
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 47(4); 2022 > Article
- Case Report Endodontic micro-resurgery and guided tissue regeneration of a periapical cyst associated to recurrent root perforation: a case report
-
Fernando Córdova-Malca1
 , Hernán Coaguila-Llerena2, Lucía Garré-Arnillas3, Jorge Rayo-Iparraguirre3, Gisele Faria2
, Hernán Coaguila-Llerena2, Lucía Garré-Arnillas3, Jorge Rayo-Iparraguirre3, Gisele Faria2 -
Restor Dent Endod 2022;47(4):e35.
DOI: https://doi.org/10.5395/rde.2022.47.e35
Published online: September 3, 2022
1Department of Endodontics, Cayetano Heredia Peruvian University (UPCH), Lima, Peru.
2Department of Restorative Dentistry, Araraquara School of Dentistry, São Paulo State University (UNESP), Araraquara, SP, Brazil.
3Academic Department of Stomatological Clinic, Cayetano Heredia Peruvian University (UPCH), Lima, Peru.
- Correspondence to Hernán Coaguila-Llerena, DDS, MSc. PhD Student, Department of Restorative Dentistry, Araraquara School of Dentistry, São Paulo State University (UNESP), Rua Humaitá 1680, Araraquara, SP 14801-903, Brazil. ehernanco@gmail.com
• Received: March 1, 2022 • Revised: April 8, 2022 • Accepted: May 22, 2022
Copyright © 2022. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Although the success rates of microsurgery and micro-resurgery are very high, the influence of a recurrent perforation combined with radicular cyst remains unclear. A 21-year-old white female patient had a history of root perforation in a previously treated right maxillary lateral incisor. Analysis using cone-beam computed tomography (CBCT) revealed an extensive and well-defined periapical radiolucency, involving the buccal and palatal bone plate. The perforation was sealed with bioceramic material (Biodentine) in the pre-surgical phase. In the surgical phase, guided tissue regeneration (GTR) was performed by combining xenograft (lyophilized bovine bone) and autologous platelet-rich fibrin applied to the bone defect. The root-end preparation was done using an ultrasonic tip. The retrograde filling was performed using a bioceramic material (Biodentine). Histopathological analysis confirmed a radicular cyst. The patient returned to her referring practitioner to continue the restorative procedures. CBCT analysis after 1-year recall revealed another perforation in the same place as the first intervention, ultimately treated by micro-resurgery using the same protocol with GTR, and a bioceramic material (MTA Angelus). The 2-year recall showed healing and bone neoformation. In conclusion, endodontic micro-resurgery with GTR showed long-term favorable results when a radicular cyst and a recurrent perforation compromised the success.
INTRODUCTION
Microorganisms in the root canal system are the main agents of persistent periapical lesions. Among large periapical lesions, radicular cysts may have their lumen with bacteria organized as biofilms [1]. Additionally, true cysts are considered self-sustainable and persist regardless of removing microbiological stimulation within the canal, which suggests a surgical approach [2].
Endodontic microsurgery is a minimally invasive procedure that combines the magnification and illumination provided by an operating microscope (OP), with proper use of micro-instruments. This procedure improves the visualization and manipulation of delicate structures [3,4]. A study revealed that the success rate of endodontic microsurgery is 94%, compared with an 88% rate for conventional surgery without OP [5]. On the other hand, the success rate of micro-resurgery has been reported as being between 87.6% and 92.9% [6,7]. Although the success rates of microsurgery and micro-resurgery are very high, the influence of a recurrent perforation combined with radicular cyst remains unclear.
Bone defects after apicoectomy are commonly large and complicated, as a consequence of large apical lesions, endoperiodontal lesions, and through-and-through lesions [8]. The guided tissue regeneration (GTR) technique has been proposed to complement endodontic surgery as a way to promote bone healing [9]. Usually, membrane barriers and/or bone grafting materials are used to prevent epithelial and gingival connective tissue from proliferating to the apical surface, and to delay the growth of both periodontal cells and the bone in bone defects [10].
Root canal perforations are artificial, and commonly iatrogenic communications between the root canal and the supporting tissues of the teeth or the oral cavity [11]. Iatrogenic pathological perforations can occur when preparing an access cavity, during instrumentation, or post preparation. The prognosis will depend on time, size, location and bacterial contamination [11,12,13,14]. This case report discusses the management of a dental periapical cyst combined with recurrent iatrogenic perforation, whose treatment involved microsurgery and micro-resurgery, accompanied by GTR.
CASE REPORT
A 21-year-old white female patient was referred for endodontic evaluation of the right maxillary lateral incisor. The medical history of the patient was non-contributory. The dental history included a root canal treatment of the referred tooth 5 years prior, and a recent post preparation with an apparent perforation by the referring colleague. The clinical examination showed sensitivity to percussion and palpation, and slight intraoral swelling. Radiographic examination revealed post preparation and enlargement of the root canal at the middle third, adjacent to the obturation material (Figure 1A). In addition, the tooth was associated with a large well-defined periapical lesion and corticalized rim. The cone-beam computed tomography (CBCT) (Planmeca ProMax 3D Classic, Planmeca, Helsinki, Finland) analysis revealed that the periapical lesion (1.3 × 1.5 × 1.3 cm) had compromised both buccal and palatal cortical plates, and that the root perforation extended along the middle third up to the apical third (Figure 1B and 1C). The pre-treatment diagnosis was “previously treated” and “symptomatic apical periodontitis”; however, acute apical abscess was also considered for differential diagnosis because of the slight intraoral swelling. The treatment alternatives were discussed with the patient, who consented to perform surgical retreatment and sealing of the perforation, as well as to have her case published in the scientific literature.
