
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 47(4); 2022 > Article
- Research Article Apical periodontitis in mesiobuccal roots of maxillary molars: influence of anatomy and quality of root canal treatment, a CBCT study
-
Samantha Jannone Carrion
 , Marcelo Santos Coelho, Adriana de Jesus Soares, Marcos Frozoni
, Marcelo Santos Coelho, Adriana de Jesus Soares, Marcos Frozoni -
Restor Dent Endod 2022;47(4):e37.
DOI: https://doi.org/10.5395/rde.2022.47.e37
Published online: September 19, 2022
Department of Endodontic, São Leopoldo Mandic School of Dentistry, Campinas, SP, Brazil.
- Correspondence to Marcelo Santos Coelho, DDS, MSc, PhD. Assistant Professor, Department of Endodontic, São Leopoldo Mandic School of Dentistry, Rua Emilio Ribas 776/13, Campinas, SP 13025-141, Brazil. coelho_marcelo@yahoo.com.br
• Received: May 4, 2022 • Revised: July 13, 2022 • Accepted: July 26, 2022
Copyright © 2022. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to evaluate the prevalence of apical periodontitis (AP) in the mesiobuccal roots of root canal-treated maxillary molars.
-
Materials and Methods One thousand cone-beam computed tomography images of the teeth were examined by 2 dental specialists in oral radiology and endodontics. The internal anatomy of the roots, Vertucci’s classification, quality of root canal treatment, and presence of missed canals were evaluated; additionally, the correlation between these variables and AP was ascertained.
-
Results A total of 1,000 roots (692 first molars and 308 second molars) encompassing 1,549 canals were assessed, and the quality of the root canal filling in the majority (56.9%) of the canals was satisfactory. AP was observed in 54.4% of the teeth. A mesiolingual canal in the mesiobuccal root (MB2 canal) was observed in 54.9% of the images, and the majority (83.5%) of these canals were not filled. Significant associations were observed between the presence of an MB2 canal and the quality of the root canal filling and the presence of AP.
-
Conclusions AP was detected in more than half of the images. The MB2 canals were frequently missed or poorly filled.
INTRODUCTION
The aim of root canal therapy is to treat or prevent the development of apical periodontitis (AP) [1]. However, several factors such as the location, adequate disinfection, and filling of the canals followed by the restoration of the tooth can affect the accomplishment of this aim. Thus, adequate knowledge about the internal anatomy of the root and removal of the biofilm from the root canal system are of utmost importance [2].
In humans, treatment of maxillary molars is often considered the most challenging, mainly due to the possible presence of a second canal in the mesiobuccal root, also known as the MB2 canal. Previously, in vitro destructive methodologies were used to study the internal anatomy, whereas currently, cone-beam computed tomography (CBCT) is considered as the best method available for in vivo applications [3,4]. CBCT images have indicated that the worldwide prevalence of the MB2 canal could vary from 48% to 98% [5,6].
Inadequate disinfection of root canals might lead to poor outcomes; this failure can be associated with an inadequate working length, insufficient root canal preparation, and failure in locating all the main canals [7,8]. Missed canals are considered one of the main reasons for root canal therapy failure [9]. In maxillary molars, a missed MB2 canal was found to be significantly associated with failure in endodontic therapy [10,11].
The association between poorly disinfected canals and AP has been demonstrated via histological examination [12,13]. However, the clinician has to rely on symptoms and radiographic images to reach an accurate diagnosis of AP. Even though bi-dimensional radiographs are easily available nowadays, they might lead to an inaccurate diagnosis [14]. A recent study using 250 µm voxel-size CBCT images, assessed the impact of root canal filling on AP; however, they concluded that further evaluations were required using smaller voxel sizes [10].
Thus, the present study aimed to assess the root canal anatomy of maxillary molars that underwent root canal treatment and to determine its association with the quality of the root canal therapy and the presence of AP.
MATERIALS AND METHODS
The research protocol used in this retrospective, observational study was reviewed and approved by the Ethical Committee of São Leopoldo Mandic School of Dentistry (#4.021.698). The images, taken for reasons not related to the present study, were selected from the database of a private radiology clinic.
The inclusion criteria were as follows: first and second maxillary molars with a mesiobuccal root and a history of root canal therapy, patient age, > 18 years old, presenting the included teeth in either right or left maxilla. The teeth should present with complete root development and the crown must have a restoration in position. The exclusion criteria were as follows: patients were under the age of 18 and those with immature apices, external root resorption, signs of fracture, and presence of metallic posts in the mesial roots. Images with artifacts in the crown or roots that prevented the proper visualization of the canals were also excluded. All images were obtained between 2015 and 2021 and assessed from March 2020 to February 2021.
