
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 40(4); 2015 > Article
- Research Article Comparison of mechanical properties of a new fiber reinforced composite and bulk filling composites
- Hazem Abouelleil1, Nelly Pradelle1,2, Cyril Villat1,3, Nina Attik1, Pierre Colon1,2, Brigitte Grosgogeat1,3
-
2015;40(4):-270.
DOI: https://doi.org/10.5395/rde.2015.40.4.262
Published online: September 2, 2015
1Laboratoire des Multimatériaux et Interfaces, UMR CNRS 5615, Université Lyon1, Villeurbanne, France.
2UFR D'odontologie, Université Paris Diderot, APHP, Hôpital Rothschild, Service d'Odontologie, Paris, France.
3UFR Odontologie, Université Lyon1, Service de Consultations et de Traitements Dentaires, Hospices Civils de Lyon, Lyon, France.
- Correspondence to Hazem Abouelleil, DDS, MD. Dental practitioner and Lecturer, Laboratoire des Multimatériaux et Interfaces, UMR CNRS 5615, Université Lyon1, Villeurbanne, France. TEL, +33(0)478778689; FAX, +33(0)478778712; hazem.abouelleilsayed@univ-lyon1.fr
• Received: April 2, 2015 • Accepted: June 30, 2015
©Copyrights 2015. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,378 Views
- 48 Download
- 69 Crossref
Abstract
-
Objectives The aim of this study was to evaluate the mechanical and physical properties of a newly developed fiber reinforced dental composite.
-
Materials and Methods Fiber reinforced composite EverX Posterior (EXP, GC EUROPE), and other commercially available bulk fill composites, including Filtek Bulk Fill (FB, 3M ESPE), SonicFill (SF, Kerr Corp.), SureFil (SDR, Dentsply), Venus Bulk Fill (VB, HerausKultzer), Tetric evoceram bulk fill (TECB, Ivoclar Vivadent), and Xtra Base (XB, Voco) were characterized. Composite samples light-cured with a LED device were evaluated in terms of flexural strength, flexural modulus (ISO 4049, n = 6), fracture toughness (n = 6), and Vickers hardness (0, 2, and 4 mm in depth at 24 hr, n = 5). The EXP samples and the fracture surface were observed under a scanning electron microscopy. Data were statistically analyzed using one-way ANOVA and unpaired t-test.
-
Results EXP, FB, and VB had significantly higher fracture toughness value compared to all the other bulk composite types. SF, EXP, and XB were not statistically different, and had significantly higher flexural strength values compared to other tested composite materials. EXP had the highest flexural modulus, VB had the lowest values. Vickers hardness values revealed SF, EXP, TECB, and XB were not statistically different, and had significantly higher values compared to other tested composite materials. SEM observations show well dispersed fibers working as a reinforcing phase.
-
Conclusions The addition of fibers to methacrylate-based matrix results in composites with either comparable or superior mechanical properties compared to the other bulk fill materials tested.
Introduction
Dental composite resin recently became the material of choice for most patients and dental practitioners.1 However, volumetric shrinkage and fracture are still considered as major concerns with dental composites.2,3 In order to overcome these weaknesses, attempts have been made toward increasing both their physical and mechanical properties.4 This necessitates the comprehensive appraisal of each of its components such as the resin matrix, the filler or the filler-resin interface, and their role in affecting the material properties. Different studies have investigated this in order to improve composite properties, either by varying the particle size, percentage, or by development of the polymer matrix chemistry.4,5
Evolution in both filler and polymer technology in dental composite resins led to a wide selection of materials that provide the adequate properties required for each clinical situation.4 Yet, the use of dental composites in high stress bearing areas remains to be a challenge for the dental practitioner, since bulk fracture is still considered one of the primary reasons for failure.2,6 Bulk fill composites were introduced in an effort to improve the performance of composite resin restorations, which was inserted in 4 mm increments mainly in the posterior areas and considered to have higher physical and mechanical properties to endure the higher masticatory stresses. Moreover, the reduced treatment time decrease the risk of air entrapment or moisture contamination.7 They are also claimed to reduce cuspal deflection and promote light transmittance.7,8 Currently, various studies reveal the difficulty in comparing between the available materials due to variation in composition and viscosity.9,10,11
Bulk filling composites usually have higher filler volume percentage, and sometimes a modified initiator system to ensure better curing in depth, as compared to conventional composites. While no long term clinical studies are available regarding their intraoral performance, Ilie et al. found bulk filling composites to have lower mechanical properties, except for flexural strength as compared to nanohybrid and microhybrid resin based composites.9 However, other studies found them equally successful compared to conventional composites.7,12 Many bulk fill composite resins have been investigated regarding different parameters like degree of conversion, polymerization stress or microleakage. Such studies have shown that bulk fill composites resins have similar properties as conventional dental composite resins.12,13,14,15,16
Finan et al. studied the degree of conversion, biaxial flexural strength and Vickers hardness of two flowable bulk composites (SDR and XB), and despite the differences between the two materials, found that the properties justify their use in 4 mm increments.17 The variation in material composition and viscosity, whether flowable or non flowable bulk composites, leads to differences in physical and mechanical properties among the bulk fill composites available in the market.7 Fiber reinforcement of conventional dental composites were also introduced with the aim of enhancing their physical and mechanical properties, and increasing their resistance to fracture. The enhancement of the material properties was due to the stress transfer from the matrix to the fibers depending on the fibers length and diameter. Garoushi et al. studied their effect, and found a significant improvement in the materials physical properties.18
It was deemed important to investigate the role of fibers added to composite compared to other commonly used bulk fill composites, and to examine the extent to which fiber reinforcement would enhance the mechanical properties of the materials. Multiple laboratory investigations have been used to evaluate dental composite resins; standardized tests present the advantage of being easily reproducible in laboratories, and allowing values obtained by different institutes to be compared. Moreover, they provide preliminary information about the material suitability in the oral environment and the extent to which they conform to the indications prescribed by the manufacturer.19 Heintze et al. found that flexural strength and flexural modulus tests can be used as a good indicator for the material durability under stress, and correlate well with the clinical longevity.19 Fracture toughness test was considered by Ilie et al. as another important method that investigates the material's ability to endure stress without fracture and monitor the crack propagation inside the material before failure.11 On the other hand, Vickers hardness assay, one of the most used mechanical experiments examines the material surface hardness, and scanning electron microscope observations reveal important information about the samples used and the mode of failure of the material.9 Standard ISO flexural strength and modulus tests consider only 2 mm thickness samples. However bulk fill composites are indicated to be used clinically in 4 mm thick increments, and accordingly investigating the material at this thickness seems more appropriate.
The aim of this study was to investigate the mechanical properties of a fiber reinforced composite compared to other commonly used bulk fill composites, and to consider its performance under laboratory settings. The null hypothesis was that there is no significant difference in mechanical properties (flexural strength, flexural modulus, fracture toughness, and Vickers hardness) among the fiber reinforced composite and other bulk fill composites.
Materials and Methods
Bulk fill dental composites used in the study were X-tra base (XB, Voco GmbH, Cuxhaven, Germany), Venus bulk fill (VB, HerausKultzer, Hanau, Germany), Filtek bulk fill (FB, 3M ESPE, St. Paul, MN, USA), Surefil SDR (SDR, Dentsply, Milford, DE, USA), Tetric evoceram bulk fill (TECB, Ivoclar Vivadent AG, Schaan, Liechtenstein), SonicFill (SF, Kerr Corp., Orange, CA, USA), and a fiber reinforced bulk fill dental composite resin, EverX Posterior (EXP, GC EUROPE NV, Leuven, Belgium). The compositions of bulk fill materials used, their shade as well as their lot numbers are listed in Table 1.
For the fracture toughness test, flexural strength and modulus tests, the number of samples for each of the materials used was 6. The tested samples were polymerized using GC G-light unit (GC EUROPE NV) from both sides for 40 seconds. A modified flexural strength test was performed using bulk fill samples with 4 mm2 cross sectional areas polymerized only from the top side as done in the clinical situation. The wavelength of the light was between 380 and 520 nm with maximal intensity at 470 nm and light intensity was 1,150 mW/cm2. The specimens from each group were stored in water at 37℃ for 48 hours before testing.
