
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 34(5); 2009 > Article
- Original Article Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
- Seok-Woo Chang1, Yong-Keun Lee2,3, Seung-Hyun Kyung4, Hyun-Mi Yoo1, Tae-Seok Oh1, Dong-Sung Park1
-
2009;34(5):-389.
DOI: https://doi.org/10.5395/JKACD.2009.34.5.383
Published online: September 30, 2009
1Department of Conservative Dentistry, The institute of Oral Health Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
2Department of Dental Biometerials Science, School of Dentistry, Seoul National University, Korea.
3Dental Research Institute, School of Dentistry, Seoul National University, Korea.
4Department of Orthodontics, The institute of Oral Health Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
- Correspondence: Dong Sung Park. Department of Conservative Dentistry, The institute of Oral Health Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, South Korea. Tel: 82-2-3410-2429, Fax: 82-2-3410-0038, dspark@skku.edu
• Received: August 26, 2009 • Revised: September 1, 2009 • Accepted: September 11, 2009
Copyright © 2009 The Korean Academy of Conservative Dentistry
- 1,859 Views
- 5 Download
Abstract
- The purpose of this study was to investigate the fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts. 48 extracted human premolars were assigned to control group and three experimental groups. Complete crown-root fractures were experimentally induced in all control and experimental teeth. In the control group, the teeth (n=12) were bonded with resin cement and endodontically treated. Thereafter, the access cavities were sealed with dual-cured composite resin. In composite resin core - post group (n=12), the teeth were endodontically treated and access cavities were sealed with dual-cured composite resin. In addition, the fractured segments in this group were fixed using horizontal posts. In composite resin core group (n=12), the teeth were endodontically treated and the access cavities were filled with dual-cured composite resin without horizontal posts. In bonded amalgam group (n=12), the teeth were endodontically treated and the access cavities were sealed with bonded amalgam. Experimental complete crown-root fractures were induced again on repaired control and experimental teeth. The ratio of fracture resistance to original fracture resistance was analyzed with Kruskal-Wallis test. The results showed that teeth in control and composite resin core - post group showed significantly higher resistance to re-fracture than those in amalgam core group (p < 0.05). The resistance to refracture was high in the order of composite resin - post group, control group, composite resin group and bonded amalgam group. Within the scope of this study, the use of horizontal post could be beneficial in increasing the fracture resistance of previously fractured teeth.
I. Introduction
Crown-root fractures are reported to frequently occur in endodontically treated teeth.1,2) The risk of crown-root fracture was reported to be affected by access cavity design,3,4) and restoration method.5) Severe crown-root fracture unfortunately requires extraction due to subsequent loss of surrounding periodontal tissues.6,7) Recently, many studies and case reports were carried out in order to develop a treatment modality for complete crown fractures.
In 1995, Takatsu et al.8) reported a new treatment method for crown-root fractured teeth. They used orthodontic elastic and wire to approximate the fractured tooth. After performing the root canal treatment, screw posts were inserted horizontally throughout the fractured segments by following the technique described by Mondelli et al.9) Thereafter, a cast crown was placed in order to protect the tooth. The restored tooth was reported to function well for more than 3.5 years, which indicated a promising prognosis. Another method of fixing fractured tooth was reported by Yokoyama et al.10) who reported a method to fix tooth with crown fracture using orthodontic arch wire. They fixed the fractured segments with a wire through four cavity holes that were made from the surface into the pulp chamber. They proclaimed that this technique allowed for the placement of the crown restoration without removing the wire. In the one-year follow-up, the restored tooth was still functional. Another approach to treat crown fractured teeth was reported by Trope et al.,11) who extracted crown fractured teeth and replanted them after bonding them with glass-ionomer bone cement with an application of Gore-tex membrane. After a year, the teeth were still functional and the periodontal tissue surrounding the teeth healed nicely.
