
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 40(1); 2015 > Article
- Research Article Calcium hydroxide dressing residues after different removal techniques affect the accuracy of Root-ZX apex locator
- Emel Uzunoglu, Ayhan Eymirli, Mehmet Özgür Uyanik, Semra Çalt, Emre Nagas
-
2014;40(1):-49.
DOI: https://doi.org/10.5395/rde.2015.40.1.44
Published online: November 5, 2014
Department of Endodontics, Faculty of Dentistry, Hacettepe University, Ankara, Turkey.
- Correspondence to Emel Uzunoglu, DDS, PhD. Research Assistant, Department of Endodontics, Faculty of Dentistry, Hacettepe University, Sihhiye, 06100 Ankara, Turkey. TEL, +903123052260; FAX, +903123104440; emel_dt@hotmail.com
• Received: June 14, 2014 • Accepted: September 11, 2014
©Copyrights 2015. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,582 Views
- 10 Download
- 16 Crossref
Abstract
-
Objectives This study compared the ability of several techniques to remove calcium hydroxide (CH) from the root canal and determined the influence of CH residues on the accuracy of the electronic apex locator.
-
Materials and Methods Root canals of 90 human maxillary lateral incisors with confirmed true working length (TWL) were prepared and filled with CH. The teeth were randomly assigned to one of the experimental groups according to the CH removal technique (n = 14): 0.9% saline; 0.9% saline + master apical file (MAF); 17% ethylenediamine tetraacetic acid (EDTA); 17% EDTA + MAF; 5.25% sodium hypochlorite (NaOCl); 5.25% NaOCl + MAF. Six teeth were used as negative control. After CH removal, the electronic working length was measured using Root-ZX (Morita Corp.) and compared with TWL to evaluate Root-ZX accuracy. All specimens were sectioned longitudinally, and the area of remaining CH (CH) and total canal area were measured using imaging software.
-
Results The EDTA + MAF and NaOCl + MAF groups showed better CH removal than other groups (p < 0.05). Root-ZX reliability to prevent overestimated working length to be > 85% within a tolerance of ± 1.0 mm (p < 0.05). There was strong negative correlation between amount of CH residues and EAL accuracy (r = -0.800 for ± 0.5 mm; r = -0.940 for ± 1.0 mm).
-
Conclusions The mechanical instrumentation improves the CH removal of irrigation solutions although none of the techniques removed the dressing completely. Residues of CH medication in root canals affected the accuracy of Root-ZX adversely.
Introduction
The determination of correct working length is essential for effective cleaning and shaping and it influences the clinical success of root canal treatment.1,2 Both radiographic and electronic methods have been used for correct working length determination. However, periapical radiographs have many limitations in determining the working length.3 Therefore, in search of more accurate working length measurements, electronic apex locators (EALs) have developed and nowadays are regarded as important tools in clinical endodontic practice and currently used in several clinical conditions.4 Although the function of EALs is consistent in 97% of cases, various factors (root canal pre-enlargement, different endodontic solutions, file size, stage of apex formation, retreatment procedures) affect the accuracy of different EALs.5,6
Although instrumentation procedures have improved considerably over the years, none of the existing techniques can completely clean the root canal system.1 Therefore, besides instrumentation, intracanal medication has been recommended in order to disinfect the root canal system and to improve the success of the root canal treatment, especially in multiple-visit cases.7 Calcium hydroxide (CH) mixed with an appropriate vehicle has become established as the most frequently used endodontic intracanal medicament owing to its good antimicrobial properties against the vast majority of endodontically relevant pathogens and its good biocompatibility.8,9 However, if this medication is not completely removed from the root canal, its presence on the dentin walls could compromise the endodontic treatment.10,11 Hence, CH dressing removal prior to the permanent root canal filling is required.12 The removal of CH is usually accomplished through several irrigation regimens in conjunction with different instrumentation techniques.12,13,14 During the removal, the most frequently described method is instrumentation of the root canal using a master apical file (MAF) and copious irrigation.13,15 However, it has been reported that the removal of CH from the root canal wall is difficult, because instrumentation and irrigation alone cannot completely clean the entire root canal.12,13,15,16
Moreover, no information is available regarding the influence of residual CH on the accuracy of EALs. Thus, the aim of this ex vivo study was to compare the ability of several techniques to remove CH from the root canal and to determine the influence of CH residues on the accuracy of the EAL.
