
Articles
- Page Path
- HOME > Restor Dent Endod > Ahead-of print articles > Article
- Research Article Impact of bacteriological testing using an anaerobic culture system on the success of non-surgical endodontic treatment: a retrospective study
-
Jun Nakanishi,*
 , Noriko Saito-Nakayama, Shizu Hirata-Tsuchiya, Daisuke Furutama, Ayaka Miyata-Arita, Tomoki Kawayanagi, Takuya Arita, Saki Nishihama, Tomoya Naruse, Wang Chutian, Song Bingxin, Naoki Sadaoka, Tomoki Kumagai, Kazuma Yoshida, Katsuhiro Takeda, Hideki Shiba
, Noriko Saito-Nakayama, Shizu Hirata-Tsuchiya, Daisuke Furutama, Ayaka Miyata-Arita, Tomoki Kawayanagi, Takuya Arita, Saki Nishihama, Tomoya Naruse, Wang Chutian, Song Bingxin, Naoki Sadaoka, Tomoki Kumagai, Kazuma Yoshida, Katsuhiro Takeda, Hideki Shiba -
Restor Dent Endod [Epub ahead of print]
DOI: https://doi.org/10.5395/rde.2026.51.e33
Published online: July 16, 2026
Department of Biological Endodontics, Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima, Japan
- *Correspondence to Jun Nakanishi, DDS, PhD Department of Biological Endodontics, Graduate School of Biomedical and Health Sciences, Hiroshima University, 1-2-3, Kasumi, Minami-ku, Hiroshima, 734-8553, Japan Email: nakanishijun@hiroshima-u.ac.jp
• Received: October 20, 2025 • Revised: February 4, 2026 • Accepted: February 10, 2026
© 2026 The Korean Academy of Conservative Dentistry
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 46 Views
- 5 Download
Abstract
-
Objectives Residual bacteria at the time of root canal obturation significantly influence endodontic treatment outcomes in teeth with apical periodontitis, and confirmation of bacterial elimination from the root canal prior to obturation may improve long-term prognosis. However, the contribution of root canal bacterial culture to treatment outcomes in teeth with infected root canals is debated. This study aimed to retrospectively evaluate treatment outcomes in cases in which root canal obturation was performed after confirming negative bacteriological test results.
-
Methods The medical records of patients with apical periodontitis or pulp necrosis in whom root canal obturation was performed after confirming a negative bacteriological test result using an anaerobic culture system at the Department of Endodontics and Operative Dentistry at Hiroshima University Hospital between April 1, 2015, and September 30, 2023, were retrospectively reviewed. Treatment outcomes were assessed by comparing dental radiographs obtained before treatment with those obtained during the follow-up, ranging from 3 to 24 months after root canal obturation.
-
Results This retrospective study included 284 teeth from 218 patients, and the success rate was 89.1%. Tooth type, number of root canals, type of treatment, preoperative radiolucency around the root apex, preoperative root canal obturation material, dentist experience, and postoperative extent of root canal obturation material did not significantly affect treatment outcomes.
-
Conclusions The findings of this retrospective study suggest that infection control incorporating bacteriological examination of root canals using an anaerobic culture system may contribute to a high success rate of nonsurgical endodontic treatment, regardless of other prognostic factors.
INTRODUCTION
Residual bacteria at the time of root canal obturation significantly influence the outcomes of endodontic treatment in teeth with apical periodontitis [1,2]; thus, confirmation of bacterial elimination from the root canal prior to obturation may improve the long-term prognosis of the tooth. The presence of bacterial infection in the root canal can be evaluated using bacteriological culture. Although various bacteria can be detected in the root canal, because the root canal is an anaerobic environment, anaerobes dominate the bacterial flora [3]. Furthermore, approximately 80% of the bacteria in infected dentin, which is caused by bacterial invasion of the root canal walls, are obligate anaerobes [4]. Therefore, anaerobic cultures are considered more appropriate than aerobic cultures for bacteriological examination of the root canal.
Few studies have reported that a negative anaerobic culture result prior to root canal obturation is associated with a favorable prognosis [5,6]. Conversely, other studies have found no significant difference in long-term outcomes between cases with negative and positive anaerobic culture results prior to obturation [7]. Thus, the contribution of bacteriological culture to treatment outcomes in infected root canals remains controversial [8].
Several factors influence the outcome of root canal treatment, including tooth type, number of root canals, type of treatment, presence of preoperative radiolucency around the root apex, type of preoperative obturation material, dentist experience, and the extent of postoperative obturation. However, the effect of these factors on the prognosis of cases in which obturation is performed after confirming a negative anaerobic culture result remains unclear.
