
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 41(2); 2016 > Article
- Research Article Biocompatibility of two experimental scaffolds for regenerative endodontics
-
Dephne Jack Xin Leong1
 , Frank C. Setzer2, Martin Trope2, Bekir Karabucak2
, Frank C. Setzer2, Martin Trope2, Bekir Karabucak2 -
2016;41(2):-105.
DOI: https://doi.org/10.5395/rde.2016.41.2.98
Published online: March 28, 2016
1Faculty of Dentistry, National University of Singapore, and University Dental Cluster (Endodontics), National University Hospital Singapore, Singapore, Singapore.
2Department of Endodontics, School of Dental Medicine, University of Pennsylvania, Philadelphia, PA, USA.
- Correspondence to Dephne Jack Xin Leong, BDS, MS. Assistant Professor, Faculty of Dentistry, National University of Singapore, and Registrar, University Dental Cluster (Endodontics), National University Hospital Singapore, 5 Lower Kent Ridge Road Main Building Level 1 Dental Centre 1, Singapore 119074, Singapore. TEL, +65-6772-4921; FAX, +65-6772-4151; dephdep@gmail.com
• Received: November 18, 2015 • Accepted: February 18, 2016
©Copyrights 2016. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,546 Views
- 12 Download
- 7 Crossref
Abstract
-
Objectives The biocompatibility of two experimental scaffolds for potential use in revascularization or pulp regeneration was evaluated.
-
Materials and Methods One resilient lyophilized collagen scaffold (COLL), releasing metronidazole and clindamycin, was compared to an experimental injectable poly(lactic-co-glycolic) acid scaffold (PLGA), releasing clindamycin. Human dental pulp stem cells (hDPSCs) were seeded at densities of 1.0 × 104, 2.5 × 104, and 5.0 × 104. The cells were investigated by light microscopy (cell morphology), MTT assay (cell proliferation) and a cytokine (IL-8) ELISA test (biocompatibility).
-
Results Under microscope, the morphology of cells coincubated for 7 days with the scaffolds appeared healthy with COLL. Cells in contact with PLGA showed signs of degeneration and apoptosis. MTT assay showed that at 5.0 × 104 hDPSCs, COLL demonstrated significantly higher cell proliferation rates than cells in media only (control, p < 0.01) or cells co-incubated with PLGA (p < 0.01). In ELISA test, no significant differences were observed between cells with media only and COLL at 1, 3, and 6 days. Cells incubated with PLGA expressed significantly higher IL-8 than the control at all time points (p < 0.01) and compared to COLL after 1 and 3 days (p < 0.01).
-
Conclusions The COLL showed superior biocompatibility and thus may be suitable for endodontic regeneration purposes.
Introduction
Root canal treatment is a highly successful procedure.1,2 However, the treatment of teeth with immature roots and pulp necrosis presents significant difficulties for the dental clinician in regard to disinfection and filling of the wide root canal space and open apex. For the practitioner, the revascularization of immature necrotic teeth has become an alternative to apexification techniques.
Current techniques involve disinfecting irrigation, placement of calcium hydroxide or an antibiotic paste as a temporary medication, and the instigation of a blood clot within the root canal space to establish the revascularization. Unfortunately, a blood clot is difficult to produce, unstable and therefore susceptible to breakdown. Moreover, it is a desirable substrate for microbes left behind in the root canal or reintroduced through reinfection from the oral cavity. While or immediately after setting, it is also difficult to seal with a coronal restoration.
To overcome some of the difficulties associated with an intracanal blood clot, the use of scaffold materials was suggested. Examples of three-dimensional organic scaffolds include collagen,3,4,5 glycosaminoglycan, fibrin, cell-sponge constructs or combinations thereof. Synthetic scaffolds are PCL (polycaprolactone),6 PEG (polyethyleneglycol), PLA (polylactic acid),5 PGA (poly-glycolic acid), PLGA (poly-lacticco-glycolic acid),7 or hydrogels. For endodontic purposes, scaffolds must provide an adequate porosity and pore size to allow pulp stem or progenitor cells to migrate and/or organize within a three-dimensional structure, be capable to support cell organization, neuro-, angioor vasculogenesis and to provide necessary nutritional support.8,9
Collagen is a natural constituent of the dental pulp. Collagen scaffolds were shown to provide a suitable environment for pulp progenitor and adult stem cells with odontoblastic properties in vitro,10 and adequate new tissue development with rare histologic inflammation in vivo.11 Cell seeded collagen scaffolds have been used in animals for in vivo pulp regeneration after pulpotomies,12 and after pulpectomies,13 demonstrating regeneration of pulp tissue with angio- and neurogenesis.12,13 Collagen and PLGA scaffolds also showed the regenerative capacity of swine dental pulp stem cells after reimplantation into minipig teeth.14 Development of dentin/pulp-like tissues was observed after subcutaneous implantation of rabbit dental pulp stem cells in PLGA scaffolds.15 PLGA was also used for growth factor or drug delivery, e.g. for pulp capping purposes containing TGF-β1 to initiate tertiary dentin formation,11 or as nanoparticles loaded with methylene blue to initiate photo-disinfecting action against Enterococcus faecalis.16
Antibiotic containing scaffold materials were suggested for pulpal regeneration.8 In periodontics, they were found to be suitable for guided tissue regeneration.17 Metronidazole or ciprofloxacin releasing polydioxanone polymer nanofiber scaffolds were recently introduced for pulp regeneration.18,19,20 This study aimed to investigate the biocompatibility of two experimental antibiotic releasing scaffolds, based on either type-I collagen or on PLGA, with human dental pulp stem cells (hDPSCs) for the potential clinical use in revascularization or regeneration procedures.
