
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 37(1); 2012 > Article
- Research Article Coronal microleakage of four temporary restorative materials in Class II-type endodontic access preparations
- Sang-Mi Yun, DDS, MSD, Lorena Karanxha, DDS, Hee-Jin Kim, DDS, MSD, Sung-Ho Jung, DDS, MSD, Su-Jung Park, DDS, MSD, Kyung-San Min, DDS, PhD
-
2012;37(1):-33.
DOI: https://doi.org/10.5395/rde.2012.37.1.29
Published online: March 2, 2012
Department of Conservative Dentistry, Wonkwang University School of Dentistry, Iksan, Korea.
- Correspondence to Kyung-San Min, DDS, PhD. Associate professor, Department of Conservative Dentistry, Wonkwang University School of Dentistry, 344-2 Shinyong-dong, Iksan, Korea 570-749. TEL, +82-63-850-6930; FAX, +82-63-859-2932; mksdd@wku.ac.kr
• Received: December 13, 2011 • Revised: January 30, 2012 • Accepted: February 1, 2012
©Copyights 2012. The Korean Academy of Conservative Dentistry.
- 2,796 Views
- 12 Download
- 3 Crossref
Abstract
-
Objectives The purpose of this study was to evaluate the microleakage of 4 temporary materials in teeth with Class II-type endodontic access preparations by using a glucose penetration model.
-
Materials and Methods Glucose reaction test was performed to rule out the presence of any reaction between glucose and temporary material. Class II-type endodontic access preparations were made in extracted human premolars with a single root (n = 10). Each experimental group was restored with Caviton (GC), Spacer (Vericom), IRM (Dentsply-Caulk), or Fuji II(GC). Microleakage of four materials used as temporary restorative materials was evaluated by using a glucose penetration model. Data were analyzed by the one-way analysis of variance followed by a multiple-comparison Tukey test. The interface between materials and tooth were examined under a scanning electron microscope (SEM).
-
Results There was no significant reaction between glucose and temporary materials used in this study. Microleakage was significantly lower for Caviton and Spacer than for Fuji II and IRM. SEM observation showed more intimate adaptation of tooth-restoration interfaces in Caviton and Spacer than in IRM and Fuji II.
-
Conclusions Compared to IRM and Fuji II, Caviton and Spacer can be considered better temporary sealing materials in Class II-type endodontic access cavities.
Introduction
The main principles of endodontic treatment should be eliminating all bacteria from the tooth, and then attempting to maintain the tooth in this disinfected state during and after treatment. During endodontic treatment, temporary restorative materials are used to create a fluid-tight seal in access cavity in order to prevent marginal leakage and ingress of oral fluids and microorganisms into the root canal.1 Therefore, the use of temporary restorative materials between appointments is one of the important factors that determines the success or failure of root canal treatment.2
Many temporary restorative materials have been studied to determine their ability to seal endodontic access preparations.2-6 Most studies have examined the materials in simple access preparations within an intact tooth structure. In clinical practice, however, the use of these materials frequently involves the restoration of a multisurface cavity preparation necessitated by the removal of caries or defective restorations. Furthermore, materials that provide adequate seals for access preparations in teeth with intact surrounding tooth structure may not be appropriate for use in teeth with Class II-type access preparations.7
The purpose of this study was to evaluate and compare the microleakage of several materials used as temporary restorative materials in teeth with Class II-type endodontic access preparations by using a glucose penetration model.
Materials and Methods
Glucose reaction test was performed by the method of Shemesh et al.8 Four temporary materials, namely, Caviton (GC, Tokyo, Japan), Spacer (Vericom, Anyang, Korea), IRM (Dentsply-Caulk, Milford, DE, USA), and Fuji II (GC, Tokyo, Japan), were mixed according to the manufacturers' instructions and inserted in 2-mm-deep round wax molds with a diameter of 4 mm (n = 10). All samples were maintained at 37℃ and 100% humidity for 24 hours. The set materials formed round discs after they were removed from the molds. Each disc was then inserted into a small test tube with 4 mL of glucose (1 mol/L) solution. Ten additional test tubes were used as controls, and these contained only 4 mL of glucose solution. After 1 week, a 0.1-mL sample of the solution was removed from each test tube and was analyzed with a glucose kit (D-glucose HK assay kit, Megazyme, Wicklow, Ireland) in an enzyme-linked immunosorbent assay (ELISA) device (SpectaMas250, Molecular Devices, Sunnyvale, CA, USA) at a wavelength of 340 nm.