Materials and Methods
Ninety maxillary lateral incisors with straight roots were used. Each tooth was decoronated at approximately the cemento-enamel junction (CEJ) to provide a flat horizontal surface to serve as a stable and unequivocal reference for all measurements. Root canal patency was evaluated using a size 10 K-file to discard any teeth with canal obstructions. After access preparation, a size 15 K-file was inserted into each canal until the tip of the file became visible through the foramen under microscope (×12). The file was then withdrawn until its tip lied tangential to the apical foramen. The silicone stop was adjusted to the nearest flat anatomical tooth landmark chosen as reference for root canal measurement. The distance from the base of the silicone stop to the file tip was measured under ×4.5 magnification with a millimeter ruler to the nearest 0.25 mm. Then 0.5 mm was subtracted from the measurement. Each measurement was repeated three times and the mean value calculated and computed. This value was recorded for each tooth as the reference length and registered as the true working length (TWL).17,18
The root canals were prepared using ProTaper rotary instruments (Dentsply-Maillefer, Ballaigues, Switzerland) up to master apical file F3 (size 30). Between each instrument, the canals were irrigated with 2 mL of 5.25% sodium hypochlorite (NaOCl), using a syringe and a 27 gauge-needle that was placed 2 mm short of the TWL. Prepared root canals were rinsed with 5 mL 17% ethylenediamine tetraacetic acid (EDTA, Vista Dental Products, Racine, WI, USA), followed by a final rinse of 5 mL distilled water, and were dried using paper points. Then, the canals were filled with an injectable CH paste (SurePaste, SureDent Co., Ltd., Seongnam, Korea). Then, radiographs were taken in mesiodistal and bucco-lingual directions to confirm the complete filling of the canals. The access cavities were temporarily sealed with cotton pellet and temporary filling material (Cavit, 3M ESPE, Seefeld, Germany). They were then stored at 37℃ and 100% relative humidity for 7 days. The teeth were randomly distributed amongst six experimental groups (n = 14) and a control group (n = 6) according to CH removal techniques (Table 1).
Electronic measurement was achieved using EAL (Root-ZX, J. Morita Corp., Tokyo, Japan) after performing CH removal techniques described in Table 1. Then, for the electronic working length (EWL) measurement, the test tubes were filled with 0.9% physiologic saline solution as an electrolyte such that the apical third of the roots was immersed into the liquid.19,20 Only one specialist (experienced in the use of EALs) measured the actual and also electronic lengths.17 To avoid bias, the measurements were taken by randomizing the order of the teeth. For the electronic measurements, the same sized (size 30) and the same tapered master apical Ni-Ti file was used with after removal of CH. The termination point used in this study was the red line on the meter designated by the manufacturer as the 'APEX' and measurements were done between 'APEX' and 1.0 mm points (green area). The silicone stop was adjusted to the nearest flat anatomical tooth landmark again and the distance from the base of the silicone stop to the file tip was measured under ×4.5 magnification with a caliper to the nearest 0.25 mm and registered the measured length as EWL. Each measurement was repeated three times and the mean value calculated and computed. The TWL was compared with the EWL. Differences were calculated (TWL - EWL), and tolerance limits of ± 0.5 and ± 1.0 mm were taken.21 A negative difference indicated that EWL was larger and file tip had crossed the foramen. A positive difference indicated that tip was short of foramen. The accuracy of Root-ZX was evaluated in terms of percentages of acceptable measurements (tolerance limit of ± 0.5 and ± 1.0 mm). Chi-square tests were used to compare the percentages (p < 0.05).