Materials and Methods
One resilient lyophilized collagen (COLL) scaffold, releasing metronidazole and clindamycin, was compared to an experimental injectable PLGA scaffold, releasing clindamycin. COLL scaffold was prepared at the University of Pennsylvania. Using cooled pipettes, 3.0 mg/mL type I bovine collagen (Ultrapure bovine collagen solution, Sigma-Aldrich, St. Louis, MO, USA) was mixed on ice with 9 mMol glucose (D-(+)-Glucose, Sigma-Aldrich), sterile ×10 phosphate buffered saline (PBS, Sigma-Aldrich), 1 N sodium hydroxide (NaOH, Sigma-Aldrich), distilled water, 10 mg/mL Metronidazole (Metronidazole, Sigma-Aldrich) and 25 mg/mL Clindamycin (Clindamycin, Sigma-Aldrich) to a final concentration of collagen 2.6 mg/mL. Two hundred microliter (µL) of the mixed solution were delivered each into one well of micro-well strips (Immuno Module Plate With PolySorp Surface, Thermo Fisher Scientific Inc., Waltham, MA, USA). The micro-well strips were then placed into an incubator for 30 minutes at 37℃ to allow gelation. Then, the collagen gels were cross-linked in a ultra-violet cross-linker (Stratalinker UV crosslinker 2400, Stratagene, La Jolla, CA, USA) for another 30 minutes. After the crosslinking process, the collagen gel was frozen at -80℃ for 24 hours and finally lyophilized in a freeze-dryer (Labconco Freezone lyophilizer, Labconco, Kansas City, MO, USA) for 12 hours until a solid and porous scaffold was observed.
The PLGA scaffold was provided by Skywalk Pharmacy (Milwaukee, WI, USA). While the exact manufacture is not being disclosed, this experimental scaffold contained 7.2 wt% Clindamycin, the remainder split between a liquid PLGA solution and N-Methyl-2-pyrrolidone (NMP), a solvent used in the pharmaceutical industry for the formulation of oral and transdermal drugs. The scaffold solidified on contact with moisture with a gel-like consistency.
hDPSCs were kindly provided by Dr. Sunday Akintoye (University of Pennsylvania School of Dental Medicine, Department of Oral Medicine). Cells were cultured in growth culture media consisting of α-modified minimum essential medium (α-MEM, GIBCO, Invitrogen, Carlsbad, CA, USA), supplemented with 20% fetal bovine serum (FBS, Equitech Bio, Kerville, TX, USA), 100 U/mL penicillin, 100 mg/mL streptomycin sulfate (GIBCO/BRL, Grand Island, NY, USA) and 2 mMol glutamine (GIBCO/BRL), and incubated in a humidified 5% CO2 atmosphere at 37℃. The growth media in the wells was changed every other day. Cells grown in medium only served as control group for all experiments.
hDPSCs were seeded at a density of 5.0 × 104 cells/well in 12-well plates (Corning Inc., Corning, NY, USA). Three hours after plating, one piece of COLL scaffold from a micro-strip well or one drop of PLGA scaffold of similar size as the COLL scaffold was completely immersed in the cell media in co-incubation with the cells. When the cells reached 90 - 95% confluence, light microscopy pictures were taken at ×100 and ×200 magnifications using a light microscope (TMS-F microscope, Nikon Instruments, Melville, NY, USA).
Actively proliferating hDPSCs were plated in 96-well plates at densities of 1.0 × 104, 2.5 × 104, and 5.0 × 104 per well. Three hours after plating, one piece of COLL scaffold or one drop of PLGA scaffold of the same dimensions as mentioned above was immersed in form of co-incubation. After 48 hours of incubation, cell proliferation was assessed using the Colorimetric MTT Cell Survival and Proliferation Assay Kit (Millipore, Chemicon International Inc., Temecula, CA, USA) according to the manufacturer's protocol. Briefly, MTT reagents were added and incubated for 4 hours. Then 100 µL isopropanol with 0.04 N HCl was added to each well. After thorough mixing using a plate shaker for 10 minutes at room temperature, the scaffolds were carefully removed from the wells and a colorimetric analysis performed with a multiplate reader (Synergy HT, Biotek, Winooski, VT, USA) at 570 nm. A solution of growth media with isopropanol and HCl served as negative control. The optical density values were obtained from triplicate samples and the experiment was repeated twice.
hDPSCs were seeded at a 5.0 × 104 cells per well density in 12-well plates. Similarly, 3 hours after plating, one piece of COLL scaffold or one drop of PLGA scaffold were immersed with the cells for co-incubation. Supernatants were collected after 24 hours (Day 1 samples), 72 hours (Day 3 samples), and 6 days (Day 6 samples), and subsequently stored at - 80℃ until use. The amount of IL-8 was measured by an enzyme-linked immunosorbent assay (ELISA) using the Human IL-8 ELISA Kit II (BD OptEIA, BD Biosciences, Bedford, MA, USA) according to the manufacturer's instructions. Growth media served as a negative control. The absorbance was read at 450 nm in the multiplate reader for triplicate samples. The experiment was repeated twice.
Prism 6.0 software (GraphPad Software Inc., La Jolla, CA, USA) was used for statistical analysis. The results of the absorbance measured using multiplate reader were analyzed using two-way analysis of variance (ANOVA) and post hoc Bonferroni test for the type of scaffold, and cell number or time point. Statistical significance was accepted at p < 0.05.