This study received approval from the Institutional Review Board of the Wonkwang Dental Hospital of Korea (WKD IRB Reference Code: 201106-01). We selected 44 freshly extracted intact human premolars with single, straight root canal for this study. Endodontic access preparations were made using a #4 carbide round bur followed by a safe-end fissure diamond bur in a high-speed handpiece. Then, a proximal box (4 × 4 mm) was created over the mesial wall by using a straight fissure diamond bur to create a standardized Class II-type access cavity preparation.
After measuring the working length, the root canals were cleaned and given shape with ProTaper rotary instruments (Dentsply-Maillefer, Ballaigues, Switzerland) under copious irrigation with 2.5% sodium hypochlorite. The finishing of canals was performed until a size F3 reached the full working length.
In all experimental groups, small cotton pellets were placed at the canal orifices, which were coronally sealed with Caviton, Spacer, IRM, or Fuji II. No pretreatment for teeth was performed before insertion of temporary material. The teeth in the negative control group were covered with 2 layers of nail varnish. The teeth in the experimental groups and in the positive control group were coated with 2 layers of nail varnish, except for 1 mm around the tooth-restoration interface and 3 mm from the apical end. Then, the teeth were placed in a device designed to measure glucose leakage (Figure 1a). The glucose leakage model used in the present study was similar to the one used by Xu et al.9
A 20 µL aliquot of the solution was drawn from the glass bottle by using a micropipette at 1, 3, 5, 7, and 14 days. After withdrawing the sample, 20 µL of fresh 0.2% NaN3 was added to the glass bottle reservoir to maintain a constant volume of 5 mL. If there was any decrease in volume in the control bottle because of evaporation, the corresponding amount of sterile deionized water was added to the glass bottle. The sample was then analyzed with a glucose kit in an ELISA device at a wavelength of 340 nm.
Two specimens from each group were randomly selected, and temporary restorative materials and cavity-wall interface were examined. Negative impressions of the proximal surface (including temporary restoration and tooth interface of the specimen) were obtained by using polyvinylsiloxane impression material (Honigum, DMG, Hamburg, Germany). Epoxy resin (Modralit 3K, Dreve Dentamid GmbH, Unna, Germany) was used to create a positive replica. This was performed by air drying, platinum sputter-coating, and observing at ×100 magnification with a scanning electron microscope (SEM, JSM-6360, JEOL, Tokyo, Japan).
Statistical analysis of glucose reaction test and microleakage test was performed by one-way analysis of variance followed by a multiple-comparison Tukey test by using the software SPSS version 12.0 (SPSS GmbH, Munich, Germany). Statistical significance was determined at p = 0.05.