The sample size was calculated considering the 95% confidence interval (CI), a statistically significant differences of 5%, and a proportion of prevalence of 70% for the first molars and 47% for the second molars. Consequently, taking into consideration a sample loss of 10%, a total of 359 and 426 MB canals were assessed in this study.
The Prexion 3D (Teracom, San Mateo, CA, USA) CBCT image scanner operating at 110 Kvp, 4 mA with a voxel size of 100 µm and field of view (FOV) of 5 × 5 cm was used.
The images were simultaneously assessed by 2 dental specialists in oral radiology and endodontics, with more than 5 years of experience. The examiners used a high-definition screen Dell U2312HM DIGITAL (1,920 × 1,080, TrueColor 32 bits, 60 Hz) in a dark room, with a dedicated memory video board of 1,024 MB (Dell Inc., Austin, TX, USA). The OnDemand 3D (Cybermed, Irvine, CA, USA) software was used, wherein the evaluators could freely orient the images in any of the multiplanar reconstructions (axial, coronal, and sagittal). The contrast, brightness, and zoom were adjusted at the discretion of the evaluator. In case of disagreement, a third evaluator (specialist in oral radiology) discussed the case until a consensus was reached. The evaluators, including the third observer, were calibrated by assessing 100 images, and all discrepancies were discussed until a consensus was reached.
Initially, the anatomical feature of the root was assessed and classified from types I to VIII following Vertucci’s classification [15]. Furthermore, the presence of a second canal in the mesiobuccal root was registered. The quality of the root canal treatment was assessed and classified as follows: 1) no root canal filling present; 2) ideal filling located at 0–2 mm from the apex with no technical errors; 3) underfilled canal; 4) overfilled canal; 5) presence of zips or ledges; and 6) presence of voids.
The classification suggested by Estrela et al. [16] for AP was used in this study. In the absence of any radiolucency, the tooth was classified as “0.” When a periapical lesion was detected, the tooth was classified from 1 to 5 depending on the size of the lesion as follows: 1 (0.5–1 mm), 2 (1–2 mm), 3 (2–4 mm), 4 (4–8 mm), and 5 (> 8 mm). The categories “E” when expansion of the cortical bone was observed and “D” when destruction was observed were added to the classification when deemed applicable. The size was measured as the largest diameter of the lesion when observed in the coronal view using the ruler tool of the software.
The Kappa test was used for interobserver reliability. The association between the quality of the root canal treatment and the number of canals and foramina and the presence of AP and also the presence of AP with the number of canals, foramina, and Vertucci’s classification were calculated using the χ2 test or G test; the odds ratio (OR) and CI were used when required. SPSS 23 (SPSS Inc., Chicago, IL, USA) was used, and a p value of 0.05 was considered statistically significant.
RESULTS
Overall, 1,549 canals from 1,000 mesiobuccal roots (692 [69.2%] first molars and 308 [30.8%] second molars) were assessed. The overall agreement between the examiners was considered excellent for all the parameters assessed (number of canals, number of foramina, Vertucci’s classification, quality of treatment in both the MB and MB2 canals, and presence of AP; Table 1).
Table 1
Kappa test showing excellent agreement rate between the observers at different variables
The prevalence of a single mesiobuccal canal was 45.1%, and 2 canals were observed in 54.9% of the teeth. A single foramen was observed in 60.7% of the teeth and 2 foramina in 39.3% of the teeth. Based on Vertucci’s classification, 44.7% of the teeth presented with type I configuration; 38.7% with type IV configuration, 15.9% with type II configuration, 0.6% with type V configuration, and 0.1% with type III configuration. None of the teeth presented with types VI, VII, and VIII configurations.
AP was detected in 544 roots (54.4%), and 466 (46.6%) teeth presented with intact bone. Of the 1,549 root canals, 623 (40.2%) presented with adequate fillings, 487 (31.4%) presented with no filling, and 439 (28.3%) presented with inadequate fillings (Table 2). Furthermore, 56.9% of the mesiobuccal canals were properly filled, 39.3% presented with inadequate fillings, and 3.8% were not filled. Similarly, 54 (9.8%) of the MB2 canals were adequately filled, 46 (4.6%) presented with inadequate fillings, and 449 (81.8%) were not filled. Table 3 depicts the overall classification of the quality of the filling in each root canal.
Table 2
Association between the number of foramina and quality of root canal treatment and association between the quality of root canal treatment and the classification of apical periodontitis
Table 3
Absolute number (percentage) of the quality of root canal treatment and prevalence of apical periodontitis in its different classifications
The Chi-square test showed a statistically significant association between the number of foramina and the quality of the root canal treatment (p < 0.001) (Figure 1). The presence of 2 foramina increased the risk of untreated canals by 3.03 times. A total of 352 out of 767 (45.9%) canals with one foramen and 271 out of 623 (34.7%) canals with 2 foramina presented with satisfactory fillings. Furthermore, no root canal fillings were observed in 146 out of 767 (19%) canals with a single foramen and 341 out of 623 (43.6%) canals with 2 foramina; unsatisfactory fillings were observed in 269 canals (35.1%) with a single foramen and 170 canals (21.7%) with 2 foramina.
