
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 41(1); 2016 > Article
- Research Article Analysis of C-shaped root canal configuration in maxillary molars in a Korean population using cone-beam computed tomography
- Hyoung-Hoon Jo, Jeong-Bum Min, Ho-Keel Hwang
-
2016;41(1):-62.
DOI: https://doi.org/10.5395/rde.2016.41.1.55
Published online: January 29, 2016
Department of Conservative Dentistry, School of Dentistry, Chosun University, Gwangju, Korea.
- Correspondence to Ho-Keel Hwang, DDS, PhD. Professor, Department of Conservative Dentistry, School of Dentistry, Chosun University, 309 Pilmun-daero, Dong-gu, Gwangju, Korea 61452. TEL, +82-62-220-3840; FAX, +82-62-223-9064; rootcanal@hanmail.net
• Received: October 20, 2015 • Accepted: January 6, 2016
©Copyrights 2016. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,788 Views
- 19 Download
- 26 Crossref
Abstract
-
Objectives The purpose of this study was to investigate the incidence of root fusion and C-shaped root canals in maxillary molars, and to classify the types of C-shaped canal by analyzing cone-beam computed tomography (CBCT) in a Korean population.
-
Materials and Methods Digitized CBCT images from 911 subjects were obtained in Chosun University Dental Hospital between February 2010 and July 2012 for orthodontic treatment. Among them, a total of selected 3,553 data of maxillary molars were analyzed retrospectively. Tomography sections in the axial, coronal, and sagittal planes were displayed by PiViewstar and Rapidia MPR software (Infinitt Co.). The incidence and types of root fusion and C-shaped root canals were evaluated and the incidence between the first and the second molar was compared using Chi-square test.
-
Results Root fusion was present in 3.2% of the first molars and 19.5% of the second molars, and fusion of mesiobuccal and palatal root was dominant. C-shaped root canals were present in 0.8% of the first molars and 2.7% of the second molars. The frequency of root fusion and C-shaped canal was significantly higher in the second molar than the first molar (p < 0.001).
-
Conclusions In a Korean population, maxillary molars showed total 11.3% of root fusion and 1.8% of C-shaped root canals. Furthermore, root fusion and C-shaped root canals were seen more frequently in the maxillary second molars.
Introduction
The main objective of root canal treatment is thorough shaping and cleaning of all pulp spaces and their complete obturation. A canal is often left untreated due to lack of meticulous diagnosis, and this untreated canal is one of the most common reasons for failure. Therefore, thorough knowledge on root canal configuration including characteristic features and anatomic variations is a key factor for successful root canal treatment.
One of the most important anatomic variations is the C-shaped root canal configuration. C-shaped root canal and its clinical implication was first described in dental journal in 1979.1 It has been difficult to diagnose and manage the C-shaped root canal because of its unique feature with presence of fins or webs connecting the individual root canals. This root canal configuration may occur in any molar area such as the mandibular first molar,2,3 first premolar,4 and maxillary molars.5 Above all, it is most frequently found in mandibular second molars.6 Owing to the high prevalence, the anatomic features of C-shaped root canal in the mandibular second molars have been well documented in many articles.6,7,8 The classification of them has been studied for decades, and the classification by Melton et al. and Fan et al. has been most representative criteria for typing C-shaped root canals.6,7 As the tooth anatomy varies according to the racial origin,9,10 the incidence of C-shaped root canals in mandibular second molars also has ethnic difference, which was higher in Asians than other racial groups.11,12
Until now, there are only limited numbers of studies reporting C-shaped root canals in maxillary molars, and its classification has not been established. Considering the high failure rate of root canal treatment in maxillary molars, understanding the canal variation such as C-shaped root canal should be more emphasized. The aim of this study was to investigate the incidence of root fusion and C-shaped root canals in maxillary molars, and to classify the types by analyzing cone-beam computed tomography (CBCT) in a Korean population.
Materials and Methods
The research protocol of present study was approved by the Institutional Review Board of the Chosun University Dental Hospital (CDMDIRB-1218-90). For the analysis of root fusion and C-shaped root canals in maxillary molars, digitized CBCT images taken for orthodontic treatments at Chosun University Dental Hospital, Gwangju, Korea between February 2010 and July 2012 were examined. Among those CBCT data, the images of 911 subjects (393 male and 518 female) who had high quality radiographic data were selected for this study. Mean age of the patients was 21.9 years, ranging from 15 to 61 years. Fully erupted and completely root formed maxillary first and second molars without root canal treatment were included, and the third molars and immature teeth were excluded. Finally, total of 3,553 maxillary molars (1,786 first molars and 1,767 second molars) were examined retrospectively.