Figure 1
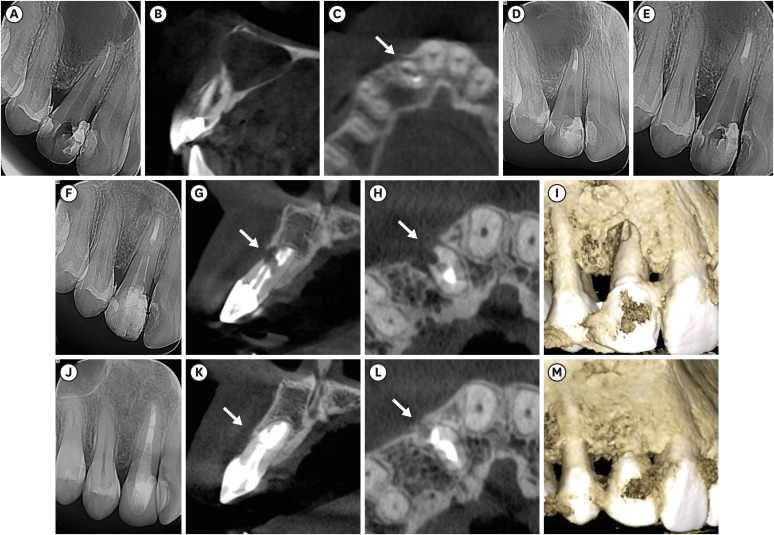
Chronological radiographs and CBCT images of the case management. Preoperative radiograph (A). Sagittal plane of a CBCT image, confirming that the cyst compromised buccal and palatal bone plates (B). Axial plane of a CBCT image, confirming the first perforation. The white arrow indicates the perforation (C). Immediate post-surgical radiograph (D). Periapical radiographs after 1 month and 1 year, respectively. As can be observed, the cyst is apparently decreasing in size (E, F). Sagittal and axial planes of CBCT images, confirming the second perforation, respectively. The white arrows indicate the perforation (G, H). Three-dimensional CBCT reconstruction. The buccal bone plate is clearly affected (I). Periapical radiograph 2 years after micro-resurgery (J). Sagittal and axial planes of CBCT images 2 years after micro-resurgery, confirming new bone formation—white arrows (K, L). Three-dimensional CBCT reconstruction 2 years after micro-resurgery (M).
CBCT, cone-beam computed tomography.
All procedures were performed using the OP (MC-M3101, DF Vasconcellos, Valença, RJ, Brazil). During the pre-surgical phase, local anesthesia was administered before rubber dam isolation, and consisted of oral infiltration of 2% lidocaine with 1:100,000 adrenaline (Alphacaine, Rio de Janeiro, RJ, Brazil), followed by rinsing with 0.12% chlorhexidine. After isolation, access was obtained, and the perforation site was identified and gauged as approximately 2–3 mm in diameter (Figure 2A). A piece of polytetrafluoroethylene (Teflon) was placed in the perforation provisionally to allow the removal of the obturation material, which was achieved with a 25.06 file from the K3XF system (Kerr Endodontics, Brea, CA, USA), and complemented by the Twisted File Adaptive System (Kerr Endodontics) up to 50/.04 file. The residual obturation material in the apical portion was removed with Hedström files up to ISO size 50. The working length was determined using an apex locator (Root ZX 2, J Morita Corp., Osaka, Japan), and confirmed radiographically. In addition, a gutta-percha cone was placed in the perforation to confirm its trajectory. The irrigation protocol was performed with 2.5% sodium hypochlorite, using a 30G side-vented needle at each file change (Endo-Eze, Ultradent Products, South Jordan, UT, USA). The final irrigation was performed with 17% ethylenediaminetetraacetic acid (Biodinâmica, Ibiporã, PR, Brazil), 2.5% sodium hypochlorite, and distilled water. The root canal was then dried with paper points, and obturated with gutta-percha cones and pulp canal sealer (Kerr Endodontics), using the continuous wave technique (System B Cordless, Kerr Endodontics). Afterwards, the provisional Teflon was removed to resume the perforation repair, which was performed using a bioceramic material (Biodentine, Septodont, Saint-Maur-des-Fossés, France). The access cavity was sealed with glass ionomer cement (Fuji IX GP Fast; GC Corporation, Tokyo, Japan). The patient was asked to undergo a complete blood count and bleeding time test for platelet-rich fibrin (PRF) preparation during the surgical phase.
