
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 37(4); 2012 > Article
- Case Report Hypoesthesia after IAN block anesthesia with lidocaine: management of mild to moderate nerve injury
- Sungjoo Moon, Seung-Jong Lee, Euiseong Kim, Chan-Young Lee
-
2012;37(4):-235.
DOI: https://doi.org/10.5395/rde.2012.37.4.232
Published online: November 21, 2012
Department of Conservative Dentistry, Yonsei University College of Dentistry, Seoul, Korea.
- Correspondence to Chan-Young Lee, DDS, MSD, PhD. Professor, Department of Conservative Dentistry, Yonsei University College of Dentistry, 50 Yonsei-ro, Seodaemun-gu, Seoul, Korea 120-752. TEL, +82-2-2228-8701; FAX, +82-2-313-7575; CHANYOUNGL@yuhs.ac
• Received: August 6, 2012 • Revised: October 8, 2012 • Accepted: October 8, 2012
©Copyights 2012. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,010 Views
- 11 Download
- 17 Crossref
Abstract
- Hypoesthesia after an inferior alveolar nerve (IAN) block does not commonly occur, but some cases are reported. The causes of hypoesthesia include a needle injury or toxicity of local anesthetic agents, and the incidence itself can cause stress to both dentists and patients. This case presents a hypoesthesia on mental nerve area followed by IAN block anesthesia with 2% lidocaine. Prescription of steroids for a week was performed and periodic follow up was done. After 1 wk, the symptoms got much better and after 4 mon, hypoesthesia completely disappeared. During this healing period, only early steroid medication was prescribed. In most cases, hypoesthesia is resolved within 6 mon, but being aware of etiology and the treatment options of hypoesthesia is important. Because the hypoesthesia caused by IAN block anesthesia is a mild to moderate nerve injury, early detection of symptom and prescription of steroids could be helpful for improvement of the hypoesthesia.
Introduction
Hypoesthesia is defined as a decrease in normal sensation. Paresthesia, which is commonly confused with hypoesthesia, might have a decrease in normal sensation or might not. It is defined as any abnormal sensation such as burning, tingling, pricking, or numbness.1 Although local anesthetics are considered to be safe, they may involve some complications. One of these complications is hypoesthesia.2 When dentists perform inferior alveolar nerve (IAN) block anesthesia, a needle is injected near the IAN and lingual nerve, and then a local anesthetic agent infiltrates into these nerves. During this procedure, a direct mechanical injury or a chemical injury derived from the local anesthetic agents can be happened. Estimates of the incidence of local anesthetic-related neurosensory disturbance vary widely ranging from 1/42 to 1/750,000.3-7 Though over 85 percent of such injuries resolve spontaneously, it can remain permanently in some cases.8 Furthermore, incidence of hypoesthesia or paresthesia itself can cause stress to both dentists and patients. Therefore, dentists should understand the etiology and degree of nerve injury to provide a proper treatment or medication when a problem happens.
This unusual case report presents the hypoesthesia after IAN block anesthesia with 2% lidocaine, and discusses about the possible causes of hypoesthesia and ways to manage it.
Case report
A 36-year-old woman was presented to the department of conservative dentistry in Yonsei University, Dental College, Seoul, Korea. She received a root canal treatment for about five times before, but complained of spontaneous pain on the mandibular right second premolar. She had no specific medical history. The mandibular right second premolar was tested positive response to percussion, so it was diagnosed as previously initiated therapy, and symptomatic apical periodontitis. A nonsurgical root canal treatment was explained to the patient. She understood the treatment options and risk factors and signed the consent forms to proceed with the nonsurgical root canal treatment.
On the first day of the treatment, the IAN block anesthesia using 2% lidocaine (1:100,000 epinephrine, Huons Co., Ltd., Sungnam, Korea) was performed, and canal irrigation was done. Two days later, she called to our clinic and complained of feeling numb on her lower right lip and chin area. She also complained about feeling weird when chewing. Since hypoesthesia was suspected, we recommended her to visit our clinic as soon as possible. She visited our clinic two days after the call. She complained about dull sensation lasting on her lower right lip and chin area which is suspected to be a mental nerve innervations region. A Light touch test and pin prick test was performed and scored one-tenth comparing to the normal left side on her lip and chin. Hypoesthesia was diagnosed, so oral steroid was prescribed for a week and the patient was informed about the tapering procedure. Also, on the same day, mapping on the hypoesthetic region was performed (Figure 1).