The CBCT images were taken with CB Mercuray (Hitachi medical Corp., Tokyo, Japan), while the scan settings were Φ 15 cm scan field of view, 0.3 mm voxel size, 120 kVp, 15 mA, with a 10 seconds exposure time. Tomography sections were displayed by PiViewSTAR and Rapidia MPR software (Infinitt Co., Seoul, Korea) in the axial, coronal, and sagittal planes. Contrast and brightness of images could be adjusted using the image processing tool of the software to ensure optimal visualization. The long axis of each tooth was determined and cross-sectional images at apical third were examined by rolling the tool bar from pulp chamber to the apex. The criteria for defining root fusion were adopted from Ross, which classified molars with fusion as fusion of entire root surface or one-third or less of the roots regardless of location of the fusion.13 As there are no criteria for defining C-shaped root canals, they were classified by the number of fused root, and subdivided by the root canal which constitutes the 'C' shape. In detail, if the C-shaped root canal was detected by the examiner, the number of roots was counted and then the involved canals in order were checked for naming it (e.g., Fusion of 2 roots, MB-P: C-shaped root canal made by 2 fused roots and the mesiobuccal root canal fused with palatal root canal).
The incidence of root fusion and C-shaped root canal between the first and the second molar was compared using Chi-square test. Statistical analysis was performed using SPSS (Version 18.0.0, SPSS Inc., Chicago, IL, USA) software. The differences were considered significant if the p value was less than 0.05.
Results
The type of root fusion was classified by the sequence of root which was fused. The roots and canals were briefly referred with abbreviation of capital letters, such as, B, buccal root/canal; MB, mesiobuccal root/canal; DB, distobuccal root/canal; P, palatal root/canal; MP, mesiopalatal root/canal; DP, distopalatal root/canal. The ' - ' between capital letters means fusion of roots or canals.
Total 9 types of root fusion are described in Table 1 and the representative CBCT images are presented. Generally, maxillary first and second molars have 3 roots. Therefore, the classification in the present study started with dividing fusion of 2 roots and fusion of 3 roots. There were also some teeth with 2 or 4 roots and those were classified into other types of root fusion. The difference between MB-DB-P and DB-MB-P was the sequence of fusion. The former made a C-shape with the opening to the mesial side, but the latter made a C-shape which opened to the distal side (Table 1). Teeth that have palatal root fused with mesiobuccal and distobuccal roots were divided into 2 types. In MB-P-DB (V-shape) type, fusion was done in serial manner and it looked like the letter 'V'. In 'All root' type, the cross-section image of coronal portion looked like the letter 'Y' or oval, and the cross-section image of the apical portion was circular (Table 1).
Table 2 presented the type and number of root fusion in maxillary first and second molars. Root fusion was present in 402 (11.3%) maxillary molars out of 3,553 teeth examined in this study. The incidence of root fusion was higher in maxillary second molars (345 teeth, 19.5%) than in maxillary first molars (57 teeth, 3.2%).
The type of C-shaped root canal was classified by each root canal which constitutes the 'C' shape. The abbreviations mean the same as used in root fusions. The fusion of root canals was classified into total 3 types according to the involved roots, and these types are also divided into subtypes. The classified types of C-shaped root canals are described with their representative CBCT images in Table 3.
From the representative images of each type of C-shaped root canal (Table 3), canals inside the roots may be separated even if the roots are fused. The C-shaped root canals could be formed by fusion of 2 roots (Type I) with the frequency of subtype C (MB-DB), subtype A (MB-P) and subtype B (DB-P) in a decreasing order. The two canals were fused partially or completely (Table 3). Larger C-shaped configuration was formed by fusion of 3 roots (Type II) with the similar frequency of subtype A (DB-MB-P) and subtype B (MB-P-DB) (Table 4). The three root canals were also fused partially or completely (Table 3). One tooth with 4 root canals was classified into Type III with the C-shaped root canal resulting from the fusion of MP with DP root canal observed in a maxillary second molar.
Table 4 shows the type and number of C-shaped root canals in maxillary first and second molars. Similar to root abbreviations, the capital letter represents each root canal instead of the root. C-shaped root canal configuration was present in 63 (1.8%) maxillary molars out of 3,553 teeth examined in this study. In first molars, the type of C-shaped root canal showed only Type I, subtype C (MB-DB: 15 teeth, 0.8%). In second molars, 48 teeth (2.7%) had C-shaped root canal and most common type was also Type I, subtype C (MB-DB: 29 teeth, 1.6%), followed by Type I, subtype A (MB-P: 11 teeth, 0.6%). The incidence of root fusion and C-shaped root canal was similar while their frequency in maxillary second molars was greater than that of maxillary first molars. Also, this difference was statistically significant (p < 0.001).
Discussion
This retrospective study investigated the incidence and type of root fusion and C-shaped root canals in the Korean maxillary molars using CBCT. Regarding the incidence of fusion in the maxillary first molars, our result (3.2%) was similar to those of Chinese (2.7%).14 Earlier studies in Burmese,15 Thai,16 Indian,17 and Chinese18 population reported no root fusion in maxillary first and second molars. Recent study in a Korean population reported 0.73% in the first molars.19 Other studies in the Caucasian,13 Chinese,20 and Irish population21 reported higher percentages of fusion in the first molars (7.7, 6.2, and 11.0%, respectively).