Thereafter, grooves were prepared with a water-cooled diamond bur on the buccal and lingual surfaces and the teeth were split along their long axis in a bucco-lingual direction using a surgical chisel.13 Both halves of the root canal were evaluated under a stereomicroscope (Olympus Corporation, Taichung, Taiwan) at ×40 magnification and photographed digitally. Digital images were imported into image analyzer software (Comef 4.3, OEG Messtechnik, Frankfurt, Germany), and the area occupied by the residual CH on the canal walls was measured (mm2). One-way ANOVA with post-hoc least significant difference (LSD) test was used for statistical analysis of collected data at a significance level of 5%. Pearson's correlation test was done to analyze the correlation between the amount of CH residues and EAL accuracy.
Results
The calculated Root-ZX accuracy (%) and the amount of residual CH (%) are presented in Table 1. There was statistically significant effect of different removal techniques tested on the accuracy of Root-ZX for tolerance limits of ± 0.5 and ± 1.0 mm (χ2 test, p < 0.05). Within ± 0.5 mm accuracy, control group's measurements was statistically different from experimental groups and within ± 1.0 mm accuracy, control and 5.25% NaOCl + MAF groups' measurements were significantly different from other groups (χ2 test, p < 0.05). When the 17% EDTA + MAF and 5.25% NaOCl + MAF were used, EAL was accurate more than 85% of the time to ± 1.0 mm from the apical foramen (Table 1). However, the EAL accuracy was 28.6% of the time to ± 0.5 mm for saline and EDTA without MAF groups. In control group, EWL measurements were always shorter than TWL even when the file extruded from apical foramen.
The 17% EDTA and MAF group and 5.25% NaOCl and MAF group showed better removal efficiency than other groups (p < 0.05, Figure 1). MAF (hand filing) improved the removal efficiency of irrigation solutions (p < 0.05). Control group showed complete coverage of the canal walls with CH remnants densely packed in the canals (Figure 1).
Pearson's correlation coefficient (r) showed that there was strong negative correlation between amount of CH residues and EAL accuracy (r = -0.800 for ± 0.5 mm; r = -0.940 for ± 1.0 mm).
Discussion
The present study was designed to assess the efficacy of different techniques for CH removal by means of a sectioning technique and to evaluate the influence of CH remnants in root canal on the accuracy of Root-ZX apex locator, in vitro. A number of methods for investigating EALs have been used in which extracted teeth were immersed in various media with electrical resistance similar to the periodontium. The advantages of these in vitro models were their simplicity, ease of use and the ability to have strict control over the experimental conditions tested. Furthermore, a greater number of canals can be tested over a shorter period of time than could have been achieved by clinical means.22 The removal of CH from radicular dentin is essential in order to maintain the integrity of the root canal seal.10,23
In the present study, the complete removal of CH from the canal walls was not obtained with any protocol tested. This result is similar to the findings of previous studies tried to achieve the best protocol to remove CH medicament before root canal filling and showed considerable amounts of CH remaining on the canal walls, notwithstanding the removal technique used.14,15,24 Compared with the NaOCl and EDTA-only groups, the combined use of NaOCl and EDTA with MAF (hand filing) improved the removal efficiency. This is in agreement with the results of a previous study, which showed the importance of recapitulation using MAF to improve the removal of CH.25 On the other hand, irrigation only with 17% EDTA performed significantly better results than those of saline and 5.25% NaOCl. This can be explained by the ability of EDTA to dissolve inorganic substances such as calcium.24 Calt and Serper reported complete removal of CH from the root canal after irrigation with EDTA and NaOCl in comparison with NaOCl alone.23 However, a previous study using the same irrigation regime (EDTA and NaOCl) could not confirm these results and still found extensive remnants of CH.15 Similarly, in the present study, although the most successful method of CH removal was EDTA + MAF combination, there is no evidence that EDTA can completely remove CH from the root canal. This difference could be a result of the variable dimensions of the root canal system and their subsequent preparation size and taper, which affects the irrigant penetration.
