers. Int Endod J 2012;45:756-762.ArticlePubMed
- 33. Roggendorf MJ, Legner M, Ebert J, Fillery E, Frankenberger R, Friedman S. Micro-CT evaluation of residual material in canals filled with Activ GP or GuttaFlow following removal with NiTi instruments. Int Endod J 2010;43:200-209.ArticlePubMed
- 34. Sağlam BC, Koçak MM, Türker SA, Koçak S. Efficacy of different solvents in removing gutta-percha from curved root canals: a micro-computed tomography study. Aust Endod J 2014;40:76-80.ArticlePubMed
- 35. Davidson IW, Sumner DD, Parker JC. Chloroform: a review of its metabolism, teratogenic, mutagenic, and carcinogenic potential. Drug Chem Toxicol 1982;5:1-87.ArticlePubMed
- 36. Margelos J, Verdelis K, Eliades G. Chloroform uptake by gutta-percha and assessment of its concentration in air during the chloroform-dip technique. J Endod 1996;22:547-550.ArticlePubMed
- 37. Chutich MJ, Kaminski EJ, Miller DA, Lautenschlager EP. Risk assessment of the toxicity of solvents of gutta-percha used in endodontic retreatment. J Endod 1998;24:213-216.ArticlePubMed
- 38. McDonald MN, Vire DE. Chloroform in the endodontic operatory. J Endod 1992;18:301-303.ArticlePubMed
- 39. Edgar SW, Marshall JG, Baumgartner JC. The antimicrobial effect of chloroform on Enterococcus faecalis after gutta-percha removal. J Endod 2006;32:1185-1187.ArticlePubMed
- 40. Tamse A, Unger U, Metzger Z, Rosenberg M. Gutta-percha solvents-a comparative study. J Endod 1986;12:337-339.ArticlePubMed
- 41. Hess D, Solomon E, Spears R, He J. Retreatability of a bioceramic root canal sealing material. J Endod 2011;37:1547-1549.ArticlePubMed
- 42. Koch KA, Brave D. EndoSequence: melding endodontics with restorative dentistry, part 3. Dent Today 2009;28:88-92.
- 43. Çanakçi BC, Er O, Dincer A. Do the sealer solvents used affect apically extruded debris in retreatment? J Endod 2015;41:1507-1509.ArticlePubMed
- 44. Bayram E, Dalat D, Bayram M. Solubility evaluation of different root canal sealing materials. J Contemp Dent Pract 2015;16:96-100.ArticlePubMed
REFERENCES
Figure 1
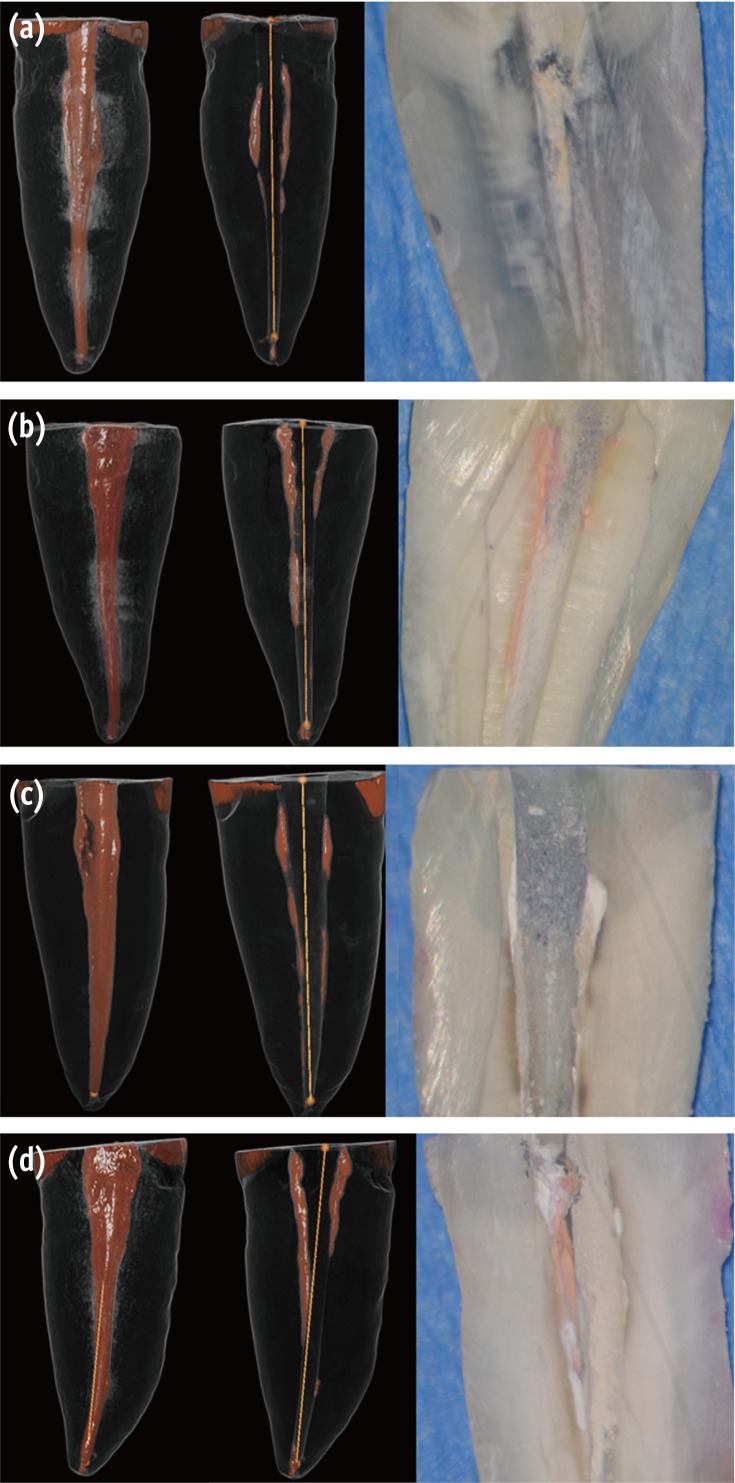
Visualization of residual sealer after retreatment. Micro-CT scans of obturated canals with (a) gutta-percha and AH Plus retreated with chloroform; (b) gutta-percha and AH Plus retreated without chloroform; (c) gutta-percha and BC Sealer retreated with chloroform; (d) gutta-percha and BC Sealer retreated without chloroform retreatment. The left-most images are representative 3D renderings of the filled canals, while the adjacent images are the same teeth following retreatment. Black, root surface; white and orange, obturation material. The right-most images are the corresponding longitudinal sections of these teeth. Micro-CT, micro-computed tomography; BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA); 3D, 3 dimensional.