To measure the fracture toughness (KIC), rectangular glass molds that were lined with polyester strips (Striproll, Kerrhawe SA, Bioggio, Switzerland) were used to prepare single-edge-notched specimens. The cured samples (3 mm × 6 mm × 25 mm) were removed without using force. A sharp central notch of specific length (a) was produced by inserting a razor blade into an accurately fabricated slot at mid-height in the mold. The slot extended down half the height to give a/W = 0.5. The crack plane was perpendicular to the specimen length. The length of the crack was checked using a stereomicroscope.
Where P is the peak load at fracture, L is the length, B is the width, W is the height, a is the average notch depth, and Y is the calibration functions for given geometry
According to the ISO 4049, samples for a three point bending test were prepared in Teflon molds between two glass slabs, resulting in bar shaped specimens (2 mm × 2 mm × 25 mm). The test was conducted under a cross-head speed of 0.5 mm/min, with a span length of 20 mm and an indenter diameter of 2 mm. All specimens were loaded in a Universal Mechanical testing machine (Servo hydraulic - Adamel Lhomargy DY-34, MTS, Roissy-en-Brie, France). Flexural strength and modulus tests, were repeated on larger samples (n = 6, 4 mm × 4 mm × 25 mm), that were cured only from the top, using the same light and stored in water at 37℃ for 48 hours before testing.
Flexural strength (Of) and flexural modulus (Ef) were calculated from the following formulas:
Where Fm is the applied load (N) at the highest point of load-deflection curve, I is the span length (20 mm), b is the width of test specimens and h is the thickness of test specimens. S is the stiffness (S = F/d, N/m) and d is the deflection corresponding to load F at a point in the straight-line portion of the trace.
The Vickers hardness test was performed with Leitz microhardness device (Leitz, Wetzlar, Germany), under a force of 200 g for 30 seconds. Ten samples for each material were prepared using a 5 mm diameter Teflon mold, with either 2 mm (n = 5) or 4 mm thickness (n = 5), placed between 2 glass plates. The materials were polymerized only on one side for 40 seconds. The excesses were removed by polishing the 2 surfaces using abrasive paper discs of decreasing coarseness from 2,400 to 4,000 grits (Struers SAS, Champigny sur Marne, France) at 3,000 rpm under water irrigation. The top surface (polymerized) and the bottom surface (non-polymerized) were marked to be identified. Each sample was tested 5 times on each side, at 24 hours after immersion in distilled water at 37℃. The Vickers hardness was calculated using the formula:
Where P (g) is the load applied, and d is the average of the 2 diagonals of the surface of the diamond indentation.
Scanning Electron microscope (S800-1, Hitachi Europe Ltd., Whitebrook, Berkshire, UK) observations were conducted under ×80, ×100, and ×250 magnification to examine the fracture mode, and to measure the fiber's diameter and length. Samples were dried, sputter-coated with metal, and observed. The type of fracture was determined for each specimen.
The statistical analysis of the current data was performed using the application of one-way analysis of variance (ANOVA). The results were compared between each test and between each material type using unpaired t-test. The results are reported as mean ± SD. Statistical significance was accepted at p < 0.05.
Results
Fracture toughness and Vickers hardness of tested composite materials are presented in Figures 1 and 2. Flexural strength and flexural modulus are presented in Table 2. The fiber reinforced composite EXP had significantly higher fracture toughness value (3.1 MPa·m1/2), compared to other bulk composites except for FB (2.52 MPa·m1/2) and VB (2.26 MPa·m1/2) where no significant difference was found with EXP. In the normalized flexural strength test (2 mm × 2 mm × 25 mm), SF (157.6 MPa), EXP (153.6 MPa), XB (150.4 MPa) and FB (140.0 MPa) were not statistically different, and these have significantly higher flexural strength values compared to other tested composite materials, except for FB which was similar to SDR. EXP had significantly higher flexural modulus (14.6 GPa), while SF (12.47 GPa), TECB (10.87 GPa), and XB (10.65 GPa) were not significantly different and came in second position. On the other hand, VB (5.02 GPa) had the lowest statistically significant value.
Considering the modified test (4 mm × 4 mm × 25 mm), there was no significant difference from those obtained in the original test, except for XB and they had the same order of the strength values from SF (147.67 MPa), EXP (140.04 MPa), and FB (139.62 MPa). On the other hand, the flexural modulus values decreased significantly in comparison with the normalized test, attaining almost half the original value, while remaining in the same order, with the highest flexural modulus for EXP (6.89 GPa), together with SF (6.55 GPa), followed by XB (5.7 GPa) and FB (4.01 GPa), which were less affected in comparison with original test.
Vickers hardness values revealed that SF had the highest value followed by EXP. The decrease in hardness between the surface and 2 mm and 4 mm depths were not significant for EXP, TECB, and VB, while other bulk composites revealed a significant difference between the curing depths.
SEM analysis revealed that the fibers stop the crack propagation along the fracture line, as shown in Figure 3.
Discussion
According to the results obtained in the current study, the null hypothesis was rejected, that is, fiber insertion into composite leads to significant increase in physical and mechanical properties, such as flexural strength, flexural modulus, fracture toughness, and Vickers hardness.
In this study, flexural strength and modulus were investigated. These tests are considered to be good indicators of the material resistance to fracture in normal masticatory conditions, taking in account the great variability in the results obtained between studies.19,20 The results obtained are in accordance with previous studies conducted on bulk composites. SF, EXP, XB, and FB had significantly higher flexural strength values, compared to VB and TECB which had the lowest.9,18,21 Moreover, as shown in previous works, the filler volume percentage is closely related to the flexural strength and flexural modulus values.9,18,21 This can be shown for SF with the highest filler volume percentage (83%) ranking the highest, TECB (61%) and XB (58%) follow next, while VB with the lesser filler volume percentage (38%) ranking the lowest. Interestingly, EXP (53.6%) performed relatively better in these two tests compared to its filler volume percentage, showing the role of the fibers in increasing the material stiffness and resistance to bending force during testing and probably during function.
In this work, the modified flexural strength and modulus tests were done on 4 mm increments cured only from the top side in an effort to mimic the clinical situation. This would eventually mean less matrix polymerization and, accordingly, a larger role of the filler type and percentage in the material behavior. The results obtained show that the flexural strength values remained significantly unchanged. In comparison to the original test, significant decrease in the flexural modulus values of the composites tested indicated a marked decrease in rigidity. This is probably due to an increase in thickness of the increments and decrease in the overall matrix polymerization. A probable explanation would be that, as a result of less matrix polymerization and the consequent lack of rigidity, the modified test samples were able to withstand flexure even at greater load relative to greater sample thickness (hence unchanged flexural strength) but with more deformation before final failure (hence lower modulus of flexure). These results, when confirmed with further studies, would throw more insight on an important aspect regarding the amount of deformation and the distortion of the material due to the decreased stiffness, most notably at the interface region. This would also provide some explanation for the discrepancies found between results obtained in the laboratories and those from clinical studies in which bulk materials are inserted in larger and thicker increments and cured only from one side.19
Results obtained acknowledge the role of fibers in increasing the material's resistance to fracture, and coincide with those of previous studies.18,22 The single edge notched beam method used in this study is one of the most commonly used fracture toughness test methods, which are used to predict resistance to fracture. The method is widely used in dental material research and is usually conducted by means of a 3 point bending apparatus, and the sharp crack created could be easily measured. This method is also very sensitive to the notch width and depth, thus making comparison difficult between different studies.11,18 In the present work, no correlation was found between the fracture toughness value and the filler volume percentage or the filler particle size.
The enhancement of the material properties was explained to be due to the stress transfer from the matrix to the fibers and also due to the action of the fibers in stopping crack propagation through the material.23 It was found that the mere insertion of fibers is not enough to enhance the composite properties, that is, the fibers length and diameter play a critical role in this mechanism. Peterson found that fibers incorporated into a material, greatly enhances its mechanical properties, on the condition that the fibers have a length that exceeds a certain minimum length. This is known as the critical fiber length, which could be calculated using the following formula:24
Where the critical length (lc) equals the ultimate tensile strength of the fiber (f) multiplied by the fiber diameter (d), and divided by twice the shear strength of the matrix interface (c)
The physical explanation of the strengthening and stiffening mechanism is that since the matrix has a much lower modulus than the fiber, the matrix strains more. The critical fiber length is therefore the minimum length at which the center of the fiber reaches its ultimate tensile strength when the matrix reaches its maximum shear strength. Accordingly, composite with fibers below critical length fail to show enhanced properties.18 In the present study, we were able to measure the fiber length and diameter using stereomicroscopy and SEM, and we found that EXP had a fiber diameter of 16 µm and a wide range of fiber length, with the average length lying between 1 and 2 mm similar to the values found in previous studies, thus exceeding the fiber length required.18 The fiber length and orientation can be shown in Figure 4.