In the maxillary second molars, incidence of fusion (19.5%) was higher than the first molars, which is in accordance with the findings of several studies that reported higher prevalence in the second molar.13,19,20,21,22
Earlier studies in Caucasian,13 Chinese,20 and Irish population21 reported higher percentages (52.9, 40.1, and 43.0%, respectively). A recent study in a Korean population reported lower prevalence (10.7%) than our result in the second molars.19 These differences among several studies could be caused by ethnic background, sample size, age of the subject, method of study, and criteria for defining root fusion. Our criteria for defining root fusion were adopted from Ross who classified the tooth with fusion of one-third or less of the roots as having fused root.13 However, the study reported lower incidence when a different criteria of regarding roots as fused only when fusion occurred on the entire root surface.19 It is still difficult to classify root numbers and shapes because there are no generally accepted guidelines.16 For example, in our study it was difficult to distinguish between MB root fused with DB root and one buccal root with 2 canals that joined at the apical part (Vertucci type II). General guidelines and clear definition of root fusion are necessary for comparing the results from other studies and for future studies.
In many studies, root fusion was classified into 5 groups.20,21,22 But in this study, there were 9 types of root fusion because we separated fusion of all roots into 4 different types and presented two additional types. This classification provides more detailed information about morphology of maxillary molars. In our study, the most common type in the first molars was fusion of MB and DB roots. This result is consistent with previous reports.14,20,21,22 In the second molars, fusion of MB and P roots was the most common type in this study. This result is consistent with previous study in Chinese population,20 whereas other studies reported fusion of MB and DB roots as the most common type.21,22
There were a few studies which reported C-shaped root canal configuration in maxillary molars. In 2002, De Moor reported estimated incidence of 0.091% in maxillary first molars by evaluating radiographs retrospectively.23 In a study from Chinese population using clearing method, Yang et al. reported 4.9% of incidence in the maxillary second molars.20 Our result was higher than that of the study of De Moor in the first molars, and lower than that of the study by Yang et al. in the second molars. These differences also could be due to ethnic background, sample size, age of the subject, method of study, and criteria for defining C-shaped root canal. In the study of Yang et al., classification was defined by connected orifice that resembles the letter 'C'.20
Several variations of C-shaped root canals in maxillary molars were also reported clinically.23,24,25,26,27 Two earlier case reports described clinical cases of C-shaped root canal resulting from fusion of DB and P root canals.5,24 In our study, Type I, subtype B (DB-P) was similar to those cases. A previous study also reported 4 cases of C-shaped root canal resulting from fusion of DB and P roots (Type I, subtype B) in maxillary first molar.23 However, there were no Type I, subtype B (DB-P) in maxillary first molars in our study. Another previous study reported a case with Type I, subtype C (MB-DB).25 Two case reports using spiral CT or CBCT described that the C-shape resulted from merging of 2 palatal canals.26,27 In our study, 3 types with 6 subtypes were found. Among these types, Type 2, subtype B (MB-P-DB) has not been reported earlier. Other 5 types correspond to the types described in previous reports. In agreement with previous reports, C-shape may also result from partial fusion of root canals, not only from the entire root canals.26,27
The C-shaped root canal configuration in mandibular molars has typical root morphology and their classification has been well-documented and generally accepted.6,7,8 But in maxillary molars with C-shaped root canals, there is no common root morphology like mandibular second molar. And the C-shaped root canals are caused by different types of root fusion. Therefore, clear description and classification of C-shaped root canal configuration in maxillary molars are necessary.
Evaluation of root canal morphology employed many methods either in vivo or in vitro. The laboratory methods include canal staining and tooth clearing,15,16,20,21,28 sectioning,6,11
in vitro radiography,10
in vitro macroscopic examination22 and micro-computed tomography.7 The techniques used in clinical studies include intraoral radiography,9,13 reviews of patient records,23 examination during endodontic treatment29 and CBCT.14,17,18,19 The advantages of computed tomography (CT) are noninvasive, and it allows 3D reconstruction and visualization of the external and internal anatomy. CBCT allows higher resolution, shorter scan time and reduction in radiation exposure than traditional CT scans.30 From the obtained personal data such as sex, age, and tooth position, inappropriate tooth samples could be excluded which might be included in the studies using extracted teeth ensuring the accuracy of the research.14 In our study, subjects had CBCT examination for orthodontic diagnosis and treatment, not for our study. So, additional cost, time and radiation exposure for this study were unnecessary. The large numbers of sample size can be easily obtained respectively because of digital imaging system. Despite these advantages, at present, CBCT has lower resolution than conventional radiographs.30 Thus, more accurate methods, such as clearing technique or micro-computed tomography using extracted teeth is inevitable to obtain more detailed information of root canal anatomy. Further studies using these techniques are needed for thorough information about C-shaped root canal configuration in maxillary molars and successful root canal treatment of this specific anatomic variation.