Results
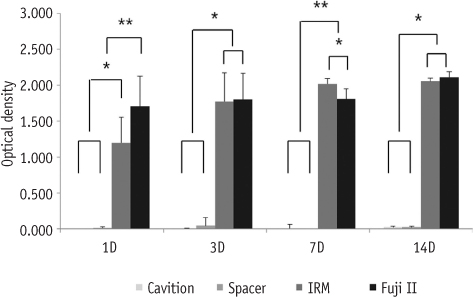
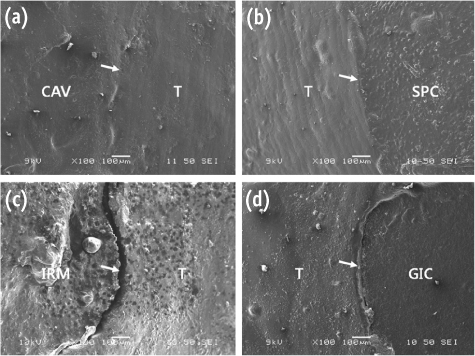
There was no significant reaction between glucose and temporary materials used in this study (Figure 1b). The negative control group showed no leakage throughout the experiment period. The positive control group showed immediate leakage. The mean microleakage values for experimental groups at specified time intervals after the insertion of restoration are presented in Figure 2. Significantly more microleakage was observed in Fuji II and IRM than in Caviton and Spacer. In IRM and Fuji II group, furthermore, microleakage was increased in time dependent manner. SEM observation of specimens showed more intimate adaptation of tooth-restoration interfaces in Caviton and Spacer than in Fuji II and IRM (Figures 3a and 3b). However, IRM and GIC showed voids and deep gaps within the material bulk and at the tooth-material interface (Figures 3c and 3d).
Discussion
In our study, Caviton and Spacer provided a better coronal marginal seal in Class II-type endodontic access preparations than IRM and Fuji II did. Caviton is a premixed temporary restorative material similar to Cavit (3M ESPE, Seefeld, Germany), which is the most widely used material in temporary restoration. It contains zinc oxide, calcium sulfate, glycol acetate, polyvinylacetate resins, polyvinyl chloride acetate, triethanolamine, and pigments. Many studies have shown that Caviton provides a good marginal seal when used to restore endodontic access preparations.4,5,10 This advantage is attributed to its high hygroscopic expansion during setting, which could increase the sealing ability between the materials and the access cavity.11,12
Spacer is a resin-based light-curing temporary filling material similar to Fermit (Vivadent, Saint-Jorioz, France), TERM (Dentsply-Caulk), or Clip (Voco, Cuxhaven, Germany), which has shown good sealing ability in previous studies.2,3,7 The results of our study indicate that the efficacy of Spacer sealing of marginal leakage is comparable to that of Caviton. Anderson et al. showed that TERM provided excellent seals and was superior to Cavit and IRM for restoring Class II-type endodontic access preparation.7 Teplitsky and Meimaries reported that the dye did not penetrate TERM.13 Cho et al. also reported that the microleakage of Spacer and Caviton was similar, but there was no correlation between polymerization shrinkage or hygroscopic expansion and microleakage.14 They suggested that other factors, including coefficient of thermal expansion, modulus of elasticity, or handling property, may affect to microleakage of resin-based temporary filling materials. Moreover, polymerization of resin-based materials is initiated by exposure to visible light source, and hence, it does not show postoperative delays to maximum function.2 In this respect, within the limitation of this study, resin-based filling material including Spacer has the potential to be used as temporary sealing material in endodontic cavity although it has been used mainly in restorative dentistry.
IRM is a zinc oxide-eugenol cement reinforced with polymethyl methacrylate. In this study, microleakage was significantly higher in IRM than in Caviton and Spacer in Class II-type endodontic cavities. The hygroscopic expansion of IRM was much lower than that of Caviton. The lack of hygroscopic expansion cannot compensate for the gap that may develop in the tooth-material interface. In addition, a powder and liquid have to be mixed together to prepare the paste; this may be the cause of reduced homogeneity. Deveaux et al. reported that they observed numerous voids when they examined the visible surfaces of IRM samples after sectioning.15
Fuji II is a glass ionomer cement that has the ability to form a chemical bond with both enamel and dentin. Use of glass ionomer cements as temporary restoration materials during endodontic treatment has been investigated in a number of studies with various results.2,6 In this study, however, Fuji II showed marginal leakage as high as that observed in the positive controls. This has been attributed to its sensitivity to manipulation and polymerization shrinkage resulting in a potential avenue of microleakage.16,17 Burrow et al. reported that numerous air inclusions were found within the glass ionomer cement.18 Xie et al. reported that the SEM image of glass ionomer cement showed an obvious marginal gap at the tooth-restoration interface.19 A failure of adhesion by polymerization shrinkage and microleakage gap may be caused by poor bond strength of the glass ionomer cement. The positive correlations between dentin bond strength and microleakage might explain why the glass ionomer cement showed high microleakage.