This retrospective study analyzed clinical data collected from the medical records of participants who had undergone treatment for infected root canals, including bacteriological examination of root canals using an anaerobic culture system. The aim was to determine whether such examinations are necessary for achieving successful outcomes in nonsurgical endodontic treatment of infected root canals, while accounting for various factors that may influence treatment prognosis.
METHODS
This retrospective study, which used data extracted from previously recorded medical charts, was approved by the Ethical Committee for Epidemiology of Hiroshima University (No. E2023-0206) and conducted in accordance with the principles of the Declaration of Helsinki. As the study used existing clinical data and involved no direct patient intervention, informed consent was obtained using an opt-out approach. Information related to the study and handling of personal data was disclosed on the website of the institution, where patients were given the opportunity to decline participation.
Root canal obturation at the Department of Endodontics and Operative Dentistry, Hiroshima University Hospital, is routinely performed only after negative bacteriological results are confirmed using an anaerobic culture system operated by the Center for Oral Clinical Examination of the hospital. In this retrospective study, we reviewed clinical data from patients who underwent infected root canal treatment, including bacteriological assessment with the anaerobic culture system, at the Department of Endodontics and Operative Dentistry between April 1, 2015 and September 30, 2023. Dentists were divided into two groups according to their experience: <5 years and ≥5 years. Patients diagnosed with apical periodontitis or pulp necrosis who had undergone root canal obturation after bacteriological examination of the root canal using the anaerobic culture system and had not refused to participate in this study were included. The exclusion criteria were (i) no follow-up between 3 and 24 months after root canal obturation, (ii) root canal treatment without rubber dam isolation, and (iii) root canal treatment prior to surgical endodontic treatment. Figure 1 shows the study flowchart according to the inclusion and exclusion criteria and the number of cases treated by dentists with <5 years and ≥5 years of experience, respectively.
The parameters analyzed were age, sex, tooth type, number of root canals, type of treatment (initial treatment or retreatment), preoperative radiolucency around the root apex, preoperative root canal obturation material, dentist experience (<5 years, or ≥5 years), and pre-and postoperative extension of the root canal obturation material (under, adequate, or over). In this retrospective study, the retreatment group included cases in which patients were referred to the hospital due to poor progress or other reasons, even though retreatment had already been initiated at other hospitals and dental clinics. Treatment outcomes were evaluated by comparing dental radiographs obtained before treatment initiation with those obtained 3–24 months after root canal obturation, using the reduction in lesion size of the apical radiolucency as a parameter. Based on previous studies, good outcomes were defined as disappearance or decrease in bone resorption around the root apex, and when the bone resorption around the root apex remained unchanged or increased, the outcome was defined as poor [9,10]. Clinical symptoms and cone-beam computed tomography images were not used for evaluation. In addition, the outcome was classified as good when the absence of bone resorption at the root apex observed before treatment initiation remained unchanged during the follow-up. In contrast, the outcomes of teeth for which surgical endodontic treatment or extraction was indicated because of poor progress during the follow-up period were classified as poor. All radiographic evaluations were performed by at least two independent evaluators. Figure 2 shows representative pre and postoperative dental radiographs illustrating good and poor outcomes. The kappa coefficient calculated to assess inter-evaluator agreement was 0.789, indicating substantial agreement. The cutoff for number of years of dental experience (5 years) was based on the Japanese Endodontic Association’s application requirements for endodontic specialists and the post-licensure training curriculum in Japan.
Prior to obturation, all dentists confirmed that the bacteriological tests of the root canal, conducted at the Center of Oral Clinical Examination, Hiroshima University Hospital, using an anaerobic culture system, showed negative results, with no clinical symptoms. The bacterial examination is outlined as follows [11]: the anaerobic culture system comprised an AnaeroPack (Mitsubishi Gas Chemical Co., Inc., Tokyo, Japan), AnaeroPack pouches and sealing clips (Mitsubishi Gas Chemical Co., Inc., Tokyo, Japan), an anaerobic indicator (Mitsubishi Gas Chemical Co., Inc., Tokyo, Japan), sterile cotton swabs, sterile paper points, and culture media that includes Brucella blood agar (Kyokuto Pharmaceutical Industrial Co., Ltd., Tokyo, Japan) and thioglycolate liquid medium (Nihon Pharmaceutical Co., Ltd., Osaka, Japan). Specimens (root canal bacteria) were collected under rubber dam isolation by inserting a sterile paper point moistened with sterile saline into the root canal. The paper point containing the specimen was immediately placed into the liquid medium and suspended. Subsequently, a portion of the liquid medium was inoculated onto blood agar plates using a sterile cotton swab. An anaerobic environment (N₂, 80% and CO₂, 20%) was established by sealing the blood agar plate containing the specimen, the liquid medium, the AnaeroPack, and the anaerobic indicator within an AnaeroPack pouch, which was incubated at 37°C. Culture evaluation was performed 4–7 days post-initiation. Colony formation on the culture medium surface was considered a positive result, whereas its absence was considered a negative result.
