
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 51(1); 2026 > Article
- Research Article Determination of optimal horizontal beam angulations for canal separation in mandibular molars using cone-beam computed tomography: a retrospective image-based analysis
-
Benedikt Schneider1
 , Tamina Tepe2, Daniel Rapp2, Wilhelm Frank3, Maria Lessani4, Constantin von See5, Sebastian Fitzek6, Jörg Philipp Tchorz2,*
, Tamina Tepe2, Daniel Rapp2, Wilhelm Frank3, Maria Lessani4, Constantin von See5, Sebastian Fitzek6, Jörg Philipp Tchorz2,* -
Restor Dent Endod 2026;51(1):e9.
DOI: https://doi.org/10.5395/rde.2026.51.e9
Published online: February 26, 2026
1Center for Oral and Maxillofacial Surgery, Department of Dentistry, Faculty of Medicine and Dentistry, Danube Private University, Krems, Austria
2Division for Endodontics, Center for Operative Dentistry and Periodontology, Department of Dentistry, Faculty of Medicine and Dentistry, Danube Private University, Krems, Austria
3Department of Health System Research, Faculty of Medicine and Dentistry, Danube Private University, Krems, Austria
4Endoclinic, Practice limited to Endodontics, North London, UK
5Research Center for Digital Technologies in Dentistry and CAD/CAM, Department of Dentistry, Faculty of Medicine and Dentistry, Danube Private University, Krems, Austria
6Medical Image Analysis & Artificial Intelligence (MIAAI) Group, Faculty of Medicine and Dentistry, Danube Private University, Krems, Austria
- *Correspondence to Jörg Philipp Tchorz, Priv. Doz. Dr. med. Dent Division for Endodontics, Center for Operative Dentistry and Periodontology, Department of Dentistry, Faculty of Medicine and Dentistry, Danube Private University, Steiner Landstraße 124, A-3500 Krems-Stein, Austria Email: joerg.tchorz@dp-uni.ac.at
• Received: September 18, 2025 • Revised: November 23, 2025 • Accepted: December 15, 2025
© 2026 The Korean Academy of Conservative Dentistry
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,338 Views
- 34 Download
Abstract
-
Objectives Two-dimensional intraoral radiographs often obscure canals due to superimposition, especially in mandibular molars with complex anatomy. This cone-beam computed tomography (CBCT) study identified the horizontal beam angles at which first and second molar canals overlap and derived clinically applicable angulations for enhanced canal separation.
-
Methods Eighty-five CBCT datasets from 100 patients met the inclusion criteria, yielding 318 mandibular molars (160 first, 158 second). Using ImageJ, absolute horizontal overlap angles (α) were measured to determine the corresponding theoretical separation angles defined as δ* = 90° – α. Separability was modeled across horizontal beam angulation increments from −45° to +45° in five steps, and Wilson’s 95% confidence intervals were computed. Group comparisons used the Mann-Whitney U and independent t-tests (p ≤ 0.05)
-
Results Minimal mesial beam angulations for effective canal separability (δ* = 90° − α) ranged from approximately 7° to 15° for mesial roots and approximately 10° to 13° for distal roots. No significant mesial differences were observed between first and second molars (p > 0.30). Distal roots of second molars exhibited significantly higher angulations (p = 0.003 coronal, p < 0.001 apical). Mesial canals achieved ≥95% separability at approximately 25° and ≥99% at approximately 35°; distal canals required approximately 30° and approximately 40°.
-
Conclusions A mesial beam angulation of 30° to 35° provides probable canal differentiation in mandibular molars, separating mesial canals in ≥99% and distal canals in ≥95% of cases. This range refines previous recommendations and supports the as low as reasonably achievable (ALARA) principle.
INTRODUCTION
The success of endodontic treatment is primarily dependent on the highest standard of chemo-mechanical preparation of the complex root canal system [1]. Untreated canals can harbor microorganisms and potentially perpetuate periapical inflammation, ultimately leading to treatment failure [2–4].
Mandibular molars exhibit highly variable and complex canal anatomy, frequently featuring multiple canals within the mesial and distal roots. Canal configurations may vary from separate canals that remain distinct to canals that merge and diverge along their course. Additionally, mandibular molars can exhibit uncommon anatomical variations, such as a third canal in the mesial root (the middle mesial canal). These complexities significantly complicate accurate endodontic diagnosis and treatment planning for both mandibular first and second molars [5,6]. Specifically, configurations involving mesiobuccal (MB), mesiolingual (ML), and possibly middle mesial canals in the mesial root, as well as distobuccal (DB) and distolingual (DL) canals in the distal root, represent considerable diagnostic challenges [2]. An important aspect influencing diagnostic accuracy is whether canals remain separate throughout the root or converge apically. Confluent canal systems may present radiographically as a single structure, whereas separate canals, particularly in buccolingual orientation, often overlap in two-dimensional (2D) projections. Thus, understanding the canal trajectory is essential to interpret radiographs accurately and avoid misdiagnosis or missed canals. The 2D intraoral radiographs remain an essential tool in the endodontic diagnosis and provision of the treatment, guiding the operator from pre‐operative canal identification to intra‐operative working‐length verification and postoperative obturation assessment [3,7]. Despite their accessibility, low radiation dose, and cost-effectiveness, 2D images inherently suffer from geometric distortion and superimposition of anatomical structures [8–11]. Therefore, due to the limitations of orthoradial views, root canals frequently overlap, causing difficulty in distinguishing individual canals, leading to repeated exposures to obtain diagnostically acceptable results. It has been reported that retake rates among clinicians and students range from 11% to 20%, predominantly resulting from such anatomical superimpositions [12,13]. The principles of parallax aid the operator and disentangle superimposed structures. Thus, practitioners apply the SLOB (same lingual, opposite buccal) rule, which uses horizontal beam angulations to infer the spatial relationships of overlapping canals [14].
However, existing literature provides inconsistent recommendations regarding optimal mesial beam angulations, ranging from 20° to 30° [2,14–16]. Haghani et al. [2] specifically found a 20° mesial beam angulation to be significantly more effective than other offsets for separating all four canals in mandibular first molars. Puapichartdumrong et al. [15] introduced an angle-adjustable film holder to refine horizontal tube angulations but focused primarily on mechanical implementation rather than on tooth-specific angulations. Setzer and Lee [16] underscored the benefits of three-dimensional (3D) imaging for canal trajectory mapping but did not translate these trajectories into actionable 2D horizontal beam angulations.
Despite these valuable insights, to date, no comprehensive investigation has systematically defined the optimal eccentric angles for both first and second mandibular molars to visualize all roots and canals on a single periapical image.
To address this gap, the present study retrospectively analyses cone-beam computed tomography (CBCT) datasets of mandibular first and second molars to determine the horizontal beam angulations at which root canals in one single root overlap, both coronally and apically, to determine the minimal beam angulation at which differentiation between anatomical structures becomes radiographically discernible. By integrating 3D canal mapping with simulated 2D projections, we aim to establish an evidence-based approach for horizontal beam angulations to enhance diagnostic precision, minimize retakes, and ultimately reduce patient radiation exposure for endodontic procedures.