Figure 2
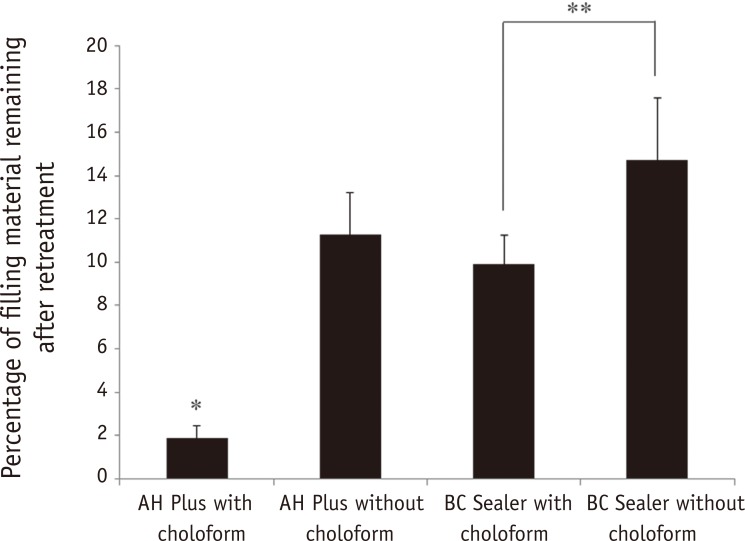
Percentage of residual filling material in the entire length of root canal. The differences in the percentage of residual root canal filling were statistically significant between the AH Plus with chloroform and the other groups (*p ≤ 0.05). The BC Sealer with chloroform group was significantly different from the BC Sealer without chloroform group (**p ≤ 0.05). BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA).
Figure 3
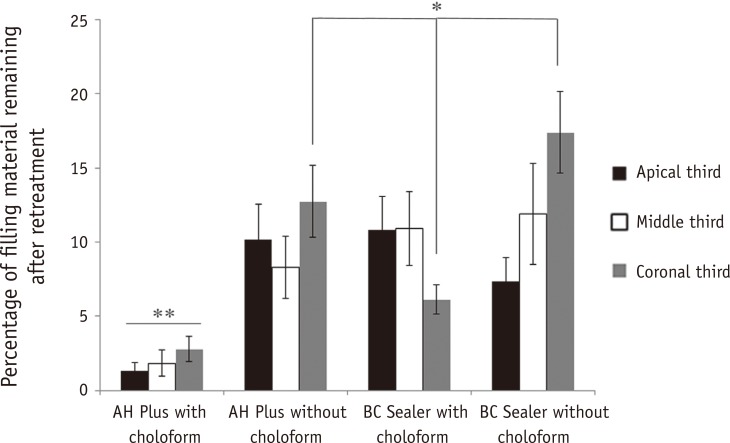
Percentage of residual filling material of apical third compared with middle and coronal third of canals. The differences in the percentage of residual root canal filling were statistically significant between the AH Plus with chloroform and the other groups (**p ≤ 0.05) and between the BC Sealer group retreated with chloroform and the AH Plus and BC Sealer groups that were not retreated with chloroform (*p ≤ 0.05). BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA).
Table 1
Ability to regain patency and re-establish working length during retreatment for the different groups
| Group 1A (%) | Group 1B (%) | Group 2A (%) | Group 2B (%) | |
|---|---|---|---|---|
| Patency Regained | 100 | 100 | 93 | 14* |
| WL re-established | 100 | 100 | 93 | 93 |
Mean volume percentages (%) of the remaining filling material are shown in the table. For patency regained, a statistically significant difference was found between Group 2B and each of the remaining groups (*p < 0.001). Patency could be regained in only 14% of cases that were obturated with BC Sealer and retreated without chloroform. For WLs there were no significant differences between the groups. WL, working length.