All patients underwent nonsurgical endodontic treatment according to standard protocols [10]. Following completion of root canal preparation, enlargement, and irrigation, bacteriological testing was performed when the operator, based on clinical symptoms, judged it appropriate to proceed with root canal obturation. Root canal obturation was performed using the lateral or vertical condensation technique with gutta-percha points (GC Corporation, Tokyo, Japan) and a eugenol-based root canal sealer (Nishika Canal Sealer; Nihon Shika Yakuhin Co., Ltd., Yamaguchi, Japan) or a non-eugenol-based root canal sealer (Canals-N; GC Showayakuhin Corporation, Tokyo, Japan).
Statistical analysis was performed using JMP Pro software (ver. 17.0; SAS Institute Inc, Cary, NC, USA). The chi-square test and multiple logistic regression analysis were used to compare success rates between the two groups, and statistical significance was set at p < 0.05. In the multiple logistic regression analysis, the postoperative extent of root canal obturation material was excluded due to unstable parameter estimates. The chi-square test results showed that for tooth type and postoperative extent of root canal obturation material, cells with expected values below 5 accounted for >20% of the total; therefore, the Fisher exact test was performed for these two groups.
RESULTS
A total of 787 infected teeth underwent root canal treatment and bacteriological examination of the root canal using an anaerobic culture system during the study period (Figure 1). Of these, 284 teeth with confirmed clinical outcomes between 3 and 24 months after root canal obturation were included (Figure 1). Among these, 67 teeth from 52 patients and 217 teeth from 170 patients were treated by dentists with <5 years and ≥5 years, respectively. The demographic distribution of the patients is shown in Table 1. The treatment success rate in this retrospective study was 89.1% (Table 2). The chi-square test and Fisher exact test show that tooth type, number of root canals, type of treatment, preoperative radiolucency around the root apex, preoperative root canal obturation material, dentist experience, and postoperative extension of the root canal obturation material did not significantly affect treatment outcomes (Table 3). The multiple logistic regression analysis showed no group significantly affects treatment outcomes, consistent with the chi-square and Fisher exact test results (data not shown).
DISCUSSION
Anaerobic bacteria predominantly form biofilms in the anaerobic environment of the root canal [3,4]. Because elimination of bacteria from the root canal significantly influences the outcome of root canal treatment [1,2], confirming the aseptic condition of the root canal after cleaning and shaping prior to obturation may increase the success rate of root canal treatment. In addition, the elimination of Enterococcus faecalis, a problematic facultative anaerobic bacterium, from the root canal is important for improving the success rate of root canal treatment [12–14]. An in vivo study in monkeys reported that treatment outcomes were influenced more by the presence of bacteria in the root canal than by the quality of root canal obturation [15]. Therefore, bacteriological examination of the root canal using an anaerobic culture system is recommended to confirm the absence of bacteria causing apical periodontitis or pulp necrosis. As the Center for Oral Clinical Examination, Hiroshima University Hospital has this culture system, dentists in the Department of Endodontics and Operative Dentistry routinely use it as a standard practice.
The treatment success rate in this retrospective study was 89.1%, which is higher than that previously reported [16–20]. Several factors influence endodontic treatment outcomes [16–25]. Particularly, rubber dam isolation during endodontic treatment significantly influences tooth survival [21] and was performed in all cases in this study. In this study, we evaluated factors that influenced the outcomes of root canal treatment in previous studies (type of treatment, preoperative radiolucency around the root apex, preoperative root canal obturation material, years of dental experience, and postoperative extension of the root canal obturation material). Surprisingly, none of these significantly affected treatment outcomes (Table 3). Particularly, this study highlighted that the dentist’s experience did not significantly influence the success rate. Previous studies have reported that treatment planning and technical skills for performing root canal treatment depend on the dentist’s experience, and that the success rate of endodontic treatment is significantly higher when performed by specialists than when performed by general dentists [22,26].
The distribution of treatment difficulty remains unclear; however, the success rate in this retrospective study did not vary with the dentist’s experience, and a high success rate was achieved. This suggests that bacteriological examination of the root canal using an anaerobic culture system may result in less clinically experienced dentists achieving successful nonsurgical endodontic treatment.