Figure 1
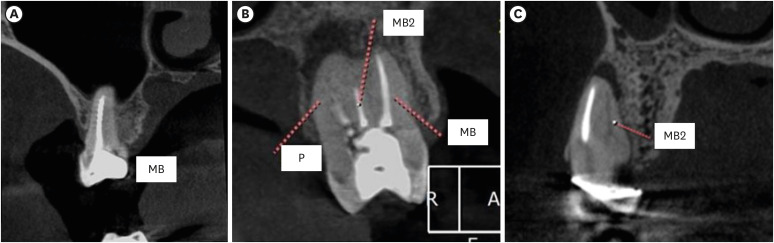
Representative images showing (A) satisfactory filling, (B) satisfactory filling (MB), unsatisfactory (MB2) and (C) Untreated (MB2).
MB, mesiobuccal; MB2, second mesiobuccal; P, palatal.
The periapical bone was normal in 681 (44.4%) canals out of 1,549 canals; among them, 310 (45.5%) canals presented with satisfactory root canal fillings. AP was observed in 868 (55.6%) canals, and 32.6% to 36.5% of them presented with satisfactory root canal fillings (Table 3).
A statistically significant association was observed between the quality of root canal treatment and the presence of AP (p < 0.05). The presence of unsatisfactory root canal fillings increased the risk of AP (classifications 1, 2, and 3 by 1.57, 1.68, and 2.15 times, respectively).
Among the 451 roots with a single canal, 251 (55.7%) presented with normal bone and 200 (44.3%) with AP; likewise, among the 549 teeth with MB2 canals, 215 (39.2%) presented with normal bone and 334 (61.8%) with AP. The risk of class 2, class 3, class 4, and class D AP was 1.72 (CI, 1.20–2.46); 3.33 (CI, 2.16–5.13), 3.00 (CI, 1.23–7.23), and 2.07 (CI, 1.32–3.26), respectively, in teeth with MB2 canals.
Among the 607 roots with a single foramen, 333 (54.9%) had normal bone and 274 (46.1%) presented with AP; among the 393 teeth with 2 separated foramina, 133 (33.8%) had normal bone and 260 (66.2%) presented with AP. The risk of class 3, class 4, and class D AP in roots with 2 separated foramina was 2.33 (CI, 1.62–3.35), 3.76 (CI, 1.65–8.57), and 2.35 (CI, 1.51–3.68) times, respectively.
The classification 0 (absence of AP) was the most prevalent in teeth with Vertucci’s type I (55.9%), type II (51.6%), type III (100%), and type IV (33.9%) configuration. Among teeth with Vertucci’s type VI anatomy, no AP was detected in 33.3% of the teeth, whereas another 33.3% presented with class D AP. No association was observed between Vertucci’s classification and the presence of AP.
DISCUSSION
AP appears to be present in 50% of the population worldwide; although it is present in only 3% of the teeth in general, the incidence of AP is considerably higher in the posterior teeth [17]. In agreement with this previous result, in the present study, AP was observed in 54.4% of the teeth [17]. AP is related to cardiovascular disease and poor outcomes in pregnant women [18,19]. A recent study demonstrated that high levels of C-reactive protein (CRP) are found in patients with AP [20]. High levels of CRP are correlated with the development of atherosclerotic plaque and serious systemic adverse effects [21]. However, proper root canal treatment, which includes the identification, adequate preparation, and filling of these teeth results in a decreased level of these proteins. The high prevalence of missed canals resulting in AP in the present study leads to the conclusion that it is important to address this issue in order to improve the health of the population.
The use of CBCT in dentistry was proposed by Mozzo et al. [22] the tri-dimensional aspect of CBCT images results in higher sensitivity for the detection of AP when compared to bi-dimensional radiographs. The interpretation of these images may vary depending on the experience of the observer; therefore, 2 observers certified in both oral radiology and endodontics were used in the current study [23]. Excellent agreement levels were reached with all the assessed parameters (Table 1). Such a level of agreement while discussing CBCT images was not reported in previous studies using dental students, residents, or oral radiologists [10,23,24].
One of the greatest challenges during the treatment of maxillary molars is the possibility of encountering a second canal in the mesiobuccal root. Similar to the findings of previous studies using CBCT, 54.9% of the teeth in the current study presented with an additional canal [6,25]. However, it is important to emphasize that this finding might not reflect that observed in a clinical setting. A previous in vitro study showed that the combined use of microscopes and ultrasonic resulted in a MB2 visualization of 74% [26]. Furthermore, a previous clinical study have reported a higher prevalence of MB2 canals than that reported in the present study [27]. Parker et al. [28] demonstrated that troughing could lead to clinical negotiating in canals that were not visible in the CBCT scan. Some roots with a single canal, especially those with appropriate fillings and AP might consist of a second canal that is not visible in the CBCT scan.
