
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 38(3); 2013 > Article
- Case Report Dilemmas pertaining to three canals in the mesiobuccal root of a maxillary second molar: a case report
- Ankit Arora1, Shashi Rashmi Acharya2, Muliya Vidya Saraswathi2, Padmaja Sharma3, Amber Ather2
-
2013;38(3):-177.
DOI: https://doi.org/10.5395/rde.2013.38.3.172
Published online: August 23, 2013
1Department of Conservative Dentistry and Endodontics, Manubhai Patel Dental College, Hospital and Oral Research Institute, Vadodara, India.
2Department of Conservative Dentistry and Endodontics, Manipal College of Dental Sciences, Manipal University, Karnataka, India.
3Department of Orthodontics and Dentofacial Orthopaedics, Manubhai Patel Dental College, Hospital and Oral Research Institute, Vadodara, India.
- Correspondence to Ankit Arora, MDS. Senior Lecturer, Department of Conservative Dentistry and Endodontics, Manubhai Patel Dental College, Hospital and Oral Research Institute, Vishwajyoti Ashram, Nr. Vidyakunj School, Munjmahuda, Vadodara, Gujarat, India, 390011. TEL, +91-9033-975629; FAX, +91-0265-278-06-64; aroraankit24@gmail.com
• Received: April 19, 2013 • Revised: June 11, 2013 • Accepted: June 17, 2013
©Copyights 2013. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,836 Views
- 9 Download
- 5 Crossref
Abstract
- The mesiobuccal root of the maxillary molars is well known to pose a hindrance during endodontic therapy. Presented here is a case of a maxillary left second molar where three canals were located in its mesiobuccal root with the use of visual and diagnostic aids. Difficulties encountered during the process of unveiling the tooth's internal anatomy were discussed. The dilemmas encountered pertained to the root canal configuration, the nomenclature of the extra canals, and the justification for the presence of a third canal. The root canal configuration of 3-2-1 was confirmed for the mesiobuccal root using information gained from clinical, radiographic, and multi-detector computed tomography (MDCT) scan findings. This case demonstrates the need for efforts to locate extra canals in the mesiobuccal root of the maxillary molars as their internal anatomy remains a mystery.
Introduction
The anatomy of the tooth has long been an unresolved mystery, and complexity of root canal morphology has been commonly found. The inability to recognize the presence of canals and treat them adequately results in unfavourable outcomes from root canal treatment.1-4 Maxillary molar morphology has been extensively studied with a specific emphasis on the mesiobuccal root because of its complexity.1,5-9 Hess and Zurcher showed that ramifications are prominent features of the mesiobuccal root of maxillary molars, and the presence of such anatomic complexities makes it difficult for clinicians to achieve endodontic treatment goals.10-12 One of the rare complexities is the presence of a third canal in the mesiobuccal root of maxillary second molar. Incidences varying from 1.6% to 16% have been reported in in vitro studies.13,14 Clinically, a third mesiobuccal canal was first reported by Ferguson et al.15 in the maxillary first molar. Ozcan et al. were first to report a third mesiobuccal canal in the maxillary second molar in a case report.16 Various canal configurations have been reported in mesiobuccal roots of maxillary second molars using different techniques in vitro.8,17-20 The canal configuration for the mesiobuccal root in the case reported by Ozcan et al. was 3-2, which is included in the classification given by Gulabivala et al. as an addition to the Vertucci classification.16,19,21 Presented here is a case where three canals were located in the mesiobuccal root of a maxillary second molar with a configuration of 3-2-1. To the best of our knowledge, the above canal configuration for the mesiobuccal root of a maxillary second molar has not been reported to date in any in vivo or in vitro studies. It was possible to confirm the internal anatomy of the mesiobuccal root and treat it adequately with the help of clinical, radiographic, and multi-detector computed tomography (MDCT) scan findings.