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Retreatment of Bioceramic Sealers Using a Novel Solvent: Dissolution, Patency, and Dentinal Effects
Jemma Hanson, Michelle Wu, Ajay Shakya, Ryan Walsh, Poorya Jalali
Journal of Endodontics.2026; 52(2): 279. CrossRef - In Vitro and Ex Vivo Evaluation of a Novel Solvent for Tricalcium Silicate-based Sealers
David Colmenar, Saaya Sakoda, Tanguy Terlier, Takashi Komabayashi, Timothy Kirkpatrick, Ji Wook Jeong
Journal of Endodontics.2026; 52(3): 436. CrossRef - Laser-activated Versus Sonic-activated Irrigation for Removing Residual Filling Materials in Mandibular Molars: A Micro–Computed Tomography Study
Yuhong Lin, Fabricio Teixeira, Jianing He, Megan Yamaguchi, Alexander Huynh, Poorya Jalali
Journal of Endodontics.2026; 52(6): 1016. CrossRef - Effect of Bioceramic-Based Obturation Techniques on the Amount of Residual Filling Material after Retreatment: An In Vitro Study
Sara Wael Nour, Abeer Abd Elhakim Elgendy, Amr Ahmed Bayoumi, Kusai Baroudi, Mohamed Ahmed Elsayed
European Journal of Dentistry.2026;[Epub] CrossRef - Effect of Endodontic Sealers on the Bond Strength of Glass Fibre Posts: A Systematic Review
Thiago Bessa Marconato Antunes, Juliana D. Bronzato, Vanessa Gallego Arias Pecorari, Jennifer Santos Pereira, Talita Tartari, Adriana de Jesus Soares, Brenda P. F. A. Gomes, Marina Angélica Marciano
Australian Endodontic Journal.2026;[Epub] CrossRef - Cone-beam computed tomography analysis of the retrievability of bioceramic-based obturating material from the root canals using ultrasonics and diode laser: An in vitro study
Aditi Paliwal, Suparna Ganguly Saha, Rolly S. Agarwal, Manasi Kewlani, Shakti Singh Meena, Katya Pandey
Endodontology.2026;[Epub] CrossRef - Retreatability of root canals filled with gutta percha and a novel bioceramic sealer- a scanning electron microscopy study
DSV Sindhuja, Prashant Bhasin, Hemanshi Kumar, Alfredo Iandolo, Dina Abdellatif, Lubna Ahmad, Alfonso Acerra
Journal of Oral Biology and Craniofacial Research.2026; 16(4): 101488. CrossRef - The effect of different bioceramic root canal sealer removal protocols on the bond strength of composite to coronal dentin in diabetic and non-diabetic patients: an ex vivo study
Arzu Şahin Mantı, Cemile Kedici Alp
BMC Oral Health.2025;[Epub] CrossRef - Influence of the Filling Technique on Endodontic Retreatment in Curved Mesial Canals of Mandibular Molars: An In Vitro Study
Felipe Andretta Copelli, Lisa Yurie Oda, Renata Maira de Souza Leal, Clarissa Teles Rodrigues, Marco Antonio Hungaro Duarte, Bruno Cavalini Cavenago
Journal of Endodontics.2025; 51(6): 755. CrossRef - Efficacy of irrigation activation methods in removal of bioceramic-based sealer in retreatment
Büşra Nur Cıkrık, Selen İnce Yusufoğlu
Odontology.2025; 113(3): 1119. CrossRef - Patterns and Practices in the Use of Endodontic Materials: Insights from Romanian Dental Practices
Diana Marian, Ramona Amina Popovici, Iustin Olariu, Dana Emanuela Pitic (Cot), Maria-Monica Marta, Ioana Veja (Ilyes)
Applied Sciences.2025; 15(3): 1272. CrossRef - Microcracks induced by XP-endo retreatment system in root canals filled with bioceramic sealer: A micro-computed tomographic analysis
Sarah M. Alkahtany
The Saudi Dental Journal.2025;[Epub] CrossRef - Retrieval of AH Plus Bioceramic and Ceraseal Versus AH Plus in Endodontic Retreatment
Eurok Shim, Jee Woo Son, Jiyoung Kwon, Hyun-Jung Kim, Ji-Hyun Jang, Seok Woo Chang, Soram Oh
Journal of Clinical Medicine.2025; 14(6): 1826. CrossRef - Comparative Evaluation of Retreatability of Two Bioceramic Sealers and Epoxy Resin Sealer with Two Different File Systems: An In Vitro Cone Beam Computed Tomography Volumetric Analysis
Rashmi Nair, Riya Jain, Neetu Maurya, Neha D Singh, Labdhi Maloo, Shanu Khan
World Journal of Dentistry.2025; 16(1): 56. CrossRef - Comparative evaluation of the efficacy of three different retreatment files in removing root canal filling material: An In vitro confocal microscopy study
Meghna Sarah Abraham, Aravind R. Kudva, Prathap M. S. Nair, Shravan Kini, Samreena Kalander, Faseeh Muhammed Bin Farookh
Endodontology.2025; 37(2): 136. CrossRef - Comparative Evaluation of Removal of Gutta Percha and Bioceramic Sealer Using EdgeFile‐XR and ProTaper Universal Retreatment Files: Micro‐Computed Tomography Study
Sindhuja Srirama, Sooriaprakas Chandrasekaran, Buvaneshwari Arul, Velmurugan Natanasabapathy
Australian Endodontic Journal.2025; 51(2): 358. CrossRef - Achieving Patency in Straight Canals Obturated with AH Plus Bioceramic Sealer: An Ex Vivo Study
Inês Ferreira, Beatriz Fernandes, Ana Cristina Braga, Maria Ascensão Lopes, Irene Pina-Vaz