There were some limitations in this study. First of all, the CBCT data were concentrated in young patients (mean age: 21.9 years). This age distribution may be difficult to generalize the results into every Korean population. Because of their young age, there were numerous teeth with immature root apex and canals under formation. To overcome the misinterpretation of the results, we thoroughly exclude the immature teeth and teeth with improper image quality. We also used precise analyzing program for investigating the morphologies of roots and canals. In the future studies, wide range of patient age should be included in the study. Second limitation could be a calibration of CBCT image reading. To minimize the errors, we designed two independent reading systems which composed of two endodontists. When the results are inconsistent, the data was re-evaluated together and discussion was done for final reading. So the possible errors could be considered to minimum level.
Conclusions
This retrospective study of young Korean adults using CBCT data showed the incidence and types of root fusion and C-shaped root canals in maxillary molars. These anatomic variations were more frequent in the maxillary second molars. Two roots fusion (MB-P), and C-shaped canal with Type 1, subtype C (MB-DB) were the most dominant type. Although C-shaped root canals are most frequently seen in the mandibular second molar, they may also appear in maxillary molars. As the root canal morphology is one of the most significant factors for successful root canal treatment, the clinician should perceive these variations in maxillary molars.
- 1. Cooke HG 3rd, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc 1979;99:836-839.ArticlePubMed
- 2. Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J 2002;35:56-62.ArticlePubMed
- 3. Bolger WL, Schindler WG. A mandibular first molar with a C-shaped root configuration. J Endod 1988;14:515-519.ArticlePubMed
- 4. Baisden MK, Kulild JC, Weller RN. Root canal configuration of the mandibular first premolar. J Endod 1992;18:505-508.ArticlePubMed
- 5. Newton CW, McDonald S. A C-shaped canal configuration in a maxillary first molar. J Endod 1984;10:397-399.ArticlePubMed
- 6. Melton DC, Krell KV, Fuller MW. Anatomical and histological features of C-shaped canals in mandibular second molars. J Endod 1991;17:384-388.ArticlePubMed
- 7. Fan B, Cheung GS, Fan M, Gutmann JL, Bian Z. C-shaped canal system in mandibular second molars: part I - anatomical features. J Endod 2004;30:899-903.ArticlePubMed
- 8. Jerome CE. C-shaped root canal systems: diagnosis, treatment, and restoration. Gen Dent 1994;42:424-427.PubMed
- 9. Trope M, Elfenbein L, Tronstad L. Mandibular premolars with more than one root canal in different race groups. J Endod 1986;12:343-345.ArticlePubMed
- 10. Weine FS, Hayami S, Hata G, Toda T. Canal configuration of the mesiobuccal root of the maxillary first molar of a Japanese sub-population. Int Endod J 1999;32:79-87.ArticlePubMed
- 11. Seo MS, Park DS. C-shaped root canals of mandibular second molars in a Korean population: clinical observation and in vitro analysis. Int Endod J 2004;37:139-144.ArticlePubMed
- 12. Yang ZP, Yang SF, Lin YC, Shay JC, Chi CY. C-shaped root canals in mandibular second molars in a Chinese population. Endod Dent Traumatol 1988;4:160-163.ArticlePubMed
- 13. Ross IF, Evanchik PA. Root fusion in molars: incidence and sex linkage. J Periodontol 1981;52:663-667.ArticlePubMed
- 14. Zheng QH, Wang Y, Zhou XD, Wang Q, Zheng GN, Huang DM. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod 2010;36:1480-1484.ArticlePubMed
- 15. Ng YL, Aung TH, Alavi A, Gulabivala K. Root and canal morphology of Burmese maxillary molars. Int Endod J 2001;34:620-630.ArticlePubMedPDF
- 16. Alavi AM, Opasanon A, Ng YL, Gulabivala K. Root and canal morphology of Thai maxillary molars. Int Endod J 2002;35:478-485.ArticlePubMed