Results
The exposure of hDPSCs to the two different scaffold materials after 7 days in co-culture revealed major morphological differences. Figure 1 shows the comparison of representative cell appearances under the light microscope at ×100 and ×200. In general, hDPSCs in the COLL group appeared healthier, well stretched and attached to the cell culture plate. Cells grew in direct proximity to the COLL scaffold with identical healthy appearance as in other areas of the culture wells (Figures 1a - 1d). Cells in co-incubation with the PLGA scaffold frequently demonstrated signs of degeneration and apoptosis, in particular in proximity to the actual material. An abundance of cell debris and rounded cell morphologies suggested non-attachment. (Figures 1e - 1h).
Table 1 and Figure 2 show the absorbance readings measured using the multiplate reader. Of the hDPSCs seeded at 3 different densities (1.0 × 104, 2.5 × 104, and 5.0 × 104), with media only, COLL or PLGA scaffolds, at 2.5 × 104 and 5.0 × 104 cell densities, COLL demonstrated significantly higher cell proliferation rates than cells in media only (control) (p < 0.05 and p < 0.01, respectively) or in co-incubation with PLGA (p < 0.05 and p < 0.01, respectively). The effect of the different cell numbers was not statistically significant.
No significant differences were observed between cells with media only and COLL at 1, 3, and 6 days. Cells incubated with PLGA expressed significantly higher IL-8 than the control at all time points (p < 0.01) and compared to COLL after 1 and 3 days (p < 0.01, Table 2 and Figure 3). The effect of the different time points was found to be statistically significant (p < 0.001).
Discussion
To date, no final approach to clinical revascularization or a common strategy to achieve pulp regeneration has been agreed upon. While it was recognized that clinical revascularization does not provide pulp or pulp-like tissues, the clinical benefits of an ingrowth of vital tissue into a disinfected tooth with a history of pulp necrosis are greatly beneficial to the patient. Successful revascularization not only provides vitality, but also generates the formation of a closed apex and strengthens the tooth structure by thickening of the root walls, thus adding prevention from fracture. While a consensus seems to exist that complete regeneration of the pulp would involve exogenously introduced cells, as cell-free regeneration after complete loss of the dental pulp appears unlikely,21 it is still unclear, which types of cells, scaffold materials and bioactive factors would provide the greatest chances of successful regeneration. Thus, clinical revascularization remains the best strategy for a practitioner to treat immature teeth with pulp necrosis. However, creating a suitable blood clot remains a challenge in clinical practice and scaffold materials may prove an alternative for clinical practice.
This study investigated two different potential scaffolds containing antibiotics. In endodontics, local antibiotics were initially used as intracanal medication to aid in the disinfection of infected, pulpless teeth.22 However, this treatment fell into disfavor and was only reestablished with new techniques for revascularization to disinfect immature, necrotic teeth. A triple antibiotic paste consisting of metronidazole, ciprofloxacin and minocycline was introduced,23 and its efficacy to penetrate dentin demonstrated in vitro.24 Several case reports on revascularization using triple antibiotic paste were published.25,26 The effectiveness of in vivo disinfection was shown by Windley et al.27 Several clinical complications were described for revascularization procedures, including discolorations by minocycline. Cefaclor was suggested as replacement for minocycline.28,29 Another problem was the potential collapse of MTA into the fresh blood clot, which could be overcome by the additional placement of a solid resorbable collagen matrix to pack MTA against.28
The placement of scaffolds for current revascularization and, possibly, future regeneration procedures could serve several purposes. For revascularization, it can provide stability placing a suitable material against the blood clot. For regeneration, a matrix can supply stem or progenitor cells to the root canal and provide support for the ingrowth of vascularization and re-innervation, as well as aid stability for early stages of tissue regeneration. For both procedures, a scaffold can provide bioactive substances.30
To use bioactive materials for the delivery of growth factors or drugs such as antibiotics in endodontic regenerative procedures was suggested earlier on.30,31 Nevertheless, only few endodontic studies introduced growth factor,32,33 or antibiotic-containing scaffolds.18,19,20 Bottino et al.18 used metronidazole or ciprofloxacin releasing nanofiber-scaffolds and tested them against Porphyromonas gingivalis and Enterococcus faecalis. In accordance with our study the metronidazole containing scaffolds demonstrated good cytocompatibility. Metronidazole inhibited only growth of Porphyromonas gingivalis, while ciprofloxacin was effective against both strains. This supports the idea of combining antibiotics to achieve a wider antibacterial spectrum, similar to triple antibiotic paste or the COLL scaffold in this investigation, combining metronidazole with clindamycin, a lincosamide, used to treat dental infections with anaerobic bacteria.34 A commercially available triple antibiotic paste (PulpVAZ, Blaze Pharmaceuticals LLC, Ankeny, IA, USA) contains clindamycin as alternative to minocycline. Clindamycin demonstrated successful antibacterial activity as an intracanal dressing in vivo.35
In vitro, it showed significantly more antibacterial activity than tetracycline.36 Clindamycin releasing fibers from ethylene vinyl acetate significantly reduced bacteria in extracted human teeth and provided sustained antibiotic release of over 2 weeks.34 This surpassed the activity of metronidazole and ciprofloxacin for 48 hours.18 Even if not directly comparable, this substantial time difference suggests that clindamycin, if biologically acceptable, may be a good alternative for pulp regeneration.