Missed canals have been associated with AP. do Carmo et al. [10] used CBCT images to evaluate the presence of missed canals in a Brazilian subpopulation and found that 48.25% of the MB2 canals were missed in maxillary molars. However, the findings of the present study are not in accordance with the results of the aforementioned study. In the present study, untreated MB2 canals were detected in 81.8% of the teeth examined. This discrepancy might be due to differences in the CBCT acquisition; while the present study used a voxel size of 100 µm, the size used in the aforementioned study was 250 µm. Voxel sizes smaller than 200 µm are more reliable in detecting the internal anatomy variances in the case of a filled MB canal [29]. Moreover, the aforementioned study comprised 3 oral radiologists, while the present study employed 2 specialists in both oral radiology and endodontics.
A recent study reported that 98% of teeth with at least one missed canal, particularly the multi-rooted teeth, was affected by AP; AP was detected in 100% of teeth presenting with a missed canal [30]. The results of the present study showed that among the 449 missed MB2 canals (representing 81.8% of the total), 166 (37.0%) had a healthy periapical status and 283 (63.0%) had AP. The OR for AP in untreated canals was 3.03 (CI, 2.36–3.90). These results seem to be less impressive compared to those reported by Costa et al. (6.25; CI, 2.92–13.37) [30]. It may be inferred that an untreated MB2 with a foramen that merges with the main MB canal might not present with AP. Roots with 2 foramina were significantly associated with AP in the current study (Table 4).
Table 4
Association between the number of canals, foramens and Vertucci’s classification with the classification of apical periodontitis
This study has some limitations owing to the large sample size. It was not possible to determine whether the root canals were treated by an endodontist or a general dentist. In the case of posterior teeth, there is a higher risk of failure if the treatment is not performed by an endodontist [31]. Despite the improved sensitivity with regard to the diagnosis of AP in untreated root canals and filled roots, there is the possibility of over-diagnosis when CBCT images are used [32]. Additionally, properly filled roots with AP could be in the healing mode, which could lead to an overestimation of the results. Therefore, care should be taken before drawing conclusions related to the presented results and invasive and unnecessary procedures should be avoided [33]. A recent study showed that CBCT studies can be present with limitations associated with the image resolution (voxel size, focal distance, FOV), artifacts created by filling or restorations, and the possible movement of patients during scanning [34].
CONCLUSIONS
Thus, based on the findings of the present study, it can be concluded that AP is a very common occurrence in the mesiobuccal roots of endodontically treated maxillary molars. The occurrence of 2 canals or foramina increases the risk of untreated canals and presence of AP. Furthermore, the majority of MB2 canals are missed, and only a few of them receive satisfactory treatment.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Carrion SJ, Coelho MS, Frozoni M.
Data curation: Carrion SJ.
Formal analysis: Carrion SJ, Coelho MS, Frozoni M.
Investigation: Carrion SJ.
Project administration: Carrion SJ.
Resources: Carrion SJ.
Supervision: Coelho MS, Frozoni M.
Visualization: Coelho MS, Soares AJ.
Writing - original draft: Coelho MS.
Writing - review & editing: Coelho MS.
- 1. American Association of Endodontists. Treatment standards. updated 2020]. cited May 2, 2022]. Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2018/04/TreatmentStandards_Whitepaper.pdf.