METHODS
A retrospective evaluation was conducted using CBCT datasets from 100 individuals, randomly selected from the university’s imaging archives. To minimize selection bias, a random-number generator was used to select 100 datasets from a full list of pseudonymized case identifiers, which were then randomly selected for analysis. All scans were acquired with a Dentsply Sirona Orthophos SL 3D system (Dentsply Sirona, Bensheim, Germany), with unit tube voltage of 60–90 kVp and tube current of 3–16 mA. Featured fields of view were either 8 × 8 cm or 11 × 10 cm, captured in either standard or high-definition modes. These images were originally obtained for various clinical indications, including implant planning, impacted third‐molar extractions, orthodontic assessments, or other diagnostic requirements, and not specifically for this investigation; therefore, no additional radiation exposure was incurred. To meet the inclusion criteria, scans had to be free from notable artifacts or recording errors and demonstrate good to excellent image quality. A cohort size of 100 CBCT volumes was chosen to align with prior research on radiographic beam angulations and canal visualization [15,17,18].
All datasets were de‐identified in accordance with regional data‐protection legislation to safeguard patient anonymity. Written informed consent was obtained from all participants. Ethical approval for this study protocol was granted by the Institutional Ethics Committee (DPU‐EK/038).
Each CBCT’s DICOM files were imported into SIDEXIS version 4.3 (Dentsply Sirona). Patient head orientation was standardized by correcting tilt and rotation: coronal, sagittal, and axial slices were realigned parallel to the transverse and horizontal reference planes by manipulating control points, following the protocol of Schneider et al. [19]. Next, multiplanar reconstructions were scrolled to locate axial views that displayed the entire canal anatomy of the target teeth. Coronal (c) and apical (a) reference images were acquired at standardized levels: immediately apical to the pulpal floor, and at the most apical axial level, maintaining distinguishable root contours. Coronal and apical axial slices were evaluated separately for mesial (MB–ML) and distal (DB–DL) canal pairs to maintain consistency across root levels.
All measurements were performed by a single investigator using the open-source software ImageJ (version 1.54f, open-source; National Institutes of Health, Bethesda, MD, USA), utilizing the central axis as a standardized reference point (Figure 1). The angle at which the individual root canals located buccally would overlap with the lingual root canal was measured for each tooth, starting from the central axis of the jaw. In roots presenting a single oval-shaped canal, the angle was measured along the axis of this anatomical structure. The aim of the study was to investigate the possible superimposition in 2D intraoral radiographs, which are normally taken parallel to the jaw and not placed centrically; therefore, the angle between the jaw and the central axis was additionally measured, and the respective angles were calculated accordingly.
The continuous variables have been summarized using means and standard deviations, and the Kolmogorov–Smirnov test assessed the assumption of normality. While depending on the distribution, intergroup comparisons were made using either the independent-samples t-test or the Mann-Whitney U test, with statistical significance defined as p ≤ 0.05. To evaluate canal overlap patterns across mandibular first and second molars, descriptive statistics of the CBCT-measured overlap angles (α) were calculated separately for mesial (MB–ML) and distal (DB–DL) canal pairs at coronal and apical levels. Subsequently, we defined the theoretical beam angulation for separation as δ* = 90° − α, where α is the CBCT-measured angle at which the mesial or distal canal pair projects as a single 2D structure (overlap). For any candidate beam angulation δ, theoretical separability occurs when δ ≥ δ*. A canal pair is considered radiographically separable once the applied beam angle exceeds the tooth-specific minimal separation threshold. Accordingly, δ represents the minimal beam angulation required to obtain a separate depiction on a 2D image. We computed theoretical separability across predefined beam angulation cutoffs from −45° to +45° in 5° increments, with Wilson 95% confidence intervals, separately for coronal and apical levels and for mesial (MB–ML) and distal (DB–DL) canal pairs. Positive δ values represent mesial angulations and negative values represent distal angulations. Reporting focuses on the clinically relevant mesial angulations. To derive additional thresholds, we additionally identified the smallest predefined δ-cutoff at which a given separability level (≥95% or ≥99%) was first reached.
Diagnostic metrics such as sensitivity, specificity, or receiver operating characteristic (ROC)/area under the curve were not calculated, as no independent 2D radiographic gold standard was available for validation. Instead, the coverage function provides an equivalent probabilistic estimate of separability based on CBCT ground-truth geometry. All statistical analyses were performed in Python version 3.11.13 (Python Software Foundation, Wilmington, DE, USA) using the pandas and NumPy libraries.
RESULTS
Of the 100 CBCT scans initially screened, 85 datasets (59.8 % female, 39.6 % male) met the inclusion criteria. CBCTs were excluded mainly due to incomplete visualization of the mandibular molar region or because the molars did not appear in full within the volume. Final measurements were performed on 318 mandibular molars: 160 on the left side (77 first and 83 second molars) and 158 teeth from the right side (75 first and 83 second molars).
Descriptive statistics for horizontal beam angles at which root canal overlap occurred have been presented (Table 1). At the coronal level, the mean angle ± standard deviation for radiographic overlap of canals within the mesial roots was α = 83.74° ± 10.63°, while the corresponding angle for the distal roots was α = 79.60° ± 11.63°. At the apical level, canal overlap in the mesial roots was achieved at a mean angle of α = 82.92° ± 10.88°, and in the distal roots at α = 78.72° ± 11.92° (Figure 2). According to δ* = 90 − α, overlap values of approximately 75° to 83° translate into theoretical separation thresholds of roughly 7° to 15°. When comparing tooth types, mesial angles of canal overlap did not differ significantly between first and second mandibular molars (p > 0.3). In contrast, distal canal overlap angles were significantly higher in second molars, particularly at the coronal level (p < 0.001), reflecting increased curvature and divergence characteristics (Table 2). No significant gender-related differences were detected across any strata (all p ≥ 0.25). To extend the overlap-based interpretation, separability was additionally evaluated across a predefined horizontal beam angulation grid from −45° to +45° in 5° increments. The proportion of separable canal pairs increased progressively with δ. At δ = 20°, approximately 90% of mesial and 85% of distal pairs were separable. For mesial canals, ≥95% separability was reached at approximately 25°, and ≥99% was achieved within the 30° to 35° interval of the 5° increment grid. Distal canals required approximately 30° for ≥95% and approximately 40° for ≥99% separability. Wilson 95% confidence intervals narrowed markedly between 25° and 35°, indicating high statistical stability in this range (Tables 3 and 4). Distal roots, particularly in second molars, benefited from slightly larger mesial angulations (approximately 35°–40°), achieving near-complete separation (Figure 3).
DISCUSSION
The provision of root canal treatment relies on radiographs (2D) and, in line with as low as reasonably achievable (ALARA) principles, operators are obliged to minimize radiation for patients while providing the highest standard of care. Many previous studies have used a trial-and-error approach with predefined horizontal beam angulations, often in ex vivo settings with extracted teeth, limiting clinical transferability due to artificial tooth alignment [2,17,20-22]. In contrast, in vivo data, such as that presented by Bardauil et al. [23], offer greater anatomical relevance. For this reason, the present study used a retrospective design based on existing CBCT data. This approach allowed for detailed, reproducible simulation of horizontal beam angulations and identification of precise angles at which root canal superimposition occurs, all while preserving the three-dimensional anatomical relationships of the mandibular arch. However, it must be acknowledged that CBCT imaging, while valuable for anatomical analysis, does not fully reproduce intraoral conditions such as sensor placement difficulty, variation in manufacturers’ production of film holders or aiming devices, patient movement, or anatomical space limitations.
Unlike studies that focus on root outlines or apex positioning, our analysis focused on the radiographic separation of root canal spaces, which is of greater relevance in endodontics, particularly during working length determination and obturation assessment. As the apical foramen may not coincide with the anatomical apex [24,25], the ability to visualize root canals clearly at both the apical and coronal levels becomes a clinically significant objective. Accordingly, we measured superimposition at both apical and coronal levels using the center lines of the canals as radiographic targets to conclude at which beam angulations separation would be possible.