This retrospective study had some limitations, including a small sample size, a wide range of observation periods (3–24 months), a lack of consideration of the type of restoration after root canal obturation, and crown leakage. Additionally, because samples are collected using sterilized paper points inserted into saline-soaked root canals with rubber dam isolation, anaerobic bacterial culture primarily detects bacteria in the main root canal(s) rather than in lateral root canals. Furthermore, the study did not include a comparison of success rates with cases in which root canal obturation was performed after confirming a positive anaerobic bacterial culture test, since the establishment of a positive control group that could potentially lead to poor clinical outcomes for patients was expected to be disapproved by the Ethical Committee for Epidemiology of Hiroshima University. Another limitation is that anaerobic culture results require 4–7 days to become available. Therefore, because an interval is necessary between sampling and obturation, intracanal medicament using calcium hydroxide paste and a tight temporary seal using a double layer of temporary stopping material and glass ionomer cement were routinely applied to minimize the risk of reinfection during nonsurgical endodontic treatment. Previous studies supporting the utility of bacterial culture have shown that, when root canal treatment and obturation were performed on infected canals, prognosis was better when bacterial culture tests were negative prior to obturation than when they were positive [1,6]. Although this study has certain limitations, anaerobic bacterial culture remains an important procedure for achieving favorable outcomes in nonsurgical endodontic treatment.
CONCLUSIONS
The success rate of root canal treatment in teeth in which obturation was performed after confirming negative anaerobic bacterial culture test results was not influenced by factors conventionally believed to affect treatment outcomes. Notably, the dentist’s experience had no impact on treatment outcomes. Based on the findings in this retrospective study, in addition to rubber dam isolation, implementing standardized infection control through bacteriological examination of the root canal using an anaerobic culture system may be considered to achieve high success rates in root canal treatment.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING/SUPPORT
The authors have no financial relationships relevant to this article to disclose.
-
ACKNOWLEDGEMENTS
We are deeply grateful for the financial support provided by Dr. Shunichi Oshima. We also sincerely appreciate the staff of the Center of Oral Clinical Examination at Hiroshima University Hospital for conducting bacteriological tests using an anaerobic culture system.
-
AUTHOR CONTRIBUTIONS
Conceptualization, Data curation, Methodology: Nakanishi J, Saito-Nakayama N. Formal analysis: Nakanishi J, Hirata-Tsuchiya S. Investigation: Furutama D, Miyata-Arita A, Kawayanagi T, Arita T, Nishihama S, Naruse T, Sadaoka N, Kumagai T, Yoshida K. Project administration: Hirata-Tsuchiya S. Supervision: Takeda K, Shiba H. Visualization: Nakanishi J. Writing - original draft: Nakanishi J. Writing - review & editing: Hirata-Tsuchiya S, Wang C, Song B, Takeda K, Shiba H. All authors read and approved the final manuscript.
-
DATA SHARING STATEMENT
The datasets are not publicly available but are available from the corresponding author upon reasonable request.
-
DISCLOSURE OF GENERATIVE AI IN SCIENTIFIC WRITING
No generative AI technologies were used in the preparation of this manuscript.
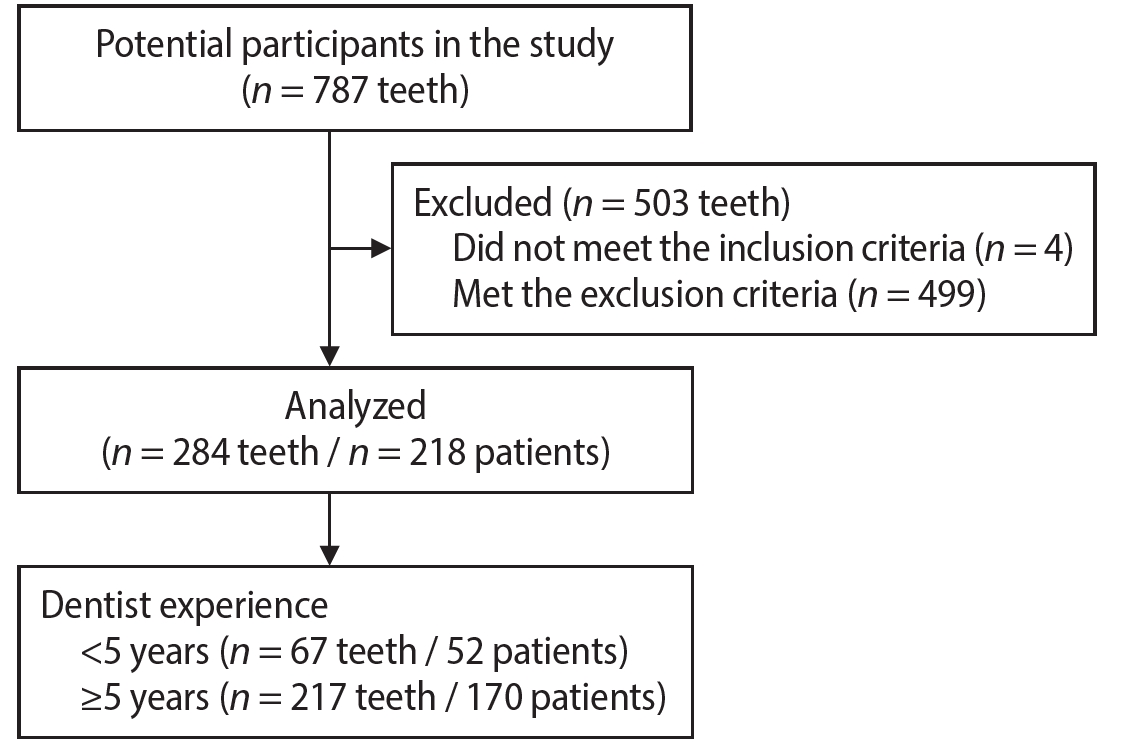
Figure 2.