Case report
A 36-year-old female came to the department with the chief complaint of dull spontaneous pain in the upper left posterior tooth for the previous 2 weeks. She reported a fractured restoration on the same tooth few months back. On examination, an open cavity with a dislodged restoration and exposed mesiobuccal pulp horn was seen with respect to the maxillary left second molar. An intraoral radiograph revealed the presence of radiolucency encroaching on the pulp horn with an apparently normal periapex. Thermal sensitivity tests elicited a lingering pain in the patient. Based on the clinical and radiographic findings, a diagnosis of irreversible pulpitis was formulated.
Subsequent to anesthesia and rubber dam isolation, access cavity preparation was initiated and the mesiobuccal, distobuccal, and palatal canals were located. Anticipating the presence of extra canals, further exploration was carried out deliberately and two sticky points were located. This led to finding of two additional canals in the mesiobuccal root on the line connecting the mesiobuccal and palatal canal orifice (Figure 1). Magnifying loupes (2.5X, ST250, STAC Dental Instruments Inc., Brampton, Canada), a DG 16 endodontic explorer, and sodium hypochlorite were the adjuncts used to locate the canals. After locating the orifices, an attempt was made to understand the internal anatomy of the mesiobuccal root using K files and intraoral periapical radiographs. While negotiating the canals individually in the mesiobuccal root, there was no hindrance in the movement of the #10 K file in any of the three canals. However, simultaneous insertion posed obstruction in the vertical movement of the files in the 2 extra canals. The above finding raised an element of doubt regarding the configuration of the canals. Intraoral periapical radiographs were taken from three different horizontal angulations (Figures 2a, 2b and 2c). However, all of the radiographs suffered from overlapping of the endodontic files radiopacity. Only a mesially angulated radiograph revealed limited information on where files associated with the second and third mesiobuccal canals were seen to be meeting in the middle third of the root approximately and continue to merge with the file in first mesiobuccal canal (Figure 2b). To avoid any missed canals, and for better understanding of the tooth's internal anatomy, a MDCT (Brilliance CT 64-channel, Philips Healthcare, Andover, MA, USA) scan was suggested because cone-beam computed tomography (CBCT) was not available in the set up or in the vicinity. The interpretation regarding the number of separate orifices and canals present in the coronal third or at the orifice level was inconsistent with the clinical or radiographic findings. In contrast to the 3 orifices and canals, clinically and radiographically, MDCT revealed only 1 large canal (Figure 3a). In the middle and apical third, 2 canals and 1 canal respectively could be distinguished in both radiographic and MDCT images (Figures 3b and 3c).
The configuration of the canals in the mesiobuccal root was perceived to be 3-2-1 (Figure 4) after correlating and computing the clinical, radiographic, and MDCT scan findings. Three separate coronal orifices extending apically to three separate canals were identified as mesiobuccal (MB), middle mesiobuccal (m-MB), and palatal mesiobuccal (p-MB) based on their anatomic positions. The m-MB and p-MB merged into one canal at a distance of approximately 5 mm from the orifice level. Following this, the canal joined the MB canal at a distance of approximately 9 mm from the orifice level. Finally, the canal ended with a single apical foramen at the apex. The distances mentioned above were calculated using the thickness of each slice of the MDCT scan images, which was 0.7 mm obtained using DentaScan software (GE Healthcare, Milwaukee, WI, USA). After understanding the anatomy of the mesiobuccal root and confirming the absence of extra canals in other roots, the treatment proceeded. The biomechanical preparation of MB, distobuccal, and palatal canals was completed using ProTaper NiTi rotary files (Dentsply Maillefer, Ballaigues, Switzerland). m-MB and p-MB canals were prepared with K-files using the step-back technique. Following one week of intracanal medication with calcium hydroxide, the canals were obturated using the cold lateral compaction technique (Figure 2d).
Discussion
Despite the reports of three mesiobuccal canals in the mesiobuccal root of the maxillary second molar, there have been very few reports of such cases. Based on the literature, many reasons can be listed for the paucity of reports. One specific reason could be the anatomic complexity of the tooth itself, making it impossible to locate additional canals. Indirect or non-specific reasons could be radiographic insensitivity, lack of visual aids during setup, or lack of practitioner's commitment.