Across all mandibular molars examined, canal overlap persisted until projection angles corresponding to minimal mesial beam angulations of approximately 7° to 15°, reflecting the earliest theoretical onset of canal separability (δ* = 90° − α). Distal canal systems required slightly larger minimal mesial angulations, with second molars showing the highest thresholds due to their greater root divergence. Specifically, second molars exhibited δ* values around 9°–13°, whereas first molars showed slightly lower minimal separability thresholds of 7° to 12° (p < 0.001), suggesting greater root divergence or curvature in second molars. These findings reinforce previously reported anatomical differences between mandibular molars [26] and highlight the need for tailored radiographic strategies depending on molar type and root group. They also indicate that canal overlap may persist even with minor deviations from the orthoradial angle, and a slightly greater mesial beam angulation is needed to achieve total radiographic separation.
However, theoretical coverage analysis further quantified this relationship, revealing that mesial canals achieved ≥95% separability at δ approximately 25° and ≥99% at approximately 35°. Distal canal pairs required δ approximately 30° to reach 95% and approximately 40° to reach 99%, reflecting the flatter divergence trajectory of distal roots. Confidence intervals narrowed substantially between 25° and 35°, confirming statistical stability of the coverage plateau. These findings identify a narrow mesial beam angulation window in which most mesial and distal canals can be visualized simultaneously.
From a clinical perspective, this mesial beam angulation range of approximately 30° to 35° provides the highest probability of complete canal differentiation with one exposure. Notably, distal beam angulations were not considered clinically meaningful, as our coverage analysis demonstrated consistently low separability across all negative δ-increments (distal shifts), with values remaining far below diagnostic thresholds and therefore offering no practical radiographic advantage.
Anatomical variations further refine this recommendation. No significant differences were observed between first and second molars for mesial canal overlap (p > 0.3), whereas distal roots of second molars showed significantly higher overlap angles (p = 0.003 coronal, p < 0.001 apical), consistent with their greater curvature and divergence. Accordingly, for first molars, a mesial beam angulation of approximately 30° is sufficient to capture both canal pairs, while second molars benefit from a slightly higher angulation of approximately 35°, which compensates for their increased distal overlap.
Within this range, mesial canals are resolved in approximately 99% and distal canals in approximately 95% of cases. Thus, selecting a single exposure within this window avoids repeated imaging, in line with the ALARA principle [3,7].
If distal canal separation remains inadequate, further increase up to approximately 40° may be considered on a case-by-case basis. Coronal overlap angles were consistently higher than apical ones, confirming the increasing canal divergence toward the root apex [26]. Consequently, apical clarity should be prioritized during working length determination and obturation control. The significantly higher distal overlap in second molars supports anatomical evidence of greater root curvature and divergence in this group [26].
The coverage-based approach introduced in this study provides a continuous, quantitative analogue to conventional diagnostic performance metrics. Although sensitivity, specificity, and ROC analysis could not be computed in the absence of an independent 2D gold standard, the coverage function represents an equivalent probabilistic measure of radiographic separability derived from CBCT ground-truth geometry. Thus, it enables precise estimation of the probability of achieving canal differentiation at any given beam angle and bridges three-dimensional anatomy with 2D radiographic optimization.
It was decided to measure the distal root if there were two canals present, but through the canal cross-section if there was only one root canal. This has the advantage that the angles obtained in our study can also be used to confirm or rule out the presence of a single canal in the distal root. To do this clinically, it is important to check whether the visible canal, instrument, or gutta-percha is centrally located within the root contour when viewing a 2D X-ray. In case CBCT data is already available, the opportunity to use multiplanar reconstructions for the simulation of tube angulation should be taken. This helps to approximate individualized projection angles for intraoral radiography and improve the diagnostic yield of initial exposures. Ultimately, these findings may aid operators, both clinicians and students, by offering clinically applicable reference values for beam angulations, enhancing the quality of periapical imaging in mandibular molars. Further in vivo studies are warranted to validate these parameters under real-world clinical conditions and to investigate tools that could assist clinicians in achieving optimal X-ray projection geometry.
Limitations of the present study include its retrospective design and the exclusive use of CBCT data. Therefore, intraoral sensor placement or patient-specific positioning constraints could not be considered. Accordingly, no direct comparison with corresponding 2D periapical radiographs was possible. Consequently, sensitivity and specificity could not be computed in a statistically valid manner, as this would require an independent test image and dichotomous outcome classification. Deriving both the “true” and “test” conditions from the same CBCT dataset would have resulted in circular inference. Instead, the study employed a theoretical coverage approach, in which the proportion of teeth achieving canal separation at different predefined beam angles was determined. This method offers an equivalent functional interpretation of diagnostic performance across beam angulations while maintaining methodological validity. Future prospective studies combining CBCT and standardized intraoral radiographs are encouraged to validate these theoretical coverage parameters under clinical conditions.
It should also be noted that all angular measurements were performed by a single examiner, and no formal intra-observer reliability testing was undertaken. However, the measurement protocol was based on clearly defined anatomical reference points and geometric centerlines, minimizing subjective interpretation. Future studies should nonetheless include repeated measurements by multiple blinded observers to validate inter- and intra-observer consistency statistically.
Furthermore, our analysis was limited to radiographic axes where root canals appeared to overlap, independent of the actual number of canals, as multiple canals are usually situated parallel to one another within the root’s center. To distinguish between a single and multiple canals clinically, a second X-ray taken at a greater horizontal angle is required. This reveals whether the canal, an inserted file, or gutta-percha is centered within the root’s outline. A noncentral position strongly suggests an additional canal. The behavior of these axes across different root canal morphologies was not investigated and represents a potential avenue for future research.
Nonetheless, the large sample size and the narrow confidence intervals across strata support the robustness of the proposed angulation thresholds. However, the individual anatomical variation, assessed via preexisting periapical radiographs or available CBCT scans, should guide final angulation choices. Application of these parameters will respect ALARA principles, may reduce the need for retakes, lower radiation exposure, and improve radiographic diagnostic quality during endodontic treatment of mandibular molars.
CONCLUSIONS
The CBCT-based analysis provided a practical approach for selecting horizontal beam angulations in intraoral radiography of mandibular molars. Based on CBCT-derived overlap geometry, the earliest theoretical onset of canal separability occurs at small mesial beam angulations of approximately 7° to 15°. This minimal range reflects the lowest angular deviation at which the first radiographic divergence of canal systems becomes detectable.
Reliable canal separability (≥95% to 99%) was achieved only at larger mesial beam angulations. First mandibular molars reached consistent separability at approximately 30°, whereas second molars benefited from slightly higher angulations of 35°. If distal canal separation remains insufficient, increasing the beam angulation toward 40° may be considered. Together, these findings identify a practical single-exposure window of 30°–35°, which provides the highest probability of complete canal differentiation while minimizing the need for repeated radiographic exposures under ALARA principles.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING/SUPPORT
The authors have no financial relationships relevant to this article to disclose.