One interesting observation found from the fracture toughness and the flexural strength test samples alike was that all fiber reinforced composite EXP samples remained attached, even after failure of the sample and formation of crack line, unlike the samples from other bulk fill brands which separated in two pieces the time the failure load was reached, as can be seen in Figure 5. Scanning electron microscope observations performed on fractured samples show the fibers traversing the crack line and between the fractured parts, as can be seen in Figure 3. Further investigation of this property is important clinically, since not only it shows the material resistance to fracture, but also its resistance to displacement at the more vulnerable interface, thus preventing cavitation and food impaction. Moreover, this property would render the material with better potential for repair.
The Vickers microhardness test samples show that SF, EXP, TECB, and XB have the highest values compared to SDR, FB, and VB. It is worth noting that though this method was criticized as an unreliable indicator of the curing quality, and that it overestimates the depth of cure. Flury et al. have shown that Vickers microhardness could be considered as an accurate tool for estimating the polymerization depth for bulk composite resins.25,26 Moreover, only SF and EXP had bottom surface hardness values that exceeded the 50 VHN considered ideal.27 However, EXP is the only composite with Vickers hardness value at 4 mm depth that exceeded the 80% ratio compared to the top surface hardness as required in literature.26,27,28,29 The results thus obtained provide evidence that EXP could be used in 4 mm increments for tooth cavity fillings.
The present results were obtained in optimized laboratory settings, however, clinical conditions are not similar and the aspects like insertion and handling could have a potential effect on the mechanical properties of the materials and their performance in vivo. Another important factor that should be taken into consideration as one of the limitations of the current study is the fiber alignment inside the composite in relation to the acting force, which is not necessarily consistent with the laboratory simulations performed during in vitro testing. Some of the important aspects considering the materials polymerization contraction and contraction stress were not included in the study. Further investigations should be conducted to test other material properties. According to the results obtained in this work, the fiber reinforced composite tested may be used as a restorative material in stress bearing areas. In order to acknowledge the results obtained with the present study, this should be followed by long term clinical studies to assure the materials performance under normal clinical conditions.
Conclusions
In the current study, fiber reinforced composite EXP had either comparable or superior resistance to fracture, flexural strength and modulus, as well as high microhardness values, compared to other bulk fill composite resins.
Acknowledgement
The dental companies GC, Voco, 3M/ESP, Dentsply, Ivoclar Vivadent, Kerr, Heraus Kultzer are gratefully acknowledged for the generous donation of the dental composites. The SEM study was supported by the Microstructures Technology Center of University Claude Bernard Lyon1.
- 1. Pallesen U, van Dijken JW, Halken J, Hallonsten AL, Höigaard R. Longevity of posterior resin composite restorations in permanent teeth in Public Dental Health Service: a prospective 8 years follow up. J Dent 2013;41:297-306.ArticlePubMed
- 2. Demarco FF, Corrêa MB, Cenci MS, Moraes RR, Opdam NJ. Longevity of posterior composite restorations: not only a matter of materials. Dent Mater 2012;28:87-101.ArticlePubMed
- 3. Sarrett DC. Clinical challenges and the relevance of materials testing for posterior composite restorations. Dent Mater 2005;21:9-20.ArticlePubMed
- 4. Cramer NB, Stansbury JW, Bowman CN. Recent advances and developments in composite dental restorative materials. J Dent Res 2011;90:402-416.ArticlePubMedPMCPDF
- 5. Ferracane JL. Resin composite-state of the art. Dent Mater 2011;27:29-38.ArticlePubMed
- 6. Da Rosa Rodolpho PA, Donassollo TA, Cenci MS, Loguércio AD, Moraes RR, Bronkhorst EM, Opdam NJ, Demarco FF. 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater 2011;27:955-963.ArticlePubMed
- 7. Walter R. Critical appraisal: bulk-fill flowable composite resins. J Esthet Restor Dent 2013;25:72-76.ArticlePubMedPDF
- 8. Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent 2012;40:500-505.ArticlePubMed
- 9. Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent 2013;38:618-625.ArticlePubMedPDF
- 10. Leprince JG, Palin WM, Vanacker J, Sabbagh J, Devaux J, Leloup G. Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent 2014;42:993-1000.ArticlePubMed
- 11. Ilie N, Hickel R, Valceanu AS, Huth KC. Fracture toughness of dental restorative materials. Clin Oral Investig 2012;16:489-498.ArticlePubMedPDF
- 12. El-Safty S, Silikas N, Watts DC. Creep deformation of restorative resin-composites intended for bulk-fill placement. Dent Mater 2012;28:928-935.ArticlePubMed
- 13. Alshali RZ, Silikas N, Satterthwaite JD. Degree of conversion of bulk-fill compared to conventional resin-composites at two time intervals. Dent Mater 2013;29:e213-e217.ArticlePubMed
- 14. Van Ende A, De Munck J, Van Landuyt KL, Poitevin A, Peumans M, Van Meerbeek B. Bulk-filling of high C-factor posterior cavities: effect on adhesion to cavity-bottom dentin. Dent Mater 2013;29:269-277.ArticlePubMed
- 15. Roggendorf MJ, Krämer N, Appelt A, Naumann M, Frankenberger R. Marginal quality of flowable 4-mm base vs. conventionally layered resin composite. J Dent 2011;39:643-647.ArticlePubMed
- 16. Poggio C, Dagna A, Chiesa M, Colombo M, Scribante A. Surface roughness of flowable resin composites eroded by acidic and alcoholic drinks. J Conserv Dent 2012;15:137-140.ArticlePubMedPMC
- 17. Finan L, Palin WM, Moskwa N, McGinley EL, Fleming GJ. The influence of irradiation potential on the degree of conversion and mechanical properties of two bulk-fill flowable RBC base materials. Dent Mater 2013;29:906-912.ArticlePubMed
- 18. Garoushi S, Säilynoja E, Vallittu PK, Lassila L. Physical properties and depth of cure of a new short fiber reinforced composite. Dent Mater 2013;29:835-841.ArticlePubMed
- 19. Heintze SD, Zimmerli B. Relevance of in vitro tests of adhesive and composite dental materials, a review in 3 parts. Part 1: approval requirements and standardized testing of composite materials according to ISO specifications. Schweiz Monatsschr Zahnmed 2011;121:804-816.PubMed
- 20. Alander P, Lassila LV, Vallittu PK. The span length and cross-sectional design affect values of strength. Dent Mater 2005;21:347-353.ArticlePubMed
- 21. Czasch P, Ilie N. In vitro comparison of mechanical properties and degree of cure of bulk fill composites. Clin Oral Investig 2013;17:227-235.ArticlePubMedPDF
- 22. Xu HH, Schumacher GE, Eichmiller FC, Peterson RC, Antonucci JM, Mueller HJ. Continuous-fiber preform reinforcement of dental resin composite restorations. Dent Mater 2003;19:523-530.ArticlePubMed
- 23. Garoushi S, Vallittu PK, Lassila LV. Short glass fiber reinforced restorative composite resin with semi-inter penetrating polymer network matrix. Dent Mater 2007;23:1356-1362.ArticlePubMed
- 24. Petersen RC. Discontinuous fiber-reinforced composites above critical length. J Dent Res 2005;84:365-370.ArticlePubMedPMCPDF
- 25. Leprince JG, Leveque P, Nysten B, Gallez B, Devaux J, Leloup G. New insight into the "depth of cure" of dimethacrylate-based dental composites. Dent Mater 2012;28:512-520.ArticlePubMed
- 26. Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A. Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dent Mater 2012;28:521-528.ArticlePubMed
- 27. Galvão MR, Caldas SG, Bagnato VS, de Souza Rastelli AN, de Andrade MF. Evaluation of degree of conversion and hardness of dental composites photo-activated with different light guide tips. Eur J Dent 2013;7:86-93.PubMedPMC
- 28. Polydorou O, Manolakis A, Hellwig E, Hahn P. Evaluation of the curing depth of two translucent composite materials using a halogen and two LED curing units. Clin Oral Investig 2008;12:45-51.ArticlePubMedPDF
- 29. Yap AU, Seneviratne C. Influence of light energy density on effectiveness of composite cure. Oper Dent 2001;26:460-466.PubMed
REFERENCES
Figure 1
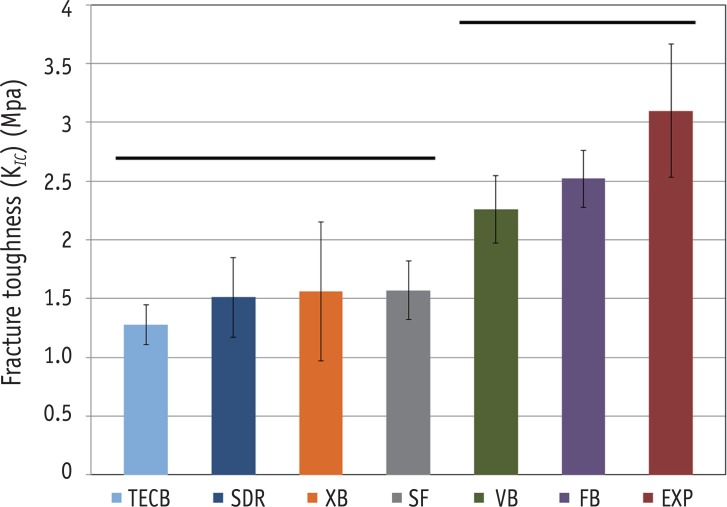
Bar graph illustrating fracture toughness (KIC). Straight line indicates that there was no statistically significant difference between the groups.