- 2. Yoo YJ, Perinpanayagam H, Oh S, Kim AR, Han SH, Kum KY. Endodontic biofilms: contemporary and future treatment options. Restor Dent Endod 2019;44:e7.ArticlePubMedPMCPDF
- 3. Kulild JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod 1990;16:311-317.ArticlePubMed
- 4. Keskin C, Keleş A, Versiani MA. Mesiobuccal and palatal interorifice distance may predict the presence of the second mesiobuccal canal in maxillary second molars with fused roots. J Endod 2021;47:585-591.ArticlePubMed
- 5. Martins JN, Kishen A, Marques D, Nogueira Leal Silva EJ, Caramês J, Mata A, Versiani MA. Preferred reporting items for epidemiologic cross-sectional studies on root and root canal anatomy using cone-beam computed tomographic technology: a systematized assessment. J Endod 2020;46:915-935.ArticlePubMed
- 6. Martins JN, Alkhawas MA, Altaki Z, Bellardini G, Berti L, Boveda C, Chaniotis A, Flynn D, Gonzalez JA, Kottoor J, Marques MS, Monroe A, Ounsi HF, Parashos P, Plotino G, Ragnarsson MF, Aguilar RR, Santiago F, Seedat HC, Vargas W, von Zuben M, Zhang Y, Gu Y, Ginjeira A. Worldwide analyses of maxillary first molar second mesiobuccal prevalence: a multicenter cone-beam computed tomographic study. J Endod 2018;44:1641-1649.e1.ArticlePubMed
- 7. Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990;16:498-504.ArticlePubMed
- 8. Saini HR, Tewari S, Sangwan P, Duhan J, Gupta A. Effect of different apical preparation sizes on outcome of primary endodontic treatment: a randomized controlled trial. J Endod 2012;38:1309-1315.ArticlePubMed
- 9. Song M, Kim HC, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endod 2011;37:1516-1519.ArticlePubMed
- 10. do Carmo WD, Verner FS, Aguiar LM, Visconti MA, Ferreira MD, Lacerda MF, Junqueira RB. Missed canals in endodontically treated maxillary molars of a Brazilian subpopulation: prevalence and association with periapical lesion using cone-beam computed tomography. Clin Oral Investig 2021;25:2317-2323.ArticlePubMedPDF
- 11. Baruwa AO, Martins JN, Meirinhos J, Pereira B, Gouveia J, Quaresma SA, Monroe A, Ginjeira A. The influence of missed canals on the prevalence of periapical lesions in endodontically treated teeth: a cross-sectional study. J Endod 2020;46:34-39.e1.ArticlePubMed
- 12. Ricucci D, Siqueira JF Jr. Biofilms and apical periodontitis: study of prevalence and association with clinical and histopathologic findings. J Endod 2010;36:1277-1288.ArticlePubMed
- 13. Ricucci D, Siqueira JF Jr, Bate AL, Pitt Ford TR. Histologic investigation of root canal-treated teeth with apical periodontitis: a retrospective study from twenty-four patients. J Endod 2009;35:493-502.ArticlePubMed
- 14. Jang YE, Kim BS, Kim Y. Clinical factors associated with apical periodontitis visible on cone-beam computed tomography but missed with periapical radiographs: a retrospective clinical study. J Endod 2020;46:832-838.ArticlePubMed
- 15. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589-599.ArticlePubMed
- 16. Estrela C, Bueno MR, Azevedo BC, Azevedo JR, Pécora JD. A new periapical index based on cone beam computed tomography. J Endod 2008;34:1325-1331.ArticlePubMed
- 17. Tibúrcio-Machado CS, Michelon C, Zanatta FB, Gomes MS, Marin JA, Bier CA. The global prevalence of apical periodontitis: a systematic review and meta-analysis. Int Endod J 2021;54:712-735.ArticlePubMedPDF
- 18. Chauhan N, Mittal S, Tewari S, Sen J, Laller K. Association of apical periodontitis with cardiovascular disease via noninvasive assessment of endothelial function and subclinical atherosclerosis. J Endod 2019;45:681-690.ArticlePubMed
- 19. Jakovljevic A, Sljivancanin Jakovljevic T, Duncan HF, Nagendrababu V, Jacimovic J, Aminoshariae A, Milasin J, Dummer PM. The association between apical periodontitis and adverse pregnancy outcomes: a systematic review. Int Endod J 2021;54:1527-1537.ArticlePubMedPDF