Figure 2
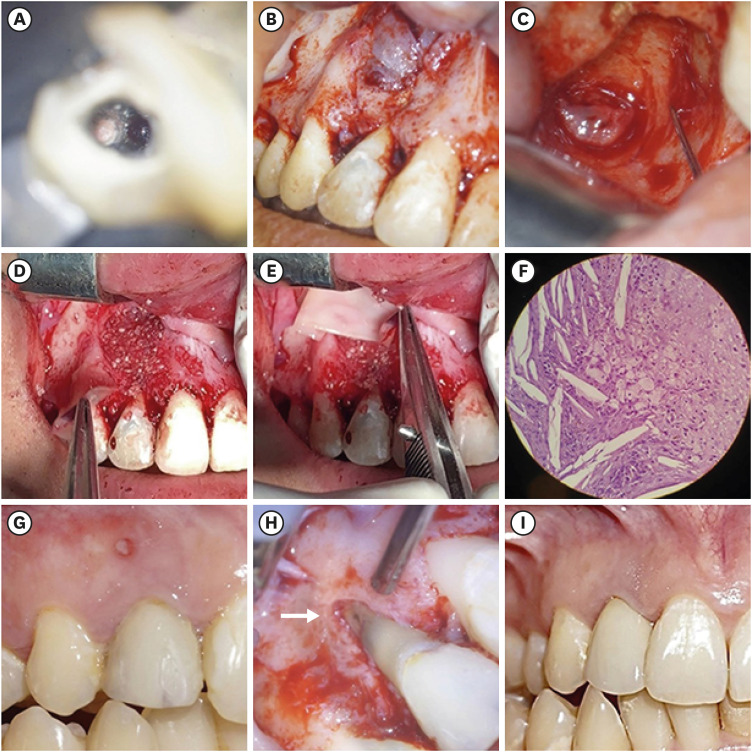
Chronological, illustrative images of the case management. A root canal perforation can be observed in the buccal root surface of the right maxillary lateral incisor, 13× OP magnification (A). The cyst involving the buccal bone plate can be observed during the surgical phase, 5× OP magnification (B). Clinical appearance after cyst removal, where it can be observed that both buccal and palatal bone plates were compromised, 13× OP magnification (C). Application of lyophilized bovine bone and autologous platelet-rich fibrin into the bone defect, 5× OP magnification (D, E). Histopathological image (original magnification ×400) of the removed tissue showing cholesterol crystals, confirming the presence of a radicular cyst (F). Intraoral photograph 1 year after first microsurgery; a sinus tract appeared and was associated with the treated tooth (G). Clinical appearance of the second perforation in the buccal root surface of the affected tooth—white arrow, 8× OP magnification (H). Intraoral photograph 2 years after micro-resurgery. The tooth was restored with a crown (I).
OP, operating microscope.
The PRF membranes were prepared a week later, prior to the surgical phase, given the normal values found for the complete blood count and bleeding time. Blood samples were collected from the patient without using an anticoagulant, by taking three 6 mL tubes that were immediately centrifuged at 3,000 rpm (800D, Hiprove, Jiangsu, China) for 10 minutes [15]. The fibrin clots were removed from the middle of the tube with sterile tweezers, and then stored in a PRF box (Process, Nice, France). Three PRF membranes were obtained from the clots, which were used at the end of the surgical phase.
The surgical phase began by applying anesthesia, consisting of an oral infiltration of 4% articaine hydrochloride with 1:100,000 epinephrine (Articaine, DFL, St. Paul, MN, USA), followed by rinsing with 0.12% chlorhexidine. A sulcular incision was made from the right maxillary second premolar to the left maxillary second premolar, and an envelope flap was lifted without opening the incisions. The osteotomy was performed using a 04-carbide drill (Angelus, Londrina, PR, Brazil), under constant irrigation with saline solution (Figure 2B). The lesion was removed for subsequent histological analysis (Figure 2C). The apicoectomy was performed by removing the apical 3 mm of root, using a high-speed cutting bur, followed by staining with methylene blue to rule out the presence of fissures, and to confirm the root configuration. The root-end preparation was performed with an ultrasonic tip (P1M, Helse Ultrasonic, Santa Rosa de Viterbo, SP, Brazil) coupled to a piezoelectric ultrasonic device (MiniEndo, Kerr Endodontics). The retrograde filling was performed using a bioceramic material (Biodentine, Septodont). The bone defects were filled sequentially with approximately 1 g of lyophilized bovine bone (Bio-Oss, Geistlich Pharma AG, Wolhusen, Switzerland), and the previously obtained PRF membranes (Figure 2D and 2E). The flap was repositioned and closed using 6-0 polydioxanone sutures (Tagum, Tagumedica S.A., Lima, Peru) and a post-surgical radiograph was taken (Figure 1D). The 1-month follow-up showed that the patient felt comfortable, and that the surgical area was healing (Figure 1E). The histopathological examination confirmed a radicular cyst (Figure 2F). The patient returned to her referring dentist to continue the restorative procedures, which included the placement of a post and composite restoration. The patient was asked to return for the 3, 6-month, and 1-year follow-ups.