Methods of extraction, bonding the fractured segments, and replantation of the bonded segments that are similar to those of Trope et al.11) have been used in many recent studies,12-17) in which bonding resin and resin cement were used to fix the fractured teeth segments instead of glass-ionomer cement. The 4-META/MMA-TBB resin cement (Super-Bond C&B, Sun Medical, Kyoto, Japan) is the most frequently used type of resin cement, as it has been reported to have superior biocompatibility. In several studies, the intentional replantation with 180°rotation method was used to avoid contact with the tooth surface where the periodontal ligament was lost and the area where the bone was lost.15)
Amalgam and composite resin are commonly used as core materials following a root canal treatment. Teeth restored with bonded amalgam were reported to have a fracture resistance that was as high as that of teeth restored with composite resin.18) However, in another study, teeth restored with bonded amalgam had a lower fracture resistance than teeth restored with composite resin.19)
The use of dual-cured composite resin has advantages over chemical cured composite resin. They have a longer working time than chemical cure core resin and the ability to polymerize in the absence of light, just like chemical cured composite resin.20)
One of the most important considerations in treating crown-root fractured teeth is fixing the fractured segments firmly. In the present study, stainless-steel posts were inserted bucco-lingually across the fractured segments to fix the segments, and a dual-cured composite resin was used to bond the segments together.
The purpose of this study was to investigate the fracture resistance of teeth that were previously fractured and fixed by dual cured composite resin with horizontal posts. The fracture resistance of teeth that were previously fractured and fixed with dual-cured composite resin or bonded amalgam was also investigated. The null hypothesis of this study was that the combined use of the post and the dual-cured composite resin core has no superior effect to other methods used in this experiment.
II. Materials and methods
A total of 48 extracted caries-free, non-restored human premolars with one fully developed root and one main canal, which were extracted for orthodontic reason, were used in this study. A groove, approximately 2 mm in depth and width, was made with a #700 carbide bur (Kerr, Orange, CA, USA) on the occlusal, mesial and distal surface of each tooth. Each tooth was then positioned vertically in the center of a copper ring with a diameter of 23 mm, which was filled with acrylic resin. In this manner, the root portion 3 mm below the cementoenamel junction was embedded into the acrylic resin.
When embedding a tooth in acrylic resin, the root part was coated with a layer of silicone impression material (Surflex F, Injection Type, GC Corp., Tokyo, Japan) in order to simulate the periodontal ligament space and to facilitate the removal and repositioning of the tooth.
Each embedded intact tooth was placed in the universal testing machine (Instron, Canton, Mass, USA) that was equipped with a wide blunt tapered tip 4 mm in thickness and 1 mm in width. The tip was fitted into the groove on the occlusal surface. Vertical force was then exerted on the occlusal surface until a complete crown root fracture occurred at a crosshead speed of 1 mm/min. The force required to fracture each intact tooth was recorded.
The 48 fractured teeth were randomly divided into a control group and one of three experimental groups. Control group teeth (n=12) were removed from the acrylic resin mold. The fractured segments were bonded with 4-META/TBB-MMA resin cement (Super Bond C&B, Sun Medical Co., Kyoto, Japan). The bonded teeth segments were firmly grasped with an extraction forcep (FX151, Osung, Kimpo, Korea) in order for the resin cement to be fully cured. Thereafter, the control group teeth were repositioned into their original positions in the mold. The teeth in the experimental groups were tied with a brass wire that was 0.7 mm in diameter (Tomy Inc., Japan) without removing them from the mold.
Root canal treatment was then performed in teeth from both the control and the experimental groups. After gaining access with No.2 round bur (Komet Brasseler, Lemgo, Germany), access cavities were enlarged with Endo Z bur (Dentsply, York, PA, USA). Thereafter, root canals were enlarged with engine driven NiTi rotary instruments (Profile; Dentsply Maillefer, York, PA, USA), in which the largest size was a #40 master apical file. All of the root canal enlargements were carried out in the following sequence: Profile #25 with a 0.04 taper → Profile #25 with a 0.06 taper → Profile #30 with a 0.06 taper → Profile #35 with a 0.06 taper → Profile #40 with a 0.06 taper. Root canals were irrigated with 5.25% sodium hypochlorite between each instrumentation. Shaped and cleaned root canals were obturated by a continuous wave of the condensation technique with gutta percha (Meta-biomed, Chungju, Korea) and a AH-26 root canal sealer (Dentsply Maillerfer). The gutta percha was then removed to 3 mm under the cementoenamel junction.