- 20. Poornima L, Ravishankar P, Abbott PV, Subbiya A, PradeepKumar AR. Impact of root canal treatment on high-sensitivity C-reactive protein levels in systemically healthy adults with apical periodontitis - a preliminary prospective, longitudinal interventional study. Int Endod J 2021;54:501-508.ArticlePubMedPDF
- 21. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation 2002;105:1135-1143.ArticlePubMed
- 22. Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol 1998;8:1558-1564.ArticlePubMedPDF
- 23. Parker JM, Mol A, Rivera EM, Tawil PZ. Cone-beam computed tomography uses in clinical endodontics: observer variability in detecting periapical lesions. J Endod 2017;43:184-187.ArticlePubMed
- 24. Beacham JT, Geist JR, Yu Q, Himel VT, Sabey KA. Accuracy of cone-beam computed tomographic image interpretation by endodontists and endodontic residents. J Endod 2018;44:571-575.ArticlePubMed
- 25. Martins JN, Marques D, Silva EJ, Caramês J, Mata A, Versiani MA. Second mesiobuccal root canal in maxillary molars—a systematic review and meta-analysis of prevalence studies using cone beam computed tomography. Arch Oral Biol 2020;113:104589.ArticlePubMed
- 26. Alaçam T, Tinaz AC, Genç O, Kayaoglu G. Second mesiobuccal canal detection in maxillary first molars using microscopy and ultrasonics. Aust Endod J 2008;34:106-109.ArticlePubMed
- 27. Coelho MS, Parker JM, Tawil PZ. Second mesiobuccal canal treatment in a predoctoral dental clinic: a retrospective clinical study. J Dent Educ 2016;80:726-730.ArticlePubMedPDF
- 28. Parker J, Mol A, Rivera EM, Tawil P. CBCT uses in clinical endodontics: the effect of CBCT on the ability to locate MB2 canals in maxillary molars. Int Endod J 2017;50:1109-1115.PubMed
- 29. Vizzotto MB, Silveira PF, Arús NA, Montagner F, Gomes BP, da Silveira HE. CBCT for the assessment of second mesiobuccal (MB2) canals in maxillary molar teeth: effect of voxel size and presence of root filling. Int Endod J 2013;46:870-876.PubMed
- 30. Costa FF, Pacheco-Yanes J, Siqueira JF Jr, Oliveira AC, Gazzaneo I, Amorim CA, Santos PH, Alves FR. Association between missed canals and apical periodontitis. Int Endod J 2019;52:400-406.ArticlePubMedPDF
- 31. Burry JC, Stover S, Eichmiller F, Bhagavatula P. Outcomes of primary endodontic therapy provided by endodontic specialists compared with other providers. J Endod 2016;42:702-705.ArticlePubMed
- 32. Kruse C, Spin-Neto R, Evar Kraft DC, Vaeth M, Kirkevang LL. Diagnostic accuracy of cone beam computed tomography used for assessment of apical periodontitis: an ex vivo histopathological study on human cadavers. Int Endod J 2019;52:439-450.PubMed
- 33. Kruse C, Spin-Neto R, Wenzel A, Vaeth M, Kirkevang LL. Impact of cone beam computed tomography on periapical assessment and treatment planning five to eleven years after surgical endodontic retreatment. Int Endod J 2018;51:729-737.ArticlePubMedPDF
- 34. Ahmed HM. A critical analysis of laboratory and clinical research methods to study root and canal anatomy. Int Endod J 2022;55(Supplement 2):229-280.ArticlePubMedPDF
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Prevalence of Unfilled MB2 Canals and Their Association with Apical Periodontitis: A CBCT-Based Cross-Sectional Study in a German Population
Maythem Al Fartousi, Christian Ralf Gernhardt
Diagnostics.2026; 16(5): 796. CrossRef - When to perform cone beam computed tomography (CBCT) in primary root canal treatment? A CBCT-based cross-sectional study on the prevalence of MB2 canal in maxillary first molars
Bledar Lilaj, Elias Salzmann, Gernot Paul Hönigl, Rinet Dauti, Anton Dobsak, Sophie Pock, Barbara Cvikl
Dentomaxillofacial Radiology.2026; 55(4): 381. CrossRef - Deep learning–based detection of the second mesiobuccal canal in maxillary first molars using cone-beam computed tomography
Jiao Lin, Jialing Liu, Yuxin Jiang, Yang Liu, Bixin Wen, Shihao Li, Chenglong Li
BMC Oral Health.2026;[Epub] CrossRef - Anatomical Configuration of the MB2 Canal Using High-Resolution Cone-Beam Computed Tomography