High reliability index in readings and more precise measurements compared with other apex locators in previous studies were the reasons to use Root-ZX Apex locater in the present study.18,26,27 McDonald recommended the use of files with sizes comparable with the root canal diameter claiming that this would result in more accurate readings.28 Hence, in the present study, the electronic measurements were performed with the same sized and the same tapered master apical Ni-Ti file after removal of CH, while the TWL measurement was done with size 15 stainless-steel K-file. Manufacturers of new-generation EALs claim that these new devices are not affected from the irrigation solutions, and work even in the presence of electrolytes without calibration.29,30 Previous studies reported that with either 5% NaOCl or 14% to 17% EDTA, no interference in detecting the apical foramen was observed.31,32 Goldberg et al. reported that the Root-ZX to be 62.7 to 68.0% accurate within ± 0.5 mm, while Dunlap et al. reported that 82% of electronic values recorded with the Root-ZX were accurate within ± 0.5 mm of the apical constriction when 2.5% NaOCl was used.33,34 In this study, accuracy values of EAL were 50.0 to 64.3% within ± 0.5 mm, when 5.25% NaOCl was used. Against those results, Haffner et al. compared some EALs under in vivo conditions and found Root-ZX more accurate when the root canals were dried with paper points.35 According to the present results, 5.25% NaOCl showed most accurate results amongst the irrigants. Moreover, EAL accuracy were enhanced when MAF combined with irrigation procedure in all groups, except for the control group within ± 0.5 and also ± 1.0 mm. Although CH residues were less in 17% EDTA and MAF group than in 5.25% NaOCl and MAF group, electronic measurements were significantly more accurate in latter group than other MAF combined groups. This can be explained with highly electro-conductive property of NaOCl, resulting in the reduction of electrical impedance of the root canal wall and the better electrical contact with the apical tissues as well.36
Conclusions
Within the limitations of this study none of the irrigants or their combination with MAF filing removed the CH completely. Nevertheless, the results of this study suggest that the addition of hand instrumentation to irrigation is more effective in removing CH from the root canal than irrigation alone. The CH dressing residues affected the accuracy of EAL adversely.
Acknowledgment
Authors are grateful to Sevilay Karahan for statistical assistance.
- 1. Hülsmann M, Peters OA, Dummer PMH. Mechanical preparation of root canals: shaping goals, techniques and means. Endod Topics 2005;10:30-76.Article
- 2. Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J 2008;41:339-344.ArticlePubMed
- 3. Vieyra JP, Acosta J. Comparison of working length determination with radiographs and four electronic apex locators. Int Endod J 2011;44:510-518.ArticlePubMed
- 4. Martins JN, Marques D, Mata A, Caramês J. Clinical efficacy of electronic apex locators: systematic review. J Endod 2014;40:759-777.ArticlePubMed
- 5. de Camargo EJ, Zapata RO, Medeiros PL, Bramante CM, Bernardineli N, Garcia RB, de Moraes IG, Duarte MA. Influence of preflaring on the accuracy of length determination with four electronic apex locators. J Endod 2009;35:1300-1302.ArticlePubMed