The present study evaluated biocompatibility and cell proliferation of hDPSCs with the experimental scaffolds. Although both scaffolds incorporated clindamycin, and both collagen and PLGA are known to be suitable scaffold materials for endodontic procedures, significant differences between the materials existed. Light microscopy permitted to observe cell morphology after co-incubation with the scaffolds. Cells in contact with the PLGA scaffolds frequently showed signs of degeneration and apoptosis. Whereas no significant difference in IL-8 concentration were found between hDPSCs cultured in media only and COLL, cells incubated with PLGA expressed significantly higher IL-8 than the control at all time points and compared to COLL after 1 and 3 days. This implied the induction of inflammation by the experimental PLGA scaffolds, suggesting less biocompatibility than the COLL scaffolds.
Several factors may be responsible for the lower biocompatibility of the experimental PLGA scaffold. PLGA itself is biocompatible; however the experimental scaffold contained a very high percentage of NMP. This stabilizer, although widely used pharmaceutically may have adverse effects on hDPSCs. The concentration of the antibiotic component itself (7.2 wt%) may have influenced the biocompatibility. High concentrations of antibiotics in triple antibiotic paste of 1, 10, and 100 mg/mL resulted in significantly lower cell viability of stem cells from the apical papilla than concentrations of 0.1 and 0.01 mg/mL or any concentration of calcium hydroxide.37 This may appear to be contradictory to the good biocompatibility of the experimental COLL scaffold containing 10 mg/mL metronidazole and 25 mg/mL clindamycin. However, Chuensombat et al. demonstrated that the adverse cell viability effect of triple antibiotic paste, when tested against human dental pulp cells and apical papilla cells was related to minocycline and ciprofloxacin, whereas no significant differences between metronidazole and the control were found up to 25 mg/mL.38 Also, antibioticcontaining scaffolds with 10 wt% metronidazole and 25 wt% ciprofloxacin were successfully tested.18,19
Although antibiotic use was suggested for regenerative procedures earlier,8 some studies advocated calcium hydroxide.37,39 However, calcium hydroxide itself may pose potential problems, including formation of a hard tissue barrier, or tooth structure weakening if applied too long.40
Conclusions
Within the limitations of this study, experimental resilient lyophilized metronidazole and clindamycin releasing collagen scaffolds could be of potential clinical use for revascularization or pulp regeneration procedures. Whereas further investigations including detailed material characterization, antimicrobial activity, and antibiotic substantivity are needed to validate the use of these scaffold materials, this pilot study demonstrated the biocompatibility and the effects on cell proliferation of antibiotic-releasing scaffolds in regenerative endodontics and gives the practitioner the insight of the potential application of scaffold materials useful for revascularization, which are cost-effective, easy to manipulate and would provide predictable positive outcomes for clinicians.
Acknowledgement
The authors thank Dr. Elisabeth Barton, Dr. Carolyn Gibson, Dr. Lee Sweeney, Dr. Ho Yugong and Dr. Daniel Safer for the use of their laboratories and machines, as well as Dr. Johnah Galicia for advice on the collagen scaffolds. The authors deny any conflict of interest related to this study.
- 1. de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study-phase 4: initial treatment. J Endod 2008;34:258-263.ArticlePubMed
- 2. Ricucci D, Russo J, Rutberg M, Burleson JA, Spångberg LS. A prospective cohort study of endodontic treatments of 1,369 root canals: results after 5 years. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:825-842.ArticlePubMed
- 3. Nirmalanandhan VS, Levy MS, Huth AJ, Butler DL. Effects of cell seeding density and collagen concentration on contraction kinetics of mesenchymal stem cell-seeded collagen constructs. Tissue Eng 2006;12:1865-1872.ArticlePubMed
- 4. Nirmalanandhan VS, Rao M, Sacks MS, Haridas B, Butler DL. Effect of length of the engineered tendon construct on its structure-function relationships in culture. J Biomech 2007;40:2523-2529.ArticlePubMed
