
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 42(2); 2017 > Article
- Research Article Intraoperative discomfort associated with the use of a rotary or reciprocating system: a prospective randomized clinical trial
- Aline Cristine Gomes1, Adriana Jesus Soares1, Erick M Souza2, Alexandre Augusto Zaia1, Emmanuel João Nogueira Leal Silva3
-
2017;42(2):-145.
DOI: https://doi.org/10.5395/rde.2017.42.2.140
Published online: April 20, 2017
1Department of Restorative Dentistry, Campinas State University (UNICAMP) Piracicaba School of Dentistry, Piracicaba, SP, Brazil.
2Department of Endodontics, Federal University of Maranhão (UFMA), São Luís, MA, Brazil.
3Department of Endodontics, Grande Rio University (UNIGRANRIO) School of Dentistry, Rio de Janeiro, RJ, Brazil.
- Correspondence to Emmanuel João Nogueira Leal da Silva, DDS, MSc, PhD. Associate Professor, Department of Endodontics, Grande Rio University (UNIGRANRIO) School of Dentistry, Rua Herotides de Oliveira, 61/902 Icaraí, Niterói, RJ, Brazil. TEL, +55-21-8357-5757; FAX, +55-21-2610-8439; nogueiraemmanuel@hotmail.com
• Received: October 26, 2016 • Accepted: February 20, 2017
©Copyrights 2017. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,804 Views
- 18 Download
- 9 Crossref
Abstract
-
Objectives The aim of this randomized, controlled, prospective clinical study was to evaluate patients' intraoperative discomfort during root canal preparations in which either multi-file rotary (Mtwo) or single-file reciprocating (Reciproc) systems were used.
-
Materials and Methods Fifty-five adult patients, aged between 25 and 69 years old, with irreversible pulpitis or pulp necrosis participated in this study. Either the mesiobuccal or the distobuccal canals for maxillary molars and either the mesiobuccal or the mesiolingual canals for mandibular molars were randomly chosen to be instrumented with Mtwo multi-file rotary or Reciproc single-file reciprocating systems. Immediately after each canal instrumentation under anesthesia, patient discomfort was assessed using a 1 - 10 visual analog scale (VAS), ranging from ‘least possible discomfort’ (1) to ‘greatest possible discomfort’ (10). The Wilcoxon signed-rank test was used to determine significant differences at p< 0.05.
-
Results Little intraoperative discomfort was found in all cases. No statistically significant differences in intraoperative discomfort between the 2 systems were found (p = 0.660).
-
Conclusions Root canal preparation with multi-file rotary or single-file reciprocating systems had similar and minimal effects on patients' intraoperative discomfort.
Introduction
The recent introduction of single-file reciprocating systems to the market has raised new perspectives for root canal preparation. The reciprocating motion relieves the stress on the instrument by special counterclockwise (cutting action) and clockwise (release of the instrument) movements and therefore increases its resistance to fatigue in comparison to systems with continuous rotary motion.1 Overall, research findings on reciprocating systems have reported a decrease in preparation time, increased cyclic fatigue life, and a similar shaping ability to rotary systems.2,3,4,5,6,7,8 Despite these advantages, during root canal preparation with reciprocating instruments, the clinician can feel a disturbing trepidation associated with a pronounced ‘click sound,’ which raises doubts regarding patients' discomfort during endodontic treatment, especially as a consequence of the kinematics. This might lead the patient to have the sensation that the treated tooth is in danger of fracturing.
This is the background of the current clinical trial, which was conducted to evaluate patients' intraoperative discomfort during root canal instrumentation by rotary (Mtwo, VDW, Munich, Germany) and reciprocating (Reciproc, VDW) systems. The null hypothesis tested was that there would be no difference in patients' intraoperative discomfort between the tested systems.