TECB, Tetric evoceram bulk fill; SDR, SureFil SDR; XB, Xtra Base; SF, SonicFill; VB, Venus bulk fill; FB, Filtek bulk fill; EXP, EverX Posterior.
Figure 2
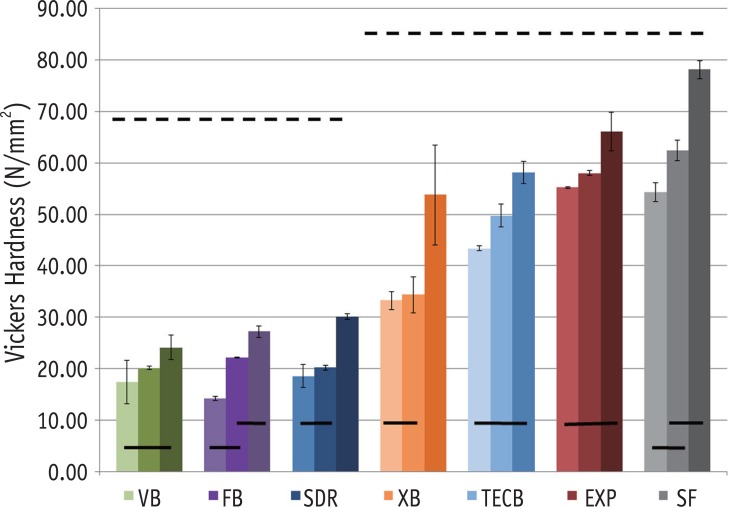
Bar graph illustrating Vickers hardness (N/mm2) at different curing depths of 4 mm, 2 mm and at the surface. Dotted line (-----) indicates that there was no statistically significant difference between the materials. Straight line (——) indicates that there was no statistically significant difference within the same material at different curing depths.
TECB, Tetric evoceram bulk fill; SDR, SureFil SDR; XB, Xtra Base; SF, SonicFill; VB, Venus bulk fill; FB, Filtek bulk fill; EXP, EverX Posterior.
Figure 3
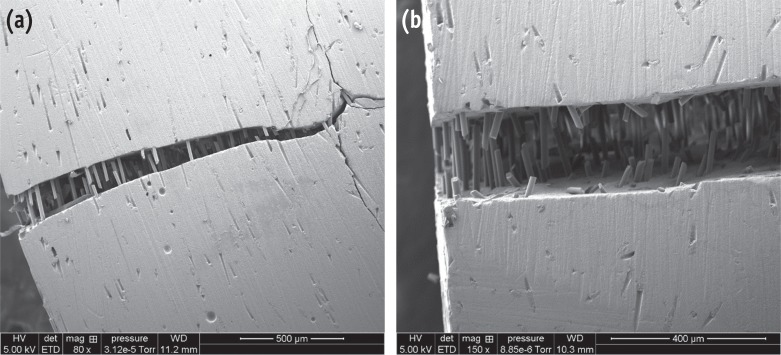
Scanning electron photomicrograph of fracture toughness sample (a) after failure; (b) the fiber orientation across the failure line are shown at higher magnification.
Figure 4
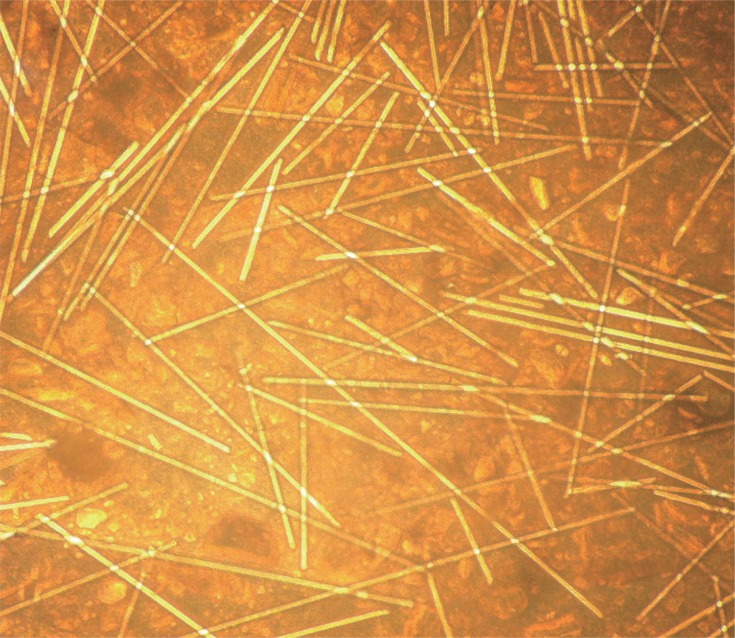
Microscopic image of EverX Posterior showing fiber length extending to the length of one millimeter and up to two milimeters.
Figure 5
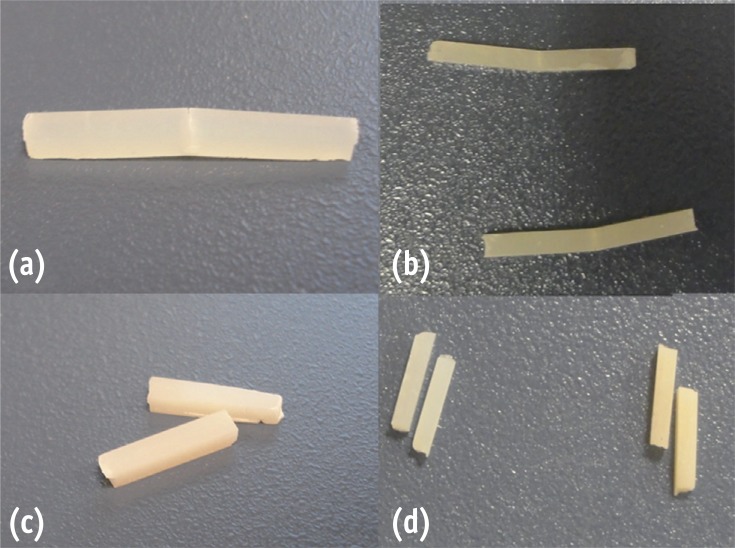
Samples of (a) fracture toughness and (b) flexural strength tests for EverX Posterior remained connected after failure, compared to other bulk composite samples after (c) fracture toughness and (d) flexural strength, which were completely separated into two fragments.