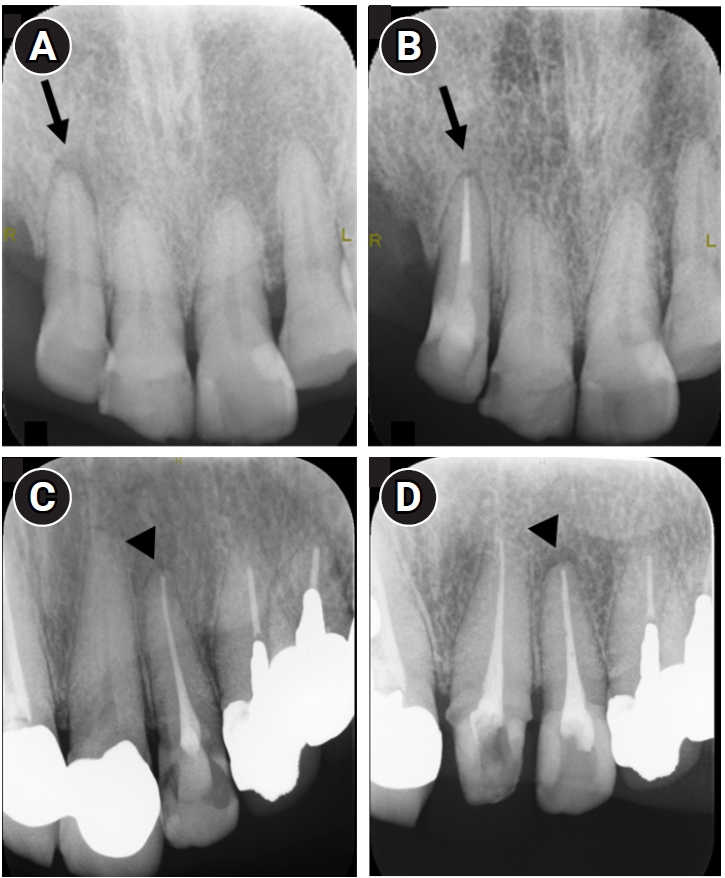
Representative pre- and postoperative dental radiographs showing good and poor outcomes. Preoperative (A) and postoperative (B) radiographs of a maxillary right lateral incisor (arrows). The 1-year and 4-month follow-up radiograph demonstrates a good outcome. Preoperative (C) and postoperative (D) radiographs of a maxillary left lateral incisor (arrowheads). The 7-month follow-up radiograph shows a poor outcome.
Table 1.
Demographic distribution of the cases
Table 2.
Treatment outcomes
| Variable | Value |
|---|---|
| Total tooth number | 284 |
| Treatment outcome | |
| Good | 253 (89.1) |
| Poor | 31 (10.9) |
Table 3.