Materials and Methods
This was a randomized, controlled, single-blinded, split-mouth, prospective clinical study with an equal allocation rate between the groups. This clinical trial was registered in the ISRCTN (registration number, ISRCTN11624674). The Ethics Committee in Research of the Piracicaba Dental School, University of Campinas (FOP-UNICAMP) approved the study with the protocol 058/2015, and written informed consent was obtained from each volunteer. All volunteers invited to participate in this clinical trial were informed of the protocols of the procedures, which were conducted by an endodontist/PhD student, the risks and benefits, and their right to self-determination regarding participation. After signing a written consent form, a copy was delivered to all volunteers.
A Wilcoxon signed-rank test from the t-test family was selected (G*Power 3.1.9.2 for Macintosh; Heinrich-Heine, Düsseldorf, Germany). Using the results of Relvas et al.,9 as a reference, who found no difference in postoperative pain after 24 hours comparing a reciprocating and a rotary system, an effect size of 0.81 was input together with an alpha-error of 0.05 and a power beta of 0.95. The estimation of participants indicated a minimum sample size of 23 individuals in order to achieve 95% confidence for a true difference between the groups.
The inclusion criteria were defined as follows: healthy (American Society of Anesthesiology [ASA] I patients) adults older than 18 years of age who had been admitted to the Endodontics Department of FOP-UNICAMP from January 2015 to December 2015, with a clinical diagnosis of irreversible pulpitis or necrosis in the first or second maxillary and mandibular molars. The clinical diagnosis of asymptomatic irreversible pulpitis was based on an increased response to the cold test with Endo-frost (Coltène-Whaledent, Langenau, Germany) and the presence of deep caries on radiography, extending to the pulp space, without any spontaneous symptoms. Diagnosis of pulp necrosis was based on the absence of response to the cold test after 10 seconds. None of the patients enrolled in this clinical trial were taking any medications that could alter their perception of pain, such as analgesic or nonsteroidal anti-inflammatory drugs. The radiographic findings included the absence of periapical radiolucencies except for a widened periodontal ligament. The mesiobuccal canals or the distobuccal canals for maxillary molars, as well as the mesiobuccal canals or the mesiolingual canals for mandibular molars, were chosen. During the root canal treatment procedure, teeth failing to be treated in a single appointment or patients who discontinued treatment were omitted from the study.
Approximately 190 patients attending consultations each month at the Endodontics Department, which operates for 9 months per year. The recruitment process for this study lasted for 1 year, during which 1,700 patients were estimated to have undergone any procedure. Of these patients, 55 were selected to take part in this clinical trial by meeting the inclusion criteria (Table 1) and signing the consent form. The exclusion criteria also included other endodontic diagnoses such as reversible pulpitis, abscess, retreatment, endodontic treatment in other teeth, patients taking medications that could interfere with the trial, pregnancy, and patients not defined as ASA I (Figure 1).
After local anesthesia using posterior superior alveolar nerve block for maxillary molars and inferior alveolar nerve block for mandibular molars with 2% lidocaine with 1:100,000 epinephrine (Alphacaine, DFL Indústria e Comércio Ltda, Rio de Janeiro, RJ, Brazil), a rubber dam was placed and the access cavity was prepared using sterile diamond burs. If patients recorded any sensation of pain during the procedure, a supplemental injection providing local infiltration with 1.8 mL of 2% lidocaine with 1:100,000 epinephrine was administered.
An initial exploration of the root canals was performed with size 10 K files (VDW), to establish the root canal length using an electronic apex locator (Root ZX II, J. Morita Corp., Tokyo, Japan). Working length (WL) was established by deducting 1 mm from the canal length. Only cases where a size 10 K file went passively and a size 15 K file did not go passively to the WL in both canals - that is, the mesiobuccal and distobuccal canals for the maxillary molars and the mesiobuccal and mesiolingual canals for the mandibular molars - were selected. These cases were classified as narrow and R25 was recommended, according to the manufacturer's protocol. All teeth received both instrumentation protocols (the Mtwo rotary system or the Reciproc reciprocation system). In this way, each patient experienced the 2 different file systems in the same teeth. A web-based program determined the randomized allocation of the instrumentation systems per canal. While the endodontist was not blinded to the allocated file system, patients were kept blinded to the allocation. Instruments were driven with the VDW Silver motor (VDW) according to each manufacturer's instructions.