- 17. Neelakantan P, Subbarao C, Ahuja R, Subbarao CV, Gutmann JL. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod 2010;36:1622-1627.ArticlePubMed
- 18. Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PM. Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J 2011;44:162-169.ArticlePubMed
- 19. Kim Y, Lee SJ, Woo J. Morphology of maxillary first and second molars analyzed by cone-beam computed tomography in a korean population: variations in the number of roots and canals and the incidence of fusion. J Endod 2012;38:1063-1068.ArticlePubMed
- 20. Yang ZP, Yang SF, Lee G. The root and root canal anatomy of maxillary molars in a Chinese population. Endod Dent Traumatol 1988;4:215-218.ArticlePubMed
- 21. al Shalabi RM, Omer OE, Glennon J, Jennings M, Claffey NM. Root canal anatomy of maxillary first and second permanent molars. Int Endod J 2000;33:405-414.ArticlePubMed
- 22. Pécora JD, Woelfel JB, Sousa Neto MD. Morphologic study of the maxillary molars. 1. External anatomy. Braz Dent J 1991;2:45-50.PubMed
- 23. De Moor RJ. C-shaped root canal configuration in maxillary first molars. Int Endod J 2002;35:200-208.ArticlePubMed
- 24. Dankner E, Friedman S, Stabholz A. Bilateral C shape configuration in maxillary first molars. J Endod 1990;16:601-603.ArticlePubMed
- 25. Yilmaz Z, Tuncel B, Serper A, Calt S. C-shaped root canal in a maxillary first molar: a case report. Int Endod J 2006;39:162-166.ArticlePubMed
- 26. Singla M, Aggarwal V. C-Shaped palatal canal in maxillary second molar mimicking two palatal canals diagnosed with the aid of spiral computerized tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:e92-e95.Article
- 27. Kottoor J, Velmurugan N, Ballal S, Roy A. Four-rooted maxillary first molar having C-shaped palatal root canal morphology evaluated using cone-beam computerized tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:e41-e45.ArticlePubMed
- 28. Manning SA. Root canal anatomy of mandibular second molars. Part II. C-shaped canals. Int Endod J 1990;23:40-45.PubMed
- 29. Haddad GY, Nehme WB, Ounsi HF. Diagnosis, classification, and frequency of C-shaped canals in mandibular second molars in the Lebanese population. J Endod 1999;25:268-271.ArticlePubMed
- 30. Tachibana H, Matsumoto K. Applicability of X-ray computerized tomography in endodontics. Endod Dent Traumatol 1990;6:16-20.ArticlePubMed
REFERENCES
Table 1
Classification of root fusion in maxillary first and second molars
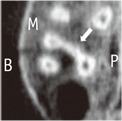

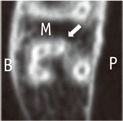
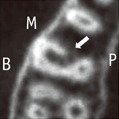
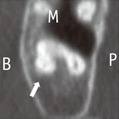
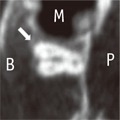
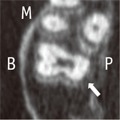

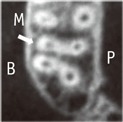
Table 2
Type and number of root fusion in maxillary first and second molars
' – ' means fusion of roots (ie, "MB-P" means mesiobuccal root fused with palatal root).
Values within parentheses are percentages of the total number of teeth in each column.
MB, mesiobuccal root; DB, distobuccal root; B, buccal root; P, palatal root; MP, mesiopalatal root; DP, distopalatal root.
*The difference between maxillary first molar and second molar was statistically significant (p < 0.05).
Table 3
Classification of C-shaped root canal in maxillary first and second molars
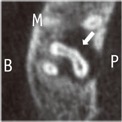
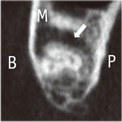




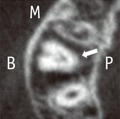
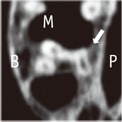
Table 4
Type and number of C-shaped root canal in maxillary first and second molars
' - 'means fusion of root canals that make C-shape.
Values within parentheses are percentages of the total number of teeth in each column.
MB, mesiobuccal root canal; DB, distobuccal root canal; P, palatal root canal; MP, mesiopalatal root canal; DP, distopalatal root canal.
*The difference between maxillary first molar and second molar was statistically significant (p < 0.05).