Luciana Magrin Blank-Gonçalves, Emmanuel João Nogueira Leal da Silva, Monikelly do Carmo Chagas Nascimento, Ana Grasiela Limoeiro, Luiz Roberto Coutinho Manhães-Jr
Journal of Endodontics.2025; 51(5): 609. CrossRef - The Effect of Age and Gender on the Distance Between the Maxillary Sinus Cortical Bone and Maxillary Molars: A Cone-Beam Tomography Analysis
Thaysa Menezes Constantino, Marília Fagury Videira Marceliano-Alves, Vivian Ronquete, Ana Grasiela da Silva Limoeiro, Pablo Andres Amoroso-Silva, Mariano Simon Pedano, Tchilalo Boukpessi, Fábio Vidal, Thais Machado de Carvalho Coutinho
Sinusitis.2025; 9(1): 9. CrossRef - Retrospective study of the morphology of third maxillary molars among the population of Lower Silesia based on analysis of cone beam computed tomography
Anna Olczyk, Barbara Malicka, Katarzyna Skośkiewicz-Malinowska, Mohmed Isaqali Karobari
PLOS ONE.2024; 19(2): e0299123. CrossRef - Relationship between apical periodontitis and missed canals in mesio-buccal roots of maxillary molars: CBCT study
Badi B. Alotaibi, Kiran I. Khan, Muhammad Q. Javed, Smita D. Dutta, Safia S. Shaikh, Nawaf M. Almutairi
Journal of Taibah University Medical Sciences.2024; 19(1): 18. CrossRef - APICAL PERIODONTITIS IN MAXILLARY MOLARS WITH MISSED SECOND MESIO-BUCCAL ROOT CANAL: A CBCT STUDY
Cristina Coralia Nistor, Ioana Suciu , Ecaterina Ionescu , Anca Dragomirescu , Elena Coculescu , Andreea Baluta
Romanian Journal of Oral Rehabilitation.2024; 16(3): 100. CrossRef - Anatomic Comparison of Contralateral Maxillary Second Molars Using High-Resolution Micro-CT
Ghassan Dandache, Umut Aksoy, Mehmet Birol Ozel, Kaan Orhan
Symmetry.2023; 15(2): 420. CrossRef
 ePub Link
ePub Link Cite
CiteApical periodontitis in mesiobuccal roots of maxillary molars: influence of anatomy and quality of root canal treatment, a CBCT study
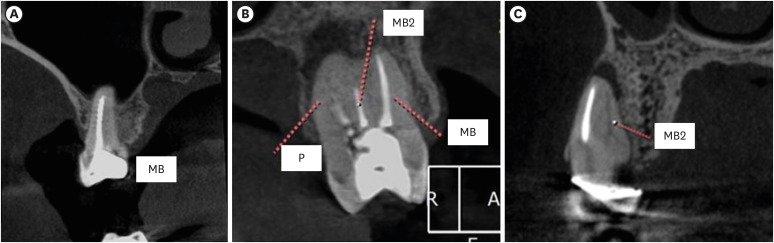
Figure 1 Representative images showing (A) satisfactory filling, (B) satisfactory filling (MB), unsatisfactory (MB2) and (C) Untreated (MB2).MB, mesiobuccal; MB2, second mesiobuccal; P, palatal.
Figure 1
Apical periodontitis in mesiobuccal roots of maxillary molars: influence of anatomy and quality of root canal treatment, a CBCT study
Kappa test showing excellent agreement rate between the observers at different variables
| Observer 1 × 2 | Kappa | Agreement |
|---|---|---|
| No. of canals | 0.897 | Excellent |
| No. of foramina | 0.875 | Excellent |
| Vertucci's classification | 0.860 | Excellent |
| Quality of treatment (MB) | 0.905 | Excellent |
| Quality of treatment (MB2) | 0.897 | Excellent |
| Apical periodontitis classification | 0.830 | Excellent |
Association between the number of foramina and quality of root canal treatment and association between the quality of root canal treatment and the classification of apical periodontitis
| Variable | Quality of root canal treatment | OR (CI) | Total | ||||
|---|---|---|---|---|---|---|---|
| Satisfactory | Unsatisfactory | Untreated | Satisfactory | Untreated | |||
| Foramina | |||||||
| 1 | 352 (45.9) | 269 (35.1) | 146 (19.0) | 0.82 (0.64–1.05) | 3.03 (2.36–3.90) | 767 | |
| 2 | 271 (34.7) | 170 (21.7) | 341 (43.6) | 782 | |||
| Total | 623 | 439 | 487 | 1,549 | |||
| Apical periodontitis | |||||||
| 0 | 310 (45.5) | 188 (27.6) | 183 (26.9) | Ref. | Ref. | 681 | |
| 1 | 61 (36.5) | 58 (34.7) | 48 (28.7) | 1.57 (1.05–2.34) | 0.75 (0.49–1.14) | 167 | |
| 2 | 95 (35.4) | 79 (29.5) | 94 (35.1) | 1.37 (0.97–1.94) | 1.68 (1.19–2.35) | 268 | |
| 3 | 75 (32.9) | 58 (25.4) | 95 (41.7) | 1.28 (0.87–1.88) | 2.15 (1.51–3.06) | 228 | |
| 4 | 14 (32.6) | 14 (32.6) | 15 (34.8) | 1.65 (0.77–1.55) | 1.82 (0.86–3.85) | 43 | |
| 5 | 1 (33.3) | 1 (33.3) | 1 (33.3) | - | - | 3 | |
| D | 67 (42.1) | 41 (25.8) | 51 (32.1) | 1.01 (0.66–1.55) | 1.29 (0.86–1.94) | 159 | |
| Total | 623 | 439 | 487 | 1,549 | |||
Values are presented as number (%).
OR, odds ratio; CI, confidence interval.