The Mtwo instruments were used according to the manufacturer's instructions in the following sequence: sizes 10/0.04, 15/0.05, 20/0.06, and 25/0.06. The motor was adjusted to 500 - 600 rpm and 1 N·cm. After 3 gentle in-and-out motion strokes, the instrument was removed from the canal and cleaned until the WL was reached.
Reciproc R25 (size 25/0.08) was introduced into the canal until resistance was felt and then activated in reciprocating motion. The instrument was moved in an apical direction using an in-and-out pecking motion of about 3 mm in amplitude with light apical pressure. After 3 pecking motions, the instrument was removed from the canal, and its flutes were cleaned off. This procedure was performed until the instrument reached the WL.
In both systems, before each file, 2% chlorhexidine gel was inserted into the canal. After each file, the root canals were irrigated with 2 mL of 0.9% sterile saline solution dispensed using a 30 G Max-i-Probe needle (Dentsply-Rinn, Elgin, IL, USA) up to 3 mm from the WL. After canal preparation, an additional rinse with 5 mL of 0.9% saline solution was performed. The total amount of solution used per canal was 20 mL. A final rinse with 5 mL of 17% ethylenediaminetetraacetic acid (EDTA) delivered for 3 minutes, followed by a 5 mL rinse with 0.9% saline solution, was performed for both groups. Then, canals were dried with absorbent paper points (VDW) and filled with gutta-percha (Dentsply, Rio de Janeiro, RJ, Brazil) and Endomethasone N (Septodont, Saint-Maur-des-Fossés Cedex, France) using warm vertical compaction with the continuous-wave technique and gutta-percha backfill. The study was finished when the endodontic treatment was completed in all subjects.
Patient discomfort was assessed using a 1 to 10 visual analog scale (VAS), ranging from ‘no discomfort’ (1) and ‘highest possible discomfort’ (10). The assessment of intraoperative discomfort was conducted immediately after receiving the treatment with each of the instrumentation protocols. The scale was presented to patients after the end of the instrumentation process with each file system.
The findings were recorded in an Excel spreadsheet (Microsoft Corp., Redmond, WA, USA) for statistical evaluation using SPSS software version 19.0 (IBM Corp., Armonk, NY, USA). The Wilcoxon signed-rank test was used to compare the number of cases recorded in each VAS score between the 2 instrumentation systems tested, and univariate analysis of variance was used to investigate the effect of demographic variables (age, gender, and tooth arc) on the VAS scores reported for the Reciproc and Mtwo systems. An alpha-type error of 5% was set as the cut-off level for significance.
Results
In the Reciproc group, the lowest discomfort value reported was 1 and the highest value was 5, while for the Mtwo group, the scores varied from 1 to 4 (Table 2). No patient experienced any adverse event.
No statistically significant difference in intraoperative discomfort between the 2 different instrumentation groups was found (Reciproc, -2.18 ± 1.02; Mtwo -2.24 ± 1.00, p = 0.660). Little intraoperative discomfort was found in all treated cases in both groups.
None of the demographic variables were found to have a statistically significant effect on the scores reported either for the Reciproc system (age, p = 0.788; gender, p = 0.988; tooth arch, p = 0.387) or the Mtwo system (age, p = 0.642; gender, p = 0.853; tooth arch, p = 0.306). The number of patients who described the same degree of discomfort was 29, while 14 patients described more discomfort for the Mtwo system and 12 patients described more discomfort for the Reciproc system.