-
AUTHOR CONTRIBUTIONS
Conceptualization, Resources, Methodology, Project administration: Schneider B, Tchorz JP. Data curation: Frank W, Fitzek S. Formal analysis: Schneider B, Tchorz JP, Frank W. Investigation, Software: Tepe T, Rapp D. Supervision: Tchorz JP, Schneider B, von See C. Validation: Lessani M, von See C, Frank W. Visualization: Frank W, Fitzek S, Lessani M. Writing - original draft: Schneider B, Tchorz JP, Tepe T, Rapp D. Writing - review & editing: Lessani M, Frank W, von See C, Schneider B, Fitzek S, Tchorz JP. All authors have read and agreed to the published version of the manuscript.
-
DATA SHARING STATEMENT
The datasets are not publicly available but are available from the corresponding author upon reasonable request.
Figure 1.
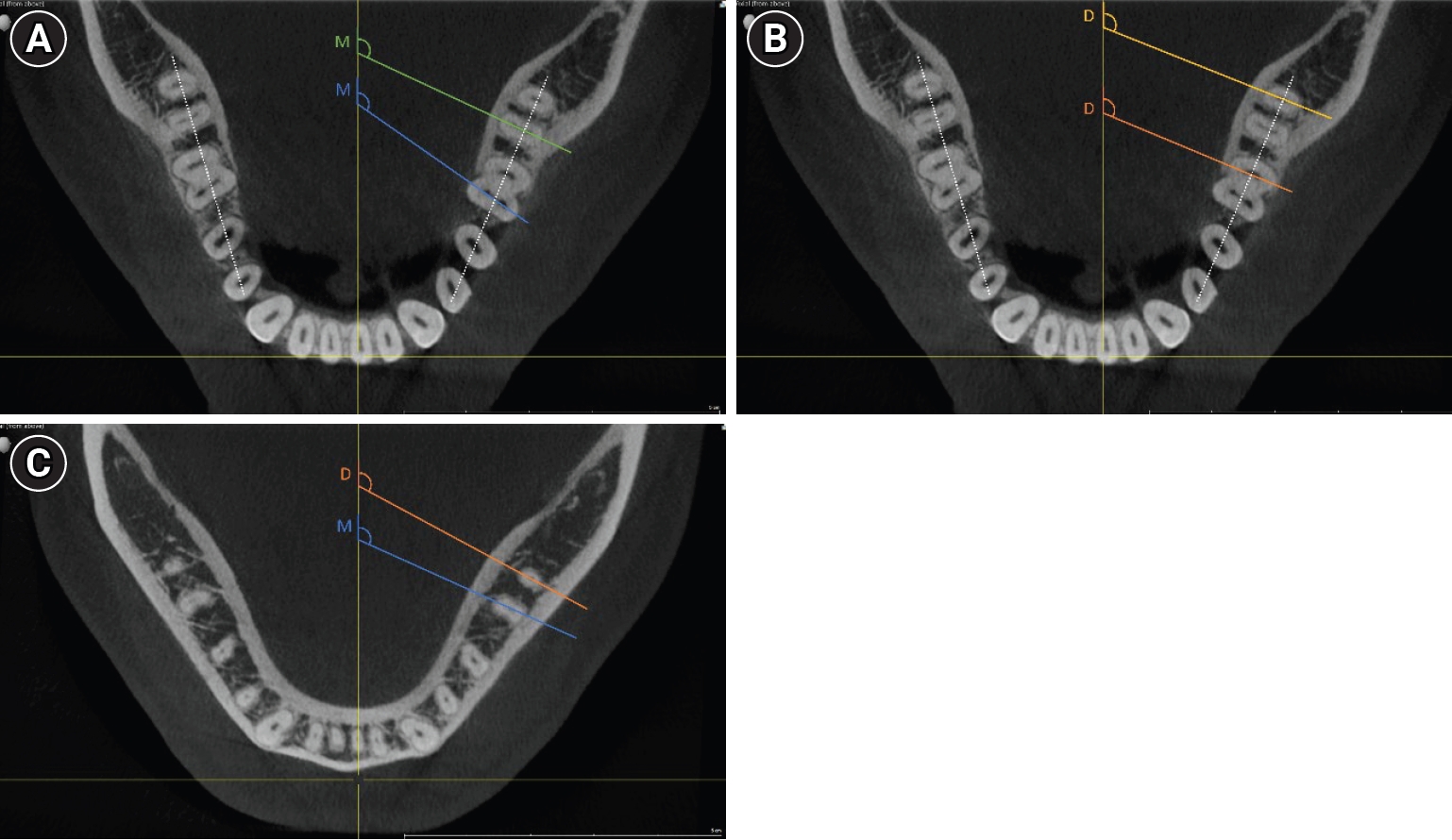
Examples of the cone-beam computed tomography measurements. Examples of measurements indicative of the angles at which root canals overlap. The measurement lines are colored for better visibility showing either mesial (M) or distal (D) canal pair measurements. In roots presenting a single oval-shaped canal, the angle was measured along the axis of this anatomical structure. The dotted line represents the mandibular arch, and the angle between this reference and the X-ray central axis was also measured for final angle calculations. (A) Mesial canal pairs (mesiobuccal–mesiolingual), coronal level. (B) Distal canal pairs (distobuccal–distolingual), coronal level. (C) Mesial and distal measurements, apical level.
Figure 2.
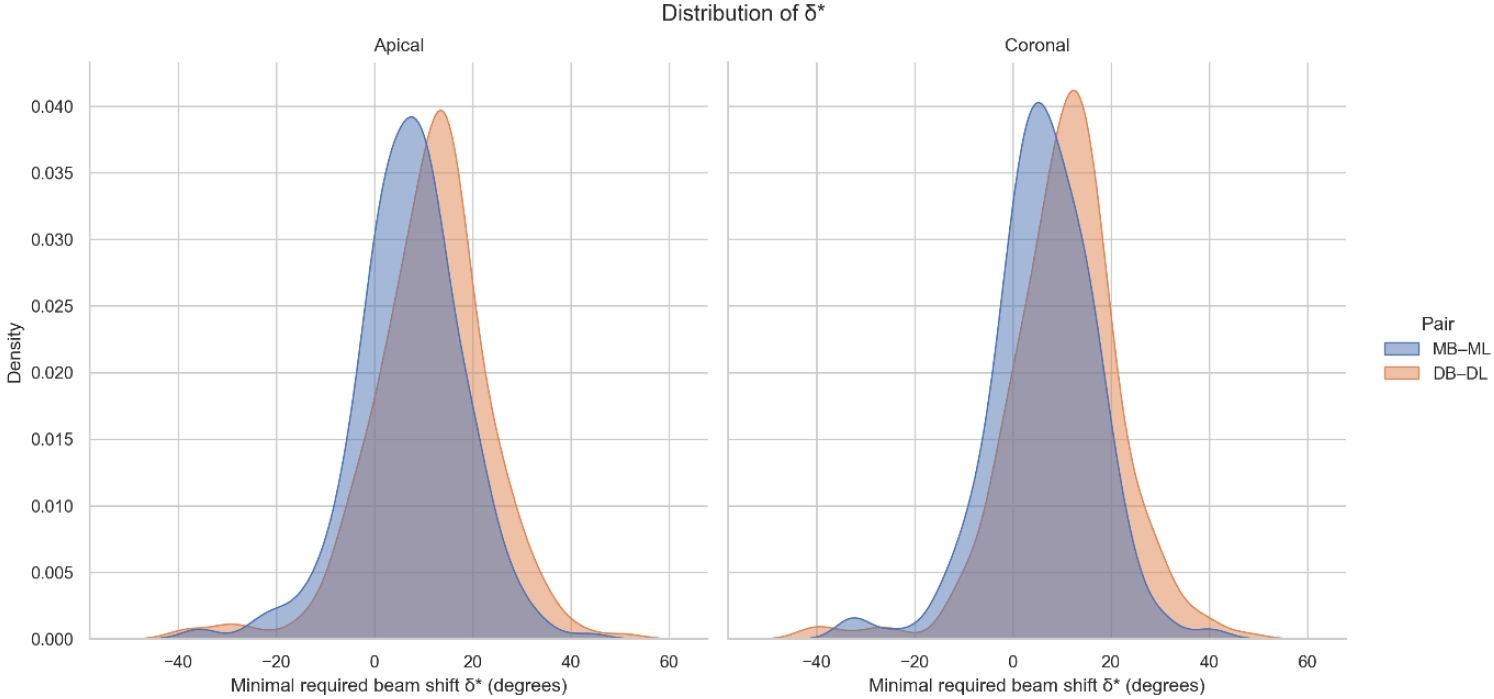
Distribution of δ values by canal pair and root level. Smoothed density distributions of the theoretical minimal horizontal beam angulation δ required to achieve radiographic separation of root canal pairs. Mesial (mesiobuccal–mesiolingual) and distal (distobuccal–distolingual) canal pairs are shown separately for the apical (left) and coronal (right) measurement levels. Distal canal pairs exhibit a right-shifted distribution, particularly at the coronal level, reflecting their generally higher beam angulation requirements compared with mesial canals.