In the present study, the marginal gap and voids of each material were evaluated by examining the material-gingival walls interface by using SEM. SEM observation of the specimens revealed intimate adaptation of tooth-restoration interfaces in Caviton and Spacer than in Fuji II and IRM. In the Fuji II and IRM specimens, however, marginal gap and voids were often observed. This might explain the deterioration of the sealing ability of Fuji II and IRM in Class II-type access preparations.
Many studies has been performed to determine the sealing ability of various materials.20 However, most studies were performed in simple access preparation within intact tooth structures, which are rarely the teeth requiring root canal treatments in clinical practice. Materials that provided appropriate sealing in simple preparations might be unacceptable in complex access preparations such as Class II-type that involved both the access preparation and multisurface cavity preparations.7
In this study, glucose was selected as the tracer because of its small molecular size (MW = 180 Da) and because it is a nutrient for bacteria. If glucose could enter the canal from the oral cavity, bacteria that might survive root canal preparation could multiply and potentially lead to periapical inflammation. Therefore, glucose was thought to be more clinically relevant than other tracers used in microleakage tests.21 Moreover, in our study, glucose reaction test was performed to exclude the possibility of reaction that may occur between glucose and materials before the main leakage test, because microleakge results can by masked by the reaction between glucose and materials.
Conclusions
With the limitations of this in vitro study, Caviton and Spacer can be considered as good temporary sealing materials in case of Class II-type access preparations. In contrast, Fuji II and IRM are not recommended as temporary sealing materials in Class II-type endodontic access cavities.
- 1. Noguera AP, McDonald NJ. Comparative in vitro coronal microleakage study of new endodontic restorative materials. J Endod. 1990;16: 523-527.PubMed
- 2. Ciftçi A, Vardarli DA, Sönmez IS. Coronal microleakage of four endodontic temporary restorative materials: an in vitro study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108: e67-e70.ArticlePubMed
- 3. Deveaux E, Hildelbert P, Neut C, Romond C. Bacterial microleakage of Cavit, IRM, TERM, and Fermit: a 21-day in vitro study. J Endod. 1999;25: 653-659.ArticlePubMed
- 4. Jung DH, Noh YS, Lee HD, Chang HS, Ryu HW, Min KS. Microleakage of endodontic temporary restorative materials under dynamic loading. J Korean Acad Conserv Dent. 2008;33: 198-203.Article
- 5. Lee YC, Yang SF, Hwang YF, Chung KH. Microleakage of endodontic temporary restoration materials. J Endod. 1993;19: 516-520.PubMed
- 6. Madarati A, Rekab MS, Watts DC, Qualtrough A. Time-dependence of coronal seal of temporary materials used in endodontics. Aust Endod J. 2008;34: 89-93.ArticlePubMed