Discussion
The present study was unable to detect significant differences in intraoperative discomfort during chemomechanical preparation using the Mtwo full-sequence rotary system and the Reciproc single-file reciprocating system. Therefore, the null hypothesis was clearly accepted. A previous study evaluated the influence of rotary versus reciprocating motion on postoperative pain;9 however, to the best of the authors' knowledge, there are no data on intraoperative discomfort evaluating different root canal preparation kinematics. Although it is possible for the clinician to notice that root canal preparation with multi-file rotary and single-file reciprocating mechanisms have marked differences, the results of the present study demonstrate that these differences did not cause pronounced discomfort in patients.
Mtwo and Reciproc are manufactured from different types of NiTi alloy (Mtwo, conventional NiTi; Reciproc, M-Wire). Moreover, ISO size 25 Mtwo and Reciproc files have a slight difference in the taper (0.06 and 0.08, respectively). However, these files have the same cross-sectional design.2 Thus, it is expected that the minute patient discomfort reported in this study was possibly related to the number of files in the rotary system and the reciprocating movement kinematics used during root canal instrumentation with Reciproc.
One of the main concerns about studying discomfort is the subjective nature of this evaluation. Each person's threshold for discomfort is unique and may be remarkably distinct from that of others. For that reason, and to provide a robust methodological comparison, maxillary and mandibular molars with similar buccal and mesial root canals were selected to provide a similar anatomically reliable baseline. This selection allowed performing root canal instrumentation using these 2 systems in the very same tooth using a split-mouth design, thereby reducing the individual subjective bias that naturally occurs in parallel-group designs. Moreover, the schematic of the discomfort evaluation is critical, and it is essential to ensure that the questions will be fully understood by the patients and easily interpreted by researchers. For this, a simple 1-to-10 VAS was used in the feedback evaluation, where 1 represented the ‘least possible discomfort’ and 10 represented the ‘greatest possible discomfort.’ This scale has been used in several clinical studies evaluating postoperative pain. Moreover, there is considerable evidence indicating that the VAS has advantages over other methods in terms of feasibility and reliability.10,11,12
Postoperative pain related to root canal instrumentation has been reported to vary from low to high incidence.13,14,15,16,17,18,19 The methodological differences related to preoperative pain, variability in protocols, and differences in the collection of clinical findings may explain this variation. In the present study, rather than postoperative pain, intraoperative discomfort was evaluated, which makes comparison among studies non-reliable. Moreover, the intraoperative evaluation is a singular study condition that may make irrelevant some demographic aspects, such as pre-treatment diagnosis, age, and gender of the patients. Intraoperative discomfort was found to be low for both the Reciproc and Mtwo systems, regardless of demographic factors.
Conclusions
Based on the findings of the present study, it can be concluded that root canal preparations with the full-sequence Mtwo rotary system or the single-file Reciproc system had a similar, and small, effect on intraoperative discomfort.
Acknowledgement
This work was supported by the CNPq process no. 305675/3013-3.