Applied Sciences.2025; 15(11): 5855. CrossRef - Cleaning protocols to enhance bond strength of fiberglass posts on root canals filled with bioceramic sealer: an in vitro comparative study
Thiago Bessa Marconato Antunes, Juliana Delatorre Bronzato, Joice Graciani, Ana Cristina Padilha Janini, Rocharles Cavalcante Fontenele, Francisco Haiter Neto, Brenda Paula Figueiredo de Almeida Gomes, Marina Angélica Marciano da Silva
Restorative Dentistry & Endodontics.2025; 50(2): e20. CrossRef - Surface Alterations of Ni‐Ti Files After Retreatment of Root Canals Filled With Different Sealers: AFM and SEM Study
Duygu Aksoy, Sibel Koçak, Mustafa Murat Koçak, Baran Can Sağlam
Microscopy Research and Technique.2025; 88(10): 2704. CrossRef - Resistance of gutta-percha and calcium silicate-based sealer to dislocation after non-surgical root canal retreatment
Reza Mahjourianqomi, Noushin Shokouhinejad, Fatemeh Hamidzadeh, Pegah Sarraf
BMC Oral Health.2025;[Epub] CrossRef - The Impact of Different Access Cavity Designs on the Retreatment Procedure of Single Oval Canals Using Reciprocating File Systems: An Ex-Vivo Study
Samia Elsherief, Sahar M Elmarsafy, Nora Abdelgawad, Haytham Sabri Abdul Hameed Jaha
The Open Dentistry Journal.2025;[Epub] CrossRef - Retrievability of NeoMTA 2 vs AH Plus Sealer from Retreated Mesial Canals of Mandibular First Molars: A Microcomputed Tomography Ex Vivo Study
Mey A Al-Habib, Mona Alsulaiman
The Journal of Contemporary Dental Practice.2025; 26(5): 493. CrossRef - Efficacy of self-adjusting file and E18 isthmus ultrasonic tip as supplementary instruments in removal of gutta-percha and bioceramic sealer from oval canals in endodontic retreatment: A cone-beam computed tomography study
Joel George Thomas Madolil, I. Sujatha, K. B. Jayalakshmi, Deena Elizabeth, B. Sowmya, Bhargavi Krishnaraj
Endodontology.2025; 37(3): 276. CrossRef - Calcium silicate-based sealers remnants in isthmuses of mesial roots of mandibular molars: an in vitro evaluation
David Saldanha de Brito Alencar, Ana Cristina Padilha Janini, Lauter Eston Pelepenko, Brenda Fornazaro Moraes, Francisco Haiter Neto, Marco Antonio Hungaro Duarte, Marina Angélica Marciano
Restorative Dentistry & Endodontics.2025; 50(3): e25. CrossRef - Thermal Behaviour of Teeth With Internal Root Resorption During Obturation and Enhancing Thermal Simulations: A Finite-Element Analysis
Alper Kabakci, Ayca Yilmaz, Dilek Helvacioglu-Yigit, Nawar Naguib Nawar, Hyeon-Cheol Kim
International Dental Journal.2025; 75(6): 103903. CrossRef - Assessing Volume of Two Sealers’ Remnants after Reinstrumentation Using 3D Imaging Technology: An In Vitro Comparative Study
Khalel Mutaz Dawod, Raghad Abdulrazzaq Al-Hashimi
The Journal of Contemporary Dental Practice.2025; 26(8): 743. CrossRef - Comparative analysis of the push-out bond strength of fiber posts: Immediate vs. delayed post-space preparation with two obturation techniques
Weilin Long, Xiongjun Xu, Li Tang, Hongwei Jiang, Yihua Huang, Miriam Fatima Zaccaro Scelza
PLOS One.2025; 20(10): e0333880. CrossRef - Removal efficacy of two different root canal sealers in retrograde cavities: a micro-CT study
Özge Başar, Ahter Şanal Çıkman, Cangül Keskin
BMC Oral Health.2025;[Epub] CrossRef - Marginal adaptation of customized gutta percha cone with calcium silicate based sealer versus MTA and biodentine apical plugs in simulated immature permanent teeth (an in vitro study)
Mary M. Mina, Sybel M. Moussa, Mahmoud R. Aboelseoud
BMC Oral Health.2024;[Epub] CrossRef - Retreatability of Bioceramic-Filled Teeth: Comparative Analysis of Single-Cone and Carrier-Based Obturation Using a Reciprocating Technique
Andrea Spinelli, Fausto Zamparini, Jacopo Lenzi, Davide Carboni, Maria Giovanna Gandolfi, Carlo Prati
Applied Sciences.2024; 14(15): 6444. CrossRef - Retreatability of calcium silicate-based sealers based on micro-computed tomographic evaluation − A systematic review
Sundus Mohammed Bukhary
The Saudi Dental Journal.2024; 36(10): 1278. CrossRef - Bioceramic and Resin-Based Sealers Removal Using XP-Endo Finisher: A Scanning Electron Microscopy Study
Meriem Fejjeri, Kawther Bel Haj Salah, Sabra Jaafoura, Saida Sahtout
European Journal of General Dentistry.2024; 13(02): 110. CrossRef - Comparative Evaluation of the Efficacy of Different Solvents on the Removal of Endodontic Bioceramic Sealers: An In vitro Study
Ruaa A. Alamoudi
Journal of the International Clinical Dental Research Organization.2024; 16(2): 126. CrossRef - The Efficiency of Different Supplementary Irrigation Techniques After Nickel-Titanium Rotary System in Endodontic Retreatment
Selin Goker Kamali, Dilek Turkaydin