The patient failed to attend the 3- and 6-month recall appointments for personal reasons, and returned after 1 year, at which time a sinus tract was identified in the same area, associated with the treated tooth (Figure 2G). The radiographic examination revealed that the radicular cyst was healing (Figure 1F), but there was clinical evidence of microsurgery failure in the area of the perforation. Since this finding could not be confirmed by radiographic examination, a tomographic examination was recommended. The CBCT analysis showed that there was a new perforation made by her referred dentist during post preparation at the previously operated site, and that the bioceramic material had been removed iatrogenically (Figure 1G-1I). After obtaining the patient’s consent, a micro-resurgery was planned in the area of the perforation, with the same anesthesia protocol, flap design, and osteotomy as the previously performed procedure (Figure 2H). Bioceramic material (MTA Angelus, Angelus) was placed in the perforation, followed by about 0.25 g of lyophilized bovine bone (Bio-Oss) and PRF membranes. The 1- and 2-week recalls showed favorable evolution, and a crown was placed on the affected tooth. After 2 years, the clinical, radiographic and tomographic examinations showed that the cyst had healed, that there was newly formed bone in the perforation area, and that the evolution was progressing uneventfully (Figure 1J-1M, Figure 2I). The tooth was fitted with a new post and crown (Figure 2I).
This case report has been written according to Preferred Reporting Items for Case reports in Endodontics (PRICE) 2020 guidelines [16] (Figure 3).
Figure 3
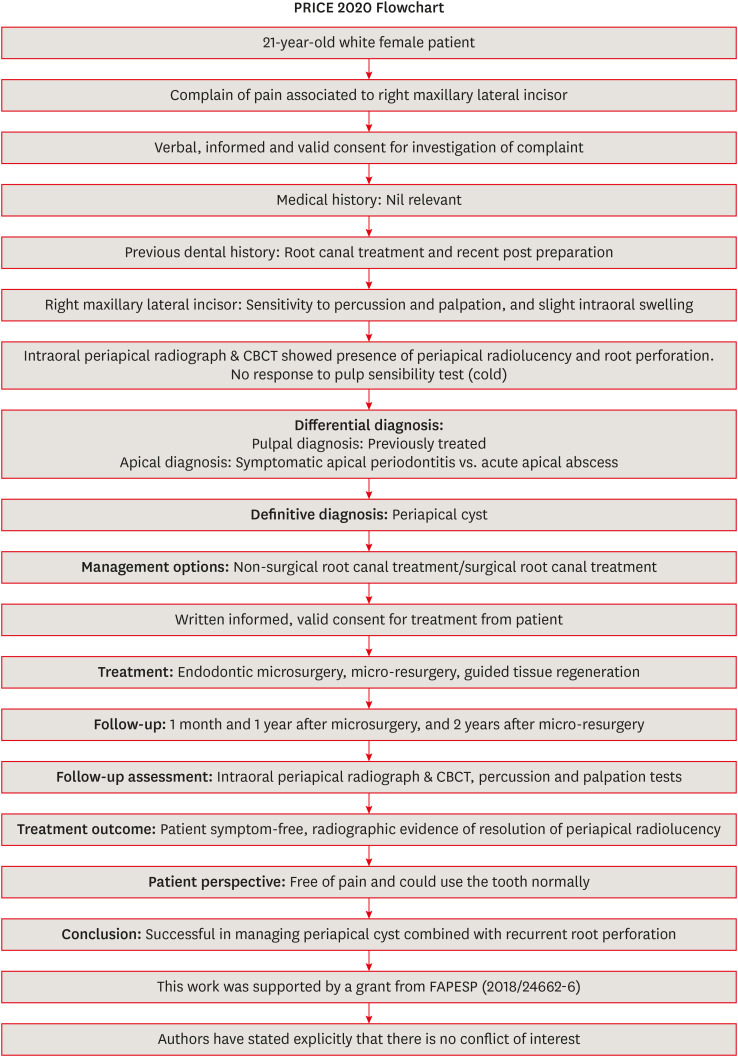
This flow chart was adopted from PRICE 2020 guidelines for reporting case reports in endodontics [16]. For further details visit: http://pride-endodonticguidelines.org/price/.
CBCT, cone-beam computed tomography.
DISCUSSION
Contemporary microsurgery and micro-resurgery should be performed with an OP, and both methods have shown high success rates [5,6,7]. An inadequate root-end preparation, and no retrograde filling have been associated with failure of primary surgery, which then requires micro-resurgery [7]. A study revealed that the success rate of primary microsurgery and micro-resurgery is 91.6% and 87.6%, respectively, and that the only failure factor of micro-resurgery is the tooth type, pointing out that molars are the dental element most vulnerable to failure [6]. Likewise, another study reported that anterior teeth had a better success rate than posterior teeth [17]. However, the maxillary lateral incisors have been reported as the anterior teeth most prone to failure and developing periapical lesions, as shown in the present case report [18]. It is important to note that failure of the first microsurgery was due to recurrent perforation of the previously operated site, and that the bioceramic material had been removed iatrogenically.