- 1. Yared G. Canal preparation using only one NiTi rotary instrument: preliminary observations. Int Endod J 2008;41:339-344.ArticlePubMed
- 2. Lopes HP, Elias CN, Vieira MV, Siqueira JF Jr, Mangelli M, Lopes WS, Vieira VT, Alves FR, Oliveira JC, Soares TG. Fatigue life of Reciproc and Mtwo instruments subjected to static and dynamic tests. J Endod 2013;39:693-696.ArticlePubMed
- 3. da Frota MF, Espir CG, Berbert FL, Marques AA, Sponchiado-Junior EC, Tanomaru-Filho M, Garcia LF, Bonetti-Filho I. Comparison of cyclic fatigue and torsional resistance in reciprocating single-file systems and continuous rotary instrumentation systems. J Oral Sci 2014;56:269-275.ArticlePubMed
- 4. Kiefner P, Ban M, De-Deus G. Is the reciprocating movement per se able to improve the cyclic fatigue resistance of instruments? Int Endod J 2014;47:430-436.ArticlePubMed
- 5. Plotino G, Grande NM, Porciani PF. Deformation and fracture incidence Reciproc instruments: a clinical evaluation. Int Endod J 2015;48:199-205.PubMed
- 6. Zuolo ML, Carvalho MC, De-Deus G. Negotiability of second mesiobuccal canals in maxillary molars using a reciprocating system. J Endod 2015;41:1913-1917.ArticlePubMed
- 7. Dincer AN, Er O, Canakci BC. Evaluation of apically extruded debris during root canal retreatment with several NiTi systems. Int Endod J 2015;48:1194-1198.ArticlePubMed
- 8. Fidler A. Kinematics of 2 reciprocating endodontic motors: the difference between actual and set values. J Endod 2014;40:990-994.ArticlePubMed
- 9. Relvas JB, Bastos MM, Marques AA, Garrido AD, Sponchiado EC Jr. Assessment of postoperative pain after reciprocating or rotary NiTi instrumentation root canals: a randomized, controlled clinical trial. Clin Oral Investig 2016;20:1987-1993.PubMed
- 10. Kherlakian D, Cunha RS, Ehrhardt IC, Zuolo ML, Kishen A, Da Silveira Bueno CE. Comparison of the incidence of postoperative pain after using 2 reciprocating systems and a continuous rotary system: a prospective randomized clinical trial. J Endod 2016;42:171-176.ArticlePubMed
- 11. Martín-González J, Echevarría-Pérez M, Sánchez-Domínguez B, Tarilonte-Delgado ML, Castellanos-Cosano L, López-Frías FJ, Segura-Egea JJ. Influence of root canal instrumentation and obturation techniques on intra-operative pain during endodontic therapy. Med Oral Patol Oral Cir Bucal 2012;17:e912-e918.PubMedPMC
- 12. Law AS, Nixdorf DR, Aguirre AM, Reams GJ, Tortomasi AJ, Manne BD, Harris DR. National Dental PBRN Collaborative Group. Predicting severe pain after root canal therapy in the National Dental PBRN. J Dent Res 2015;94:37S-43S.ArticlePubMedPMCPDF
- 13. Pasqualini D, Mollo L, Scotti N, Cantatore G, Castellucci A, Migliaretti G, Berutti E. Postoperative pain after manual and mechanical glide path: a randomized clinical trial. J Endod 2012;38:32-36.ArticlePubMed
- 14. Mehrvarzfar P, Abbott PV, Saghiri MA, Delvarani A, Asgar K, Lotfi M, Karamifar K, Kharazifard MJ, Khabazi H. Effects of three oral analgesics on postoperative pain following root canal preparation: a controlled clinical trial. Int Endod J 2012;45:76-82.ArticlePubMed