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Prevalence of C‐Shaped Canals in Maxillary Molars in an Iranian Population: A Cone‐Beam Computed Tomography Analysis
Amin Salem Milani, Shahin Namvar Asl Amirkhizi, Tahmineh Razi, Ahmad Nouroloyouni, Pouya Sabanik, Nikhat Kaura
International Journal of Clinical Practice.2026;[Epub] CrossRef - Prevalence of c-shaped canal morphology in premolar and molar teeth assessed by cone-beam computed tomography: systematic review and meta-analysis
Faezeh Yousefi, Younes Mohammadi, Elham Shokri
BMC Oral Health.2025;[Epub] CrossRef - A Cone‐Beam Computed Tomography Evaluation of C‐Shaped Canal Configuration in Maxillary Molars Among an Iranian Population
Nafiseh Nikkerdar, Mohammad Moslehi, Amin Golshah, Mario Dioguardi
International Journal of Dentistry.2024;[Epub] CrossRef - Endodontic treatment of a C‐shaped mandibular second molar with narrow dentinal thickness: A case report
Mina Mehrjouei, Hamid Jafarzadeh, Pourya Esmaeelpour, Maryam Khorasanchi
Clinical Case Reports.2024;[Epub] CrossRef - Evaluation of 2- and 3-dimensional anatomic parameters of C-shaped root canals with cone beam computed tomography, microcomputed tomography, and nanocomputed tomography
Miguel Angel Ventura Molina, Giovane Oliveira Silva, Amanda Pelegrin Candemil, Rafael Verardino de Camargo, Ruben Pauwels, Reinhilde Jacobs, Manoel Damião Sousa-Neto, Jardel Francisco Mazzi-Chaves
Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology.2023; 136(6): 759. CrossRef - Cone-Beam Computed Tomography (CBCT) Analysis of an Unusual Configuration of the Upper First Molar With a C-shaped Canal With Apically Fused Roots: A Case Report
Kapil D Wahane, Anand V Bansod, Sudha mattigatti, Rushikesh Mahaparale, Yuvraj B Rote, Mayur B Wanjari
Cureus.2023;[Epub] CrossRef - Assessment of C-Shaped Canal Morphology in Mandibular and Maxillary Second Molars in an Iraqi Subpopulation Using Cone-Beam Computed Tomography
Kazhan Abdalrahman, Ranjdar Talabani, Sara Kazzaz, Dlsoz Babarasul, Berndt Koslowski
Scanning.2022; 2022: 1. CrossRef - Root and canal-specific features of maxillary first molars with fused roots
Katarina Beljic-Ivanovic, Branislav Karadzic
Vojnosanitetski pregled.2022; 79(11): 1092. CrossRef - Diagnosis and treatment of maxillary molar with abnormality
Kkot-Byeol Bae, Bin-Na Lee, Hoon-Sang Chang, In-Nam Hwang, Won-Mann Oh, Yun-Chan Hwang
Oral Biology Research.2022; 46(4): 195. CrossRef - Endodontic treatment of the maxillary first molar with palatal canal variations: A case report and review of literature
Kai Chen, Xing Ran, Yan Wang
World Journal of Clinical Cases.2022; 10(32): 12036. CrossRef - Evaluation of C-shaped canals in maxillary molars in a Chinese population using CBCT
Yuyan Qian, Yamei Li, Jukun Song, Ping Zhang, Zhu Chen
BMC Medical Imaging.2022;[Epub] CrossRef - Comprehensive evaluation of root and root canal morphology of mandibular second molars in a Saudi subpopulation evaluated by cone-beam computed tomography
Moazzy I. Almansour, Saad M. Al‑Zubaidi, Abdulmjeed S. Enizy, Ahmed A. Madfa
BMC Oral Health.2022;[Epub] CrossRef - Evaluation of C-shaped canal configuration in maxillary molars: A retrospective cone-beam computed tomography study
Emre KÖSE, Rüya AK
Clinical and Experimental Health Sciences.2021; 11(3): 444. CrossRef - Maxillary First Molars with Two Palatal Root Canals
Kun-Hwa Sung, Ho-Keel Hwang, Hyoung-Hoon Jo, Konstantinos Michalakis
Case Reports in Dentistry.2021;[Epub] CrossRef - Preferred Reporting Items for Epidemiologic Cross-sectional Studies on Root and Root Canal Anatomy Using Cone-beam Computed Tomographic Technology: A Systematized Assessment
Jorge N.R. Martins, Anil Kishen, Duarte Marques, Emmanuel João Nogueira Leal Silva, João Caramês, António Mata, Marco A. Versiani
Journal of Endodontics.2020; 46(7): 915. CrossRef - Evaluation of root and root canal morphology of elderly Korean patients maxillary molars using cone-beam computed tomography
Tae-Yong Lee, Mi-Yeon Kim, Sun-Ho Kim, Jeong-Hee Kim
The Journal of Korean Academy of Prosthodontics.2020; 58(2): 95. CrossRef - Second mesiobuccal root canal in maxillary molars—A systematic review and meta-analysis of prevalence studies using cone beam computed tomography
Jorge N.R. Martins, Duarte Marques, Emmanuel João Nogueira Leal Silva, João Caramês, António Mata, Marco A. Versiani
Archives of Oral Biology.2020; 113: 104589. CrossRef - Prevalência estimada de canais “C- Shaped”: Uma revisão sistemática e meta-análise
Natália Pereira da Silva Falcão, Sandro Junio de Oliveira Tavares, Ludmila Silva Guimarães, Katherine Azevedo Batistela Rodrigues Thuller, Leonardo dos Santos Antunes, Estefano Borgo Sarmento, Fellipe Navarro Azevedo de Azevedo, Cinthya Cristina Gomes, Ca