After a week, she felt better but tickling sensation persisted on the region. Light touch test and pin prick test was again performed and scored one-half to two-thirds comparing to the left side. It was thought that healing was taking place, so additional medicine was not prescribed. At the 2 weeks follow up, the hypoesthesia was consistently getting better and 80 to 90 percent of sensation was recovered, compared to the left side. Five weeks after hypoesthesia was noticed, mapping was performed again (Figure 2). Comparing with the first mapping, the hypoesthetic region was decreased in size. During this period, non-surgical root canal treatment was accomplished including several canal irrigation appointments.
Four months later, she came to our office for a regular check-up. The hypoesthesia was completely resolved.
Discussion
Hypoesthesia can occur when any kind of injuries cause damage to the nerve fiber. The causes of injury are direct injury from needle injection around the nerve fiber, mechanical injury including indirect pressure to the mandibular canal during surgical procedures, and toxicity of local anesthetic agents.2,7,9 The needle injury can be a direct injection to the nerve fiber or a vascular damage around the nerve making hematoma that presses the nerve fiber. Furthermore, surgical dental procedure such as implant surgery or orthognatic surgery can also cause hypoesthesia. Although it is not commonly accepted but toxicity of local anesthetic agents may also offer a chance to cause hypoesthesia. It had been reported that hypoesthesia happened more often with 4% articaine or prilocaine.10
In the current study, we did not perform any surgical procedure. Therefore, a needle injury or local anesthetic agent toxicity was suspected to be the possible causes of the hypoesthesia. After carefully examining the possible causes of hypoesthesia, we first excluded the needle injury from the possible causes because of the following reasons. When performing IAN block anesthesia, shooting sensation or any uncomfortable feeling was not detected. In addition, it is hard to inject directly to the IAN because of the low tension of the nerve.
The toxicity of local anesthetic agents, which was the second possibility of the causes, is not clearly identified, but it is known that the toxicity can be a problem only when local anesthetic agents are used in animal studies with high dose.11
In vivo, some case reports suggested that the articaine or prilocaine can cause hypoesthesia or paresthesia more frequently, but it was self-reporting article and the incidence could have been overestimated. In our case, 2% lidocaine was used during the procedure and is known to be safe in most reports, so we also excluded this possibility.12
Lastly, hematoma can occur when the feeding vessels near the IAN are damaged. Inside or outside the epineurium, there are some feeding vessels running along the IAN. When these vessels are damaged by the needle during local anesthetic procedure, hematoma can be resulted. If the formed hematoma is large enough to press the nerve, then complications like hypoesthesia or paresthesia can develop. We concluded this to be only possible explanation to the hypoesthesia because other reasons cannot fully explain the hypoesthesia.
When hypoesthesia is suspected, there is a clinical testing called a neurosensory testing and it is performed in two parts: mechanical stimulation and nociceptive stimulation.13 From these tests, we can examine condition of nerve fiber. A light touch test is to test mechanical stimulation and a pin prick test is to test nociceptive stimulation. Among many other tests, in our case light touch test and pin prick test are used because additional special instrument is not needed and easy to perform. Since there was no abnormal sensation and just reduced sensation, hypoesthesia is diagnosed and treated accordingly.
In management of hypoesthesia, understanding the degree of injury is important. According to the classification by Sunderland, nerve injury is divided into 5 categories, from degree 1 which means conduction block to degree 5 which is nerve damage to epineurium.14 In this case, hypoesthesia was caused by the hematoma, so the injury was estimated to be degree 1. It is also called neuropraxia in Seddon's classification.15 Since the severity was in the degree 1, complete healing was expected.