- 6. Aggarwal V, Singla M, Kabi D. An in vitro evaluation of performance of two electronic root canal length measurement devices during retreatment of different obturating materials. J Endod 2010;36:1526-1530.ArticlePubMed
- 7. Kawashima N, Wadachi R, Suda H, Yeng T, Parashos P. Root canal medicaments. Int Dent J 2009;59:5-11.ArticlePubMed
- 8. Siqueira JF Jr, Magalhães KM, Rôças IN. Bacterial reduction in infected root canals treated with 2.5% NaOCl as an irrigant and calcium hydroxide/camphorated paramonochlorophenol paste as an intracanal dressing. J Endod 2007;33:667-672.ArticlePubMed
- 9. Athanassiadis B, Abbott PV, Walsh LJ. The use of calcium hydroxide, antibiotics and biocides as antimicrobial medicaments in endodontics. Aust Dent J 2007;52(Supplement 1):S64-S82.ArticlePubMed
- 10. Kim SK, Kim YO. Influence of calcium hydroxide intracanal medication on apical seal. Int Endod J 2002;35:623-628.ArticlePubMed
- 11. Vilela DD, Neto MM, Villela AM, Pithon MM. Evaluation of interference of calcium hydroxide-based intracanal medication in filling root canal systems. J Contemp Dent Pract 2011;12:368-371.ArticlePubMed
- 12. Nandini S, Velmurugan N, Kandaswamy D. Removal efficiency of calcium hydroxide intracanal medicament with two calcium chelators: volumetric analysis using spiral CT, an in vitro study. J Endod 2006;32:1097-1101.ArticlePubMed
- 13. Lambrianidis T, Kosti E, Boutsioukis C, Mazinis M. Removal efficacy of various calcium hydroxide/chlorhexidine medicaments from the root canal. Int Endod J 2006;39:55-61.ArticlePubMed
- 14. Kenee DM, Allemang JD, Johnson JD, Hellstein J, Nichol BK. A quantitative assessment of efficacy of various calcium hydroxide removal techniques. J Endod 2006;32:563-565.ArticlePubMed
- 15. Lambrianidis T, Margelos J, Beltes P. Removal efficiency of calcium hydroxide dressing from the root canal. J Endod 1999;25:85-88.ArticlePubMed
- 16. Wu MK, van der Sluis LW, Wesselink PR. The capability of two hand instrumentation techniques to remove the inner layer of dentine in oval canals. Int Endod J 2003;36:218-224.ArticlePubMedPDF
- 17. Thomas AS, Hartwell GR, Moon PC. The accuracy of the Root ZX electronic apex locator using stainless-steel and nickel-titanium files. J Endod 2003;29:662-663.ArticlePubMed
- 18. Plotino G, Grande NM, Brigante L, Lesti B, Somma F. Ex vivo accuracy of three electronic apex locators: Root ZX, Elements Diagnostic Unit and Apex Locator and ProPex. Int Endod J 2006;39:408-414.ArticlePubMed
- 19. Hör D, Krusy S, Attin T. Ex vivo comparison of two electronic apex locators with different scales and frequencies. Int Endod J 2005;38:855-859.ArticlePubMed
- 20. Stoll R, Urban-Klein B, Roggendorf MJ, Jablonski-Momeni A, Strauch K, Frankenberger R. Effectiveness of four electronic apex locators to determine distance from the apical foramen. Int Endod J 2010;43:808-817.ArticlePubMed
- 21. Pascon EA, Marrelli M, Congi O, Ciancio R, Miceli F, Versiani MA. An ex vivo comparison of working length determination by 3 electronic apex locators. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e147-e151.ArticlePubMed
- 22. Erdemir A, Eldeniz AU, Ari H, Belli S, Esener T. The influence of irrigating solutions on the accuracy of the electronic apex locator facility in the Tri Auto ZX handpiece. Int Endod J 2007;40:391-397.ArticlePubMed