European Journal of Therapeutics.2024; 30(6): 859. CrossRef - Evaluation of canal patency and cleanliness following retreatment of bioceramic sealer‐obturated root canals using three different irrigant activation protocols
Daiasharailang Lyngdoh, Sharique Alam, Huma Iftekhar, Surendra Kumar Mishra
Australian Endodontic Journal.2024; 50(3): 475. CrossRef - Optimizing Non-surgical Endodontic Retreatment: A 3D CBCT Quantification of Root Canal Bioceramic Filling Material Removal
Kostadin Zhekov, Vesela Stefanova
The Open Dentistry Journal.2024;[Epub] CrossRef - The Effect of Different Obturation Techniques Using Different Root Canal Sealers on the Residual Filling Material After Retreatment Procedures
M Sarı, K Yılmaz
Nigerian Journal of Clinical Practice.2024; 27(2): 174. CrossRef - Dentinal Tubule Penetrability and Bond Strength of Two Novel Calcium Silicate-Based Root Canal Sealers
Karissa Shieh, Jack Yang, Elsa Heng Zhu, Ove Andreas Peters, Sepanta Hosseinpour
Materials.2023; 16(9): 3309. CrossRef - Efficiency of diode laser and ultrasonic‐activated irrigation in retreatment of gutta percha and bioceramic sealer: An in vitro study
Rahaf A. Almohareb, Reem M. Barakat, Noor Aljarallah, Halah Mudhish, Amjaad Almutairi, Fahda N. Algahtani
Australian Endodontic Journal.2023; 49(2): 318. CrossRef - The efficiency of different irrigation activation techniques in the removal of calcium silicate‐based endodontic sealer from artificially created groove
Meltem Sümbüllü, Afzal Ali, Mine Büker, Hakan Arslan
Australian Endodontic Journal.2023; 49(S1): 238. CrossRef - Global survey of endodontic practice and adoption of newer technologies
Monique Charlene Cheung, Ove Andreas Peters, Peter Parashos
International Endodontic Journal.2023; 56(12): 1517. CrossRef - Efficiency of the new reciprocating and rotary systems with or without ultrasonics in removing root-canals filling with calcium silicate-based sealer (MTA)
Ahmad A. Madarati, Aya M. N. Sammani, Ahmad A. Alnazzawi, Ali Alrahlah
BMC Oral Health.2023;[Epub] CrossRef - Effect of endodontic sealers on push-out bond strength of CAD-CAM or prefabricated fiber glass posts
Andréa Pereira de Souza PINTO, Fabiana Mantovani Gomes FRANÇA, Roberta Tarkany BASTING, Cecilia Pedroso TURSSI, José Joatan RODRIGUES JÚNIOR, Flávia Lucisano Botelho AMARAL
Brazilian Oral Research.2023;[Epub] CrossRef - Microcomputed tomographic analysis of the efficiency of two retreatment techniques in removing root canal filling materials from mandibular incisors
Xueqin Yang, Ye Wang, Mengzhen Ji, Yanyao Li, Hao Wang, Tao Luo, Yuan Gao, Ling Zou
Scientific Reports.2023;[Epub] CrossRef - Effectiveness of Two Endodontic Instruments in Calcium Silicate-Based Sealer Retreatment
Antoun Farrayeh, Samar Akil, Ammar Eid, Valentina Macaluso, Davide Mancino, Youssef Haïkel, Naji Kharouf
Bioengineering.2023; 10(3): 362. CrossRef - Clinical applications of calcium silicate‐based materials: a narrative review
S Küçükkaya Eren
Australian Dental Journal.2023;[Epub] CrossRef - Retreatability of Bioceramic Sealer Using One Curve Rotary File Assessed by Microcomputed Tomography
Dina G Mufti, Saad A Al-Nazhan
The Journal of Contemporary Dental Practice.2022; 22(10): 1175. CrossRef - Medium- and Long-Term Re-Treatment of Root Canals Filled with a Calcium Silicate-Based Sealer: An Experimental Ex Vivo Study
Giulia Bardini, Elisabetta Cotti, Terenzio Congiu, Claudia Caria, Davide Aru, Montse Mercadè
Materials.2022; 15(10): 3501. CrossRef - An in vitro comparative evaluation of retreatability of a bioceramic and resin sealer using cone-beam computed tomography analysis
Sumit Sharma, Ramya Raghu, Ashish Shetty, Subhashini Rajasekhara, Harika Lakshmisetty, G. Bharath
Endodontology.2022; 34(3): 173. CrossRef - Removal of the Previous Root Canal Filling Material for Retreatment: Implications and Techniques
Flávio R. F. Alves, Isabela N. Rôças, José C. Provenzano, José F. Siqueira
Applied Sciences.2022; 12(20): 10217. CrossRef - Efficacy of retreatment NiTi files for root canals filled with calcium silicate-based sealer
Jae-Yun Hyun, Kyung-Mo Cho, Se-Hee Park, Yoon Lee, Yoon-Joo Lee, Jin-Woo Kim
Journal of Dental Rehabilitation and Applied Science.2022; 38(4): 213. CrossRef - Dissolving efficacy of xylene on epoxy resin-based and bioceramic-based root canal sealers
Cindy Willie
Scientific Dental Journal.2022; 6(1): 32. CrossRef - Comparison of the efficacy of three different supplementary cleaning protocols in root-filled teeth with a bioceramic sealer after retreatment—a micro-computed tomographic study
Chanakarn Sinsareekul, Sirawut Hiran-us