Table 1
Materials, manufacturers, chemical composition of the matrix, fillers and filler contents
Table 2
Flexural strength (σ, MPa) and Flexural Modulus (Eflexural, GPa) for the 2 mm and 4 mm sample groups
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Shear bond strength of the adhesive interface between NeoPUTTY and bulk-fill composites: An in vitro pilot study
Farah Salim Shnan, Hemn Muhssin Suleman
Saudi Endodontic Journal.2026; 16(2): 194. CrossRef - Surface Physical and Mechanical Properties of Short Fibre Reinforced Composite Resins in Direct Restorative Dentistry: A Systematic Review
Murray Macpherson, Michael Liddell, Touraj Nejatian
Australian Dental Journal.2026;[Epub] CrossRef - Influence of Water Storage on the Mechanical Properties of Short Fiber-Reinforced Dental Resin Composites
Yoshiki Ishida, Daisuke Miura, Yasuhiro Hotta, Akikazu Shinya
Fibers.2026; 14(6): 71. CrossRef - Tailoring the interfacial properties of glass fiber-epoxy microcomposites through the development of a self-healing poly(ϵ-caprolactone) coating
Laura Simonini, Markus Kakkonen, Royson Dsouza, Mikko Kanerva, Haroon Mahmood, Andrea Dorigato, Alessandro Pegoretti
Composites Science and Technology.2025; 261: 110991. CrossRef - Assessing the bond strength of short fiber composites to dentin using various air abrasion particles
Ece Ucar Başol, Isil Cekic-Nagas, Sufyan Garoushi, Emre Nagas, Pekka Kalevi Vallittu, Lippo Veli Juhana Lassila
Journal of Prosthodontic Research.2025; 69(3): 429. CrossRef - Effect of using different materials and restorative techniques on cuspal deflection and microleakage in endodontically treated teeth
Ceyda Sari, Oya Bala, Sinem Akgul, Cemile Kedici Alp
BMC Oral Health.2025;[Epub] CrossRef - Error analysis in bending tests of short specimens and the new accurate formulas for elastic and shear moduli
A. V. Khokhlov
Industrial laboratory. Diagnostics of materials.2025; 91(2): 54. CrossRef - Assessing Toxicological Safety of EverX Posterior and Filtek Ultimate: An In-Depth Extractable and Leachable Study Under ISO 10993-17 and 10993-18 Standards
Aysu Aydınoǧlu, Yelda Erdem Hepşenoǧlu, Can Özgür Yalçın, Kadir Saǧır, Yeşim Ölçer Us, Şeyda Erşahan Eroǧlu, Afife Binnaz Hazar Yoruç
ACS Omega.2025; 10(10): 9903. CrossRef - Poly(butylene adipate-co-terephthalate) as a new healing agent for epoxy/basalt composites
Laura Simonini, Daniele Rigotti, Jeevan Kishore Reddy Pidapa, Alessandro Pegoretti
Composites Part A: Applied Science and Manufacturing.2025; 196: 109010. CrossRef - EFFECT OF DELAMINATION OF LOW SHEAR STRENGTH MATERIALS ON FRACTURE AND TEST RESULTS UNDER THREE-POINT BENDING
A. V. KHOKHLOV, S. N. GALYSHEV, B. I. ATANOV, V. I. ORLOV
Fizicheskaya Mezomekhanika.2025;[Epub] CrossRef - Mechanical and physical evaluation of fiber-reinforced resin composite in comparison with conventional and bulk fill composite
Manal A. El-Ebiary, Enas S. Sadek, Hend Elkafrawy
Tanta Dental Journal.2025; 22(2): 242. CrossRef - Comparison of Commercial and Experimental Fibre-Reinforced Composites in Restoring Endodontically Treated Teeth with Minimal Coronal Dentine: An In Vitro Study
Amre R Atmeh, Faisal Masaud, Luba AlMuhaish, Abdulkarim Alanazi, Hadeel Almutiri, Saqib Ali, Hassan Almoqhawi, Abdul Samad Khan
Journal of Functional Biomaterials.2025; 16(9): 335. CrossRef - Effect of Delamination of Low Shear Strength Materials on Fracture and Test Results under Three-Point Bending
A. V. Khokhlov, S. N. Galyshev, B. I. Atanov, V. I. Orlov
Physical Mesomechanics.2025; 28(4): 439. CrossRef - Evaluation of fracture resistance and crack propensity of bulk-fill composite restorations reinforced by polyethylene fiber
Ayşe Aslı Şenol, Aybike Manav, Bengü Doğu Kaya, Pınar Yılmaz Atalı, Erkut Kahramanoğlu, Bilge Tarçın, Cafer Türkmen
BMC Oral Health.2025;[Epub] CrossRef - A comparison of the effects of incremental and snowplow techniques on the mechanical properties of composite restorations
Y Ölçer Us, A Aydınoğlu, Ş Erşahan, Y Erdem Hepşenoğlu, K Sağır, A Üşümez
Australian Dental Journal.2024; 69(1): 40. CrossRef - Biomimetic approach to strengthen the incisal fracture composite build-up: an in vitro study
Ganesh R. Jadhav, Priya Mittal, Siddharth Shinde, Mohammed A. Al-Qarni, Mohammed Al-Obaid, Shahabe Saquib Abullais, Marco Cicciù, Giuseppe Minervini
BMC Oral Health.2024;[Epub] CrossRef - Mechanical properties and degree of conversion of resin-based core build-up materials and short fiber-reinforced flowable resin-based composite
Abdulrahman ALSHABIB, Carlos A. JURADO, Francisco X. AZPIAZU-FLORES, Khalid ALDOSARY, Akimasa TSUJIMOTO, Hamad ALGAMAIAH
Dental Materials Journal.2024; 43(3): 453. CrossRef - Comparative estimation of fracture resistance of teeth restored with new fiber impregnated composite, short fiber composite, and nanohybrid composite – An in-vitro study
P. Doshi, P. Oswal, S. R. Srinidhi, M. Bhujbal, K. Malu
Endodontics Today.2024; 22(3): 220. CrossRef - Development of Mineral Fillers for Acid-Resistant Filling Composites
Laila M. Kalimoldina, Sandugash O. Abilkasova, Saule O. Akhmetova, Mariya Sh. Suleimenova, Zhanat E. Shaikhova
Journal of Composites Science.2024; 8(7): 284. CrossRef - Fracture resistance of postendodontic restoration using self-adhesive bioactive resin and a bulk-fill composite with or without resin-impregnated glass fibers: An in vitro study
Aishika Paul, Rohit Dubey, Sonal B. Joshi, Anand C. Patil, Pranjali S. Narvekar
Journal of Conservative Dentistry and Endodontics.2024; 27(9): 908. CrossRef - Fracture Toughness of Short Fibre-Reinforced Composites—In Vitro Study
Noor Kamourieh, Maurice Faigenblum, Robert Blizard, Albert Leung, Peter Fine
Materials.2024; 17(21): 5368. CrossRef - Comparative Evaluation of Different Designs of Mesio-occlusal-distal Cavities and Different Composite Systems on Fracture Resistance: An In Vitro Study