Treatment outcomes according to each characteristic
- 1. Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997;30:297-306.ArticlePubMed
- 2. Zandi H, Petronijevic N, Mdala I, Kristoffersen AK, Enersen M, Rôças IN, et al. Outcome of endodontic retreatment using 2 root canal irrigants and influence of infection on healing as determined by a molecular method: a randomized clinical trial. J Endod 2019;45:1089-1098.e5.ArticlePubMed
- 3. Sato T, Yamaki K, Ishida N, Hashimoto K, Takeuchi Y, Shoji M, et al. Cultivable anaerobic microbiota of infected root canals. Int J Dent 2012;2012:609689.ArticlePubMedPMCPDF
- 4. Ando N, Hoshino E. Predominant obligate anaerobes invading the deep layers of root canal dentin. Int Endod J 1990;23:20-27.ArticlePubMed
- 5. Yoneda M, Kita S, Suzuki N, Macedo SM, Iha K, Hirofuji T. Application of a chairside anaerobic culture test for endodontic treatment. Int J Dent 2010;2010:942130.ArticlePubMedPMCPDF
- 6. Waltimo T, Trope M, Haapasalo M, Ørstavik D. Clinical efficacy of treatment procedures in endodontic infection control and one year follow-up of periapical healing. J Endod 2005;31:863-866.ArticlePubMed
- 7. Peters LB, Wesselink PR. Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganisms. Int Endod J 2002;35:660-667.ArticlePubMed
- 8. Sathorn C, Parashos P, Messer HH. How useful is root canal culturing in predicting treatment outcome? J Endod 2007;33:220-225.ArticlePubMed
- 9. Hoskinson SE, Ng YL, Hoskinson AE, Moles DR, Gulabivala K. A retrospective comparison of outcome of root canal treatment using two different protocols. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:705-715.ArticlePubMed
- 10. Hirata-Tsuchiya S, Furutama D, Saito-Nakayama N, Naruse T, Kawayanagi T, Nishihama S, et al. Increasing the apical sizes of root enlarged for root canal obturation influences the outcome of single-root-canal teeth affected by apical periodontitis. Eur Endod J 2024;9:418-424.ArticlePubMedPMCPDF
- 11. Iwata T, Hino T, Kitamoto Y, Shiba H, Ogawa I, Morimoto M, et al. Bacterial examination with anaerobic culture system for samples from root canals for the achievement of biological root canal treatment. J Jpn Endod Assoc 2007;28:1-8.
- 12. Stuart CH, Schwartz SA, Beeson TJ, Owatz CB. Enterococcus faecalis: its role in root canal treatment failure and current concepts in retreatment. J Endod 2006;32:93-98.ArticlePubMed
- 13. Alghamdi F, Shakir M. The influence of enterococcus faecalis as a dental root canal pathogen on endodontic treatment: a systematic review. Cureus 2020;12:e7257.ArticlePubMedPMC