- 23. Calt S, Serper A. Dentinal tubule penetration of root canal sealers after root canal dressing with calcium hydroxide. J Endod 1999;25:431-433.ArticlePubMed
- 24. Rödig T, Vogel S, Zapf A, Hülsmann M. Efficacy of different irrigants in the removal of calcium hydroxide from root canals. Int Endod J 2010;43:519-527.ArticlePubMed
- 25. Salgado RJ, Moura-Netto C, Yamazaki AK, Cardoso LN, de Moura AA, Prokopowitsch I. Comparison of different irrigants on calcium hydroxide medication removal: microscopic cleanliness evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:580-584.ArticlePubMed
- 26. Duran-Sindreu F, Stöber E, Mercadé M, Vera J, Garcia M, Bueno R, Roig M. Comparison of in vivo and in vitro readings when testing the accuracy of the Root ZX apex locator. J Endod 2012;38:236-239.ArticlePubMed
- 27. D'Assunção FL, Albuquerque DS, Salazar-Silva JR, Dos Santos VC, Sousa JC. Ex vivo evaluation of the accuracy and coefficient of repeatability of three electronic apex locators using a simple mounting model: a preliminary report. Int Endod J 2010;43:269-274.ArticlePubMed
- 28. McDonald NJ. The electronic determination of working length. Dent Clin North Am 1992;36:293-307.ArticlePubMed
- 29. Jenkins JA, Walker WA 3rd, Schindler WG, Flores CM. An in vitro evaluation of the accuracy of the root ZX in the presence of various irrigants. J Endod 2001;27:209-211.ArticlePubMed
- 30. Kang JA, Kim SK. Accuracies of seven different apex locators under various conditions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:e57-e62.ArticlePubMed
- 31. Saito T, Yamashita Y. Electronic determination of root canal length by newly developed measuring device. Influences of the diameter of apical foramen, the size of K-file and the root canal irrigants. Dent Jpn (Tokyo) 1990;27:65-72.PubMed
- 32. Ebrahim AK, Wadachi R, Suda H. An in vitro evaluation of the accuracy of Dentaport ZX apex locator in enlarged root canals. Aust Dent J 2007;52:193-197.ArticlePubMed
- 33. Goldberg F, De Silvio AC, Manfré S, Nastri N. In vitro measurement accuracy of an electronic apex locator in teeth with simulated apical root resorption. J Endod 2002;28:461-463.ArticlePubMed
- 34. Dunlap CA, Remeikis NA, BeGole EA, Rauschenberger CR. An in vivo evaluation of an electronic apex locator that uses the ratio method in vital and necrotic canals. J Endod 1998;24:48-50.ArticlePubMed
- 35. Haffner C, Folwaczny M, Galler K, Hickel R. Accuracy of electronic apex locators in comparison to actual length-an in vivo study. J Dent 2005;33:619-625.ArticlePubMed
- 36. Pilot TF, Pitts DL. Determination of impedance changes at varying frequencies in relation to root canal file position and irrigant. J Endod 1997;23:719-724.ArticlePubMed
REFERENCES
Figure 1
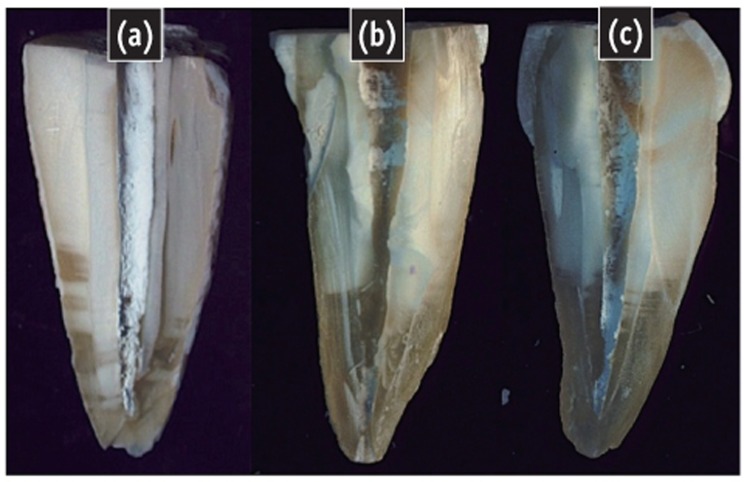
Representative stereomicroscopic images. (a) Control group, Root canal is completely filled with calcium hydroxide (CH); (b) CH removed with 17% EDTA + MAF, Root canal is almost empty except apical section; (c) CH removed with 5.25% NaOCl, Less than half of the root canal is filled with CH.
Table 1
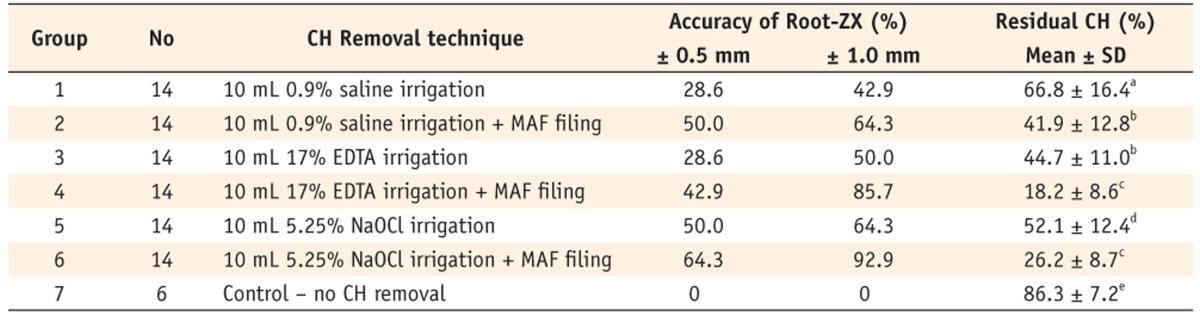
Accuracy (%) of electronic apex locator after removal of calcium hydroxide (CH) (tolerance limit, ± 0.5 and ± 1.0 mm) and percentage of residual CH remaining in the canal (mean ± standard deviation)
Same lowercase superscript letter means no significant difference at the p = 0.05 level.