Figure 3.
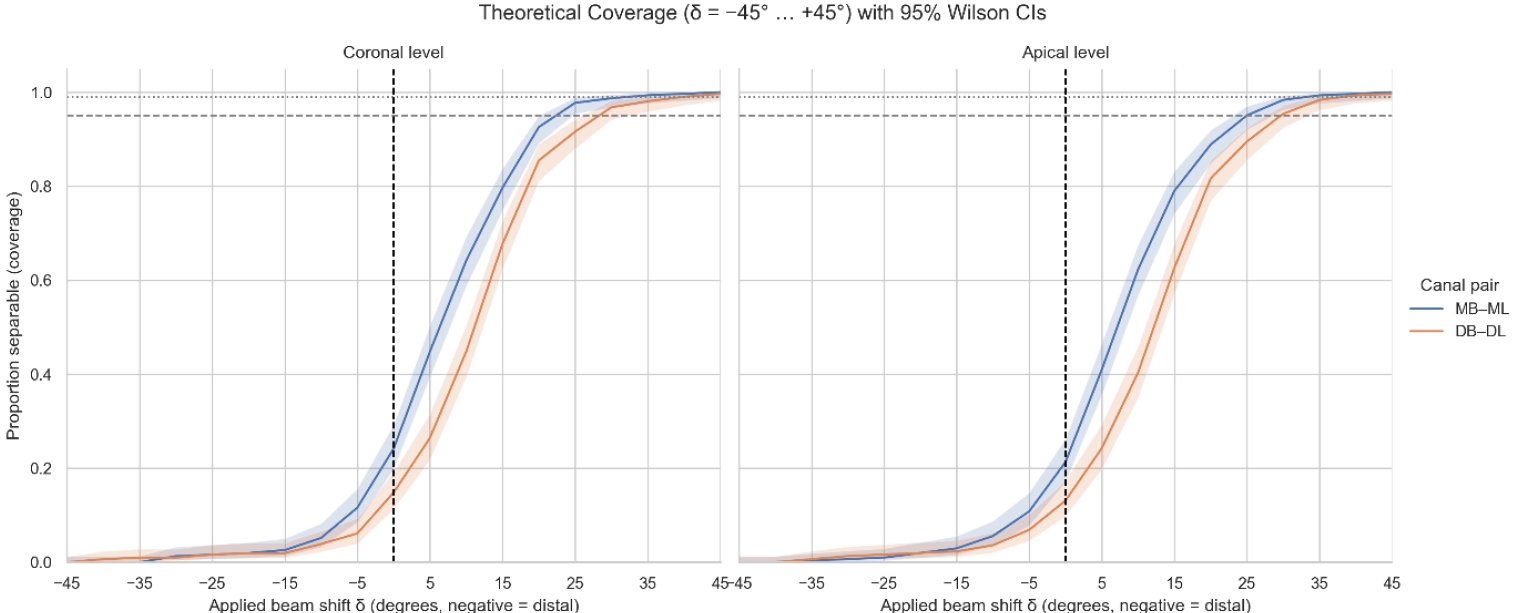
Theoretical coverage (δ = −45° to +45°) with 95% Wilson confidence intervals. Theoretical separability (coverage) of mesial (MB–ML) and distal (DB–DL) canal pairs plotted across the full range of applied horizontal beam angulations (δ = −45° to +45°). Curves represent the proportion of canal pairs predicted to be radiographically separable at each δ value, with shaded bands indicating 95% Wilson confidence intervals. Positive δ values correspond to mesial beam angulations; negative δ values represent distal angulations. Mesial canals (MB–ML) reach ≥95% separability between approximately 22° and 25°, and ≥99% at around 32°. Distal canals (DB–DL) require larger angulations, achieving ≥95% at approximately 30° and ≥99% at approximately 40°. The steep rise and subsequent plateau between approximately 25° and approximately 35° indicate the clinically relevant window in which most canal pairs become reliably distinguishable on a single periapical radiograph. MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual.
Table 1.
Mean overlap angles (α) by root level and canal pair
| Position | Canal pair | N | Mean ± SD (°) |
|---|---|---|---|
| Coronal | MB–ML (mesial) | 310 | 83.74 ± 10.63 |
| Coronal | DB–DL (distal) | 310 | 79.60 ± 11.63 |
| Apical | MB–ML | 305 | 82.92 ± 10.88 |
| Apical | DB–DL | 305 | 78.72 ± 11.92 |
Values are presented separately for mesial (MB–ML) and distal (DB–DL) canal pairs at coronal and apical levels. Angles (α, in degrees [°]) were measured from CBCT-derived canal centerlines within each root, representing the projection at which canal outlines fully overlap in two-dimensional radiographs. SD, standard deviation; MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual; CBCT, cone-beam computed tomography.
Table 2.
Comparison of first and second mandibular molars (Welch t-tests for α)
| Position | Canal pair | t (df) | p-value | Interpretation |
|---|---|---|---|---|
| Coronal | MB–ML | −0.65 (305.1) | 0.518 | NS (no difference) |
| Coronal | DB–DL | −2.96 (302.9) | 0.0033* | Second molars > first molars |
| Apical | MB–ML | 0.94 (302.7) | 0.347 | NS |
| Apical | DB–DL | −4.45 (302.7) | 1.2 × 10⁻⁵* | Second molars > first molars |
Reported are test statistics, degrees of freedom (df), and two-sided p-values for mesial (MB–ML) and distal (DB–DL) canal pairs at coronal and apical levels.
Positive values denote higher overlap angles in second molars, consistent with increased distal root curvature.
MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual; NS, not significant.
*p < 0.05, statistically significant differences.
Table 3.
Theoretical beam angle thresholds (δ) for ≥95% and ≥99% canal separability
| Position | Canal pair | δ for ≥95% (°) | δ for ≥99% (°) |
|---|---|---|---|
| Coronal | MB–ML | 22 | 32 |
| Coronal | DB–DL | 30 | 40 |
| Apical | MB–ML | 25 | 32 |
| Apical | DB–DL | 30 | 40 |
Theoretical beam angulations were derived from δ* = 90° − α; thresholds represent the smallest δ at which coverage ≥95% or ≥99% was achieved. Values represent the minimal mesial horizontal angulations at which the corresponding proportion of canal pairs can be radiographically distinguished.
MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual.
Table 4.
Wilson 95% CIs for theoretical coverage (proportion of separable canals)
Values are presented as percentage (95% confidence interval).
Coverage represents the proportion of canals achieving theoretical separability (δ* ≤ δ) at each predefined mesial beam angulation (δ). Confidence intervals narrow progressively between 25° and 35° indicating statistical stability of the separability plateau. Data were computed for coronal levels using the Wilson method for binomial proportions.
CIs, confidence intervals; MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual.
- 1. Gulabivala K, Ng YL. Factors that affect the outcomes of root canal treatment and retreatment: a reframing of the principles. Int Endod J 2023;56 Suppl 2:82-115.ArticlePubMedPDF
- 2. Haghani J, Raoof M, Pourahmadi S. Ex-vivo evaluation of x-ray horizontal angle for separating the canals of four-canal first mandibular molars. Iran Endod J 2008;2:143-146.PubMedPMC
- 3. Kazzi D, Horner K, Qualtrough AC, Martinez-Beneyto Y, Rushton VE. A comparative study of three periapical radiographic techniques for endodontic working length estimation. Int Endod J 2007;40:526-531.ArticlePubMed
- 4. Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J 2006;39:249-281.ArticlePubMed
- 5. Gomez F, Brea G, Gomez-Sosa JF. Root canal morphology and variations in mandibular second molars: an in vivo cone-beam computed tomography analysis. BMC Oral Health 2021;21:424.ArticlePubMedPMCPDF
- 6. Ordinola-Zapata R, Bramante CM, Versiani MA, Moldauer BI, Topham G, Gutmann JL, et al. Comparative accuracy of the Clearing Technique, CBCT and Micro-CT methods in studying the mesial root canal configuration of mandibular first molars. Int Endod J 2017;50:90-96.ArticlePubMed
- 7. Fava LR, Dummer PM. Periapical radiographic techniques during endodontic diagnosis and treatment. Int Endod J 1997;30:250-261.ArticlePubMed
- 8. Eliasson S, Lavstedt S, Wouters F, Ostlin L. Quality of intraoral radiographs sent by private dental practitioners for therapy evaluation by the Social Insurance Office. Swed Dent J 1990;14:81-89.PubMed
- 9. Patel JR. Intraoral radiographic errors. Oral Surg Oral Med Oral Pathol 1979;48:479-483.ArticlePubMed
- 10. Javed MQ, Kolarkodi SH, Riaz A, Nawabi S. Quality assurance audit of digital intraoral periapical radiographs at the undergraduate dental clinics. J Coll Physicians Surg Pak 2020;30:1339-1342.ArticlePubMed
- 11. Siddique SN, Anwar MA, Zaman H, Haider I, Ahmad A, Umair M, et al. Quality assessment of periapical radiographs taken by dental assistants using the recent Faculty of General Dental Practice (FGDP) guidelines. Cureus 2024;16:e68508.ArticlePubMedPMC
- 12. Senior A, Winand C, Ganatra S, Lai H, Alsulfyani N, Pachêco-Pereira C. Digital intraoral imaging re-exposure rates of dental students. J Dent Educ 2018;82:61-68.ArticlePubMedPDF
- 13. Almutairi N, Alharbi A. Difficulties faced by undergraduates while conducting endodontic therapy. Cureus 2024;16:e52217.ArticlePubMedPMC
- 14. Abella F, Patel S, Durán-Sindreu F, Mercadé M, Roig M. Mandibular first molars with disto-lingual roots: review and clinical management. Int Endod J 2012;45:963-978.ArticlePubMed
- 15. Puapichartdumrong P, Eakpunyakul N, Tanpumiprathet S, Khueankaew P, Saelim P, Piyapattamin T. Efficacy of a newly designed angulation-adjustable film holder for reducing cone-cutting errors and saving time in horizontal tube-shift technique by dental students. Heliyon 2022;8:e11567.ArticlePubMedPMC
- 16. Setzer FC, Lee SM. Radiology in endodontics. Dent Clin North Am 2021;65:475-486.ArticlePubMed
- 17. Karnasuta P, Vajrabhaya LO, Chongkonsatit W, Chavanaves C, Panrenu N. An efficacious horizontal angulation separated radiographically superimposed canals in upper premolars with different root morphologies. Heliyon 2020;6:e04294.ArticlePubMedPMC