- 14. Kayaoglu G, Erten H, Bodrumlu E, Ørstavik D. The resistance of collagen-associated, planktonic cells of Enterococcus faecalis to calcium hydroxide. J Endod 2009;35:46-49.ArticlePubMed
- 15. Fabricius L, Dahlén G, Sundqvist G, Happonen RP, Möller AJ. Influence of residual bacteria on periapical tissue healing after chemomechanical treatment and root filling of experimentally infected monkey teeth. Eur J Oral Sci 2006;114:278-285.ArticlePubMed
- 16. Elemam RF, Pretty I. Comparison of the success rate of endodontic treatment and implant treatment. ISRN Dent 2011;2011:640509.ArticlePubMedPMCPDF
- 17. Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990;16:498-504.ArticlePubMed
- 18. de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: the Toronto study: phases 3 and 4: orthograde retreatment. J Endod 2008;34:131-137.ArticlePubMed
- 19. de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: the Toronto study: phase 4: initial treatment. J Endod 2008;34:258-263.ArticlePubMed
- 20. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004;30:1-4.ArticlePubMed
- 21. Lin PY, Huang SH, Chang HJ, Chi LY. The effect of rubber dam usage on the survival rate of teeth receiving initial root canal treatment: a nationwide population-based study. J Endod 2014;40:1733-1737.ArticlePubMed
- 22. Alley BS, Kitchens GG, Alley LW, Eleazer PD. A comparison of survival of teeth following endodontic treatment performed by general dentists or by specialists. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:115-118.ArticlePubMed
- 23. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature--Part 2. Influence of clinical factors. Int Endod J 2008;41:6-31.ArticlePubMed
- 24. Azim AA, Griggs JA, Huang GT. The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J 2016;49:6-16.ArticlePubMed
- 25. Mello FW, Miguel AF, Ribeiro DM, Pasternak B, Porporatti AL, Flores-Mir C, et al. The influence of apical extent of root canal obturation on endodontic therapy outcome: a systematic review. Clin Oral Investig 2019;23:2005-2019.ArticlePubMedPDF
- 26. Nagi SE, Khan FR, Rahman M. Practice of endodontic re-treatment in four cities of Pakistan. J Ayub Med Coll Abbottabad 2017;29:445-449.PubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteImpact of bacteriological testing using an anaerobic culture system on the success of non-surgical endodontic treatment: a retrospective study
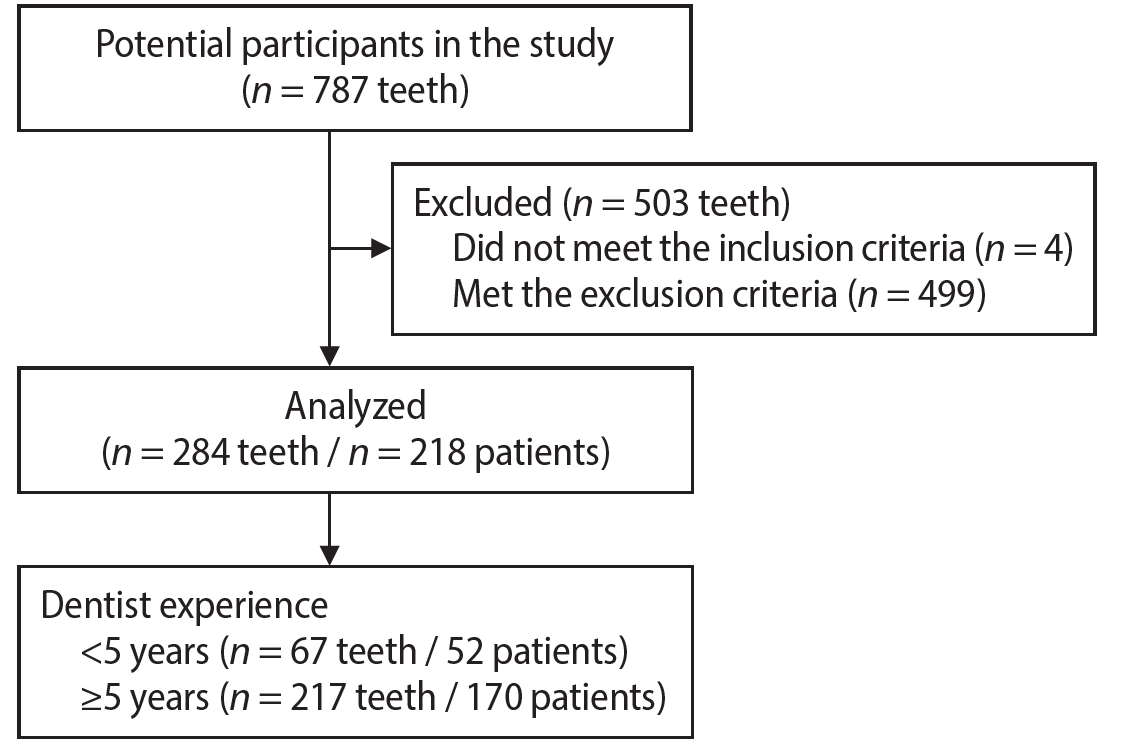
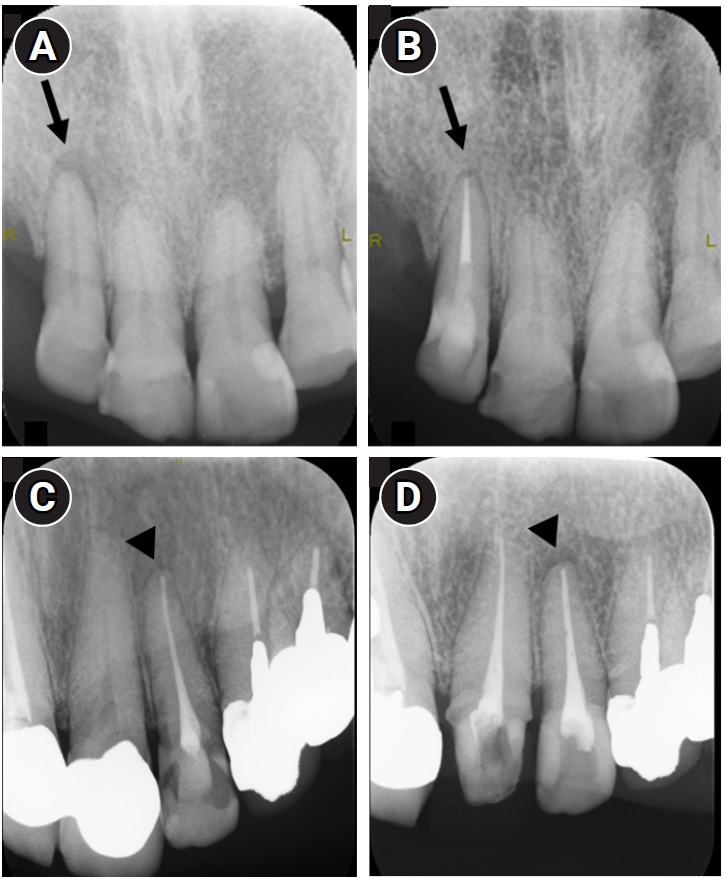
Figure 1. Study flow chart.