Anshul Arora, Vedika Talwar, Sonali Taneja
World Journal of Dentistry.2024; 15(6): 472. CrossRef - Fracture Resistance of Endodontically Treated Tooth Restored with Fiber Reinforced Composite Core and Crown at Different Heights of Ferrule
Saleem D Makandar, Dara Khorsyiah Yakob, Rabihah Alawi, Nor Aidaniza Abdul Muttlib, Normastura Abd Rahman
World Journal of Dentistry.2023; 14(3): 238. CrossRef - Fracture Resistance of Endodontically Treated Teeth Restored With Short Fiber Reinforced Composite and a Low Viscosity Bulk Fill Composite in Class II Mesial-Occlusal-Distal Access Cavities: An Ex-vivo Study
Harish Selvaraj, Jogikalmat Krithikadatta
Cureus.2023;[Epub] CrossRef - Physical Properties and Clinical Performance of Short Fiber Reinforced Resin-based Composite in Posterior Dentition: Systematic Review and Meta-analysis
A Aram, H Hong, C Song, M Bass, JA Platt, S Chutinan
Operative Dentistry.2023; 48(5): E119. CrossRef - Effect of short fiber-reinforced composite combined with polyethylene fibers on fracture resistance of endodontically treated premolars
Sabrina L. Soto-Cadena, Norma V. Zavala-Alonso, Bernardino I. Cerda-Cristerna, Marine Ortiz-Magdaleno
The Journal of Prosthetic Dentistry.2023; 129(4): 598.e1. CrossRef - Systematic review fracture resistance of endodontically treated posterior teeth restored with fiber reinforced composites- a systematic review
Harish Selvaraj, Jogikalmat Krithikadatta, Deepti Shrivastava, Meshal Aber Al Onazi, Hmoud Ali Algarni, Swapna Munaga, May Osman Hamza, Turki saad Al-fridy, Kavalipurapu Venkata Teja, Krishnamachari Janani, Mohammad Khursheed Alam, Kumar Chandan Srivastav
BMC Oral Health.2023;[Epub] CrossRef - Effect of Fibres on Physico-Mechanical Properties of Bulk-Fill Resin Composites
Abdulrahman Alshabib, Nick Silikas, Hamad Algamaiah, Abdullah S. Alayad, Rahaf Alawaji, Shaikha Almogbel, Ahad Aldosari, Abdulaziz Alhotan
Polymers.2023; 15(16): 3452. CrossRef - Shrinkage‐induced cuspal deformation and strength of three different short fiber‐reinforced composite resins
Pascal Magne, Marco Aurelio Carvalho, Taban Milani
Journal of Esthetic and Restorative Dentistry.2023; 35(1): 56. CrossRef - Effects of ceramic thickness, ceramic translucency, and light transmission on light-cured bulk-fill resin composites as luting cement of lithium disilicate based-ceramics
Ting-An Chen, Pei-Ying Lu, Po-Yen Lin, Chih-Wen Chi, Hon Yin Cheng, Yu-Jung Lai, Fajen Wang, Yu-Chih Chiang
Journal of Prosthodontic Research.2023; 68(2): 255. CrossRef - A COMPARATIVE EVALUATION OF COMPRESSIVE STRENGTH AND FLEXURAL STRENGTH OF BULK- FILL RESIN- BASED COMPOSITES: AN INVITRO STUDY
Anindita Saikia, Chandana Kalita, Anija R, Tribisha Kalita, A. C .Bhuyan
INDIAN JOURNAL OF APPLIED RESEARCH.2022; : 62. CrossRef - Comparison of physical and biological properties of a flowable fiber reinforced and bulk filling composites
Nina Attik, Pierre Colon, Rémy Gauthier, Charlène Chevalier, Brigitte Grosgogeat, Hazem Abouelleil
Dental Materials.2022; 38(2): e19. CrossRef - Fracture resistance and flexural strength of endodontically treated teeth restored by different short fiber resin composites: a preclinical study
Wael Gamal, Ahmed Abdou, Ghada A. Salem
Bulletin of the National Research Centre.2022;[Epub] CrossRef - In Vitro Evaluation of the Strength of Dentin Replacement in Complex Posterior Tooth Restoration
Nurhayaty Natsir, Farida Rahim, Juni Jekti Nugroho, Christine Anastasia Rovani, Syamsiah Syam, Muhammad Ruslin, Takashi Saito, Keng-Liang Ou
Applied Sciences.2022; 12(14): 6877. CrossRef - Polymerization Shrinkage of Short Fiber Reinforced Dental Composite Using a Confocal Laser Analysis
Daisuke Miura, Yoshiki Ishida, Akikazu Shinya
Polymers.2021; 13(18): 3088. CrossRef - Comparative Evaluation of Mechanical Properties of Titanium Dioxide Nanoparticle Incorporated in Composite Resin as a Core Restorative Material
Dhanasekaran Sihivahanan, Venugopal V Nandini
The Journal of Contemporary Dental Practice.2021; 22(6): 686. CrossRef - Microtensile Bond Strength, Marginal Leakage, and Antibacterial Effect of Bulk Fill Resin Composite with Alkaline Fillers versus Incremental Nanohybrid Composite Resin
Nada Ismail Mohamed, Rehab Khalil Safy, Ahmed Fawzy Abo Elezz
European Journal of Dentistry.2021; 15(03): 425. CrossRef - The Use of Bulk-Fill Flow in the Customization of Glass Fiber Post
Camila Ferreira Silva, Victor Mota Martins, Anahi de Paula Melo, Laís Carvalho Martins, Paulo Cesar Freitas Santos-Filho
European Journal of Dentistry.2021; 15(01): 139. CrossRef - Comparative Evaluation of Flexural Strength of Two Newer Composite Resin Materials: An in Vitro Study
Akshata Patil, Shashi Rashmi Acharya, Kishore Ginjupalli
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2021;[Epub] CrossRef - Analysis of marginal integrity in dentistry composite fillings with flow layer under compression test
Monika Ostapiuk, Janusz Tarczydło, Iwona Łuszczewska‐Sierakowska, Radosław Śledź, Barbara Tymczyna‐Borowicz
Microscopy Research and Technique.2021; 84(7): 1442. CrossRef - Effect of the incorporation of silica blow spun nanofibers containing silver nanoparticles (SiO2/Ag) on the mechanical, physicochemical, and biological properties of a low-viscosity bulk-fill composite resin
Soraya Salmanzadeh Ardestani, Roberta Ferreti Bonan, Mariaugusta Ferreira Mota, Rosiane Maria da Costa Farias, Romualdo Rodrigues Menezes, Paulo Rogério Ferreti Bonan, Panmella Pereira Maciel, Flávia Maria de Moraes Ramos-Perez, André Ulisses Dantas Batis
Dental Materials.2021; 37(10): 1615. CrossRef - An in vitro investigation on the reinforcing potential of contemporary composites in weakened bicuspids
ApurvaRamchandra Kale, Shishir Singh, Rajesh Podar, Mohan Kumar, Padmini Chandrasekhar, Gaurav Kulkarni