When hypoesthesia or paresthesia occurs, it is recommended to prescribe oral steroids within 10 days since the nerve injury. Usually, steroids are used to treat nerve injuries such as facial palsy, optic neuritis, and spinal cord injury.16-19 Steroid is effective in healing of an early nerve injury because it reduces cytotoxic edema and improves nerve cell survival. Because of these same reasons, steroid is widely used and effective not only in nerve injuries but also in hypoesthesia.20 Steroids play a significant role in the anti-inflammatory action to subside the swelling. When the symptom persists, prescription of gabapentin or tricylclic antidepressants (TCA) is recommended from 10 days to 3 months after the nerve injury. After 3 months, a combination of these medications is indicated, and a surgery can be considered. Usually medications used after 10 days since the nerve injury is only effective for pain control and not for treating the symptoms of hypoesthesia or paresthesia. If the patients do not complain any painful feelings, additional medications are not indicated. However, when patients feel severe pain, additional NSAIDs can be helpful for pain control.21,22
In our study, the hypoesthesia was from the hematoma, and the degree of injury was 1 according to the Sunderland's classification. The patient did not feel any kind of pain. Therefore, we expected the complete healing within 6 months aided by early steroid prescription. As expected, the hypoesthesia was completely resolved at the 4 month follow-up visit. Prescription of oral steroids was the proper management in this case. If she had complained painful feeling, NSAIDs could have been prescribed additionally.
Conclusions
This case report presents a hypoesthesia after IAN block anesthesia that finally resolved in 4 months. The hypoesthesia may have been caused by a hematoma formation near the IAN which resulted pressure to the nerve. The patient did not complain of any pain from the region; therefore early oral steroid prescription was done which can be helpful to overcome the hypoesthesia. Because overprescribing of medication is not recommended, dentists should be aware of degree of nerve injury, timing of intervention, and proper management methods including medication prescription to ensure a better prognosis dealing with hypoesthesia.
- 1. Lichtor T, Mullan JF. A 10-year follow-up review of percutaneous microcompression of the trigeminal ganglion. J Neurosurg 1990;72:49-54.ArticlePubMed
- 2. Hillerup S, Jensen RH, Ersbøll BK. Trigeminal nerve injury associated with injection of local anesthetics: needle lesion or neurotoxicity? J Am Dent Assoc 2011;142:531-539.PubMed
- 3. Haas DA, Lennon D. A 21 year retrospective study of reports of paresthesia following local anesthetic administration. J Can Dent Assoc 1995;61:319-320. 323-326. 329-330.PubMed
- 4. Krafft TC, Hickel R. Clinical investigation into the incidence of direct damage to the lingual nerve caused by local anaesthesia. J Craniomaxillofac Surg 1994;22:294-296.PubMed
- 5. Dower JS Jr. Anesthetic study questioned. J Am Dent Assoc 2007;138:708. 710; author reply 710, 712.Article
- 6. Pogrel MA, Thamby S. Permanent nerve involvement resulting from inferior alveolar nerve blocks. J Am Dent Assoc 2000;131:901-907.PubMed
- 7. Pogrel MA, Bryan J, Regezi J. Nerve damage associated with inferior alveolar nerve blocks. J Am Dent Assoc 1995;126:1150-1155.ArticlePubMed