Figure 2. Representative pre- and postoperative dental radiographs showing good and poor outcomes. Preoperative (A) and postoperative (B) radiographs of a maxillary right lateral incisor (arrows). The 1-year and 4-month follow-up radiograph demonstrates a good outcome. Preoperative (C) and postoperative (D) radiographs of a maxillary left lateral incisor (arrowheads). The 7-month follow-up radiograph shows a poor outcome.
Figure 1.
Figure 2.
Impact of bacteriological testing using an anaerobic culture system on the success of non-surgical endodontic treatment: a retrospective study
| Variable | Value |
|---|---|
| Total tooth number | 284 |
| Age (yr) | 62 (48–72) |
| Sex | |
| Male | 73 (25.7) |
| Female | 211 (74.3) |
| Tooth type | |
| Maxillary anterior | 70 (24.7) |
| Maxillary premolars | 44 (15.5) |
| Maxillary molars | 51 (18.0) |
| Mandibular anterior | 27 (9.5) |
| Mandibular premolars | 29 (10.2) |
| Mandibular molars | 63 (22.2) |
| Number of root canals | |
| Single | 150 (52.8) |
| Multiple | 134 (47.2) |
| Type of treatment | |
| Initial treatment | 101 (35.6) |
| Retreatment | 183 (64.4) |
| Preoperative radiolucency around the root apex | |
| Absent | 82 (28.9) |
| Present | 202 (71.1) |
| Preoperative root canal obturation material | |
| Absent | 130 (45.8) |
| Present | 154 (54.2) |
| Preoperative extent of root canal obturation material | |
| Under | 87 (30.6) |
| Adequate | 55 (19.4) |
| Over | 3 (1.1) |
| Postoperative location of root canal obturation material | |
| Under | 25 (8.8) |
| Adequate | 249 (76.8) |
| Over | 10 (3.5) |
| Dentist experience | |
| <5 yr | 67 (23.6) |
| ≥5 yr | 217 (76.4) |
| Variable | Value |
|---|---|
| Total tooth number | 284 |
| Treatment outcome | |
| Good | 253 (89.1) |
| Poor | 31 (10.9) |
| Variable | Good | Poor | p-value |
|---|---|---|---|
| Tooth type | |||
| Maxillary anterior | 64 (22.5) | 6 (2.1) | 0.2906 |
| Maxillary premolars | 42 (14.8) | 2 (0.7) | |
| Maxillary molars | 44 (15.5) | 7 (2.5) | |
| Mandibular anterior | 23 (8.1) | 4 (1.4) | |
| Mandibular premolars | 23 (8.1) | 6 (2.1) | |
| Mandibular molars | 57 (20.1) | 6 (2.1) | |
| Number of root canals | |||
| Single | 134 (47.2) | 16 (5.6) | 0.8869 |
| Multiple | 119 (41.9) | 15 (5.6) | |
| Type of treatment | |||
| Initial treatment | 93 (32.8) | 8 (2.8) | 0.2292 |
| Retreatment | 160 (56.3) | 23 (8.1) | |
| Preoperative radiolucency around the root apex | |||
| Absent | 77 (27.1) | 5 (1.8) | 0.0971 |
| Present | 176 (62.0) | 26 (9.2) | |
| Preoperative root canal obturation material | |||
| Absent | 120 (42.3) | 10 (3.5) | 0.1095 |
| Present | 133 (46.8) | 21 (7.4) | |
| Dentist experience | |||
| <5 yr | 62 (21.8) | 5 (1.8) | 0.2998 |
| ≥5 yr | 191 (67.3) | 26 (9.2) | |
| Postoperative extent of root canal obturation material | |||
| Under | 25 (8.8) | 0 (0) | 0.1113 |
| Adequate | 218 (76.8) | 31 (10.9) | |
| Over | 10 (3.5) | 0 (0) |
Table 1. Demographic distribution of the cases
Values are presented as number, median (interquartile range), or number (%).
Table 2. Treatment outcomes
Values are presented as number or number (%).
Table 3. Treatment outcomes according to each characteristic
Values are presented as number (%).