After the root canal obturation and the temporary sealing of the access cavities with the Caviton (GC, Tokyo, Japan), the teeth from the control and the experimental groups were stored at 100% relative humidity and 37℃ for 24 hours in order to allow the sealer to set.
In the composite resin core - post group, the post space was prepared bucco-lingually and perpendicular to the fracture line across the fractured segments with high speed No. 1 round burs (Komet Brasseler, Lemgo, Germany) and low speed drills that were supplied by the manufacturer (Parapost, Coltene/Whaledent, Cuyahoga Falls, OH, USA). After acid etching the prepared spaces for 15 sec (ETCH 37, Bisco, Schaumberg, IL, USA) and the application of the adhesive (One-Step, Bisco), the pulpal chamber was filled with dual-cured composite resin (Bis-core, Bisco) with a syringe (Centrix, Germany). A stainless steel post (Parapost, Coltene/Whaledent) that was 0.9 mm in diameter was placed through the two prepared holes across the fractured segments before the core materials were allowed to set. The core material was cured with a light-curing unit (Optilux 501, Kerr, Danbury, USA). After the setting of the core material, the extruded part of the post was cut at the buccal and palatal surface of the tooth with a diamond bur (Komet Brasseler, Lemgo, Germany) and the brass wire was removed. In this method, the two fractured tooth segments were bonded tightly by the combined action of the dual-cured composite resin and the bucco-lingually placed post.
In the composite resin core group, the pulpal space was etched, coated with adhesive and filled with dual-cured composite resin in the same manner as in the composite resin core - post group, except for the post space preparation and the post placement.
In the amalgam core group, the pulpal chamber was etched for 15 seconds (ETCH 37, Bisco, Schaumberg, IL), coated with adhesive (One-Step, Bisco, Schaumberg, IL). After light curing of the adhesive with visible light curing unit for 10 seconds (Optilux402, Demetron/Kerr, Danbury, CT, USA), the access cavities were filled with amalgam (Woori Dongmyung, Seoul, Korea). Thereafter, the brass-wire was removed.
In the control group, the surface of the fractured segments were etched, coated with an adhesive and bonded with resin cement (Super Bond C&B, Sun Medical Co., Kyoto, Japan). The access cavities were filled with the dual-cured composite resin in the same manner as the experimental groups. The difference between the control group and the experimental groups was the method that was used to reconstruct the fractured segments. In the control group, the fractured teeth were extracted from the mold and the segments were bonded with 4-META/TBB-MMA resin cement on the fractured surface. On the contrary, the fractured segments in the experimental groups were not extracted from the mold but were bonded with bonding resin and composite resin core at only the coronal parts of the fractured teeth. The experimental design is illustrated in Figure 1.
After 24 hours, each treated tooth was re-fractured with the universal testing machine by precisely repeating the same procedure as when the intact teeth were fractured. Again, the force required to refracture each of the bonded teeth was recorded. These data were compared statistically using the Kruskal-Wallis test and the multiple comparison test using ranks.
III. Results
The forces that are required to fracture intact teeth and bonded teeth are presented in Table 1. The forces required to fracture intact teeth were 59.8 KgF, 64.5 KgF, 54.2 KgF and 73.2 KgF in control, composite resin - post group, composite resin group and amalgam core group, respectively. The forces required to fracture the bonded teeth were 32.2 KgF, 45.4 KgF, 20.1 KgF, and 17.9 KgF in control, composite resin - post group, composite resin group, and amalgam core group, respectively. The forces required to fracture the bonded teeth were considerably lower than the forces required to fracture the intact teeth. The ratios of the forces required to fracture the bonded teeth to the forces required to fracture intact teeth were 0.56, 0.73, 0.42 and 0.29 in control, composite resin - post group, composite resin group, and amalgam core group, respectively. There was a significant difference in the ratios between the composite resin core - post group versus amalgam core group (p=0.0009), as well as the control group versus amalgam core group (p=0.0289), which indicated that the resistance to fracture was greater in the composite resin core - post group and the control group than in the amalgam core group. The fracture resistance of bonded teeth fracture was highest in the resin core - post group, lower in the control group, even lower in the resin core group and the lowest in the amalgam core group.