Anatomically, the openings of canals situated palatal to the MB canal are difficult to locate because of their smaller size. As explained by Eskoz et al., initially the canal in the MB root is the shape of a kidney bean.5 With continued deposition of secondary dentin, the isthmus between the poles becomes narrower and eventually may even close, resulting in multiple canals. Because the mesiolingual segment of the canal surrounds the smaller of the poles of the kidney bean, it will close off leaving a small space, thus making it more difficult to locate.
The small size and superimposition over another root canal account for the difficulty in the location of extra canals.25 The information acquired using radiographs is valuable, but it suffers from insensitivity and lack of reliability when it comes to assessment of the number of root canals present.26,27 However, with the increasing use of visual aids, especially the endodontic microscope, locating and finding canals has become easier.28,29 Loupes have also been proven to be equally effective as the endodontic microscope in locating the second mesiobuccal canal.30 Apart from the factors mentioned above, careful clinical examination and the practitioner's commitment also play a major role in the detection of extra canals.27,31
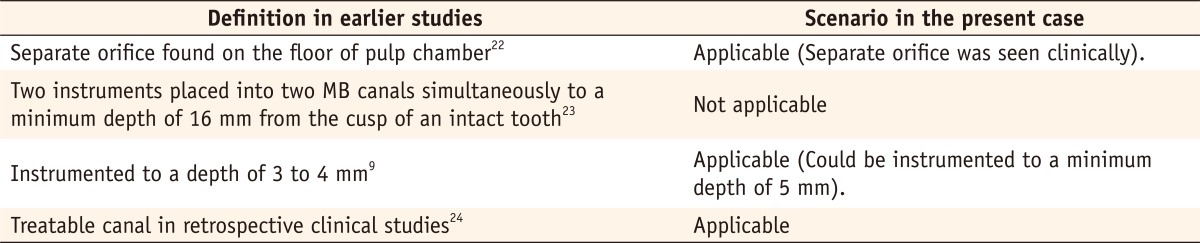
The literature has not been able to provide a clear definition of what constitutes a canal. After comparing the present case with some of the definitions given earlier, it was reasonable to assume that a third canal was present in the mesiobuccal root in the present case (Table 1).
Confusion has prevailed over the nomenclature of canals, especially in the maxillary molars. For instance, the second mesiobuccal canal has been termed the MB2, or the mesiopalatal or mesiolingual canal.32-34 Ozcan et al. termed the third mesiobuccal canal the MB3.16 However, the numbers do not reveal the anatomic location but only the presence of additional canals.35 In a recent clinical study, a new nomenclature was suggested for maxillary molars, based on which the canals in the present case were named.35 The proposed nomenclature is easy to understand and communicate, and is self-explanatory.
In the above case, a mesially angulated radiograph uncovered the internal anatomy, but because of inherent disadvantages of intraoral periapical radiographs, application of an advanced imaging modality such as CBCT was found to be valid, given its ability to localize and describe the internal and external anatomy in three dimensions.36,37 However, due to the non-availability of a CBCT unit in the vicinity, an MDCT scan was recommended. Although the MDCT provides a better image quality compared to conventional CT systems, CBCT has been proven to be better for imaging hard tissues in the maxillofacial region.38,39 In the present case, the inability of the MDCT scan to reveal three separate orifices seen clinically could be attributed to various causes. Firstly, the MDCT used here had a spatial resolution of 0.32 mm, which could be larger than the fine septa dividing the canals. Secondly, the larger voxel size could have had a negative impact. As proved by Bauman et al., detection of MB2 canals increased from 60.1% at a 0.4 mm voxel size (CBCT) to 93.3% at a 0.125 mm voxel size, and the voxel size of the MDCT used here was 0.23 mm with a slice thickness of 0.7 mm.40 Thirdly, in the present case an artifact was seen to be hindering the clarity of the MDCT images (Figure 3d). As proven before, metal objects including dental restorations in the scan field can lead to severe streaking artifacts.41-42 In the present case, an amalgam restoration on the right maxillary second molar caused a streaking artifact that distorted the images obtained at the level of the orifice and coronal third of canals from left maxillary second molar. It has been shown that MDCT suffers more from metal artifacts, which is another reason to opt for CBCT over MDCT.43
Caution was taken to avoid over-preparation of m-MB since the "danger zone" in the MB root exists across most of the distal surface of the MB root anatomically near to where the root joins the crown of the tooth.13 Henceforth, K files were used for biomechanical preparation to avoid aggressive preparation.