Clinical Oral Investigations.2022; 26(4): 3515. CrossRef - The efficacy of different sealer removal protocols on the microtensile bond strength of adhesives to a bioceramic sealer-contaminated dentin
ZG Bek Kurklu, HO Yoldas
Nigerian Journal of Clinical Practice.2022; 25(3): 336. CrossRef - A micro-computed tomographic analysis of obturation quality and retreatability of an epoxy resin-based sealer
Roula S. ABIAD, Prasanna NEELAKANTAN, Ivan BUSCEMA, Islam A. ALI, Gianluca CONTE, Giusy R. M. LA ROSA, Luigi GENERALI, Marco CICCIÙ, Eugenio PEDULLÀ
Minerva Dental and Oral Science.2022;[Epub] CrossRef - Tricalcium silicate cement sealers
Anita Aminoshariae, Carolyn Primus, James C. Kulild
The Journal of the American Dental Association.2022; 153(8): 750. CrossRef - Antimicrobial effectiveness of root canal sealers againstEnterococcus faecalis
Paola Castillo-Villagomez, Elizabeth Madla-Cruz, Fanny Lopez-Martinez, Idalia Rodriguez-Delgado, Jorge Jaime Flores-Treviño, Guadalupe Ismael Malagon-Santiago, Myriam Angelica de La Garza-Ramos
Biomaterial Investigations in Dentistry.2022; 9(1): 47. CrossRef - Perspective of endodontic sealers based on calcium silicate
Yong-Bum Cho
Korean Journal of Dental Materials.2022; 49(4): 243. CrossRef - Efficiency of reciprocating systems reciprocated at different angles in removing root-canals fillings with an MTA-type sealer: an Ex-vivo study
Ahmad A. Madarati, Aya M. N. Sammani, Ahmad A. Alnazzawi, Ali Alrahlah, Eugenio Pedullà
BMC Oral Health.2022;[Epub] CrossRef - Comparative Evaluation of the Depth of Penetration and Persistence of Sealer Residues in Retreated Dentinal Tubules
Jeslee A Jose, Karthik V Thomas, Prathap MS Nair, Vivian F D'Costa, Nithin Suvarna
World Journal of Dentistry.2022; 13(6): 647. CrossRef - Calcium Silicate-Based Root Canal Sealers: A Narrative Review and Clinical Perspectives
Germain Sfeir, Carla Zogheib, Shanon Patel, Thomas Giraud, Venkateshbabu Nagendrababu, Frédéric Bukiet
Materials.2021; 14(14): 3965. CrossRef - The effect of two endodontic sealers and interval before post-preparation and cementation on the bond strength of fiber posts
He Yuanli, Wu Juan, Ji Mengzhen, Chen Xuan, Xiong Kaixin, Yang Xueqin, Qiao Xin, Hu Hantao, Gao Yuan, Zou Ling
Clinical Oral Investigations.2021; 25(11): 6211. CrossRef - Comparison of the efficacy of laser-activated and ultrasonic-activated techniques for the removal of tricalcium silicate-based sealers and gutta-percha in root canal retreatment: a microtomography and scanning electron microscopy study
Ruiqi Yang, Yuqing Han, Zhaohui Liu, Zhezhen Xu, Hongyan Liu, Xi Wei
BMC Oral Health.2021;[Epub] CrossRef - Improvement of the efficacy of endodontic solvents by ultrasonic agitation
Inês Ferreira, Ana Cristina Braga, Maria Ascensão Lopes, Irene Pina-Vaz
The Saudi Dental Journal.2021; 33(1): 39. CrossRef - Retreatability of BC Sealer and AH Plus root canal sealers using new supplementary instrumentation protocol during non-surgical endodontic retreatment
Bruno Monguilhott Crozeta, Fabiane Carneiro Lopes, Renato Menezes Silva, Yara Teresinha Correa Silva-Sousa, Letícia Freiria Moretti, Manoel Damião Sousa-Neto
Clinical Oral Investigations.2021; 25(3): 891. CrossRef - Retrievability of bioceramic-based sealers in comparison with epoxy resin-based sealer assessed using microcomputed tomography: A systematic review of laboratory-based studies
Buvaneshwari Arul, Aswathi Varghese, Anisha Mishra, Subashini Elango, Sairathna Padmanaban, Velmurugan Natanasabapathy
Journal of Conservative Dentistry.2021; 24(5): 421. CrossRef - Positive and negative properties of four endodontic sealant groups: a systematic review
E. V. Chestnyh, I. O. Larichkin, M. V. Iusufova, D. I. Oreshkina, E. I. Oreshkina, V. S. Minakova, S. V. Plekhanova
Kuban Scientific Medical Bulletin.2021; 28(3): 130. CrossRef - Comparative Evaluation of Retreatability of Calcium Silicate-Based Root Canal Sealers and Epoxy Resin-Based Root Canal Sealers in Curved Canals-An In-Vitro Micro-Ct Analysis
MV Mavishna, Kondas Vijay Venkatesh
Indian Journal of Dental Research.2021; 32(1): 79. CrossRef - Micro CT pilot evaluation of removability of two endodontic sealers
David Colmenar, Tenzin Tamula, Qiang Zhu, Chul Ahn, Carolyn Primus, Takashi Komabayashi
Journal of Oral Science.2021; 63(4): 306. CrossRef - Efficacy of Reciprocating Instruments in the Removal of Bioceramic and Epoxy Resin-Based Sealers: Micro-CT Analysis
Marko Rajda, Ivana Miletić, Gorana Baršić, Silvana Jukić Krmek, Damir Šnjarić, Anja Baraba
Materials.2021; 14(21): 6670. CrossRef - Comparison of Obturation Quality between Calcium Silicate-Based Sealers and Resin-Based Sealers for Endodontic Re-treatment
Hye-Ryeon Jin, Young-Eun Jang, Yemi Kim