- 5. Chandrahasa S, Murray PE, Namerow KN. Proliferation of mature ex vivo human dental pulp using tissue engineering scaffolds. J Endod 2011;37:1236-1239.ArticlePubMed
- 6. Huang GT, Sonoyama W, Liu Y, Liu H, Wang S, Shi S. The hidden treasure in apical papilla: the potential role in pulp/dentin regeneration and bioroot engineering. J Endod 2008;34:645-651.ArticlePubMedPMC
- 7. Zhang W, Walboomers XF, Jansen JA. The formation of tertiary dentin after pulp capping with a calcium phosphate cement, loaded with PLGA microparticles containing TGF-beta1. J Biomed Mater Res A 2008;85:439-444.PubMed
- 8. Murray PE, Garcia-Godoy F, Hargreaves KM. Regenerative endodontics: a review of current status and a call for action. J Endod 2007;33:377-390.ArticlePubMed
- 9. Sachlos E, Czernuszka JT. Making tissue engineering scaffolds work. Review: the application of solid freeform fabrication technology to the production of tissue engineering scaffolds. Eur Cell Mater 2003;5:29-39.ArticlePubMed
- 10. Inuyama Y, Kitamura C, Nishihara T, Morotomi T, Nagayoshi M, Tabata Y, Matsuo K, Chen KK, Terashita M. Effects of hyaluronic acid sponge as a scaffold on odontoblastic cell line and amputated dental pulp. J Biomed Mater Res B Appl Biomater 2010;92:120-128.ArticlePubMed
- 11. Zhang W, Walboomers XF, van Kuppevelt TH, Daamen WF, Bian Z, Jansen JA. The performance of human dental pulp stem cells on different three-dimensional scaffold materials. Biomaterials 2006;27:5658-5668.ArticlePubMed
- 12. Iohara K, Zheng L, Ito M, Ishizaka R, Nakamura H, Into T, Matsushita K, Nakashima M. Regeneration of dental pulp after pulpotomy by transplantation of CD31(-)/ CD146(-) side population cells from a canine tooth. Regen Med 2009;4:377-385.ArticlePubMed
- 13. Iohara K, Murakami M, Takeuchi N, Osako Y, Ito M, Ishizaka R, Utunomiya S, Nakamura H, Matsushita K, Nakashima M. A novel combinatorial therapy with pulp stem cells and granulocyte colony-stimulating factor for total pulp regeneration. Stem Cells Transl Med 2013;2:521-533.ArticlePubMedPMCPDF
- 14. Kodonas K, Gogos C, Papadimitriou S, Kouzi-Koliakou K, Tziafas D. Experimental formation of dentinlike structure in the root canal implant model using cryopreserved swine dental pulp progenitor cells. J Endod 2012;38:913-919.ArticlePubMed
- 15. El-Backly RM, Massoud AG, El-Badry AM, Sherif RA, Marei MK. Regeneration of dentine/pulp-like tissue using a dental pulp stem cell/poly(lactic-co-glycolic) acid scaffold construct in New Zealand white rabbits. Aust Endod J 2008;34:52-67.ArticlePubMed
- 16. Pagonis TC, Chen J, Fontana CR, Devalapally H, Ruggiero K, Song X, Foschi F, Dunham J, Skobe Z, Yamazaki H, Kent R, Tanner AC, Amiji MM, Soukos NS. Nanoparticlebased endodontic antimicrobial photodynamic therapy. J Endod 2010;36:322-328.ArticlePubMed
- 17. Cheng CF, Lee YY, Chi LY, Chen YT, Hung SL, Ling LJ. Bacterial penetration through antibiotic-loaded guided tissue regeneration membranes. J Periodontol 2009;80:1471-1478.ArticlePubMed
- 18. Bottino MC, Kamocki K, Yassen GH, Platt JA, Vail MM, Ehrlich Y, Spolnik KJ, Gregory RL. Bioactive nanofibrous scaffolds for regenerative endodontics. J Dent Res 2013;92:963-969.ArticlePubMedPMCPDF
- 19. Albuquerque MT, Valera MC, Moreira CS, Bresciani E, de Melo RM, Bottino MC. Effects of ciprofloxacincontaining scaffolds on enterococcus faecalis biofilms. J Endod 2015;41:710-714.ArticlePubMed
- 20. Kamocki K, Nör JE, Bottino MC. Effects of ciprofloxacincontaining antimicrobial scaffolds on dental pulp stem cell viability-in vitro studies. Arch Oral Biol 2015;60:1131-1137.ArticlePubMedPMC
- 21. Huang GT, Al-Habib M, Gauthier P. Challenges of stem cell-based pulp and dentin regeneration: a clinical perspective. Endod Topics 2013;28:51-60.ArticlePubMedPMC
- 22. Grossman LI. Polyantibiotic treatment of pulpless teeth. J Am Dent Assoc 1951;43:265-278.ArticlePubMed
- 23. Sato T, Hoshino E, Uematsu H, Noda T. In vitro antimicrobial susceptibility to combinations of drugs on bacteria from carious and endodontic lesions of human deciduous teeth. Oral Microbiol Immunol 1993;8:172-176.PubMed
- 24. Hoshino E, Kurihara-Ando N, Sato I, Uematsu H, Sato M, Kota K, Iwaku M. In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int Endod J 1996;29:125-130.ArticlePubMed
- 25. Iwaya SI, Ikawa M, Kubota M. Revascularization of an immature permanent tooth with apical periodontitis and sinus tract. Dent Traumatol 2001;17:185-187.ArticlePubMedPDF