- 7. Anderson RW, Powell BJ, Pashley DH. Microleakage of temporary restorations in complex endodontic access preparations. J Endod. 1989;15: 526-529.ArticlePubMed
- 8. Shemesh H, Souza EM, Wu MK, Wesselink PR. Glucose reactivity with filling materials as a limitation for using the glucose leakage model. Int Endod J. 2008;41: 869-872.PubMed
- 9. Xu Q, Fan MW, Fan B, Cheung GS, Hu HL. A new quantitative method using glucose for analysis of endodontic leakage. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99: 107-111.ArticlePubMed
- 10. Lai YY, Pai L, Chen CP. Marginal leakage of different temporary restorations in standardized complex endodontic access preparations. J Endod. 2007;33: 875-878.ArticlePubMed
- 11. Cruz EV, Shigetani Y, Ishikawa K, Kota K, Iwaku M, Goodis HE. A laboratory study of coronal microleakage using four temporary restorative materials. Int Endod J. 2002;35: 315.ArticlePubMed
- 12. Uçtaşli MB, Tinaz AC. Microleakage of different types of temporary restorative materials used in endodontics. J Oral Sci. 2000;42: 63. 67.ArticlePubMed
- 13. Teplitsky PE, Meimaris IT. Sealing ability of Cavit and TERM as intermediate restorative materials. J Endod. 1988;14: 278-282.ArticlePubMed
- 14. Cho NY, Lee IB. Polymerization shrinkage, hygroscopic expansion and microleakage of resin-based temporary filling materials. J Korean Acad Conserv Dent. 2008;33: 115-124.Article
- 15. Deveaux E, Hildelbert P, Neut C, Boniface B, Romond C. Bacterial microleakage of Cavit, IRM, and Term. Oral Surg Oral Med Oral Pathol. 1992;74: 634-643.ArticlePubMed
- 16. Uranga A, Blum JY, Esber S, Parahy E, Prado C. A comparative study of four coronal obturation materials in endodontic treatment. J Endod. 1999;25: 178-180.ArticlePubMed
- 17. Zaia AA, Nakagawa R, De Quadros I, Gomes BP, Ferraz CC, Teixeira FB, Souza-Filho FJ. An in vitro evaluation of four materials as barriers to coronal microleakage in root-filled teeth. Int Endod J. 2002;35: 729-734.ArticlePubMed
- 18. Burrow MF, Nopnakeepong U, Phrukkanon S. A comparison of microtensile bond strengths of several dentine bonding systems to primary and permanent dentine. Dent Mater. 2002;18: 239-245.PubMed
- 19. Xie H, Zhang F, Wu Y, Chen C, Liu W. Dentine bond strength and microleakage of flowable composite, compomer and glass ionomer cement. Aust Dent J. 2008;53: 325-331.ArticlePubMed
- 20. Naoum HJ, Chandler NP. Temporization for endodontics. Int Endod J. 2002;35: 964-978.ArticlePubMed
- 21. Friedman S. Retrograde approaches in endodontic therapy. Endod Dent Traumatol. 1991;7: 97-107.ArticlePubMed
REFERENCES
Figure 1
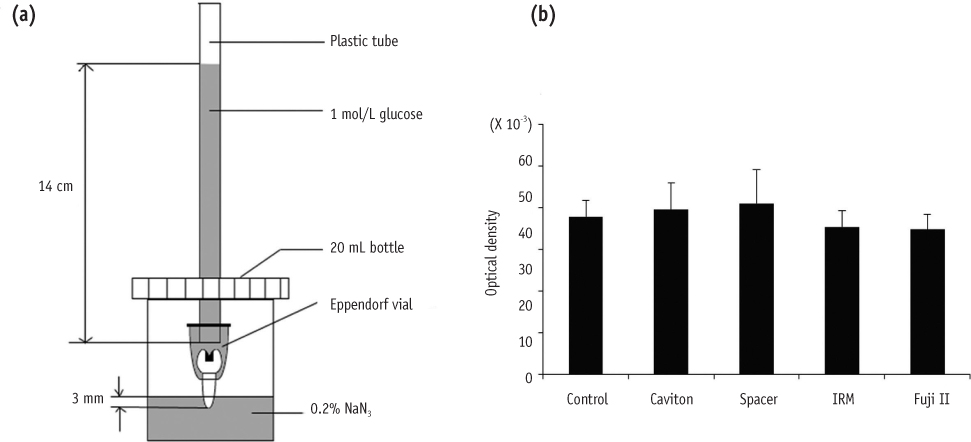
(a) Glucose leakage model; (b) Glucose reaction test. The temporary materials used in this study showed no significantly difference compared with control in optical density (p < 0.05).