Materials.2021; 15(1): 72. CrossRef - Micro-computed tomographic evaluation of the flow and filling ability of endodontic materials using different test models
Fernanda Ferrari Esteves Torres, Juliane Maria Guerreiro-Tanomaru, Gisselle Moraima Chavez-Andrade, Jader Camilo Pinto, Fábio Luiz Camargo Villela Berbert, Mario Tanomaru-Filho
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - Evaluation of Passive Ultrasonic Irrigation and GentleWave System as Adjuvants in Endodontic Retreatment
Bruno Monguilhott Crozeta, Letícia Chaves de Souza, Yara Teresinha Correa Silva-Sousa, Manoel D. Sousa-Neto, David Enrique Jaramillo, Renato Menezes Silva
Journal of Endodontics.2020; 46(9): 1279. CrossRef - Micro-computed tomographic evaluation of a new system for root canal filling using calcium silicate-based root canal sealers
Mario Tanomaru-Filho, Fernanda Ferrari Esteves Torres, Jader Camilo Pinto, Airton Oliveira Santos-Junior, Karina Ines Medina Carita Tavares, Juliane Maria Guerreiro-Tanomaru
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - Micro–computed Tomographic Assessment of Supplementary Cleaning Techniques for Removing Bioceramic Sealer and Gutta-percha in Oval Canals
Andrea Volponi, Rina Andréa Pelegrine, Augusto Shoji Kato, Carolina Pessoa Stringheta, Ricardo Tadeu Lopes, Aline Saddock de Sá Silva, Carlos Eduardo da Silveira Bueno
Journal of Endodontics.2020; 46(12): 1901. CrossRef - Reciproc and Reciproc Blue in the removal of bioceramic and resin-based sealers in retreatment procedures
Kaline Romeiro, Andressa de Almeida, Marcely Cassimiro, Luciana Gominho, Eugênia Dantas, Nayane Chagas, Christianne Velozo, Laila Freire, Diana Albuquerque
Clinical Oral Investigations.2020; 24(1): 405. CrossRef - Micro-CT analysis of dentinal microcracks on root canals filled with a bioceramic sealer and retreated with reciprocating instruments
Andressa Almeida, Kaline Romeiro, Marcely Cassimiro, Luciana Gominho, Eugênia Dantas, Silmara Silva, Diana Albuquerque
Scientific Reports.2020;[Epub] CrossRef - An international survey on the use of calcium silicate-based sealers in non-surgical endodontic treatment
M. Guivarc’h, C. Jeanneau, T. Giraud, L. Pommel, I. About, A.A. Azim, Frédéric Bukiet
Clinical Oral Investigations.2020; 24(1): 417. CrossRef - Efficacy and Cytotoxicity of Binary Mixtures as Root Canal Filling Solvents
Inês Ferreira, Liliana Grenho, Pedro Gomes, Ana Cristina Braga, Maria Helena Fernandes, Maria Ascensão Lopes, Irene Pina-Vaz
Materials.2020; 13(14): 3237. CrossRef - Comprehensive review of current endodontic sealers
Takashi KOMABAYASHI, David COLMENAR, Nicholas CVACH, Aparna BHAT, Carolyn PRIMUS, Yohji IMAI
Dental Materials Journal.2020; 39(5): 703. CrossRef - Effect of ultrasonic cleaning on the bond strength of fiber posts in oval canals filled with a premixed bioceramic root canal sealer
Fernando Peña Bengoa, Maria Consuelo Magasich Arze, Cristobal Macchiavello Noguera, Luiz Felipe Nunes Moreira, Augusto Shoji Kato, Carlos Eduardo Da Silveira Bueno
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - Retreatment efficacy of hydraulic calcium silicate sealers used in single cone obturation
M. Garrib, J. Camilleri
Journal of Dentistry.2020; 98: 103370. CrossRef - Influence of endodontic sealers with different chemical compositions on bond strength of the resin cement/glass fiber post junction to root dentin
Isadora Mello Vilarinho Soares, Bruno Monguilhott Crozeta, Rodrigo Dantas Pereira, Ricardo Gariba Silva, Antonio Miranda da Cruz-Filho
Clinical Oral Investigations.2020; 24(10): 3417. CrossRef - Micro-computed tomography evaluation of root canal filling quality with apical negative pressure
Jinxia Li, Brian E. Bergeron, Jing Chao, Ting Xu, Franklin R. Tay, Bing Fan
Journal of Dentistry.2020; 100: 103431. CrossRef - Comparative Evaluation of Retreatability of Endodontically Treated Teeth using AH 26, Fluoride Varnish and Mineral Trioxide Aggregate-based Endodontic Sealers
Zakiyeh Donyavi, Abbas Shokri, Zahra Pakseresht, Leili Tapak, Alireza Falahi, Hadiseh Abbaspourrokni
The Open Dentistry Journal.2019; 13(1): 183. CrossRef - Bioactive Glass-Based Endodontic Sealer as a Promising Root Canal Filling Material without Semisolid Core Materials
Ayako Washio, Takahiko Morotomi, Shinji Yoshii, Chiaki Kitamura
Materials.2019; 12(23): 3967. CrossRef - Micro‐CT evaluation of the removal of root fillings using the ProTaper Universal Retreatment system supplemented by the XP‐Endo Finisher file
H. Aksel, S. Küçükkaya Eren, S. Askerbeyli Örs, A. Serper, M. Ocak, H. H. Çelik