IV. Discussion
The method used in this study was a modification of the method used in a previous study by Friedman et al., which tested the resistance of teeth that were previously fractured and bonded with various materials.21) In their study, the teeth were fractured experimentally and bonded with Ionos bone cement, Permabond 910, cyanoacrylate adhesive, and the Gluma bonding system without root canal treatment. Our experiment was different from their study in that we cleaned, shaped and obturated the root canals of the fractured teeth prior to bonding the fractured segments. When treating teeth with complete crown root fractures, endodontic treatment is usually inevitable in order to eliminate bacteria within the root canal system and the fractured gap before the placement of restoration. Root canal treatment might have an effect on the resistance of bonded teeth to fracture.22) In this sense, our experimental design more closely simulated the clinical situation and is more relevant to clinical practices. Friedman et al. reported that the force required to fracture bonded roots was at the most 20% of that required for intact roots. In our experiments, these values ranged from 19 to 70%. This can be explained by the use of the post, because it provides additional resistance to fracture.
Trushkowsky23) suggested that the use of bonded amalgam to restore a cracked tooth may be a more conservative and less expensive method than that of cast restoration. Bearn et al.24) also presented the successful treatment of cracked-tooth syndrome with the bonded amalgam restoration. De Souza et al.25) evaluated the fracture resistance of teeth restored with amalgam and bonded amalgam. They reported that the fracture resistance of teeth that were restored with Scotchbond multi-purpose plus and amalgam was superior to those restored with only amalgam. In our experiment, bonded amalgam was used to seal the access cavities in the teeth in the amalgam core group, and the teeth in this group showed a significantly lower resistance to fractures than teeth restored with composite resin and post. This means that the tooth strengthening effect of bonded amalgam was poor when compared to the other methods used in our experiments. Considering these results, it can be proposed that the bonded amalgam may increase the fracture resistance of bonded teeth, but that the strengthening effect was less than that of bonding resin. These results are also in accordance with the study by Oliveira et al.26) and Coltak et al.,27) in which they compared the fracture resistance of endodontically treated teeth that were restored with either amalgam or composite resin. In these studies, the teeth restored with composite resin were stronger that those restored with amalgam in terms of fracture resistance. Reill et al.28) also reported that the fracture resistance of endodontically treated teeth was dependent on the type of core material used.
The 4-META/TBB-MMA resin cement that was used in this study was used in many previous studies. It has been reported to have good bond strength,29) marginal integrity,30) and acceptable biocompatibility.31) These reports are consistent with the results of our study, in that the fracture resistance of the bonded teeth in the control group had the second highest value among the four groups in this study.
The placement of a post across the buccal and lingual segment to strengthen the fractured teeth has been attempted by a few researchers, and we also tried to evaluate the re-fracture resistance of this method in our in vitro experiment. Our results show that a post placed across the fractured segments does increase the resistance of teeth to fracture by holding the buccal and lingual fractured tooth segments together. Future studies are needed to evaluate the fracture resistance of fractured teeth that are restored with crown restoration. The study on the effect of complete crown root fractures on the loss of periodontal apparatus is also needed.
V. Conclusion
This study evaluated various methods that are used to strengthen bonded teeth segments to increase the resistance to fracture. Within the scope of this study, we suggest the use of resin cement rather than bonded amalgam to resist fractures. Moreover, the use of a post that crosses the fractured fragments could be considered as an additional method to enhance the fracture resistance of a repaired tooth.