Xenograft material (Bio-Oss) and a PRF membrane were used to promote the GTR. The ideal bone graft should induce osteogenesis, allow cementogenesis, and facilitate formation of a functional periodontal ligament [19]. The xenograft materials are reabsorbed very slowly, and are osteoconductive [20]. Scientific evidence is divergent, since there is no consensus on the benefits of these materials for hard tissue healing [21,22,23]. However, when both buccal and palatal bone plates are compromised (through-and-through lesion), the GTR combined with a xenograft can have a positive effect on bone healing [21]. It is important to consider that the simple placing of a barrier (membrane and/or bone grafting material) does not necessarily result in the complete regeneration of the tissues [9]. Recent evidence indicates that the use of a PRF membrane has no major favorable effect on the repair of bone defects, hence on the outcome [24,25]. However, patients undergoing periapical surgery present with discomfort, swelling, and chewing problems and pain [26]. Regarding this, the use of a PRF membrane may play an important role in controlling inflammation [27]. A study showed that there was no significant difference whether or not PRF membranes were applied in periapical surgeries regarding postoperative pain after 1 week [28]. However, the authors of that study observed that there was also a high variability of pain perception in the control group, and hypothesized that the PRF membranes may have reduced the perception of severe pain.
One critical aspect to be considered in the present case is that the same operator should have performed the post placement after the first microsurgery to avoid a recurrent perforation; however, the patient was referred by another colleague, who continued the restorative procedures. As a consequence, the patient underwent 2 recurrent iatrogenic root perforations of medium size (2–3 mm in diameter) in the middle third, an unfavorable confluence leading to an outcome marked by damaged tissue, and chances of infection and leakage [14]. However, one of the factors influencing prognosis is the fast response to administer treatment, since a shorter response time favors healing, as occurred in the first surgical intervention of the study [11]. Unfortunately, a second perforation was detected in the same location after 1 year; however, the fact that both perforations occurred in the middle third may have affected the ultimate success of the procedure favorably [11,14]. Furthermore, both surgical interventions used bioceramic materials such as MTA and Biodentine, which promote an adequate seal and favor the repair of periodontal tissues [13,29,30]. For micro-resurgery, considering the intimate contact with oral fluids, MTA was used instead of Biodentine, considering the high solubility of the latter [31].
CONCLUSIONS
Endodontic micro-resurgery showed long-term favorable results when a radicular cyst and a recurrent perforation compromised the endodontic success. The GTR allowed an adequate resolution of the case.
-
Funding: This research was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (grant number 18/24662-6).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Córdova-Malca F, Coaguila-Llerena H.
Funding acquisition: Coaguila-Llerena H.
Methodology: Córdova-Malca F, Coaguila-Llerena H, Garré-Arnillas L, Rayo-Iparraguire J.
Resources: Córdova-Malca F, Garré-Arnillas L.
Supervision: Faria G.
Visualization: Córdova-Malca F, Coaguila-Llerena H, Garré-Arnillas L, Rayo-Iparraguire J, Faria G.