- 8. Haas DA. An update on local anesthetics in dentistry. J Can Dent Assoc 2002;68:546-551.PubMed
- 9. Reina MA, López A, De Andrés JA, Machés F. Possibility of nerve lesions related to peripheral nerve blocks. A study of the human sciatic nerve using different needles. Rev Esp Anestesiol Reanim 2003;50:274-283.PubMed
- 10. Garisto GA, Gaffen AS, Lawrence HP, Tenenbaum HC, Haas DA. Occurrence of paresthesia after dental local anesthetic administration in the United States. J Am Dent Assoc 2010;141:836-844.ArticlePubMed
- 11. Kirihara Y, Saito Y, Sakura S, Hashimoto K, Kishimoto T, Yasui Y. Comparative neurotoxicity of intrathecal and epidural lidocaine in rats. Anesthesiology 2003;99:961-968.ArticlePubMedPDF
- 12. Gaffen AS, Haas DA. Retrospective review of voluntary reports of nonsurgical paresthesia in dentistry. J Can Dent Assoc 2009;75:579.PubMed
- 13. Omer GE Jr. Methods of assessment of injury and recovery of peripheral nerves. Surg Clin North Am 1981;61:303-319.ArticlePubMed
- 14. Sunderland S. A classification of peripheral nerve injuries producing loss of function. Brain 1951;74:491-516.ArticlePubMed
- 15. Seddon HJ, Medawar PB, Smith H. Rate of regeneration of peripheral nerves in man. J Physiol 1943;102:191-215.ArticlePubMedPMC
- 16. Lagalla G, Logullo F, Di Bella P, Provinciali L, Ceravolo MG. Influence of early high-dose steroid treatment on Bell's palsy evolution. Neurol Sci 2002;23:107-112.ArticlePubMedPDF
- 17. Austin JR, Peskind SP, Austin SG, Rice DH. Idiopathic facial nerve paralysis: a randomized double blind controlled study of placebo versus prednisone. Laryngoscope 1993;103:1326-1333.ArticlePubMed
- 18. Wray SH. Optic neuritis: guidelines. Curr Opin Neurol 1995;8:72-76.PubMed
- 19. Ramsey MJ, DerSimonian R, Holtel MR, Burgess LP. Corticosteroid treatment for idiopathic facial nerve paralysis: a meta-analysis. Laryngoscope 2000;110:335-341.ArticlePubMed
- 20. Seo K, Tanaka Y, Terumitsu M, Someya G. Efficacy of steroid treatment for sensory impairment after orthognathic surgery. J Oral Maxillofac Surg 2004;62:1193-1197.ArticlePubMed
- 21. Lewis MA, Sankar V, De Laat A, Benoliel R. Management of neuropathic orofacial pain. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:S32.e1-S32.e24.ArticlePubMed
- 22. Park JH, Lee SH, Kim ST. Pharmacologic management of trigeminal nerve injury pain after dental implant surgery. Int J Prosthodont 2010;23:342-346.PubMed
REFERENCES


Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Botulinum Toxin-A, Generating a Hypothesis for Orofacial Pain Therapy
Yair Sharav, Rafael Benoliel, Yaron Haviv
Toxins.2025; 17(8): 389. CrossRef - Intranasal CRMP2-Ubc9 inhibitor regulates NaV1.7 to alleviate trigeminal neuropathic pain
Santiago I. Loya-Lopez, Heather N. Allen, Paz Duran, Aida Calderon-Rivera, Kimberly Gomez, Upasana Kumar, Rory Shields, Rui Zeng, Akshat Dwivedi, Saumya Saurabh, Olga A. Korczeniewska, Rajesh Khanna
Pain.2024; 165(3): 573. CrossRef - İMPLANT CERRAHİSİ SONRASI HİPOESTEZİ-6 AYLIK TAKİP: VAKA SERİSİ
Sefa AYDINDOĞAN, Emine Elif MUTAFCİLAR VELİOĞLU, Yunus Emre BALABAN
Selcuk Dental Journal.2023; 10(4): 350. CrossRef - Pathophysiology of Post-Traumatic Trigeminal Neuropathic Pain
Olga A. Korczeniewska, Divya Kohli, Rafael Benoliel, Sita Mahalakshmi Baddireddy, Eli Eliav
Biomolecules.2022; 12(12): 1753. CrossRef - Shape and anatomical relationship of the mental foramen to the mandibular premolars in an Indian sub-population: a retrospective CBCT analysis