CH, calcium hydroxide; MAF, master apical file; EDTA, ethylenediamine tetra acetic acid; NaOCl, sodium hypochlorite.
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Evaluation of the Effect of Calcium Hydroxide Residues Including Different Vehicles on the Accuracy of Electronic Apex Locators
Simay Koç, Damla Erkal, Dide Tekinarslan, Kürs¸at Er
Journal of Advanced Oral Research.2025; 16(1): 54. CrossRef - Evaluation of heated sodium hypochlorite’s effect on the accuracy of contemporary electronic apex locators: an in vitro study
İkbal Sena Çelebi Keskin, Turgut Yağmur Yalçın
BMC Oral Health.2025;[Epub] CrossRef - Factors influencing the accuracy of electronic apex locators: A scoping review
Shayan Golkar, Abbasali Khademi, Amin Saatchi, Amir Ghorani, Pedram Iranmanesh
Dental Research Journal.2025;[Epub] CrossRef - Effectiveness of a new irrigation solution -RISA- on removing calcium hydroxide from artificial standardized grooves in root canals - an in vitro study
İpek Eraslan Akyüz, Salih Düzgün, Hüseyin Sinan Topçuoğlu
BMC Oral Health.2025;[Epub] CrossRef - Comparative evaluation of the accuracy of electronic apex locators and cone-beam computed tomography in detection of root canal perforation and working length during endodontic retreatment
Simay Koç, Hatice Harorlı, Alper Kuştarcı
BMC Oral Health.2024;[Epub] CrossRef - Effects of Intracanal Medicaments on the Measurement Accuracy of Four Apex Locators: An In Vitro Study
Hamza Cudal, Tuğrul Aslan, Bertan Kesim
Meandros Medical and Dental Journal.2023; 24(3): 215. CrossRef - Electronic Apex Locators and their Implications in Contemporary Clinical Practice: A Review
Zainab Shirazi, Anas Al-Jadaa, Abdul Rahman Saleh
The Open Dentistry Journal.2023;[Epub] CrossRef - Influence of Apical Patency, Coronal Preflaring and Calcium Hydroxide on the Accuracy of Root ZX Apex Locator for Working Length Determination: An In Vitro Study
Mostafa Godiny, Reza Hatam, Roya Safari-Faramani, Atefeh Khavid, Mohammad Reza Rezaei
Journal of Advanced Oral Research.2022; 13(1): 38. CrossRef - Endodontic cement penetration after removal of calcium hydroxide dressing using XP-endo finisher
Alyssa Sales dos Santos, Maria Aparecida Barbosa de Sá, Marco Antônio Húngaro Duarte, Martinho Campolina Rebello Horta, Frank Ferreira Silveira, Eduardo Nunes
Brazilian Oral Research.2022;[Epub] CrossRef - Efficacy of glycolic acid for the removal of calcium hydroxide from simulated internal Resorption cavities
Cangül Keskin, Ali Keleş, Öznur Sarıyılmaz
Clinical Oral Investigations.2021; 25(7): 4407. CrossRef - Accuracy of electronic apex locator in the presence of different irrigating solutions
Padmanabh Jha, Vineeta Nikhil, Shalya Raj, Rohit Ravinder, Preeti Mishra