The present case is the first report of three canals in the mesiobuccal root of the maxillary second molars in an Indian population. No other case report on an Indian population could be found in Pubmed Search. Additionally, in an in vitro study using CBCT in an Indian population, none of the maxillary second molars were reported to have three canals in the mesiobuccal root.12 The root canal configuration of 3-2-1 encountered here is not included in the Vertucci classification or its modification, and a similar configuration was only found in the maxillary first molar in an in vitro study on a Turkish population.44
Conclusions
Finding extra canals demands anticipating their presence and commitment to locate them by careful exploration. Different diagnostic modalities may sometimes fail to be independently conclusive unless the relevant findings from them are interpreted collectively.
- 1. Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol 1969;28:419-425.ArticlePubMed
- 2. Neaverth EJ, Kotler LM, Kaltenbach RF. Clinical investigation (in vivo) of endodontically treated maxillary first molars. J Endod 1987;13:506-512.ArticlePubMed
- 3. Cheung GS. Endodontic failures - changing the approach. Int Dent J 1996;46:131-138.PubMed
- 4. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005;10:3-29.Article
- 5. Eskoz N, Weine FS. Canal configuration of the mesiobuccal root of the maxillary second molar. J Endod 1995;21:38-42.ArticlePubMed
- 6. Stropko JJ. Canal morphology of maxillary molars: clinical observations of canal configurations. J Endod 1999;25:446-450.ArticlePubMed
- 7. Blattner TC, George N, Lee CC, Kumar V, Yelton CD. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: a pilot study. J Endod 2010;36:867-870.ArticlePubMed
- 8. Neelakantan P, Subbarao C, Ahuja R, Subbarao CV, Gutmann JL. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod 2010;36:1622-1627.ArticlePubMed
- 9. Vertucci FJ. The endodontic significance of the mesiobuccal root of the maxillary first molar. US Navy Med 1974;63:29-31.PubMed
- 10. Hess W, Zurcher E. The anatomy of the root canals of the teeth of the permanent and deciduous dentition. New York: William Wood & Co.; p. 192-195.
- 11. Schilder H. Filling root canals in three dimensions. Dent Clin North Am 1967;11:723-744.Article
- 12. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am 1974;18:269-296.ArticlePubMed
- 13. Degerness RA, Bowles WR. Dimension, anatomy and morphology of the mesiobuccal root canal system in maxillary molars. J Endod 2010;36:985-989.ArticlePubMed