Komal Sheth, Kulvinder Singh Banga, Ajinkya M. Pawar, James L. Gutmann, Hyeon-Cheol Kim
Restorative Dentistry & Endodontics.2022;[Epub] CrossRef - Trigeminal neuralgia and persistent idiopathic facial pain (atypical facial pain)
Gary W. Jay, Robert L. Barkin
Disease-a-Month.2022; 68(6): 101302. CrossRef - Differential roles of NMDAR subunits 2A and 2B in mediating peripheral and central sensitization contributing to orofacial neuropathic pain
Yan-Yan Zhang, Fei Liu, Zhong-Han Fang, Yue-Ling Li, Hong-Lin Liao, Qin-Xuan Song, Cheng Zhou, Jie-Fei Shen
Brain, Behavior, and Immunity.2022; 106: 129. CrossRef - Visualization of Inferior Alveolar and Lingual Nerve Pathology by 3D Double-Echo Steady-State MRI: Two Case Reports with Literature Review
Adib Al-Haj Husain, Daphne Schönegg, Silvio Valdec, Bernd Stadlinger, Thomas Gander, Harald Essig, Marco Piccirelli, Sebastian Winklhofer
Journal of Imaging.2022; 8(3): 75. CrossRef - Molecular mechanisms of painful traumatic trigeminal neuropathy—Evidence from animal research and clinical correlates
Olga A. Korczeniewska, Junad Khan, Eli Eliav, Rafael Benoliel
Journal of Oral Pathology & Medicine.2020; 49(6): 580. CrossRef - Behavioral changes in calves 11 days after cautery disbudding: Effect of local anesthesia
Sarah J.J. Adcock, Danielle M. Cruz, Cassandra B. Tucker
Journal of Dairy Science.2020; 103(9): 8518. CrossRef - Frequency of Lower Lip Paresthesia in Patients Receiving Implant-Supported Mandibular Dentures in Tabriz, Iran in 2017-2018
Farrokh Farhadi, Reza Khorshidi-Khiavi, Fereshteh Taheri, Milad Ghanizadeh
Avicenna Journal of Dental Research.2019; 11(1): 26. CrossRef - Persistent idiopathic facial pain
Rafael Benoliel, Charly Gaul
Cephalalgia.2017; 37(7): 680. CrossRef - Painful Traumatic Trigeminal Neuropathy
Rafael Benoliel, Sorin Teich, Eli Eliav
Oral and Maxillofacial Surgery Clinics of North America.2016; 28(3): 371. CrossRef - Neuropathy of Trigeminal Nerve Branches After Oral and Maxillofacial Treatment
Jimoh Olubanwo Agbaje, Elke Van de Casteele, Marjolein Hiel, Ciska Verbaanderd, Ivo Lambrichts, Constantinus Politis
Journal of Maxillofacial and Oral Surgery.2016; 15(3): 321. CrossRef - The Enigma of the Mental Foramen as It Relates to Plastic Surgery
Raphael Alves Chu, Fabio Xerfan Nahas, Marcello Di Martino, Fernanda Abibi Soares, Neil Ferreira Novo, Ricardo Luiz Smith, Lydia Masako Ferreira
Journal of Craniofacial Surgery.2014; 25(1): 238. CrossRef - Mental nerve paresthesia secondary to initiation of endodontic therapy: a case report
Syed Mukhtar-Un-Nisar Andrabi, Sharique Alam, Afaf Zia, Masood Hasan Khan, Ashok Kumar
Restorative Dentistry & Endodontics.2014; 39(3): 215. CrossRef - Pain Sensation and Postsurgical Complications in Posterior Mandibular Implant Placement Using Ridge Mapping, Panoramic Radiography, and Infiltration Anesthesia
Ali Saad Thafeed AlGhamdi
ISRN Dentistry.2013; 2013: 1. CrossRef
 ePub Link
ePub Link Cite
CiteHypoesthesia after IAN block anesthesia with lidocaine: management of mild to moderate nerve injury

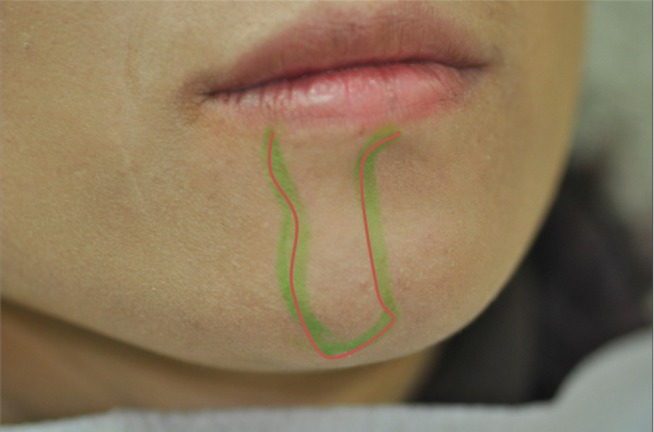
Figure 1 Mapping from the first visit after nerve injury indicates that the hypoesthesia was on the right mental nerve area.
Figure 2 Mapping at 5 weeks follow-up after the nerve injury. The hypoesthetic region was reduced compared to the first mapping.
Figure 1
Figure 2
Hypoesthesia after IAN block anesthesia with lidocaine: management of mild to moderate nerve injury