- 15. Gambarini G, Testarelli L, De Luca M, Milana V, Plotino G, Grande NM, Rubini AG, Al Sudani D, Sannino G. The influence of three different instrumentation techniques on the incidence of postoperative pain after endodontic treatment. Ann Stomatol (Roma) 2013;4:152-155.ArticlePubMedPMC
- 16. Silva EJ, Menaged K, Ajuz N, Monteiro MR, Coutinho-Filho TS. Postoperative pain after foraminal enlargement in anterior teeth with necrosis and apical periodontitis: a prospective and randomized clinical trial. J Endod 2013;39:173-176.ArticlePubMed
- 17. Singh RD, Khatter R, Bal RK, Bal CS. Intracanal medications versus placebo in reducing postoperative endodontic pain: a double-blind randomized clinical trial. Braz Dent J 2013;24:25-29.ArticlePubMed
- 18. Caviedes-Bucheli J, Moreno JO, Carreño CP, Delgado R, Garcia DJ, Solano J, Diaz E, Munoz HR. The effect of single-file reciprocating systems on substance P and calcitonin gene-related peptide expression in human periodontal ligament. Int Endod J 2013;46:419-426.PubMed
- 19. Nekoofar MH, Sheykhrezae MS, Meraji N, Jamee A, Shirvani A, Jamee J, Dummer PM. Comparison of the effect of root canal preparation by using Waveone and Protaper on postoperative pain: a randomized clinical trial. J Endod 2015;41:575-578.ArticlePubMed
REFERENCES
Figure 1
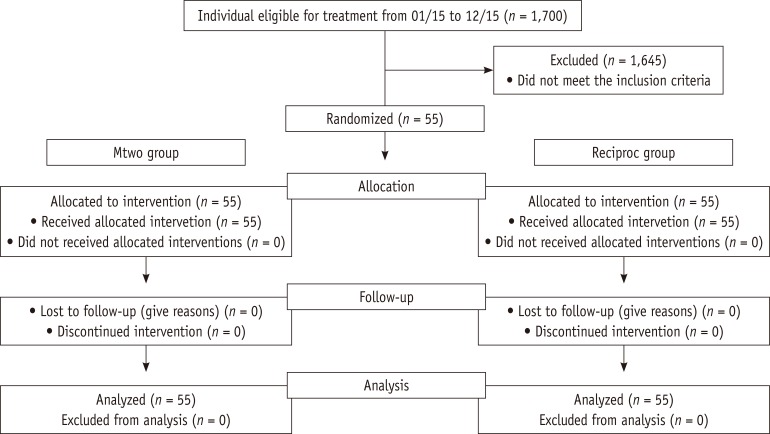
CONSORT flow diagram for randomized clinical trials. Mtwo, multi-file rotary; Reciproc, single-file reciprocating.
Table 1
Demographic and clinical characteristics of participants
| Gender | Male | 26 |
| Female | 29 | |
| Age, years | 46 ± 18 | |
| Mandibular first molar | 15 | |
| Mandibular second molar | 10 | |
| Maxillary first molar | 25 | |
| Maxillary second molar | 5 | |
| Total | 55 | |
Table 2
Descriptive outcome of the pain scores of VAS
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Post-Operative Pain in Reciprocating Versus Rotary Kinematics Post-Endodontic Treatment: A Systematic Review
Youssef Algarni
Archives of Pharmacy Practice.2024; 15(2): 53. CrossRef - Postoperative pain perception and associated risk factors in children after continuous rotation versus reciprocating kinematics: A randomised prospective clinical trial
Ahmad Abdel Hamid Elheeny, Dania Ibrahem Sermani, Mahmoud Ahmed Abdelmotelb
Australian Endodontic Journal.2023; 49(S1): 345. CrossRef - Patient discomfort levels during instrumentation procedure using nickel‐titanium files with different kinetic movements
So‐Ra Park, Se‐Hee Park, Kyung‐Mo Cho, Jin‐Woo Kim, Hyeon‐Cheol Kim
Australian Endodontic Journal.2022; 48(3): 372. CrossRef - Effect of XP‐endo Shaper versus conventional rotary files on postoperative pain and bacterial reduction in oval canals with necrotic pulps: a randomized clinical study
R. S. Emara, S. I. Gawdat, H. M. M. El‐Far
International Endodontic Journal.2021; 54(7): 1026. CrossRef - Effectiveness of a reciprocating single file, single cone endodontic treatment approach: a randomized controlled pragmatic clinical trial