- 18. Hishikawa T, Izumi M, Naitoh M, Furukawa M, Yoshinari N, Kawase H, et al. The effect of horizontal X-ray beam angulation on the detection of furcation defects of mandibular first molars in intraoral radiography. Dentomaxillofac Radiol 2010;39:85-90.ArticlePubMedPMC
- 19. Schneider B, Klinkhamels L, Frank W, von See C, Tchorz JP. Evaluation of the ideal horizontal X-ray beam angulation to accurately identify two separate canals in maxillary first premolars: a retrospective clinical study using cone-beam computed tomography in an Austrian subpopulation. Dent J (Basel) 2025;13:151.ArticlePubMedPMC
- 20. Martínez-Lozano MA, Forner-Navarro L, Sánchez-Cortés JL. Analysis of radiologic factors in determining premolar root canal systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88:719-722.ArticlePubMed
- 21. Naoum HJ, Love RM, Chandler NP, Herbison P. Effect of X-ray beam angulation and intraradicular contrast medium on radiographic interpretation of lower first molar root canal anatomy. Int Endod J 2003;36:12-19.ArticlePubMedPDF
- 22. Wang Q, Yu G, Zhou XD, Peters OA, Zheng QH, Huang DM. Evaluation of X-ray projection angulation for successful radix entomolaris diagnosis in mandibular first molars in vitro. J Endod 2011;37:1063-1068.ArticlePubMed
- 23. Bardauil MR, Moura Netto Cd, Moura AA. Evaluation of the maxillary premolar roots dissociation using radiographic holders with conventional and digital radiography. Braz Oral Res 2010;24:284-289.ArticlePubMed
- 24. Martos J, Ferrer-Luque CM, González-Rodríguez MP, Castro LA. Topographical evaluation of the major apical foramen in permanent human teeth. Int Endod J 2009;42:329-334.ArticlePubMed
- 25. Martos J, Lubian C, Silveira LF, Suita de Castro LA, Ferrer Luque CM. Morphologic analysis of the root apex in human teeth. J Endod 2010;36:664-667.ArticlePubMed
- 26. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589-599.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteDetermination of optimal horizontal beam angulations for canal separation in mandibular molars using cone-beam computed tomography: a retrospective image-based analysis
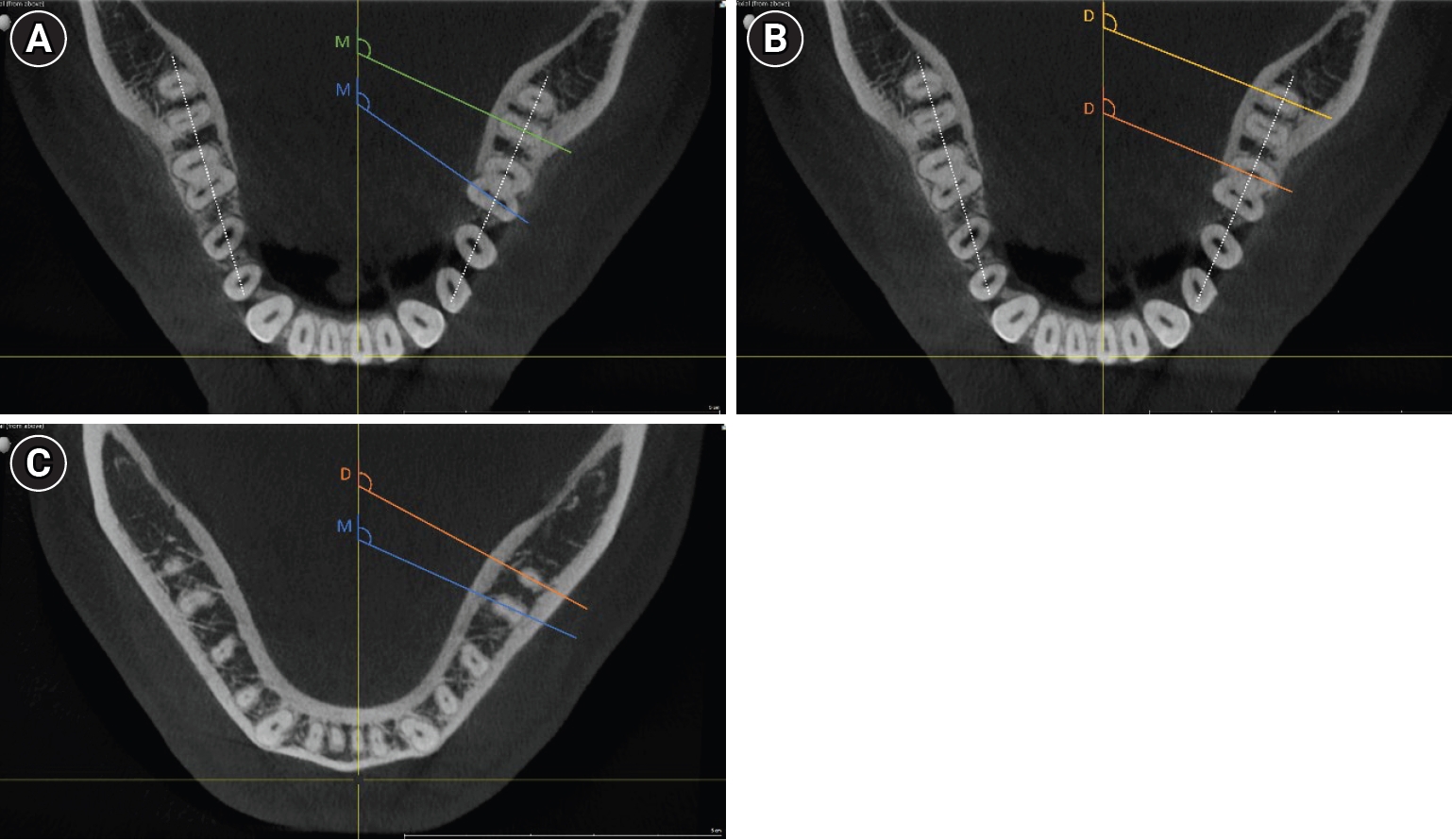
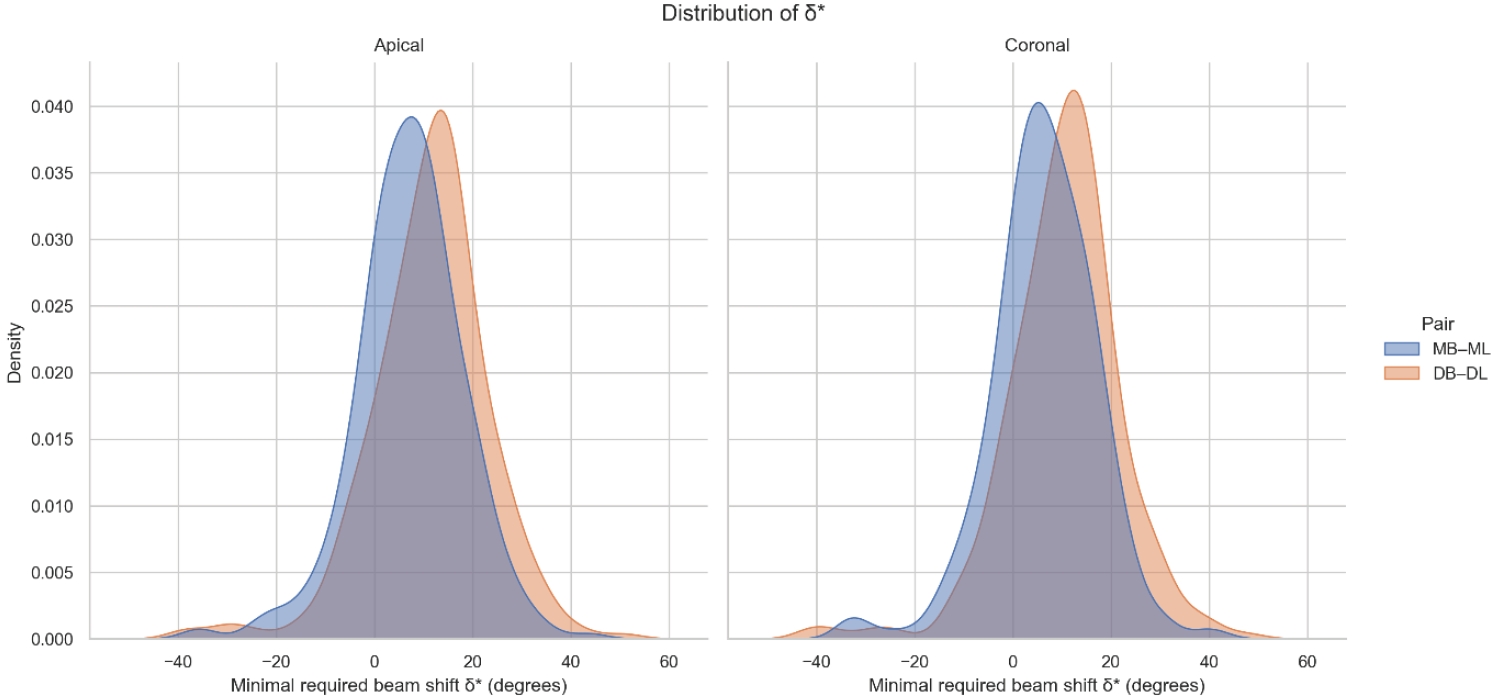
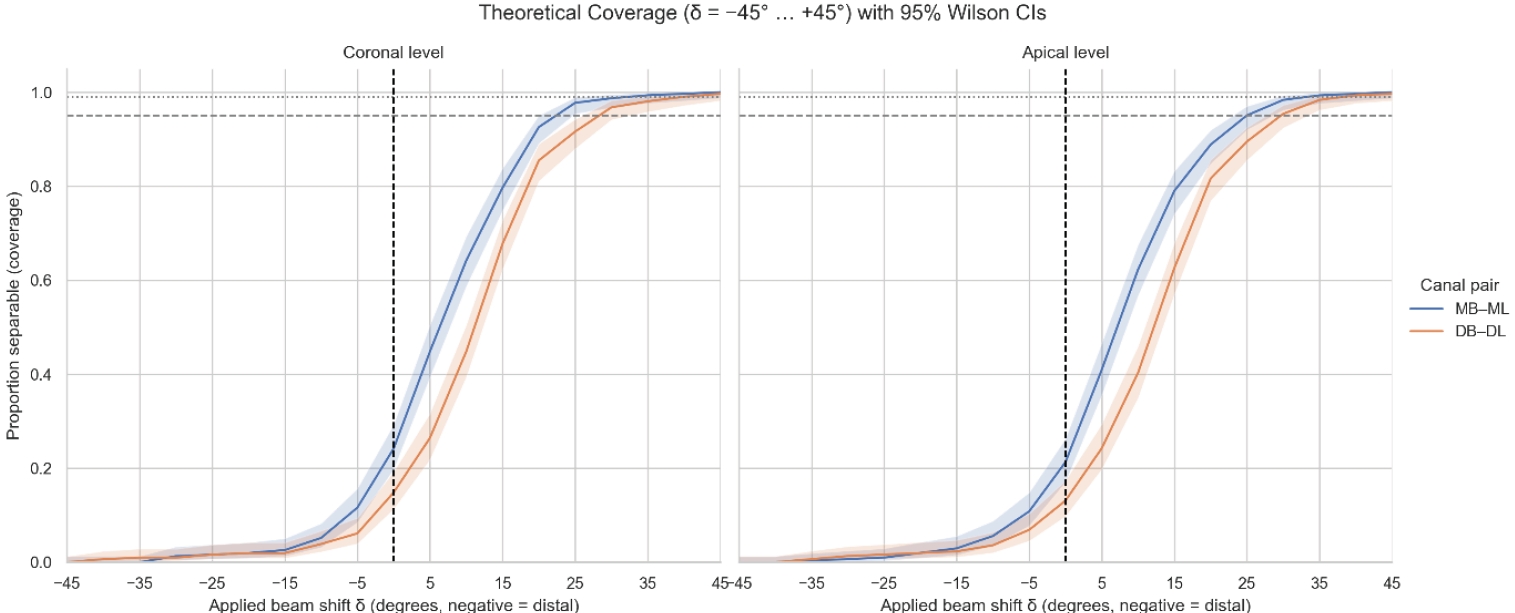
Figure 1. Examples of the cone-beam computed tomography measurements. Examples of measurements indicative of the angles at which root canals overlap. The measurement lines are colored for better visibility showing either mesial (M) or distal (D) canal pair measurements. In roots presenting a single oval-shaped canal, the angle was measured along the axis of this anatomical structure. The dotted line represents the mandibular arch, and the angle between this reference and the X-ray central axis was also measured for final angle calculations. (A) Mesial canal pairs (mesiobuccal–mesiolingual), coronal level. (B) Distal canal pairs (distobuccal–distolingual), coronal level. (C) Mesial and distal measurements, apical level.
Figure 2. Distribution of δ values by canal pair and root level. Smoothed density distributions of the theoretical minimal horizontal beam angulation δ required to achieve radiographic separation of root canal pairs. Mesial (mesiobuccal–mesiolingual) and distal (distobuccal–distolingual) canal pairs are shown separately for the apical (left) and coronal (right) measurement levels. Distal canal pairs exhibit a right-shifted distribution, particularly at the coronal level, reflecting their generally higher beam angulation requirements compared with mesial canals.