Revista Científica Multidisciplinar Núcleo do Conhecimento.2020; : 91. CrossRef - Evaluation of the internal anatomy of paramolar tubercles using cone-beam computed tomography
G. Colakoglu, I. Kaya Buyukbayram, M. A. Elcin, M. Kazak, H. Sezer
Surgical and Radiologic Anatomy.2020; 42(1): 15. CrossRef - Analysis of Prevalence of Pyramidal Molars in Adolescent
Woojin Kwon, Hyung-Jun Choi, Jaeho Lee, Je Seon Song
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2020; 47(4): 389. CrossRef - Prevalence Studies on Root Canal Anatomy Using Cone-beam Computed Tomographic Imaging: A Systematic Review
Jorge N.R. Martins, Duarte Marques, Emmanuel João Nogueira Leal Silva, João Caramês, Marco A. Versiani
Journal of Endodontics.2019; 45(4): 372. CrossRef - Fused roots of maxillary molars: characterization and prevalence in a Latin American sub-population: a cone beam computed tomography study
Maytté Marcano-Caldera, Jose Luis Mejia-Cardona, María del Pilar Blanco-Uribe, Elena Carolina Chaverra-Mesa, Didier Rodríguez-Lezama, Jose Hernán Parra-Sánchez
Restorative Dentistry & Endodontics.2019;[Epub] CrossRef - An original micro‐CT study and meta‐analysis of the internal and external anatomy of maxillary molars—implications for endodontic treatment
Iwona M. Tomaszewska, Anna Jarzębska, Bendik Skinningsrud, Przemysław A. Pękala, Sebastian Wroński, Joe Iwanaga
Clinical Anatomy.2018; 31(6): 838. CrossRef - A Cone-beam Computed Tomographic Study of Root and Canal Morphology of Maxillary First and Second Permanent Molars in a Thai Population
Roserin Ratanajirasut, Anchana Panichuttra, Soontra Panmekiate
Journal of Endodontics.2018; 44(1): 56. CrossRef - Retrospective Assessment of Healing Outcome of Endodontic Treatment for Mandibular Molars with C-shaped Root Canal
Kishore Kumar Majety, Basanta Kumar Choudhury, Anika Bansal, Achla Sethi, Jaina Panjabi
The Journal of Contemporary Dental Practice.2017; 18(7): 591. CrossRef - The morphology of maxillary first and second molars analyzed by cone-beam computed tomography in a polish population
Katarzyna Olczak, Halina Pawlicka
BMC Medical Imaging.2017;[Epub] CrossRef
 ePub Link
ePub Link Cite
Cite- Related articles
-
- Determination of optimal horizontal beam angulations for canal separation in mandibular molars using cone-beam computed tomography: a retrospective image-based analysis
- Dentin thickness of C-shaped root canal walls in mandibular premolars based on cone-beam computed tomography: a retrospective cross-sectional study
Analysis of C-shaped root canal configuration in maxillary molars in a Korean population using cone-beam computed tomography
Analysis of C-shaped root canal configuration in maxillary molars in a Korean population using cone-beam computed tomography
Classification of root fusion in maxillary first and second molars
| Type of root fusion | CBCT Image representing the type | Description | |
|---|---|---|---|
| Fusion of 2 roots | MB-P | Mesiobuccal root fused with palatal root | |
| DB-P | Distobuccal root fused with palatal root | ||
| MB-DB | Mesiobuccal root fused with distobuccal root | ||
| Fusion of 3 roots | MB-DB-P | Mesiobuccal root fused with distobuccal root and palatal root | |
| DB-MB-P | Distobuccal root fused with mesiobuccal root and palatal root | ||
| MB-P-DB (V shape) | Mesiobuccal root fused with palatal root and distobuccal root | ||
| All root (Y or cone shape) | All 3 roots are fused to apical direction without any sequence | ||
| Other types of root fusion | B-P (teeth with 2 root) | Single buccal root fused with palatal root | |
| MB-MP and DB-DP | Mesiobuccal root fused with mesiopalatal root and distobuccal root fused with distopalatal root | ||
In the CBCT image, the arrows indicate the fusion of examined teeth, the capital letter indicate each aspect.
CBCT, cone-beam computed tomography; M, Mesial; B, Buccal; P, Palatal.
Type and number of root fusion in maxillary first and second molars
| Type of root fusion | Total (n = 3,553) | Maxillary first molar (n = 1,786) | Maxillary second molar (n = 1,767) | ||
|---|---|---|---|---|---|
| Fusion of 2 roots | MB-P | 217 (6.1) | 129 (3.6) | 6 (0.3) | 123 (7.0) |
| DB-P | 16 (0.4) | 11 (0.6) | 5 (0.3) | ||
| MB-DB | 72 (2.0) | 31 (1.7) | 41 (2.3) | ||
| Fusion of 3 roots | MB-DB-P | 124 (3.4) | 7 (0.2) | 6 (0.3) | 1 (0.1) |
| DB-MB-P | 40 (1.1) | 0 (0.0) | 40 (2.3) | ||
| MB-P-DB (V shape) | 15 (0.4) | 2 (0.1) | 13 (0.7) | ||
| All root (Y or cone shape) | 62 (1.7) | 0 (0.0) | 62 (3.5) | ||
| Other types of root fusion | B-P (teeth with 2 root) | 61 (1.7) | 60 (1.68) | 1 (0.1) | 59 (3.3) |
| MB-MP and DB-DP | 1 (0.03) | 0 (0.0) | 1 (0.1) | ||
| Total | 402 (11.3) | 57 (3.2)* | 345 (19.5)* | ||
' – ' means fusion of roots (ie, "MB-P" means mesiobuccal root fused with palatal root).