Fabricio Eneas Diniz de Figueiredo, Laila F. Lima, Ludmila S. Oliveira, Maria A. Ribeiro, Marcos B. Correa, Manoel Brito-Junior, André L. Faria-e-Silva
Clinical Oral Investigations.2020; 24(7): 2247. CrossRef - Influence of glide path kinematics during endodontic treatment on the occurrence and intensity of intraoperative and postoperative pain: a systematic review of randomized clinical trials
Thaís Christina Cunha, Felipe de Souza Matos, Luiz Renato Paranhos, Ítalo de Macedo Bernardino, Camilla Christian Gomes Moura
BMC Oral Health.2020;[Epub] CrossRef - Comparison of postoperative pain intensity following the use of three different instrumentation techniques: A randomized clinical trial
Mehmet Adiguzel, Pelin Tufenkci, ismail Ilker Pamukcu
Journal of Dental Research, Dental Clinics, Dental Prospects.2019; 13(2): 133. CrossRef - Reciprocating kinematics leads to lower incidences of postoperative pain than rotary kinematics after endodontic treatment: A systematic review and meta-analysis of randomized controlled trial
ChristineMen Martins, VictorEduardo De Souza Batista, AmandaCaselato Andolfatto Souza, AnaCristina Andrada, GrazielaGarrido Mori, JoaoEduardo Gomes Filho
Journal of Conservative Dentistry.2019; 22(4): 320. CrossRef - Intraoperative Pain During Glide Path Creation with the Use of a Rotary or Reciprocating System
Pelin TUFENKCİ, Mehmet ADIGUZEL, Koray YILMAZ
Cumhuriyet Dental Journal.2019; 22(1): 66. CrossRef
 ePub Link
ePub Link Cite
CiteIntraoperative discomfort associated with the use of a rotary or reciprocating system: a prospective randomized clinical trial
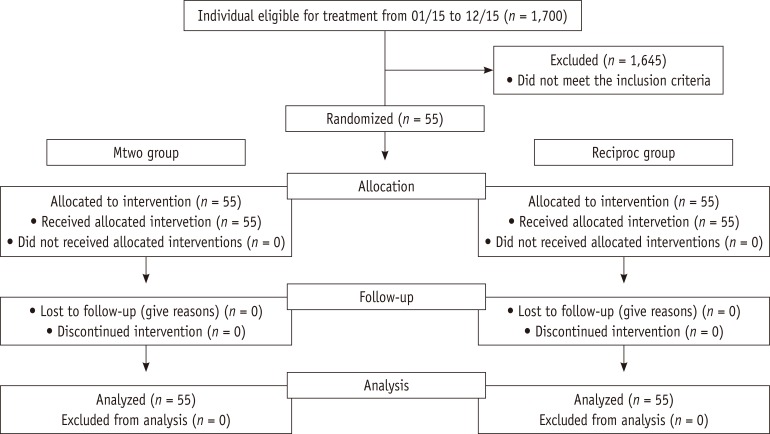
Figure 1 CONSORT flow diagram for randomized clinical trials. Mtwo, multi-file rotary; Reciproc, single-file reciprocating.
Figure 1
Intraoperative discomfort associated with the use of a rotary or reciprocating system: a prospective randomized clinical trial
Demographic and clinical characteristics of participants
| Gender | Male | 26 |
| Female | 29 | |
| Age, years | 46 ± 18 | |
| Mandibular first molar | 15 | |
| Mandibular second molar | 10 | |
| Maxillary first molar | 25 | |
| Maxillary second molar | 5 | |
| Total | 55 | |
Descriptive outcome of the pain scores of VAS
| Score | File used (%) | |
|---|---|---|
| Mtwo (n = 55) | Reciproc (n = 55) | |
| 0 | 0 (0) | 0 (0) |
| 1 | 15 (27.27) | 16 (29.09) |
| 2 | 19 (34.54) | 20 (36.36) |
| 3 | 14 (25.45) | 13 (23.64) |
| 4 | 7 (12.73) | 5 (9.09) |
| 5 | 0 (0) | 1 (1.82) |
| 6 | 0 (0) | 0 (0) |
| 7 | 0 (0) | 0 (0) |
| 8 | 0 (0) | 0 (0) |
| 9 | 0 (0) | 0 (0) |
| 10 | 0 (0) | 0 (0) |
| Total | 55 (100) | 55 (100) |
VAS, visual analog scale; Mtwo, multi-file rotary; Reciproc, single-file reciprocating.
Table 1 Demographic and clinical characteristics of participants
Table 2 Descriptive outcome of the pain scores of VAS
VAS, visual analog scale; Mtwo, multi-file rotary; Reciproc, single-file reciprocating.