- 1. Gher ME Jr, Dunlap RM, Anderson MH, Kuhl LV. Clinical survey of fractured teeth. J Am Dent Assoc. 1987;114: 174-177.ArticlePubMed
- 2. Morfis AS. Vertical root fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1990;69: 631-635.Article
- 3. Lee YG, Shin HJ, Park SH, Cho KM, Kim JW. The influence of different access cavity designs on the fracture strength in endodontically treated mandibular anterior teeth. J Korean Acad Conserv Dent. 2004;29: 515-519.Article
- 4. Choi HS, Shin DH. Fracture resistance of the three types of undermined cavity filled with composite resin. J Korean Acad Conserv Dent. 2008;33: 177-183.Article
- 5. Jung WY, Cho HW, Dong JK. A study of the fracture loads on the endodontically treated teeth by restorative techniques. J WonKwang Dent Res Inst. 1993;3: 327-337.
- 6. Talim ST, Gohil KS. Management of coronal fractures of permanent posterior teeth. J Prosthet Dent. 1974;31: 172-178.ArticlePubMed
- 7. Silvestri AR Jr, Singh I. Treatment rationale of fractured posterior teeth. J Am Dent Assoc. 1978;97: 806-810.ArticlePubMed
- 8. Takatsu T, Sano H, Burrow MF. Treatment and prognosis of a vertically fractured maxillary molar with widely separated segments: a case report. Quintessence Int. 1995;26: 479-484.PubMed
- 9. Mondelli J, Ishikiriama A, Pereira JC, Francischone CE, de Lima Navarro MF, Galan Junior J, et al. Cross-splinting a weakened tooth with a horizontal pin: a new method. J Prosthet Dent. 1987;57: 442-445.ArticlePubMed
- 10. Yokoyama K, Matsumoto K, Kinoshita J, Sasaki H, Komori T. Treatment of maxillary molars with vertical fractures. Endod Dent Traumatol. 1998;14: 287-289.ArticlePubMed
- 11. Trope M, Rosenberg ES. Multidisciplinary approach to the repair of vertically fractured teeth. J Endod. 1992;18: 460-463.ArticlePubMed
- 12. Hayashi M, Kinomoto Y, Miura M, Sato I, Takeshige F, Ebisu S. Short-term evaluation of intentional replantation of vertically fractured roots reconstructed with dentin-bonded resin. J Endod. 2002;28: 120-124.ArticlePubMed
- 13. Hayashi M, Kinomoto Y, Takeshige F, Ebisu S. Prognosis of intentional replantation of vertically fractured roots reconstructed with dentin-bonded resin. J Endod. 2004;30: 145-148.ArticlePubMed
- 14. Kudou Y, Kubota M. Replantation with intentional rotation of a complete vertically fractured root using adhesive resin cement. Dent Traumatol. 2003;19: 115-117.ArticlePubMedPDF
- 15. Kawai K, Masaka N. Vertical root fracture treated by bonding fragments and rotational replantation. Dent Traumatol. 2002;18: 42-45.ArticlePubMedPDF
- 16. Chen Q, Chen LL, Yu LY, Xiong HG. [Three dimensional finite element stress analysis in the vertical fractured first premolar after bonding and replantation]. Shanghai Kou Qiang Yi Xue. 2006;15: 202-205.PubMed
- 17. Arikan F, Franko M, Gurkan A. Replantation of a vertically fractured maxillary central incisor after repair with adhesive resin. Int Endod J. 2008;41: 173-179.ArticlePubMed
- 18. Sagsen B, Aslan B. Effect of bonded restorations on the fracture resistance of root filled teeth. Int Endod J. 2006;39: 900-904.ArticlePubMed
- 19. Camacho GB, Goncalves M, Nonaka T, Osorio AB. Fracture strength of restored premolars. Am J Dent. 2007;20: 121-124.PubMed
- 20. Foxton RM, Nakajima M, Tagami J, Miura H. Adhesion to root canal dentine using one and two-step adhesives with dual-cure composite core materials. J Oral Rehabil. 2005;32: 97-104.ArticlePubMed
- 21. Firedman S, Moshonov J, Trope M. Resistance to vertical fracture of roots, previously fractured and bonded with glass ionomer cement, composite resin and cyanoacrylate cement. Endod Dent Traumatol. 1993;9: 101-105.ArticlePubMed