Journal of Conservative Dentistry.2021; 24(6): 589. CrossRef - Fracture strength of endodontically treated teeth restored with different fiber post and core systems
Taha Özyürek, Can Topkara, İmran Koçak, Koray Yılmaz, Mustafa Gündoğar, Gülşah Uslu
Odontology.2020; 108(4): 588. CrossRef - Comparative evaluation of the surface hardness of different esthetic restorative materials: An in vitro study
Anoop Samuel, Rinsa Raju, KB Sreejith, BinithaM Kalathil, Deepthi Nenavath, VS Chaitra
Journal of Pharmacy And Bioallied Sciences.2020; 12(5): 124. CrossRef - Restoration of a Nonvital Tooth with Fiber Reinforce Composite (Wallpapering Technique)
Sara Valizadeh, Ladan Ranjbar Omrani, Simone Deliperi, Farzaneh Sadeghi Mahounak, Ali I. Abdalla
Case Reports in Dentistry.2020;[Epub] CrossRef - Cracked Tooth Syndrome Management Part 2: Integrating the Old with the New
Oliver Bailey
Dental Update.2020; 47(7): 570. CrossRef - Synthesis and characterization of bioactive glass fiber-based dental restorative composite
Mariam Raza Syed, Nida Zehra Bano, Sarah Ghafoor, Hina Khalid, Shahreen Zahid, Usama Siddiqui, Abbas Saeed Hakeem, Anila Asif, Muhammad Kaleem, Abdul Samad Khan
Ceramics International.2020; 46(13): 21623. CrossRef - Performance of fibre reinforced composite as a post-endodontic restoration on different endodontic cavity designs— an in-vitro study
Sriprakash Shah, D.P. Shilpa-Jain, Natanasabapathy Velmurugan, Chandrasekaran Sooriaprakas, Jogikalmat Krithikadatta
Journal of the Mechanical Behavior of Biomedical Materials.2020; 104: 103650. CrossRef - Influence of Bulk-fill Restoration on Polymerization Shrinkage Stress and Marginal Gap Formation in Class V Restorations
AMO Correia, MR Andrade, JPM Tribst, ALS Borges, TMF Caneppele
Operative Dentistry.2020; 45(4): E207. CrossRef - BULK-FİLL KOMPOZİTLERDE KALINLIĞIN ARTIŞININ MİKROSERTLİK ÜZERİNE ETKİSİ
Evrim ELİGÜZELOĞLU DALKILIÇ, Fehime ALKAN, Hacer DENİZ ARISU
Selcuk Dental Journal.2020; 7(2): 141. CrossRef - Hardness and fracture toughness of resin-composite materials with and without fibers
Abdulrahman Alshabib, Nick Silikas, David C. Watts
Dental Materials.2019; 35(8): 1194. CrossRef - Effect of interface surface design on the fracture behavior of bilayered composites
Tarek A. Omran, Sufyan Garoushi, Lippo V. Lassila, Pekka K. Vallittu
European Journal of Oral Sciences.2019; 127(3): 276. CrossRef - Bonding interface affects the load-bearing capacity of bilayered composites
Tarek A. OMRAN, Sufyan GAROUSHI, Lippo LASSILA, Akikazu SHINYA, Pekka K. VALLITTU
Dental Materials Journal.2019; 38(6): 1002. CrossRef - Properties of a New Nanofiber Restorative Composite
EM Yancey, W Lien, CS Nuttall, JA Brewster, HW Roberts, KS Vandewalle
Operative Dentistry.2019; 44(1): 34. CrossRef - Comparison of the fracture resistance of three different recent composite systems in large Class II mesio-occlusal distal cavities: An in vitro study
YajuvenderSingh Hada, Sumita Panwar
Journal of Conservative Dentistry.2019; 22(3): 287. CrossRef - Physicomechanical and thermal analysis of bulk-fill and conventional composites
Armiliana Soares NASCIMENTO, José Filipe Bacalhau RODRIGUES, Rodolfo Henrique Nogueira TORRES, Kleilton Oliveira SANTOS, Marcus Vinicius Lia FOOK, Monica Soares de ALBUQUERQUE, Eliane Alves de LIMA, Pedro Tardelly Diniz FILGUEIRA, João Batista Morais dos
Brazilian Oral Research.2019;[Epub] CrossRef - Fracture Resistance of Various Bulk-fill Composite Resins in Class II MOD Cavity on Premolars: An In Vitro Study
Wandania Farahanny, Desilia Sihombing
World Journal of Dentistry.2019; 10(3): 166. CrossRef - Physicochemical properties of discontinuous S2-glass fiber reinforced resin composite
Qiting HUANG, Wei QIN, Sufyan GAROUSHI, Jingwei HE, Zhengmei LIN, Fang LIU, Pekka K. VALLITTU, Lippo V. J. LASSILA
Dental Materials Journal.2018; 37(1): 95. CrossRef - Load-bearing capacity of novel resin-based fixed dental prosthesis materials
Isil CEKIC-NAGAS, Ferhan EGILMEZ, Gulfem ERGUN, Pekka Kalevi VALLITTU, Lippo Veli Juhana LASSILA
Dental Materials Journal.2018; 37(1): 49. CrossRef - Structural and mechanical properties of a giomer-based bulk fill restorative in different curing conditions
Mustafa Sarp Kaya, Meltem Bakkal, Ali Durmus, Zehra Durmus
Journal of Applied Oral Science.2018;[Epub] CrossRef - Short fiber‐reinforced composite restorations: A review of the current literature
Sufyan Garoushi, Ausama Gargoum, Pekka K. Vallittu, Lippo Lassila
Journal of Investigative and Clinical Dentistry.2018;[Epub] CrossRef - Optimization of large MOD restorations: Composite resin inlays vs. short fiber-reinforced direct restorations
Luciana Mara Soares, Mehrdad Razaghy, Pascal Magne
Dental Materials.2018; 34(4): 587. CrossRef - A comparative study of bulk-fill composites: degree of conversion, post-gel shrinkage and cytotoxicity
Flávia Gonçalves, Luiza Mello de Paiva Campos, Ezequias Costa Rodrigues-Júnior, Fabrícia Viana Costa, Pamela Adeline Marques, Carlos Eduardo Francci, Roberto Ruggiero Braga, Letícia Cristina Cidreira Boaro
Brazilian Oral Research.2018;[Epub] CrossRef - Spot-Bonding and Full-Bonding Techniques for Fiber Reinforced Composite (FRC) and Metallic Retainers
Andrea Scribante, Paola Gandini, Paola Tessera, Pekka Vallittu, Lippo Lassila, Maria Sfondrini
International Journal of Molecular Sciences.2017; 18(10): 2096. CrossRef - Bond strength of fiber posts and short fiber-reinforced composite to root canal dentin following cyclic loading
Emre Nagas, Isil Cekic-Nagas, Ferhan Egilmez, Gulfem Ergun, Pekka K. Vallittu, Lippo V. J. Lassila
Journal of Adhesion Science and Technology.2017; 31(13): 1397. CrossRef - Fracture resistance of endodontically treated teeth restored with short fiber composite used as a core material—An in vitro study