Figure 3. Theoretical coverage (δ = −45° to +45°) with 95% Wilson confidence intervals. Theoretical separability (coverage) of mesial (MB–ML) and distal (DB–DL) canal pairs plotted across the full range of applied horizontal beam angulations (δ = −45° to +45°). Curves represent the proportion of canal pairs predicted to be radiographically separable at each δ value, with shaded bands indicating 95% Wilson confidence intervals. Positive δ values correspond to mesial beam angulations; negative δ values represent distal angulations. Mesial canals (MB–ML) reach ≥95% separability between approximately 22° and 25°, and ≥99% at around 32°. Distal canals (DB–DL) require larger angulations, achieving ≥95% at approximately 30° and ≥99% at approximately 40°. The steep rise and subsequent plateau between approximately 25° and approximately 35° indicate the clinically relevant window in which most canal pairs become reliably distinguishable on a single periapical radiograph. MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual.
Figure 1.
Figure 2.
Figure 3.
Determination of optimal horizontal beam angulations for canal separation in mandibular molars using cone-beam computed tomography: a retrospective image-based analysis
| Position | Canal pair | N | Mean ± SD (°) |
|---|---|---|---|
| Coronal | MB–ML (mesial) | 310 | 83.74 ± 10.63 |
| Coronal | DB–DL (distal) | 310 | 79.60 ± 11.63 |
| Apical | MB–ML | 305 | 82.92 ± 10.88 |
| Apical | DB–DL | 305 | 78.72 ± 11.92 |
| Position | Canal pair | t (df) | p-value | Interpretation |
|---|---|---|---|---|
| Coronal | MB–ML | −0.65 (305.1) | 0.518 | NS (no difference) |
| Coronal | DB–DL | −2.96 (302.9) | 0.0033 |
Second molars > first molars |
| Apical | MB–ML | 0.94 (302.7) | 0.347 | NS |
| Apical | DB–DL | −4.45 (302.7) | 1.2 × 10⁻⁵ |
Second molars > first molars |
| Position | Canal pair | δ for ≥95% (°) | δ for ≥99% (°) |
|---|---|---|---|
| Coronal | MB–ML | 22 | 32 |
| Coronal | DB–DL | 30 | 40 |
| Apical | MB–ML | 25 | 32 |
| Apical | DB–DL | 30 | 40 |
| δ (°) | Mesial MB–ML coronal (%) | Distal DB–DL coronal (%) |
|---|---|---|
| 20 | 92.6 (89.1–95.0) | 85.5 (81.1–88.9) |
| 25 | 97.7 (95.4–98.9) | 91.6 (88.0–94.2) |
| 30 | 98.7 (96.7–99.5) | 96.8 (94.2–98.2) |
| 35 | 99.3 (97.7–99.8) | 98.1 (95.8–99.1) |
| 40 | 99.7 (98.2–99.9) | 99.0 (97.2–99.7) |
Table 1. Mean overlap angles (α) by root level and canal pair
Values are presented separately for mesial (MB–ML) and distal (DB–DL) canal pairs at coronal and apical levels. Angles (α, in degrees [°]) were measured from CBCT-derived canal centerlines within each root, representing the projection at which canal outlines fully overlap in two-dimensional radiographs. SD, standard deviation; MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual; CBCT, cone-beam computed tomography.
Table 2. Comparison of first and second mandibular molars (Welch t-tests for α)
Reported are test statistics, degrees of freedom (df), and two-sided Positive values denote higher overlap angles in second molars, consistent with increased distal root curvature. MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual; NS, not significant.
Table 3. Theoretical beam angle thresholds (δ) for ≥95% and ≥99% canal separability
Theoretical beam angulations were derived from δ* = 90° − α; thresholds represent the smallest δ at which coverage ≥95% or ≥99% was achieved. Values represent the minimal mesial horizontal angulations at which the corresponding proportion of canal pairs can be radiographically distinguished. MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual.
Table 4. Wilson 95% CIs for theoretical coverage (proportion of separable canals)
Values are presented as percentage (95% confidence interval). Coverage represents the proportion of canals achieving theoretical separability (δ* ≤ δ) at each predefined mesial beam angulation (δ). Confidence intervals narrow progressively between 25° and 35° indicating statistical stability of the separability plateau. Data were computed for coronal levels using the Wilson method for binomial proportions. CIs, confidence intervals; MB–ML, mesiobuccal–mesiolingual; DB–DL, distobuccal–distolingual.