Writing - original draft: Córdova-Malca F, Coaguila-Llerena H, Garré-Arnillas L, Rayo-Iparraguire J, Faria G.
Writing - review & editing: Córdova-Malca F, Coaguila-Llerena H, Garré-Arnillas L, Rayo-Iparraguire J, Faria G.
- 1. Ricucci D, Siqueira JF Jr, Lopes WS, Vieira AR, Rôças IN. Extraradicular infection as the cause of persistent symptoms: a case series. J Endod 2015;41:265-273.ArticlePubMed
- 2. Nair PN. New perspectives on radicular cysts: Do they heal? Int Endod J 1998;31:155-160.ArticlePubMed
- 3. Floratos S, Kim S. Modern endodontic microsurgery concepts: a clinical update. Dent Clin North Am 2017;61:81-91.PubMed
- 4. Niemczyk SP. Essentials of endodontic microsurgery. Dent Clin North Am 2010;54:375-399.ArticlePubMed
- 5. Setzer FC, Kohli MR, Shah SB, Karabucak B, Kim S. Outcome of endodontic surgery: a meta-analysis of the literature--Part 2: comparison of endodontic microsurgical techniques with and without the use of higher magnification. J Endod 2012;38:1-10.ArticlePubMed
- 6. Kim D, Kim S, Song M, Kang DR, Kohli MR, Kim E. Outcome of endodontic micro-resurgery: retrospective study based on propensity score–matched survival analysis. J Endod 2018;44:1632-1640.PubMed
- 7. Song M, Shin SJ, Kim E. Outcomes of endodontic micro-resurgery: a prospective clinical study. J Endod 2011;37:316-320.ArticlePubMed
- 8. Yoshikawa G, Murashima Y, Wadachi R, Sawada N, Suda H. Guided bone regeneration (GBR) using membranes and calcium sulphate after apicectomy: a comparative histomorphometrical study. Int Endod J 2002;35:255-263.ArticlePubMed
- 9. Lin L, Chen MY, Ricucci D, Rosenberg PA. Guided tissue regeneration in periapical surgery. J Endod 2010;36:618-625.ArticlePubMed
- 10. Rankow HJ, Krasner PR. Endodontic applications of guided tissue regeneration in endodontic surgery. Oral Health 1996;86:33-35.Article
- 11. Tsesis I, Fuss Z. Diagnosis and treatment of accidental root perforations. Endod Topics 2006;13:95-107.Article
- 12. Estrela C, Decurcio DA, Rossi-Fedele G, Silva JA, Guedes OA, Borges ÁH. Root perforations: a review of diagnosis, prognosis and materials. Braz Oral Res 2018;32:e73.ArticlePubMed
- 13. Nakata TT, Bae KS, Baumgartner JC. Perforation repair comparing mineral trioxide aggregate and amalgam using an anaerobic bacterial leakage model. J Endod 1998;24:184-186.ArticlePubMed
- 14. Fuss Z, Trope M. Root perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol 1996;12:255-264.ArticlePubMed
- 15. Silberman JJ, Moldauer BI, Torres J, Gallardo C, Sanabria-Liviac D. Palatal root surgery of a maxillary molar using a piezosurgery transantral approach with simultaneous sinus lift grafting: a case report. Int Endod J 2021;54:464-475.ArticlePubMedPDF
- 16. Nagendrababu V, Chong BS, McCabe P, Shah PK, Priya E, Jayaraman J, Pulikkotil SJ, Setzer FC, Sunde PT, Dummer PM. PRICE 2020 guidelines for reporting case reports in endodontics: a consensus-based development. Int Endod J 2020;53:619-626.ArticlePubMedPDF
- 17. Pallarés-Serrano A, Glera-Suarez P, Tarazona-Alvarez B, Peñarrocha-Diago M, Peñarrocha-Diago M, Peñarrocha-Oltra D. Prognostic factors after endodontic microsurgery: a retrospective study of 111 cases with 5 to 9 years of follow-up. J Endod 2021;47:397-403.ArticlePubMed
- 18. Çalışkan MK, Kaval ME, Tekin U, Ünal T. Radiographic and histological evaluation of persistent periapical lesions associated with endodontic failures after apical microsurgery. Int Endod J 2016;49:1011-1019.ArticlePubMed