Values within parentheses are percentages of the total number of teeth in each column.
MB, mesiobuccal root; DB, distobuccal root; B, buccal root; P, palatal root; MP, mesiopalatal root; DP, distopalatal root.
*The difference between maxillary first molar and second molar was statistically significant (p < 0.05).
Classification of C-shaped root canal in maxillary first and second molars
| Type of C-shaped root canal | CBCT Image representing the type | Description | |
|---|---|---|---|
| Type I Fusion of 2 root canals | Subtype A MB-P | mesiobuccal root canal fused with palatal root canal (fusion of 2 roots) | |
| mesiobuccal root canal fused with palatal root canal (fusion of 3 roots) | |||
| Subtype B DB-P | distobuccal root canal fused with palatal root cana | ||
| Subtype C MB-DB | mesiobuccal root canal fused with distobuccal root canal (fusion of 2 roots) | ||
| mesiobuccal root canal fused with distobuccal root canal (fusion of 3 roots) | |||
| Type II Fusion of 3 root canals | Subtype A DB-MB-P | distobuccal root canal fused with mesiobuccal root canal and palatal root canal | |
| Subtype B MB-P-DB (V shape) | mesiobuccal root canal fused with palatal root canal and distobuccal root canal | ||
| Type III Other type of root canal fusion | MP-DP (tooth with 4 root canals) | mesiopalatal root canal fused with distopalatal root canal | |
In the CBCT image, the arrows indicate the C-shaped root canal of examined teeth, the capital letter indicate each aspect.
M, Mesial; B, Buccal; P, Palatal.
Type and number of C-shaped root canal in maxillary first and second molars
| Type of C-shaped root canal | Total (n = 3,553) | Maxillary first molar (n = 1,786) | Maxillary second molar (n = 1,767) | ||
|---|---|---|---|---|---|
| Type I Fusion of 2 roots | Subtype A: MB-P | 57 (1.6) | 11 (0.3) | 0 (0.0) | 11 (0.6) |
| Subtype B: DB-P | 2 (0.06) | 0 (0.0) | 2 (0.1) | ||
| Subtype C: MB-DB | 44 (1.2) | 15 (0.8) | 29 (1.6) | ||
| Type II Fusion of 3 roots | Subtype A: DB-MB-P | 5 (0.14) | 3 (0.08) | 0 (0.0) | 3 (0.2) |
| Subtype B: MB-P-DB (V shape) | 2 (0.06) | 0 (0.0) | 2 (0.1) | ||
| Type III Other type of root canal fusion | MP-DP (teeth with 4 root canals) | 1 (0.03) | 0 (0.0) | 1 (0.1) | |
| Total | 63 (1.8) | 15 (0.8)* | 48 (2.7)* | ||
' - 'means fusion of root canals that make C-shape.
Values within parentheses are percentages of the total number of teeth in each column.
MB, mesiobuccal root canal; DB, distobuccal root canal; P, palatal root canal; MP, mesiopalatal root canal; DP, distopalatal root canal.
*The difference between maxillary first molar and second molar was statistically significant (p < 0.05).
Table 1 Classification of root fusion in maxillary first and second molars
In the CBCT image, the arrows indicate the fusion of examined teeth, the capital letter indicate each aspect. CBCT, cone-beam computed tomography; M, Mesial; B, Buccal; P, Palatal.
Table 2 Type and number of root fusion in maxillary first and second molars
' – ' means fusion of roots (ie, "MB-P" means mesiobuccal root fused with palatal root). Values within parentheses are percentages of the total number of teeth in each column. MB, mesiobuccal root; DB, distobuccal root; B, buccal root; P, palatal root; MP, mesiopalatal root; DP, distopalatal root. *The difference between maxillary first molar and second molar was statistically significant (
Table 3 Classification of C-shaped root canal in maxillary first and second molars
In the CBCT image, the arrows indicate the C-shaped root canal of examined teeth, the capital letter indicate each aspect. M, Mesial; B, Buccal; P, Palatal.
Table 4 Type and number of C-shaped root canal in maxillary first and second molars
' - 'means fusion of root canals that make C-shape. Values within parentheses are percentages of the total number of teeth in each column. MB, mesiobuccal root canal; DB, distobuccal root canal; P, palatal root canal; MP, mesiopalatal root canal; DP, distopalatal root canal. *The difference between maxillary first molar and second molar was statistically significant (