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Impact of spacers and thermocycling on porosity and gaps in class II endodontic temporary restorations evaluated by microcomputed tomography
Fahda N. Algahtani, Manal Alkadi, Hiba R. Talic, Sarah S. AlShalawi, Lujain M. Alqarni, Reem M. Barakat, Rasha Haridy, Sara M. ElKhateeb, Rahaf A. Almohareb
Scientific Reports.2025;[Epub] CrossRef - Comparative Evaluation of Sealing Ability, Water Absorption, and Solubility of Three Temporary Restorative Materials: An in vitro Study
AR Prabhakar, N Shantha Rani
International Journal of Clinical Pediatric Dentistry.2017; 10(2): 136. CrossRef - Sealing Ability of Three Different Materials Used as Retrograde Filling
Ji-Hoon Park, Seung-Bok Kang, Yong-Hoon Choi, Ji-Hyun Bae
Journal of Korean Dental Science.2012; 5(2): 60. CrossRef
 ePub Link
ePub Link Cite
CiteCoronal microleakage of four temporary restorative materials in Class II-type endodontic access preparations
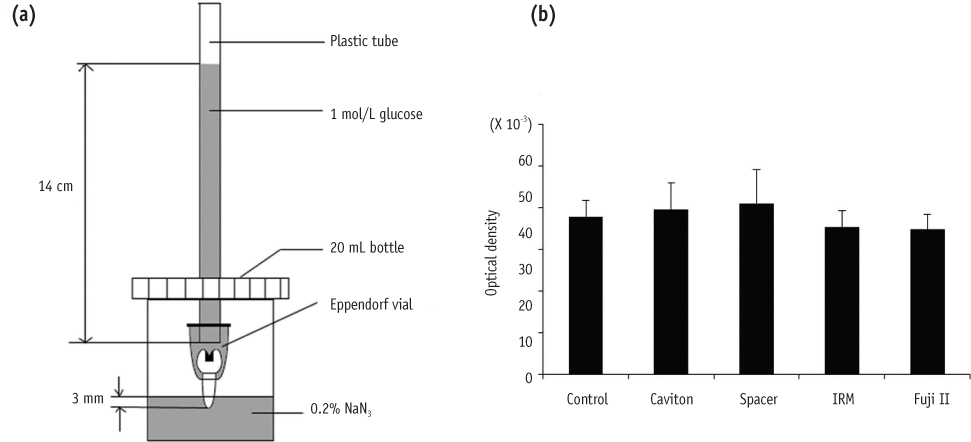
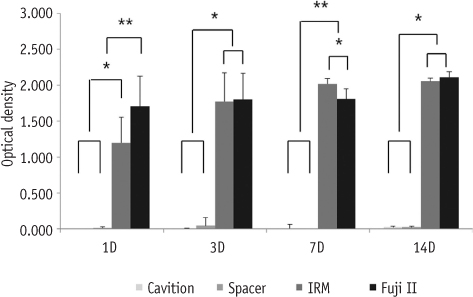
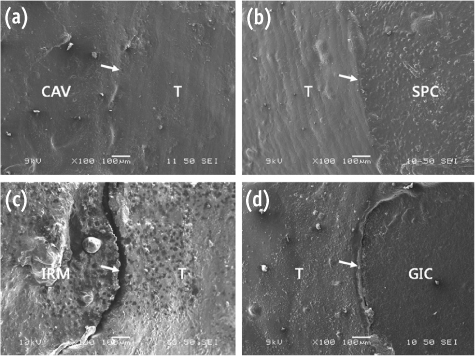
Figure 1
(a) Glucose leakage model; (b) Glucose reaction test. The temporary materials used in this study showed no significantly difference compared with control in optical density (p < 0.05).
Figure 2
Microleakage in Class II-type endodontic access preparations. Amounts of glucose penetrating the temporary materials and canal were represented the optical density (*p < 0.05). Asterisk means statistically significant difference.
Figure 3
Scanning electron microscopic (SEM) images (×100) on gingival margin of temporary restoration materials and cavity-wall interface (white arrows). (a) Caviton; (b) Spacer; (c) IRM; (d) Fuji II.
T, tooth; CAV, Caviton; SPC, Spacer; GIC, Fuji II.
Figure 1
Figure 2
Figure 3
Coronal microleakage of four temporary restorative materials in Class II-type endodontic access preparations