- 26. Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol. J Endod 2004;30:196-200.ArticlePubMed
- 27. Windley W 3rd, Teixeira F, Levin L, Sigurdsson A, Trope M. Disinfection of immature teeth with a triple antibiotic paste. J Endod 2005;31:439-443.ArticlePubMed
- 28. Dabbagh B, Alvaro E, Vu DD, Rizkallah J, Schwartz S. Clinical complications in the revascularization of immature necrotic permanent teeth. Pediatr Dent 2012;34:414-417.PubMed
- 29. Bezgin T, Yılmaz AD, Celik BN, Sönmez H. Concentrated platelet-rich plasma used in root canal revascularization: 2 case reports. Int Endod J 2014;47:41-49.ArticlePubMed
- 30. Moioli EK, Clark PA, Xin X, Lal S, Mao JJ. Matrices and scaffolds for drug delivery in dental, oral and craniofacial tissue engineering. Adv Drug Deliv Rev 2007;59:308-324.ArticlePubMedPMC
- 31. Enkel B, Dupas C, Armengol V, Akpe Adou J, Bosco J, Daculsi G, Jean A, Laboux O, LeGeros RZ, Weiss P. Bioactive materials in endodontics. Expert Rev Med Devices 2008;5:475-494.ArticlePubMed
- 32. Kitamura C, Nishihara T, Terashita M, Tabata Y, Washio A. Local regeneration of dentin-pulp complex using controlled release of fgf-2 and naturally derived spongelike scaffolds. Int J Dent 2012;2012:190561.ArticlePubMedPDF
- 33. Yang X, Han G, Pang X, Fan M. Chitosan/collagen scaffold containing bone morphogenetic protein-7 DNA supports dental pulp stem cell differentiation in vitro and in vivo. J Biomed Mater Res A 2012 2 18 [Epub ahead of print].ArticlePDF
- 34. Gilad JZ, Teles R, Goodson M, White RR, Stashenko P. Development of a clindamycin-impregnated fiber as an intracanal medication in endodontic therapy. J Endod 1999;25:722-727.ArticlePubMed
- 35. Molander A, Dahlén G. Evaluation of the antibacterial potential of tetracycline or erythromycin mixed with calcium hydroxide as intracanal dressing against Enterococcus faecalis in vivo. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:744-750.ArticlePubMed
- 36. Lin S, Levin L, Peled M, Weiss EI, Fuss Z. Reduction of viable bacteria in dentinal tubules treated with clindamycin or tetracycline. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:751-756.ArticlePubMed
- 37. Ruparel NB, Teixeira FB, Ferraz CC, Diogenes A. Direct effect of intracanal medicaments on survival of stem cells of the apical papilla. J Endod 2012;38:1372-1375.ArticlePubMed
- 38. Chuensombat S, Khemaleelakul S, Chattipakorn S, Srisuwan T. Cytotoxic effects and antibacterial efficacy of a 3-antibiotic combination: an in vitro study. J Endod 2013;39:813-819.ArticlePubMed
- 39. Soares Ade J, Lins FF, Nagata JY, Gomes BP, Zaia AA, Ferraz CC, de Almeida JF, de Souza-Filho FJ. Pulp revascularization after root canal decontamination with calcium hydroxide and 2% chlorhexidine gel. J Endod 2013;39:417-420.ArticlePubMed
- 40. Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol 2002;18:134-137.ArticlePubMedPDF
REFERENCES
Figure 1
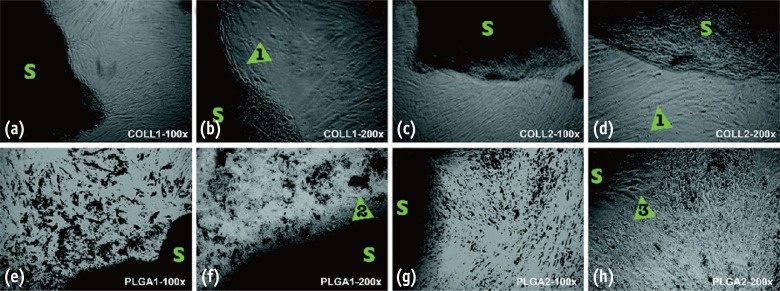
Comparison of representative cell appearances under the light microscope at ×100 and ×200. 'S' denotes scaffolds. (a - d) Cells grown in proximity to COLL scaffolds demonstrated a generally healthy appearance similar to other areas of the culture wells and controls (arrows 1); (e - f) Co-incubation with the PLGA scaffold often displayed signs of apoptosis and cell degeneration, particularly close to the actual material. Cell debris (arrow 2) and rounded cell morphologies (arrow 3) suggested non-attachment. COLL, lyophilized collagen; PLGA, poly-lactic-co-glycolic acid.
Figure 2
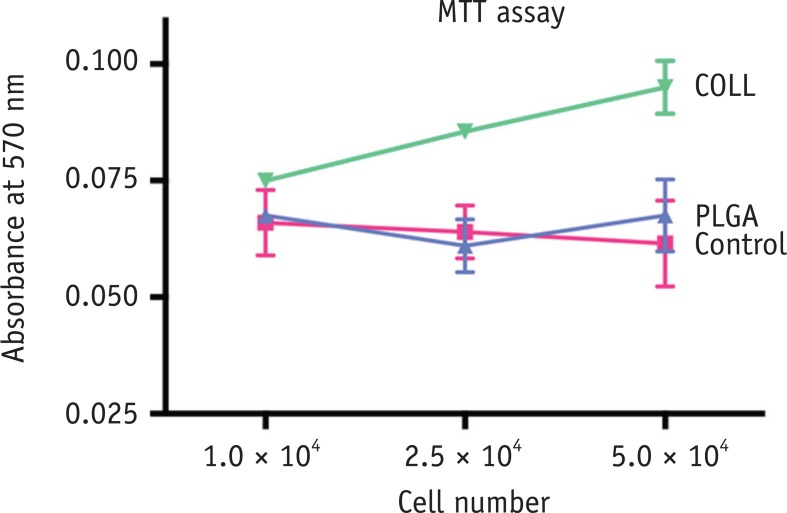
MTT assay. Absorbance measured using a multiplate reader. hDPSCs were seeded at 3 different densities (1.0 × 104, 2.5 × 104, and 5.0 × 104) with media only (red), PLGA scaffold (blue) or COLL scaffold (green). Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. hDPSC, human dental pulp stem cells; PLGA, poly-lactic-co-glycolic acid; COLL, lyophilized collagen.
Figure 3
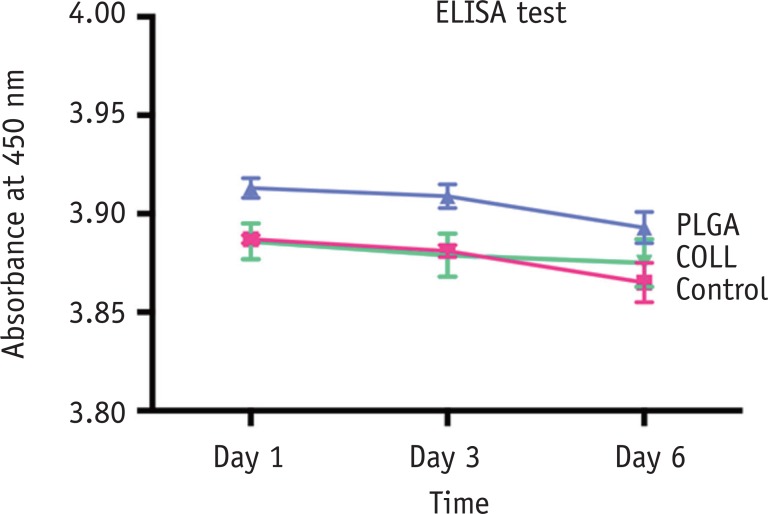
IL-8 ELISA test. Absorbance measured using a multiplate reader at 3 different time points (Days 1, 3, and 6). hDPSCs were seeded at 5.0 × 104 cell density with media only (red), PLGA scaffold (blue) or COLL scaffold (green). Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. hDPSC, human dental pulp stem cells; PLGA, poly-lactic-coglycolic acid; COLL, lyophilized collagen.