- 14. Calişkan MK, Pehlivan Y, Sepetçioğlu F, Türkün M, Tuncer SS. Root canal morphology of human permanent teeth in a Turkish population. J Endod 1995;21:200-204.ArticlePubMed
- 15. Ferguson DB, Kjar KS, Hartwell GR. Three canals in the mesiobuccal root of a maxillary first molar: a case report. J Endod 2005;31:400-402.ArticlePubMed
- 16. Ozcan E, Aktan AM, Ari H. A case report: unusual anatomy of maxillary second molar with 3 mesiobuccal canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:e43-e46.Article
- 17. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol 1972;33:101-110.PubMed
- 18. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589-599.ArticlePubMed
- 19. Alavi AM, Opasanon A, Ng YL, Gulabivala K. Root and canal morphology of Thai maxillary molars. Int Endod J 2002;35:478-485.ArticlePubMed
- 20. Weng XL, Yu SB, Zhao SL, Wang HG, Mu T, Tang RY, Zhou XD. Root canal morphology of permanent maxillary teeth in the Han nationality in Chinese Guanzhong area: a new modified root canal staining technique. J Endod 2009;35:651-656.ArticlePubMed
- 21. Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc 1978;97:47-50.ArticlePubMed
- 22. Nosonowitz DM, Brenner MR. The major canals of the mesiobuccal root of the maxillary 1st and 2nd molars. N Y J Dent 1973;43:12-15.PubMed
- 23. Seidberg BH, Altman M, Guttuso J, Suson M. Frequency of two mesiobuccal root canals in maxillary permanent first molars. J Am Dent Assoc 1973;87:852-856.ArticlePubMed
- 24. Fogel HM, Peikoff MD, Christie WH. Canal configuration in the mesiobuccal root of the maxillary first molar: a clinical study. J Endod 1994;20:135-137.ArticlePubMed
- 25. Libfeld H, Rotstein I. Incidence of four-rooted maxillary second molars: literature review and radiographic survey of 1,200 teeth. J Endod 1989;15:129-131.ArticlePubMed
- 26. Nattress BR, Martin DM. Predictability of radiographic diagnosis of variations in root canal anatomy in mandibular incisor and premolar teeth. Int Endod J 1991;24:58-62.ArticlePubMed
- 27. Bedford JM, Martin DM, Youngson CC. Assessment of a contrast medium as an adjunct to endodontic radiography. Int Endod J 2004;37:806-813.ArticlePubMed
- 28. Kim S, Baek S. The microscope and endodontics. Dent Clin North Am 2004;48:11-18.ArticlePubMed
- 29. Carr GB, Murgel CA. The use of the operating microscope in endodontics. Dent Clin North Am 2010;54:191-214.ArticlePubMed
- 30. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification in locating the MB2 canal in maxillary molars. J Endod 2002;28:324-327.PubMed
- 31. Imura N, Hata GI, Toda T, Otani SM, Fagundes MI. Two canals in mesiobuccal roots of maxillary molars. Int Endod J 1998;31:410-414.ArticlePubMed