Endodontology.2021; 33(4): 232. CrossRef - Farklı Kanal İçi Ortamların Apeks Bulucuların Doğruluğu Üzerine Etkisi
Asena OKUR, Tuğrul ASLAN, Burak SAĞSEN
Selcuk Dental Journal.2021; 8(3): 859. CrossRef - Evaluation of the accuracy of different apex locators in determiningthe working length during root canal retreatment
Pelin Tufenkci, Aylin Kalaycı
Journal of Dental Research, Dental Clinics, Dental Prospects.2020; 14(2): 125. CrossRef - Influence of calcium hydroxide residues after using different irrigants on the accuracy of two electronic apex locators: An in vitro study
NooshinSadat Shojaee, Zahra Zaeri, MohammadMehdi Shokouhi, Fereshteh Sobhnamayan, Alireza Adl
Dental Research Journal.2020; 17(1): 48. CrossRef - The Effect of Calcium Hydroxide and File Sızes on the Accuracy of the Electronic Apex Locator in Simulated Immature Teeth
Leyla AYRANCİ, Ahmet ÇETİNKAYA, Serkan ÖZKAN
Middle Black Sea Journal of Health Science.2019; 5(3): 273. CrossRef - The Effect of File Size and Type and Irrigation Solutions on the Accuracy of Electronic Apex Locators: AnIn VitroStudy on Canine Teeth
Maciej Janeczek, Piotr Kosior, Dagmara Piesiak-Pańczyszyn, Krzysztof Dudek, Aleksander Chrószcz, Agnieszka Czajczyńska-Waszkiewicz, Małgorzata Kowalczyk-Zając, Aleksandra Gabren-Syller, Karol Kirstein, Aleksandra Skalec, Ewelina Bryła, Maciej Dobrzyński
BioMed Research International.2016; 2016: 1. CrossRef
 ePub Link
ePub Link Cite
CiteCalcium hydroxide dressing residues after different removal techniques affect the accuracy of Root-ZX apex locator
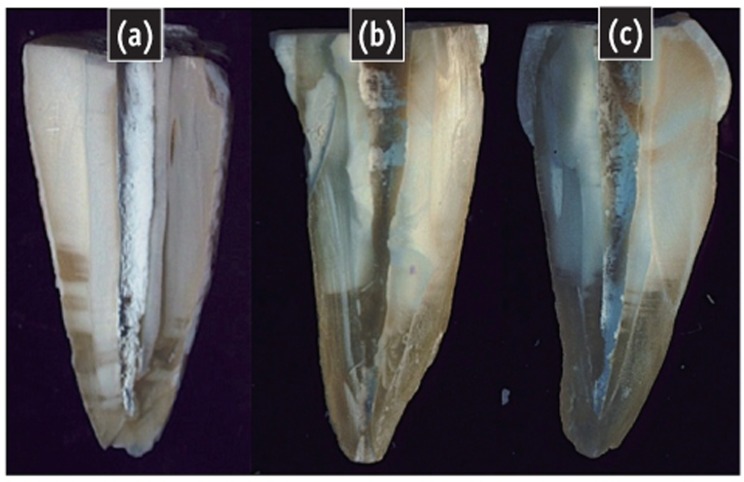
Figure 1 Representative stereomicroscopic images. (a) Control group, Root canal is completely filled with calcium hydroxide (CH); (b) CH removed with 17% EDTA + MAF, Root canal is almost empty except apical section; (c) CH removed with 5.25% NaOCl, Less than half of the root canal is filled with CH.
Figure 1
Calcium hydroxide dressing residues after different removal techniques affect the accuracy of Root-ZX apex locator
Accuracy (%) of electronic apex locator after removal of calcium hydroxide (CH) (tolerance limit, ± 0.5 and ± 1.0 mm) and percentage of residual CH remaining in the canal (mean ± standard deviation)

Same lowercase superscript letter means no significant difference at the p = 0.05 level.
CH, calcium hydroxide; MAF, master apical file; EDTA, ethylenediamine tetra acetic acid; NaOCl, sodium hypochlorite.
Table 1 Accuracy (%) of electronic apex locator after removal of calcium hydroxide (CH) (tolerance limit, ± 0.5 and ± 1.0 mm) and percentage of residual CH remaining in the canal (mean ± standard deviation)
Same lowercase superscript letter means no significant difference at the CH, calcium hydroxide; MAF, master apical file; EDTA, ethylenediamine tetra acetic acid; NaOCl, sodium hypochlorite.