Tejesh Gupta Garlapati, Jogikalmat Krithikadatta, Velmurugan Natanasabapathy
Journal of Prosthodontic Research.2017; 61(4): 464. CrossRef - Mechanical and structural characterization of discontinuous fiber-reinforced dental resin composite
Jasmina Bijelic-Donova, Sufyan Garoushi, Lippo V.J. Lassila, Filip Keulemans, Pekka K. Vallittu
Journal of Dentistry.2016; 52: 70. CrossRef - Letter to the Editor, “Dentin Bonding Testing Using a Mini-interfacial Fracture Toughness Approach”
N.D. Ruse
Journal of Dental Research.2016; 95(8): 953. CrossRef - Evaluation of Shear Bond Strength of Fiber-reinforced Composite and Methacrylate-based Composite to Pure Tricalcium-based Cement
Ravula A Reddy, RS Basavanna
CODS Journal of Dentistry.2016; 8(1): 25. CrossRef
 ePub Link
ePub Link Cite
CiteComparison of mechanical properties of a new fiber reinforced composite and bulk filling composites
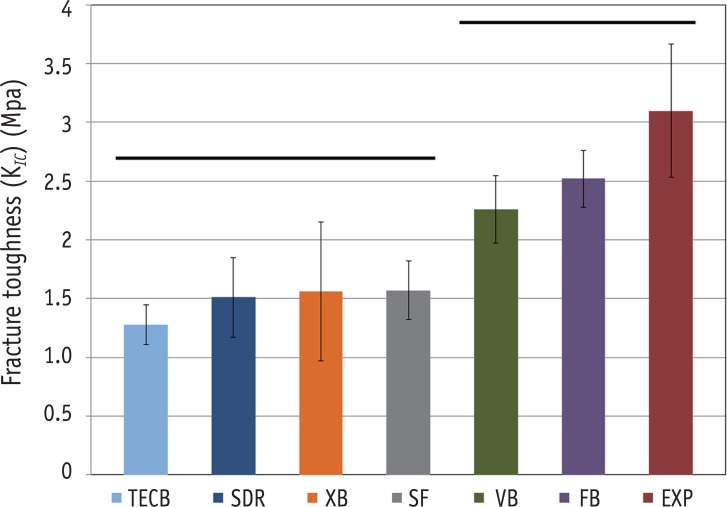
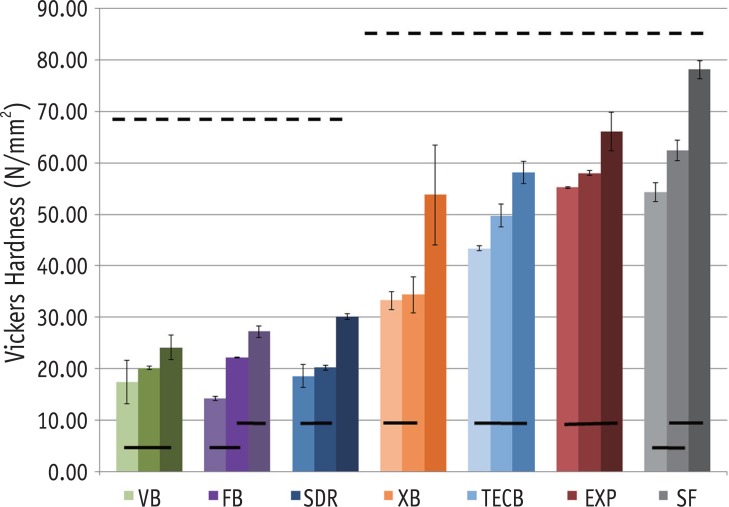
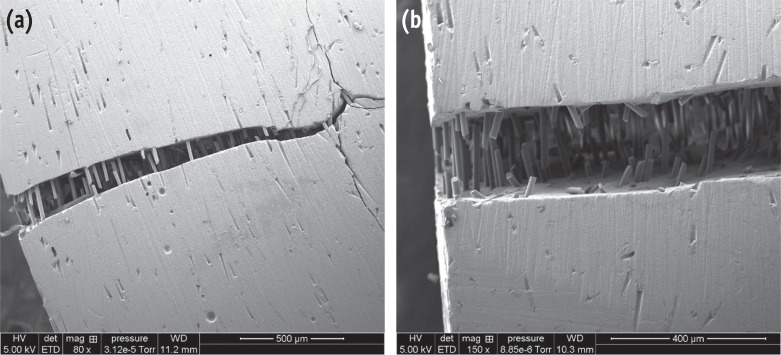
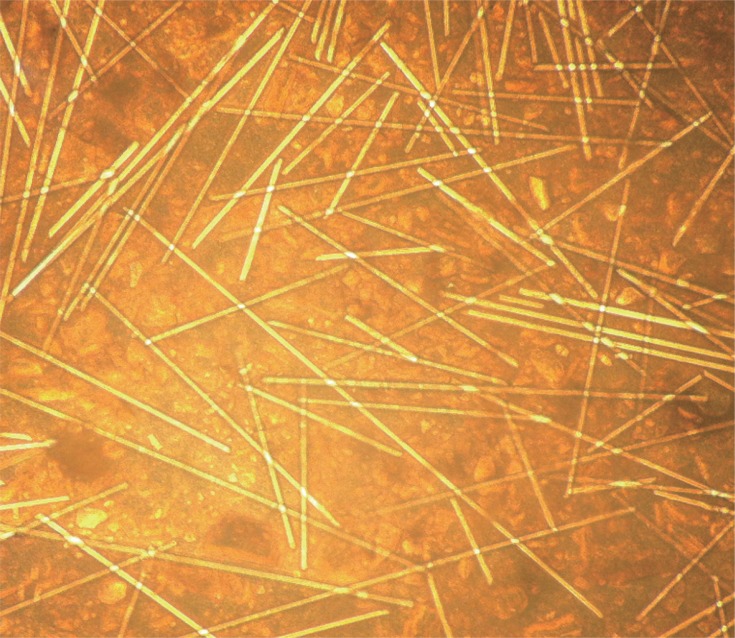
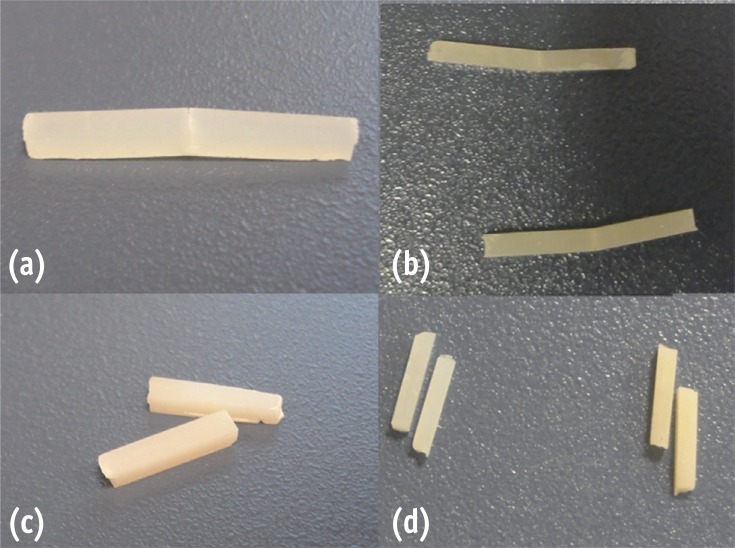
Figure 1 Bar graph illustrating fracture toughness (KIC). Straight line indicates that there was no statistically significant difference between the groups.TECB, Tetric evoceram bulk fill; SDR, SureFil SDR; XB, Xtra Base; SF, SonicFill; VB, Venus bulk fill; FB, Filtek bulk fill; EXP, EverX Posterior.
Figure 2 Bar graph illustrating Vickers hardness (N/mm2) at different curing depths of 4 mm, 2 mm and at the surface. Dotted line (-----) indicates that there was no statistically significant difference between the materials. Straight line (——) indicates that there was no statistically significant difference within the same material at different curing depths.TECB, Tetric evoceram bulk fill; SDR, SureFil SDR; XB, Xtra Base; SF, SonicFill; VB, Venus bulk fill; FB, Filtek bulk fill; EXP, EverX Posterior.
Figure 3 Scanning electron photomicrograph of fracture toughness sample (a) after failure; (b) the fiber orientation across the failure line are shown at higher magnification.
Figure 4 Microscopic image of EverX Posterior showing fiber length extending to the length of one millimeter and up to two milimeters.
Figure 5 Samples of (a) fracture toughness and (b) flexural strength tests for EverX Posterior remained connected after failure, compared to other bulk composite samples after (c) fracture toughness and (d) flexural strength, which were completely separated into two fragments.
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Comparison of mechanical properties of a new fiber reinforced composite and bulk filling composites
Materials, manufacturers, chemical composition of the matrix, fillers and filler contents
| Material | Code name | Manufacturer | Resin matrix | Inorganic filler | Lot |
|---|---|---|---|---|---|
| X-tra base | XB | Voco, Cuxhaven, Germany | Bis-EMA, MMA | 75 wt%, 58 vol% silica | 1305261 |
| Venus Bulk Fill | VB | HerausKultzer, Hanau, Germany | UDMA, EBADMA | 65 wt%, 38 vol% Barium silicate glass and silica | 100325 |
| Filtek Bulk Fill | FB | 3M ESPE, St. Paul, MN, USA | Bis-GMA, Bis-EMA, UDMA | 64 wt%, 42 vol% Zirconia | N414680 |
| Surefil SDR | SDR | Dentsply, Milford, DE, USA | TEGDMA, EBADMA | 68 wt%, 44 vol%, Barium borosilicate glass | 1202174 |
| Tetric EvoCeram Bulk Fill | TECB | Ivoclar Vivadent AG, Schaan, Liechtenstein | Bis-GMA, UDMA, Bis-EMA | 80 wt%, 61 vol% Barium glass filler | S01118 |
| SonicFill | SF | Kerr Corp., Orange, CA, USA | Bis-GMA, Bis-EMA, TEGDMA | 83 vol% Filler | 4252491 |
| EverX Posterior | EXP | GC EUROPE N.V., Leuven, Belgium | Bis-GMA, PMMA, TEGDMA | 74.2 wt%, 53.6 vol% Short E-glass fiber filler, barium glass | 1212261 |
Bis-EMA, ethoxylatedbisphenol A dimethacrylate; MMA, methylmethacrylate; UDMA, urethane dimethacrylate; EBADMA, ethoxylatedbisphenol A dimethacrylate; Bis-GMA, bisphenylglycidyldimethacrylate; TEGDMA, triethylene glycol dimethacrylate; PMMA, polymethyl methacrylate.
Flexural strength (σ, MPa) and Flexural Modulus (Eflexural, GPa) for the 2 mm and 4 mm sample groups
| Flexural strength (σ, MPa) | Flexural Modulus (Eflexural, GPa) | |||
|---|---|---|---|---|
| 2 mm | 4 mm | 2 mm | 4 mm | |
| SonicFill | 157 ± 16K | 147 ± 20k | 12.4 ± 1.6A | 6.5 ± 0.5a* |
| EverX Posterior | 153 ± 9K | 140 ± 14kl | 14.6 ± 1.6A | 6.9 ± 0.5a* |
| X-tra base | 150 ± 8K | 124 ± 13lm | 10.7 ± 1.3A | 5.7 ± 0.4b* |
| Filtek bulk fill | 139 ± 9KL | 139 ± 9kl | 6.3 ± 0.4B | 4.0 ± 0.1c* |
| Surefil SDR | 129 ± 13LM | 121 ± 19lm | 7.2 ± 1.2B | 3.9 ± 0.4c* |
| Tetric evoceram bulk fill | 118 ± 11L | 112 ± 26l | 10.8 ± 0.6A | 5.6 ± 0.2b* |
| Venus bulk fill | 116 ± 5L | 121 ± 10l | 5.0 ± 0.4B | 2.8 ± 0.2d* |
Uppercase letters identify statistically homogenous groups for 2 mm thickness samples. Lower case letters identify statistically homogenous groups for 4 mm thickness samples. Asterisks identify statistical difference between 2 mm and 4 mm thickness samples of the same material (p < 0.05).
Table 1 Materials, manufacturers, chemical composition of the matrix, fillers and filler contents
Bis-EMA, ethoxylatedbisphenol A dimethacrylate; MMA, methylmethacrylate; UDMA, urethane dimethacrylate; EBADMA, ethoxylatedbisphenol A dimethacrylate; Bis-GMA, bisphenylglycidyldimethacrylate; TEGDMA, triethylene glycol dimethacrylate; PMMA, polymethyl methacrylate.
Table 2 Flexural strength (σ, MPa) and Flexural Modulus (Eflexural, GPa) for the 2 mm and 4 mm sample groups
Uppercase letters identify statistically homogenous groups for 2 mm thickness samples. Lower case letters identify statistically homogenous groups for 4 mm thickness samples. Asterisks identify statistical difference between 2 mm and 4 mm thickness samples of the same material (