Table 1
Absorbance readings for MTT assay of various cell numbers and types of scaffold
Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. There was no significant difference in absorbance readings depending on cell number (p = 0.285 [α]), but a statistically significant difference depending on scaffold type (p = 0.002 [β]). PLGA, poly-lactic-co-glycolic acid; COLL, lyophilized collagen.
Table 2
Absorbance readings for IL-8 ELISA test of various time points and types of scaffold
| Time | Control | PLGA | COLL | p value* |
|---|---|---|---|---|
| Day 1 | 3.887 ± 0.002 | 3.913 ± 0.005 | 3.886 ± 0.009 | α = 0.001 |
| Day 3 | 3.881 ± 0.003 | 3.909 ± 0.006 | 3.879 ± 0.011 | β = 0.0001 |
| Day 6 | 3.865 ± 0.010 | 3.893 ± 0.008 | 3.875 ± 0.012 |
Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. There was a statistically significant difference in absorbance readings depending on time point (p = 0.001 [α]) and scaffold type (p = 0.0001 [β]). PLGA, poly-lactic-co-glycolic acid; COLL, lyophilized collagen.
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- The Future of Biomaterials in Dentistry: Innovations in Drug Delivery and Regenerative Medicine
Rosana Farjaminejad, Samira Farjaminejad, Franklin Garcia-Godoy, Melika Hassani, Kourosh Rahimikia
Journal of Applied Dentistry and Oral Sciences.2025; 11(4): 160. CrossRef - Advances in scaffolds used forpulp–dentinecomplex tissue engineering: A narrative review
Parisa Noohi, Mohammad J. Abdekhodaie, Mohammad H. Nekoofar, Kerstin M. Galler, Paul M. H. Dummer
International Endodontic Journal.2022; 55(12): 1277. CrossRef - In vitro performance of a nanobiocomposite scaffold containing boron-modified bioactive glass nanoparticles for dentin regeneration
Reza Moonesi Rad, Engin Pazarçeviren, Elif Ece Akgün, Zafer Evis, Dilek Keskin, Sıla Şahin, Ayşen Tezcaner
Journal of Biomaterials Applications.2019; 33(6): 834. CrossRef - Biological effects of silk fibroin 3D scaffolds on stem cells from human exfoliated deciduous teeth (SHEDs)
M. Collado-González, M. P. Pecci-Lloret, D. García-Bernal, S. Aznar-Cervantes, R. E. Oñate-Sánchez, J. M. Moraleda, J. L. Cenis, F. J. Rodríguez-Lozano
Odontology.2018; 106(2): 125. CrossRef - Pulp Regeneration Concepts for Nonvital Teeth: From Tissue Engineering to Clinical Approaches
Valérie Orti, Pierre-Yves Collart-Dutilleul, Sofía Piglionico, Orsolya Pall, Frédéric Cuisinier, Ivan Panayotov
Tissue Engineering Part B: Reviews.2018; 24(6): 419. CrossRef - Investigation of Human Dental Pulp Cells on a Potential Injectable Poly(lactic-co-glycolic acid) Microsphere Scaffold
Huiru Zou, Guanhua Wang, Fang Song, Xudong Shi
Journal of Endodontics.2017; 43(5): 745. CrossRef - Biocompatibility of hydrogel-based scaffolds for tissue engineering applications
Sheva Naahidi, Mousa Jafari, Megan Logan, Yujie Wang, Yongfang Yuan, Hojae Bae, Brian Dixon, P. Chen
Biotechnology Advances.2017; 35(5): 530. CrossRef
 ePub Link
ePub Link Cite
CiteBiocompatibility of two experimental scaffolds for regenerative endodontics
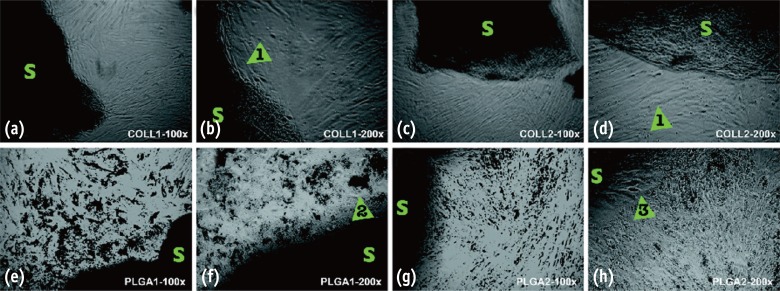
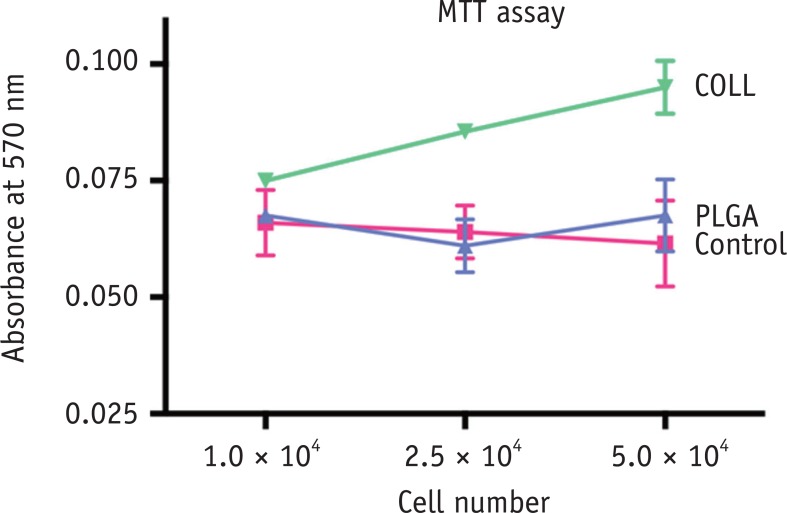