- 19. Trasatti C, Spears R, Gutmann JL, Opperman LA. Increased Tgf-β1 production by rat osteoblasts in the presence of PepGen P-15 in vitro . J Endod 2004;30:213-217.PubMed
- 20. Bashutski JD, Wang HL. Periodontal and endodontic regeneration. J Endod 2009;35:321-328.ArticlePubMed
- 21. Taschieri S, Del Fabbro M, Testori T, Saita M, Weinstein R. Efficacy of guided tissue regeneration in the management of through-and-through lesions following surgical endodontics: a preliminary study. Int J Periodontics Restorative Dent 2008;28:265-271.PubMed
- 22. Taschieri S, Del Fabbro M, Testori T, Weinstein R. Efficacy of xenogeneic bone grafting with guided tissue regeneration in the management of bone defects after surgical endodontics. J Oral Maxillofac Surg 2007;65:1121-1127.ArticlePubMed
- 23. Dietrich T, Zunker P, Dietrich D, Bernimoulin JP. Periapical and periodontal healing after osseous grafting and guided tissue regeneration treatment of apicomarginal defects in periradicular surgery: results after 12 months. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:474-482.ArticlePubMed
- 24. Dhiman M, Kumar S, Duhan J, Sangwan P, Tewari S. Effect of platelet-rich fibrin on healing of apicomarginal defects: a randomized controlled trial. J Endod 2015;41:985-991.ArticlePubMed
- 25. Karan NB, Aricioğlu B. Assessment of bone healing after mineral trioxide aggregate and platelet-rich fibrin application in periapical lesions using cone-beam computed tomographic imaging. Clin Oral Investig 2020;24:1065-1072.ArticlePubMedPDF
- 26. Christensen CE, McNeal SF, Eleazer P. Effect of lowering the pH of sodium hypochlorite on dissolving tissue in vitro . J Endod 2008;34:449-452.PubMed
- 27. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, Gogly B. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part III: leucocyte activation: a new feature for platelet concentrates? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:e51-e55.ArticlePubMed
- 28. Soto-Peñaloza D, Peñarrocha-Diago M, Cervera-Ballester J, Peñarrocha-Diago M, Tarazona-Alvarez B, Peñarrocha-Oltra D. Pain and quality of life after endodontic surgery with or without advanced platelet-rich fibrin membrane application: a randomized clinical trial. Clin Oral Investig 2020;24:1727-1738.ArticlePubMedPDF
- 29. Makhlouf M, Zogheib C, Makhlouf AC, Kaloustian MK, El Hachem C, Habib M. Sealing ability of calcium silicate-based materials in the repair of furcal perforations: a laboratory comparative study. J Contemp Dent Pract 2020;21:1091-1097.ArticlePubMed
- 30. da Fonseca TS, Silva GF, Guerreiro-Tanomaru JM, Delfino MM, Sasso-Cerri E, Tanomaru-Filho M, Cerri PS. Biodentine and MTA modulate immunoinflammatory response favoring bone formation in sealing of furcation perforations in rat molars. Clin Oral Investig 2019;23:1237-1252.ArticlePubMedPDF
- 31. Coaguila-Llerena H, Ochoa-Rodriguez VM, Castro-Núñez GM, Faria G, Guerreiro-Tanomaru JM, Tanomaru-Filho M. Physicochemical properties of a bioceramic repair material - BioMTA. Braz Dent J 2020;31:511-515.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Outcome of endodontic micro-resurgery: A systematic review
Faisal Alnassar, Riyadh Alroomy, Qamar Hashem, Abdullah Alqedairi, Nabeel Almotairy
Saudi Endodontic Journal.2025; 15(2): 112. CrossRef - Platelet-Rich Plasma and Platelet-Rich Fibrin in Endodontics: A Scoping Review
Simão Rebimbas Guerreiro, Carlos Miguel Marto, Anabela Paula, Joana Rita de Azevedo Pereira, Eunice Carrilho, Manuel Marques-Ferreira, Siri Vicente Paulo