Absolute number (percentage) of the quality of root canal treatment and prevalence of apical periodontitis in its different classifications
| Variable | Quality of root canal treatment (MB1) | Total | Quality of root canal treatment (MB2) | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| Satisfactory | Unsatisfactory | Untreated | Satisfactory | Unsatisfactory | Untreated | ||||
| Foramina | |||||||||
| 1 | 332 (54.7) | 253 (41.7) | 22 (3.6) | 607 | 20 (12.5) | 16 (10.0) | 124 (77.5) | 160 | |
| 2 | 237 (60.3) | 140 (35.6) | 16 (4.1) | 393 | 34 (8.7) | 30 (7.7) | 325 (83.5) | 389 | |
| Total | 569 | 393 | 38 | 1,000 | 54 | 46 | 449 | 549 | |
| Apical periodontitis | |||||||||
| 0 | 284 (60.9) | 165 (35.4) | 17 (3.7) | 466 | 26 (12.1) | 23 (10.7) | 166 (77.2) | 215 | |
| 1 | 55 (49.5) | 54 (48.6) | 2 (1.8) | 111 | 6 (10.7) | 4 (7.1) | 46 (82.1) | 56 | |
| 2 | 90 (53.6) | 70 (41.7) | 8 (4.7) | 168 | 5 (5.0) | 9 (9.0) | 86 (86.0) | 100 | |
| 3 | 70 (53.4) | 55 (42.0) | 6 (4.6) | 131 | 5 (5.2) | 3 (3.1) | 89 (91.7) | 97 | |
| 4 | 13 (52.0) | 12 (48.0) | 0 (0.0) | 25 | 1 (5.6) | 2 (11.1) | 15 (83.3) | 18 | |
| 5 | 1 (50.0) | 1 (50.0) | 0 (0.0) | 2 | 0 (0.0) | 0 (0.0) | 1 (100.0) | 1 | |
| D | 56 (57.7) | 36 (37.1) | 5 (5.2) | 97 | 11 (17.7) | 5 (8.1) | 46 (74.2) | 62 | |
| Total | 569 | 393 | 38 | 1,000 | 54 | 46 | 449 | 549 | |
Association between the number of canals, foramens and Vertucci’s classification with the classification of apical periodontitis
| Variable | Apical periodontitis classification | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | D | |||
| Canals | |||||||||
| 1 | 251 (55.7) | 55 (12.2) | 68 (15.1) | 34 (7.5) | 7 (1.6) | 1 (0.2) | 35 (7.8) | 451 | |
| 2 | 215 (39.2) | 56 (10.2) | 100 (18.2) | 97 (17.7) | 18 (3.3) | 1 (0.2) | 62 (11.3) | 549 | |
| Total | 466 | 111 | 168 | 131 | 25 | 2 | 97 | 1,000 | |
| OR (CI) | Ref. | 0.84 (0.56–1.27) | 1.72 (1.20–2.46) | 3.33 (2.16–5.13) | 3.00 (1.23–7.32) | - | 2.07 (1.32–3.26) | ||
| Foramina | |||||||||
| 1 | 333 (54.9) | 70 (11.5) | 87 (14.3) | 56 (9.2) | 10 (1.6) | 1 (0.2) | 50 (8.2) | 607 | |
| 2 | 133 (33.8) | 41 (10.4) | 81 (20.6) | 75 (19.1) | 15 (3.8) | 1 (0.3) | 47 (12.0) | 393 | |
| Total | 466 | 111 | 168 | 131 | 25 | 2 | 97 | 1,000 | |
| OR (CI) | Ref. | 0.68 (0.44–1.05) | 1.47 (0.95–2.27) | 2.33 (1.62–3.35) | 3.76 (1.65–8.57) | - | 2.35 (1.51–3.68) | ||
| Vertucci's classification | |||||||||
| Type I | 250 (55.9) | 55 (12.3) | 67 (15.0) | 33 (7.4) | 7 (1.6) | 1 (0.2) | 34 (7.6) | 447 | |
| Type II | 82 (51.6) | 15 (9.4) | 20 (12.6) | 23 (14.5) | 3 (1.9) | 0 (0.0) | 16 (10.1) | 159 | |
| Type III | 1 (100.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 | |
| Type IV | 131 (33.9) | 41 (10.6) | 80 (20.7) | 74 (19.1) | 15 (3.9) | 1 (0.3) | 45 (11.6) | 387 | |
| Type VI | 2 (33.3) | 0 (0.0) | 1 (16.7) | 1 (16.7) | 0 (0.0) | 0 (0.0) | 2 (33.3) | 6 | |
| Total | 466 | 111 | 168 | 131 | 25 | 2 | 97 | 1,000 | |
Values are presented as number (%). Bold numbers indicate positive association between the variables.
OR, odds ratio; CI, confidence interval.
Table 1 Kappa test showing excellent agreement rate between the observers at different variables
Table 2 Association between the number of foramina and quality of root canal treatment and association between the quality of root canal treatment and the classification of apical periodontitis
Values are presented as number (%).
OR, odds ratio; CI, confidence interval.
Table 3 Absolute number (percentage) of the quality of root canal treatment and prevalence of apical periodontitis in its different classifications
Table 4 Association between the number of canals, foramens and Vertucci’s classification with the classification of apical periodontitis
Values are presented as number (%). Bold numbers indicate positive association between the variables.
OR, odds ratio; CI, confidence interval.