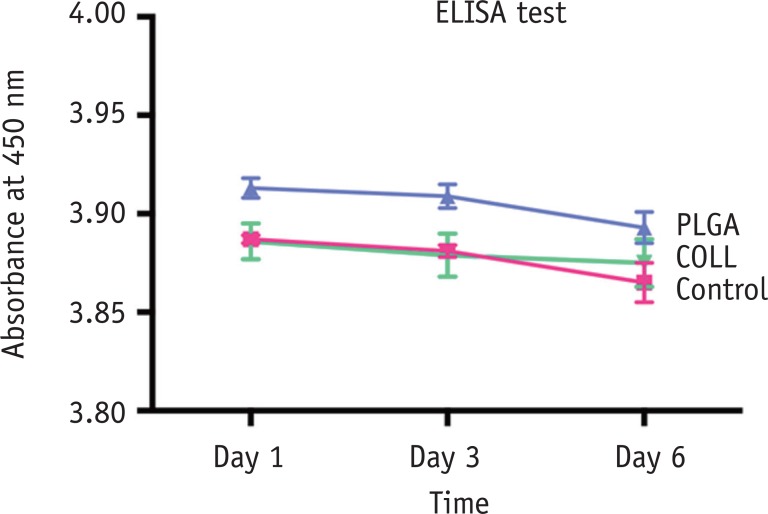
Figure 1 Comparison of representative cell appearances under the light microscope at ×100 and ×200. 'S' denotes scaffolds. (a - d) Cells grown in proximity to COLL scaffolds demonstrated a generally healthy appearance similar to other areas of the culture wells and controls (arrows 1); (e - f) Co-incubation with the PLGA scaffold often displayed signs of apoptosis and cell degeneration, particularly close to the actual material. Cell debris (arrow 2) and rounded cell morphologies (arrow 3) suggested non-attachment. COLL, lyophilized collagen; PLGA, poly-lactic-co-glycolic acid.
Figure 2 MTT assay. Absorbance measured using a multiplate reader. hDPSCs were seeded at 3 different densities (1.0 × 104, 2.5 × 104, and 5.0 × 104) with media only (red), PLGA scaffold (blue) or COLL scaffold (green). Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. hDPSC, human dental pulp stem cells; PLGA, poly-lactic-co-glycolic acid; COLL, lyophilized collagen.
Figure 3 IL-8 ELISA test. Absorbance measured using a multiplate reader at 3 different time points (Days 1, 3, and 6). hDPSCs were seeded at 5.0 × 104 cell density with media only (red), PLGA scaffold (blue) or COLL scaffold (green). Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. hDPSC, human dental pulp stem cells; PLGA, poly-lactic-coglycolic acid; COLL, lyophilized collagen.
Figure 1
Figure 2
Figure 3
Biocompatibility of two experimental scaffolds for regenerative endodontics
Absorbance readings for MTT assay of various cell numbers and types of scaffold
| Cell number | Control | PLGA | COLL | p value* |
|---|---|---|---|---|
| 1.0 × 104 | 0.0660 ± 0.0071 | 0.0675 ± 0.0007 | 0.0750 ± 0.0014 | α = 0.285 |
| 2.5 × 104 | 0.0640 ± 0.0057 | 0.0610 ± 0.0057 | 0.0855 ± 0.0007 | β = 0.002 |
| 5.0 × 104 | 0.0615 ± 0.0092 | 0.0675 ± 0.0078 | 0.0950 ± 0.0057 |
Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. There was no significant difference in absorbance readings depending on cell number (p = 0.285 [α]), but a statistically significant difference depending on scaffold type (p = 0.002 [β]). PLGA, poly-lactic-co-glycolic acid; COLL, lyophilized collagen.
Absorbance readings for IL-8 ELISA test of various time points and types of scaffold
| Time | Control | PLGA | COLL | p value* |
|---|---|---|---|---|
| Day 1 | 3.887 ± 0.002 | 3.913 ± 0.005 | 3.886 ± 0.009 | α = 0.001 |
| Day 3 | 3.881 ± 0.003 | 3.909 ± 0.006 | 3.879 ± 0.011 | β = 0.0001 |
| Day 6 | 3.865 ± 0.010 | 3.893 ± 0.008 | 3.875 ± 0.012 |
Mean ± SEM for N = 6 per condition. *p < 0.05, by 2-way ANOVA and Bonferroni post hoc test. There was a statistically significant difference in absorbance readings depending on time point (p = 0.001 [α]) and scaffold type (p = 0.0001 [β]). PLGA, poly-lactic-co-glycolic acid; COLL, lyophilized collagen.
Table 1 Absorbance readings for MTT assay of various cell numbers and types of scaffold
Mean ± SEM for N = 6 per condition. *
Table 2 Absorbance readings for IL-8 ELISA test of various time points and types of scaffold
Mean ± SEM for N = 6 per condition. *