- 32. Favieri A, Barros FG, Campos LC. Root canal therapy of a maxillary first molar with five root canals: case report. Braz Dent J 2006;17:75-78.ArticlePubMed
- 33. Adanir N. An unusual maxillary first molar with four roots and six canals: a case report. Aust Dent J 2007;52:333-335.ArticlePubMed
- 34. Kottoor J, Velmurugan N, Sudha R, Hemamalathi S. Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning: a case report. J Endod 2010;36:915-921.ArticlePubMed
- 35. Kottoor J, Albuquerque DV, Velmurugan N. A new anatomically based nomenclature for the roots and root canals - part 1: maxillary molars. Int J Dent 2012;2012:120565; doi: 10.1155/2012/120565. Epub 2011 Dec 15.ArticlePubMedPDF
- 36. Patel S, Horner K. The use of cone beam computed tomography in endodontics. Int Endod J 2009;42:755-756.ArticlePubMed
- 37. Lim YJ, Nam SH, Jung SH, Shin DR, Shin SJ, Min KS. Endodontic management of a maxillary lateral incisor with dens invaginatus and external root irregularity using cone-beam computed tomography. Restor Dent Endod 2012;37:50-53.Article
- 38. Flohr TG, Schaller S, Stierstorfer K, Bruder H, Ohnesorge BM, Schoepf UJ. Multi-detector row CT sytems and image-reconstruction techniques. Radiology 2005;235:756-773.ArticlePubMed
- 39. Hashimoto K, Kawashima S, Kameoka S, Akiyama Y, Honjoya T, Ejima K, Sawada K. Comparison of image validity between cone beam computed tomography for dental use and multidetector row helical computed tomography. Dentomaxillofac Radiol 2007;36:465-471.ArticlePubMed
- 40. Bauman R, Scarfe W, Clark S, Morelli J, Scheetz J, Farman A. Ex vivo detection of mesiobuccal canals in maxillary molars using CBCT at four different isotropic voxel dimensions. Int Endod J 2011;44:752-758.ArticlePubMed
- 41. Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. Radiographics 2004;24:1679-1691.ArticlePubMed
- 42. White SC, Pharoah MJ. The evolution and application of dental maxillofacial imaging modalities. Dent Clin North Am 2008;52:689-705.ArticlePubMed
- 43. Loubele M, Maes F, Jacobs R, van Steenberghe D, White SC, Suetens P. Comparative study of image quality for MSCT and CBCT scanners for dentomaxillofacial radiology applications. Radiat Prot Dosimetry 2008;129:222-226.ArticlePubMed
- 44. Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 2004;30:391-398.ArticlePubMed
REFERENCES

Figure 2
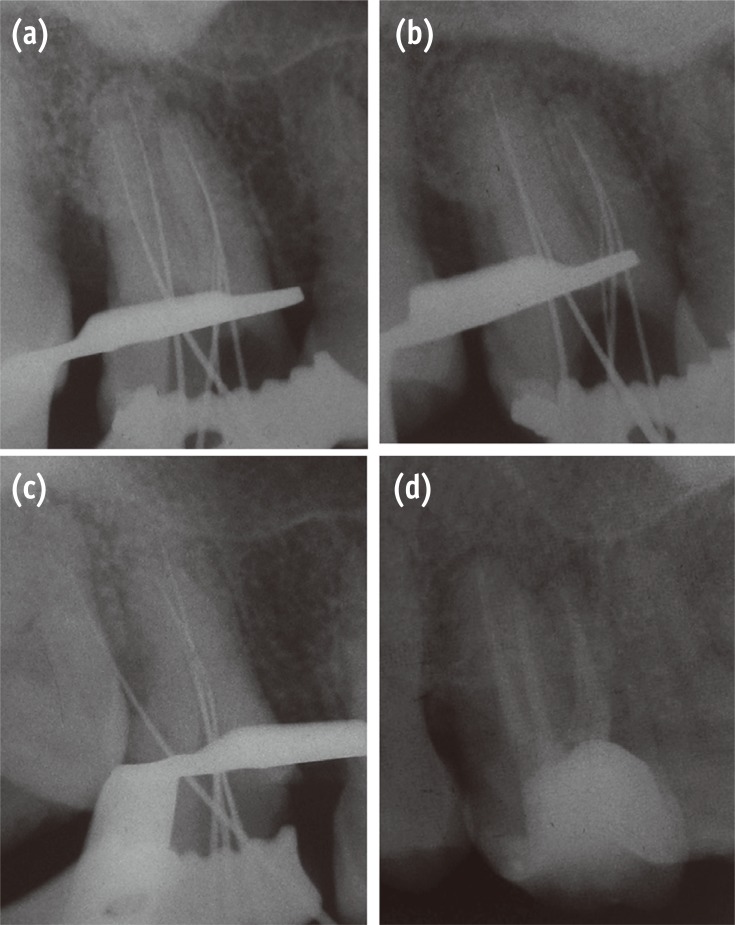
Radiographic findings. (a) Straight on angulation; (b) Mesial angulation; (c) Distal angulation; (d) Post obturation.
Figure 3
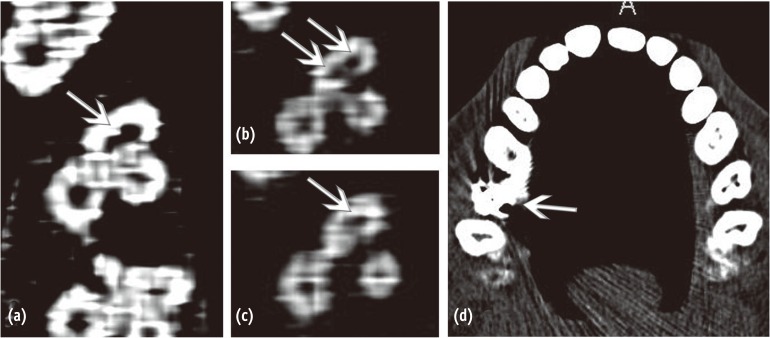
MDCT findings. (a) Orifice level; (b) Mid root level; (c) Apical region; (d) Source of artifact.

Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Incidence of an Uncommon Canal Configuration of Mesiobuccal Root with MB3 Canal in the Maxillary First Molar in Indian Population
Naveena Veeramalai, Rajesh Sasidharan Nair, Sarah Renjelina Christopher, Vijil Vimala Ravi
Indian Journal of Dental Sciences.2026;[Epub] CrossRef - Clinical Significance of Mesiobuccal and Distobuccal Canal Variations in Maxillary Molars: A Case Series and a Mini Review
Mohsen Aminsobhani, Somayeh Majidi, Vlaho Brailo
Case Reports in Dentistry.2025;[Epub] CrossRef - A case report on endodontic management of the rarest Vertucci's Type VIII configuration in maxillary second molar with three mesiobuccal canals
ShrustiAjay Govil, Geeta Asthana, Shikha Kanodia, Abhishek Parmar
Journal of Conservative Dentistry.2021; 24(4): 404. CrossRef - The MB3 canal in maxillary molars: a micro-CT study
Ronald Ordinola-Zapata, Jorge N. R. Martins, Hugo Plascencia, Marco A. Versiani, Clovis M. Bramante
Clinical Oral Investigations.2020; 24(11): 4109. CrossRef - Three Root Canals in the Mesiobuccal Root of Maxillary Molars: Case Reports and Literature Review