- 22. Sornkul E, Stannard JG. Strength of roots before and after endodontic treatment and restoration. J Endod. 1992;18: 440-443.ArticlePubMed
- 23. Trushkowsky R. Restoration of a cracked tooth with a bonded amalgam. Quintessence Int. 1991;22: 397-400.PubMed
- 24. Bearn DR, Saunders EM, Saunders WP. The bonded amalgam restoration--a review of the literature and report of its use in the treatment of four cases of cracked-tooth syndrome. Quintessence Int. 1994;25: 321-326.PubMed
- 25. Dias de Souza GM, Pereira GD, Dias CT, Paulillo LA. Fracture resistance of premolars with bonded class II amalgams. Oper Dent. 2002;27: 349-353.PubMed
- 26. Oliveira Fde C, Denehy GE, Boyer DB. Fracture resistance of endodontically prepared teeth using various restorative materials. J Am Dent Assoc. 1987;115: 57-60.ArticlePubMed
- 27. Coltak KM, Yanikoglu ND, Bayindir F. A comparison of the fracture resistance of core materials using different types of posts. Quintessence Int. 2007;38: e511-e516.PubMed
- 28. Reill MI, Rosentritt M, Naumann M, Handel G. Influence of core material on fracture resistance and marginal adaptation of restored root filled teeth. Int Endod J. 2008;41: 424-430.ArticlePubMed
- 29. Piwowarczyk A, Bender R, Ottl P, Lauer HC. Long-term bond between dual-polymerizing cementing agents and human hard dental tissue. Dent Mater. 2007;23: 211-217.ArticlePubMed
- 30. Federlin M, Sipos C, Hiller KA, Thonemann B, Schmalz G. Partial ceramic crowns. Influence of preparation design and luting material on margin integrity--a scanning electron microscopic study. Clin Oral Investig. 2005;9: 8-17.ArticlePubMedPDF
- 31. de Souza Costa CA, Hebling J, Randall RC. Human pulp response to resin cements used to bond inlay restorations. Dent Mater. 2006;22: 954-962.ArticlePubMed
REFERENCES
Figure 1
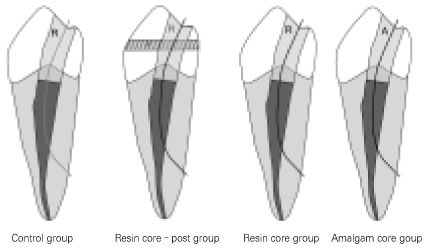
Experimental design
Control group: Fractured segments were bonded with bonding resin and the access cavities were filled with composite resin (C)
Composite resin core - post group : Access cavities were filled with composite resin (R) and horizontal posts (P) were placed across the fractured segments
Composite resin core group: Access cavities were filled with composite resin (R)
Bonded amalgam core group: Access cavities were filled with bonded amalgam (A)

Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteFracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
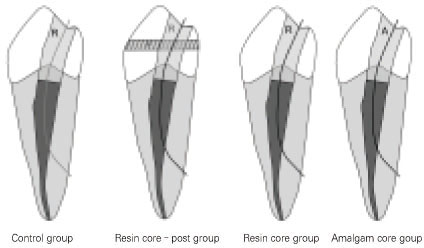
Figure 1
Experimental design
Control group: Fractured segments were bonded with bonding resin and the access cavities were filled with composite resin (C)
Composite resin core - post group : Access cavities were filled with composite resin (R) and horizontal posts (P) were placed across the fractured segments
Composite resin core group: Access cavities were filled with composite resin (R)
Bonded amalgam core group: Access cavities were filled with bonded amalgam (A)
Figure 1
Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
The forces required to fracture intact teeth (FI), fracture the bonded teeth (FB), and the ratios of FI to FB.
(NOTE. Values are mean-standard deviation. Mean values followed by the same superscript letter were not significantly different (p > 0.05))
Table 1
The forces required to fracture intact teeth (FI), fracture the bonded teeth (FB), and the ratios of FI to FB.
(NOTE. Values are mean-standard deviation. Mean values followed by the same superscript letter were not significantly different (