International Journal of Molecular Sciences.2025; 26(12): 5479. CrossRef - Non-surgical Approach to a Maxillary Cyst-Like Lesion: Orthograde Endodontic Treatment With Neodymium-Doped Yttrium Aluminum Garnet (Nd:YAG) Decontamination of the Canal System
Beatrice Spaggiari, Paolo Vescovi, Silvia Pizzi, Roberta Iaria, Ilaria Giovannacci
Cureus.2025;[Epub] CrossRef - Persistent Periradicular Lesion Associated With Concurrent Root Fracture and Odontogenic Keratocyst: A Case Report
Mehdi Vatanpour, Fatemeh Rezaei
Clinical Case Reports.2025;[Epub] CrossRef - Management of Apico-marginal Defects With Endodontic Microsurgery and Guided Tissue Regeneration: A Report of Thirteen Cases
Abayomi O. Baruwa, Jorge N.R. Martins, Mariana D. Pires, Beatriz Pereira, Pedro May Cruz, António Ginjeira
Journal of Endodontics.2023; 49(9): 1207. CrossRef
 ePub Link
ePub Link Cite
CiteEndodontic micro-resurgery and guided tissue regeneration of a periapical cyst associated to recurrent root perforation: a case report
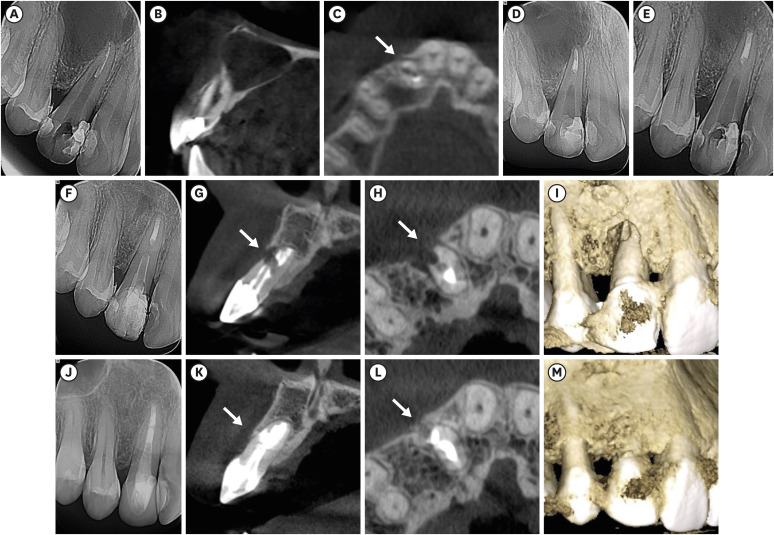
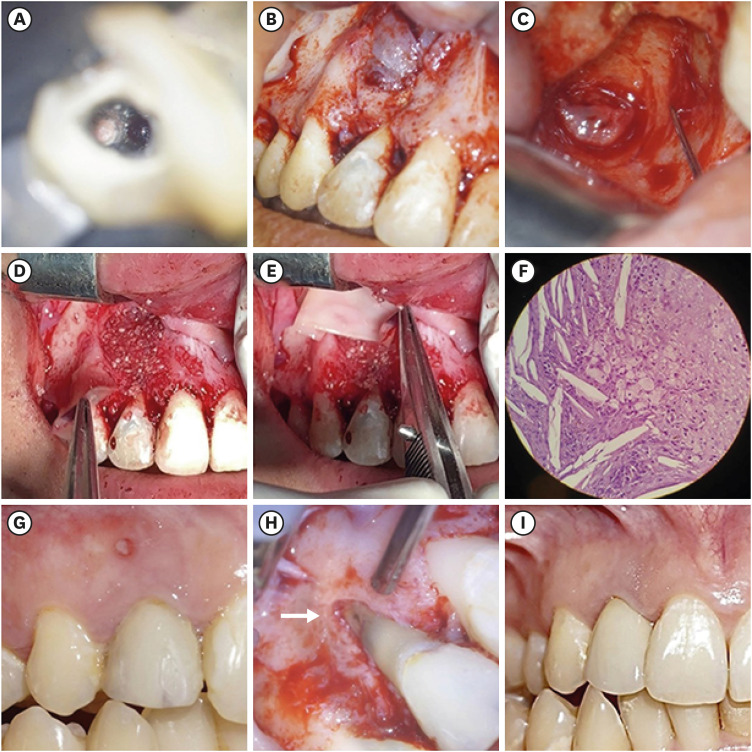
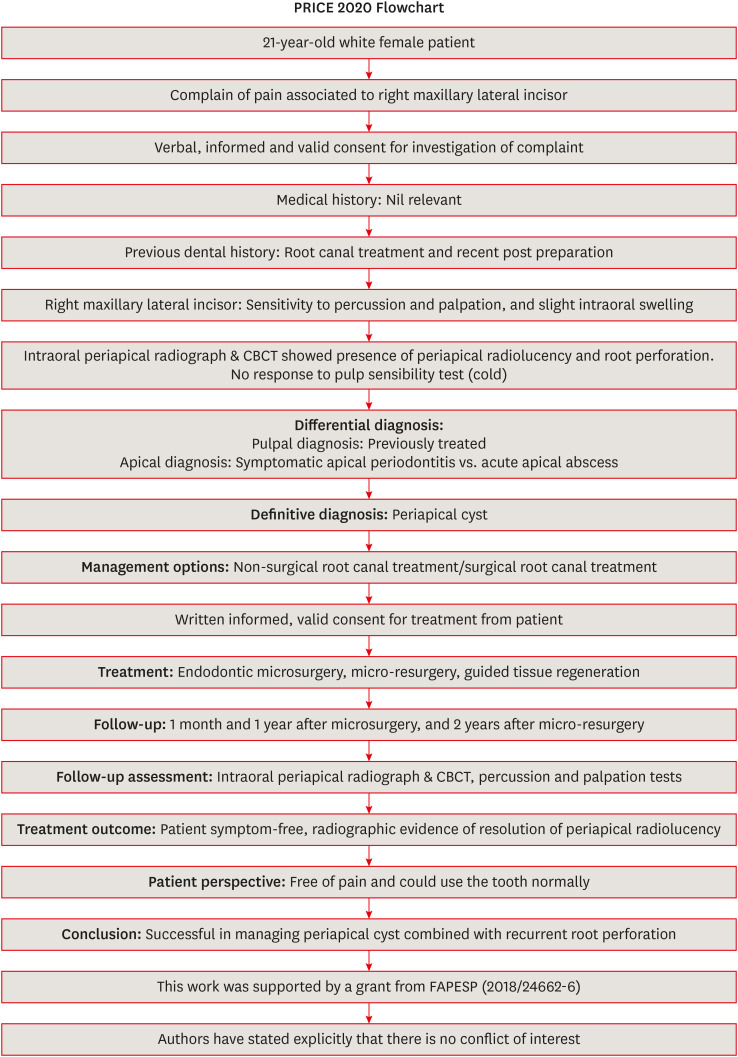
Figure 1 Chronological radiographs and CBCT images of the case management. Preoperative radiograph (A). Sagittal plane of a CBCT image, confirming that the cyst compromised buccal and palatal bone plates (B). Axial plane of a CBCT image, confirming the first perforation. The white arrow indicates the perforation (C). Immediate post-surgical radiograph (D). Periapical radiographs after 1 month and 1 year, respectively. As can be observed, the cyst is apparently decreasing in size (E, F). Sagittal and axial planes of CBCT images, confirming the second perforation, respectively. The white arrows indicate the perforation (G, H). Three-dimensional CBCT reconstruction. The buccal bone plate is clearly affected (I). Periapical radiograph 2 years after micro-resurgery (J). Sagittal and axial planes of CBCT images 2 years after micro-resurgery, confirming new bone formation—white arrows (K, L). Three-dimensional CBCT reconstruction 2 years after micro-resurgery (M).CBCT, cone-beam computed tomography.
Figure 2 Chronological, illustrative images of the case management. A root canal perforation can be observed in the buccal root surface of the right maxillary lateral incisor, 13× OP magnification (A). The cyst involving the buccal bone plate can be observed during the surgical phase, 5× OP magnification (B). Clinical appearance after cyst removal, where it can be observed that both buccal and palatal bone plates were compromised, 13× OP magnification (C). Application of lyophilized bovine bone and autologous platelet-rich fibrin into the bone defect, 5× OP magnification (D, E). Histopathological image (original magnification ×400) of the removed tissue showing cholesterol crystals, confirming the presence of a radicular cyst (F). Intraoral photograph 1 year after first microsurgery; a sinus tract appeared and was associated with the treated tooth (G). Clinical appearance of the second perforation in the buccal root surface of the affected tooth—white arrow, 8× OP magnification (H). Intraoral photograph 2 years after micro-resurgery. The tooth was restored with a crown (I).OP, operating microscope.
Figure 3 This flow chart was adopted from PRICE 2020 guidelines for reporting case reports in endodontics [16]. For further details visit: http://pride-endodonticguidelines.org/price/.CBCT, cone-beam computed tomography.
Figure 1
Figure 2
Figure 3
Endodontic micro-resurgery and guided tissue regeneration of a periapical cyst associated to recurrent root perforation: a case report