Ibrahim Ali Ahmad, Anas Al-Jadaa
Journal of Endodontics.2014; 40(12): 2087. CrossRef
 ePub Link
ePub Link Cite
CiteDilemmas pertaining to three canals in the mesiobuccal root of a maxillary second molar: a case report

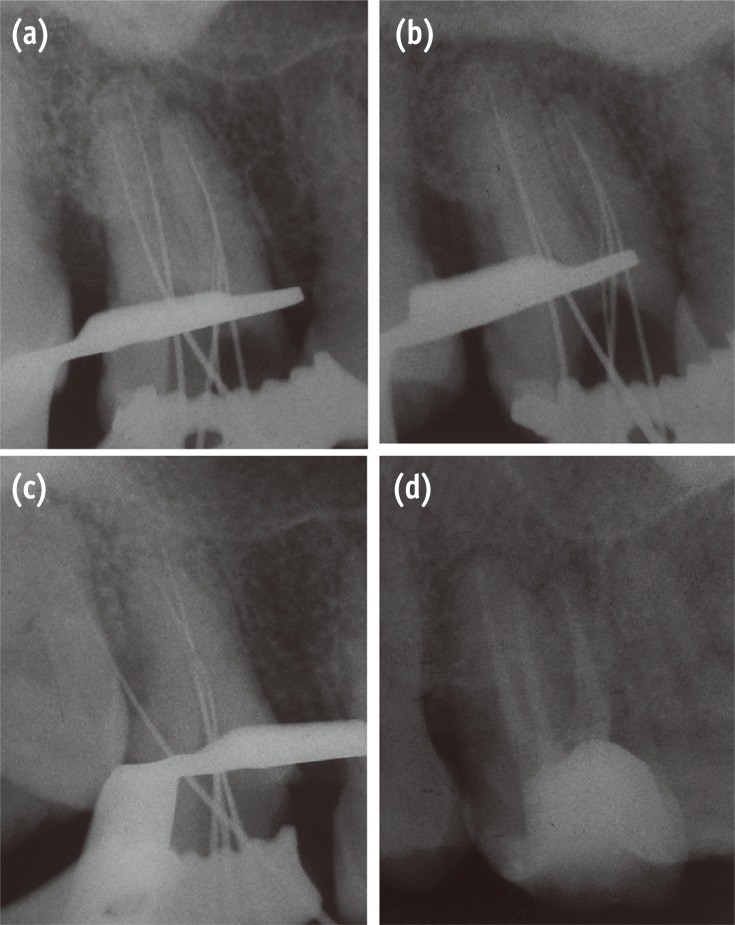
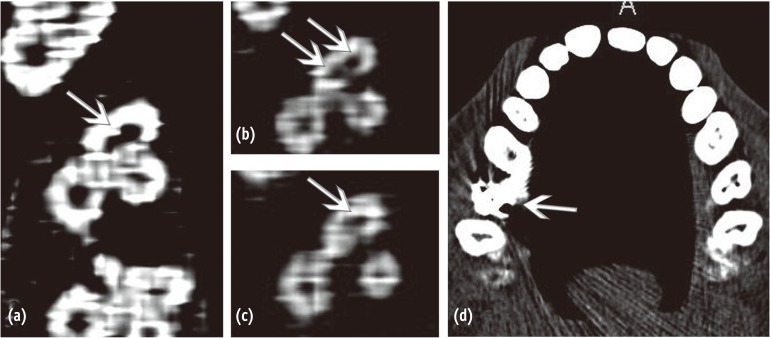
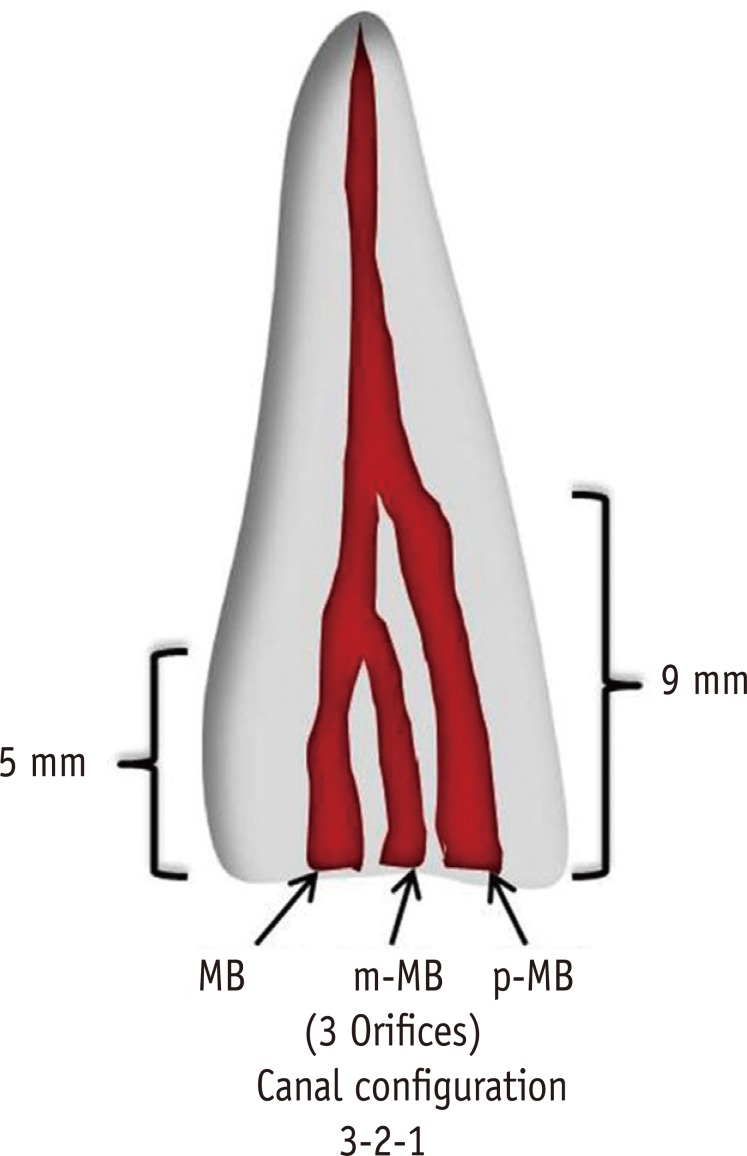
Figure 1 Three canals seen in the mesiobuccal root.
Figure 2 Radiographic findings. (a) Straight on angulation; (b) Mesial angulation; (c) Distal angulation; (d) Post obturation.
Figure 3 MDCT findings. (a) Orifice level; (b) Mid root level; (c) Apical region; (d) Source of artifact.
Figure 4 Schematic representation of canal configuration. MB, mesiobuccal; m-MB, middle mesiobuccal; p-MB, palatal mesiobuccal.
Figure 1
Figure 2
Figure 3
Figure 4
Dilemmas pertaining to three canals in the mesiobuccal root of a maxillary second molar: a case report
Justification of the presence of a third canal

Table 1 Justification of the presence of a third canal