International Endodontic Journal.2019; 52(7): 1070. CrossRef - Retreatability of two hydraulic calcium silicate‐based root canal sealers using rotary instrumentation with supplementary irrigant agitation protocols: a laboratory‐based micro‐computed tomographic analysis
E. Pedullà, R. S. Abiad, G. Conte, K. Khan, K. Lazaridis, E. Rapisarda, P. Neelakantan
International Endodontic Journal.2019; 52(9): 1377. CrossRef - A micro-computed tomographic study of remaining filling materials of two bioceramic sealers and epoxy resin sealer after retreatment
KyungJae Kim, Da Vin Kim, Sin-Young Kim, SungEun Yang
Restorative Dentistry & Endodontics.2019;[Epub] CrossRef - Endodontic sealers based on calcium silicates: a systematic review
David Donnermeyer, Sebastian Bürklein, Till Dammaschke, Edgar Schäfer
Odontology.2019; 107(4): 421. CrossRef - Ex Vivo Evaluation of Endodontic Retreatment Using Four Rotary File Systems and Hand Hedstrom Files in the Removal of Gutta-percha and MTA-based Salicylate Resin Sealer
Vasundhara Shivanna, Nerulgundi M Dhanyakumar, Sushant Sharma
CODS - Journal of Dentistry.2018; 10(2): 29. CrossRef - Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part II: other clinical applications and complications
M. Torabinejad, M. Parirokh, P. M. H. Dummer
International Endodontic Journal.2018; 51(3): 284. CrossRef - Effect of different endodontic sealers and time of cementation on push-out bond strength of fiber posts
Danielle Araújo Vilas-Boas, Renata Grazziotin-Soares, Diego Machado Ardenghi, José Bauer, Patrícia Oliveira de Souza, George Táccio de Miranda Candeiro, Etevaldo Matos Maia-Filho, Ceci Nunes Carvalho
Clinical Oral Investigations.2018; 22(3): 1403. CrossRef
 ePub Link
ePub Link Cite
CiteRetreatability of two endodontic sealers, EndoSequence BC Sealer and AH Plus: a micro-computed tomographic comparison
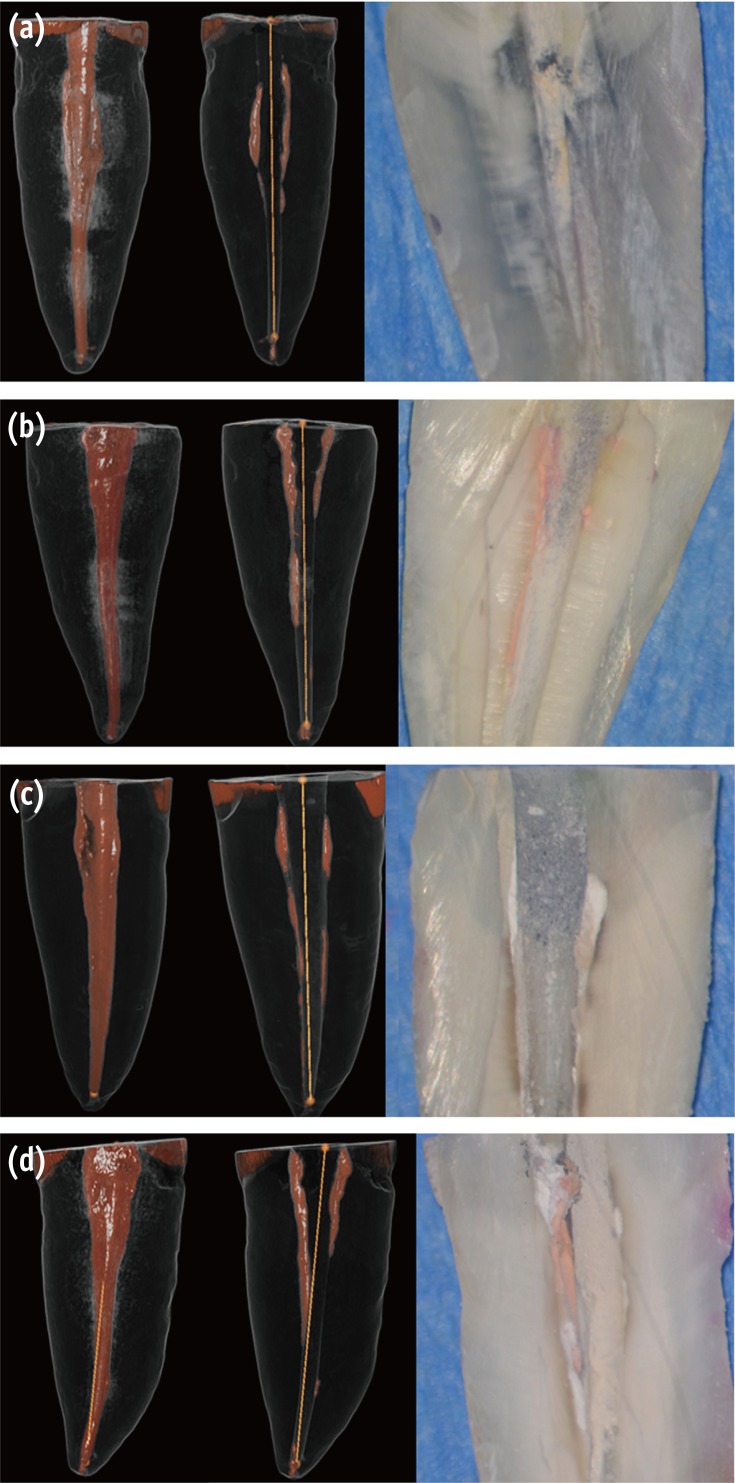
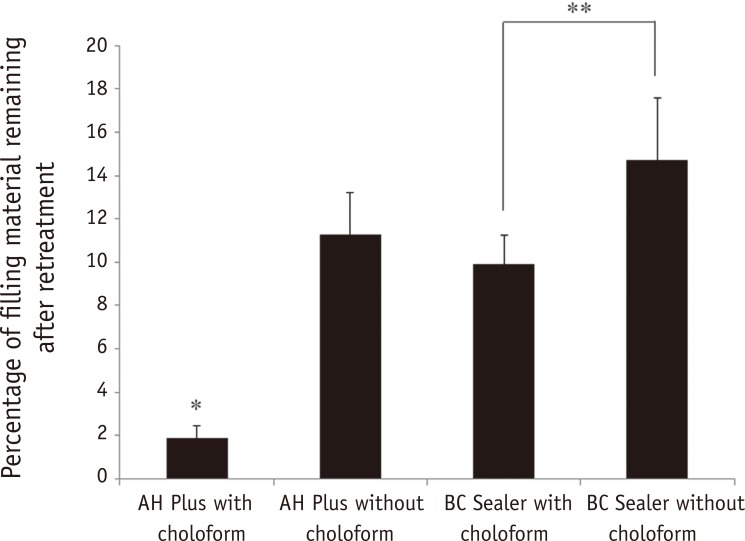

Figure 1 Visualization of residual sealer after retreatment. Micro-CT scans of obturated canals with (a) gutta-percha and AH Plus retreated with chloroform; (b) gutta-percha and AH Plus retreated without chloroform; (c) gutta-percha and BC Sealer retreated with chloroform; (d) gutta-percha and BC Sealer retreated without chloroform retreatment. The left-most images are representative 3D renderings of the filled canals, while the adjacent images are the same teeth following retreatment. Black, root surface; white and orange, obturation material. The right-most images are the corresponding longitudinal sections of these teeth. Micro-CT, micro-computed tomography; BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA); 3D, 3 dimensional.
Figure 2 Percentage of residual filling material in the entire length of root canal. The differences in the percentage of residual root canal filling were statistically significant between the AH Plus with chloroform and the other groups (*p ≤ 0.05). The BC Sealer with chloroform group was significantly different from the BC Sealer without chloroform group (**p ≤ 0.05). BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA).
Figure 3 Percentage of residual filling material of apical third compared with middle and coronal third of canals. The differences in the percentage of residual root canal filling were statistically significant between the AH Plus with chloroform and the other groups (**p ≤ 0.05) and between the BC Sealer group retreated with chloroform and the AH Plus and BC Sealer groups that were not retreated with chloroform (*p ≤ 0.05). BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA).
Figure 1
Figure 2
Figure 3
Retreatability of two endodontic sealers, EndoSequence BC Sealer and AH Plus: a micro-computed tomographic comparison
Ability to regain patency and re-establish working length during retreatment for the different groups
| Group 1A (%) | Group 1B (%) | Group 2A (%) | Group 2B (%) | |
|---|---|---|---|---|
| Patency Regained | 100 | 100 | 93 | 14* |
| WL re-established | 100 | 100 | 93 | 93 |
Mean volume percentages (%) of the remaining filling material are shown in the table. For patency regained, a statistically significant difference was found between Group 2B and each of the remaining groups (*p < 0.001). Patency could be regained in only 14% of cases that were obturated with BC Sealer and retreated without chloroform. For WLs there were no significant differences between the groups. WL, working length.
Table 1 Ability to regain patency and re-establish working length during retreatment for the different groups
Mean volume percentages (%) of the remaining filling material are shown in the table. For patency regained, a statistically significant difference was found between Group 2B and each of the remaining groups (*

