
Search
- Page Path
- HOME > Search
Research Articles
- Assessment of mechanical allodynia in healthy teeth adjacent and contralateral to endodontically diseased teeth: a clinical study
- Vaishnavi Ratnakar Patankar, Ashish K Jain, Rahul D Rao, Prajakta R Rao
- Restor Dent Endod 2024;49(3):e31. Published online July 29, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e31
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
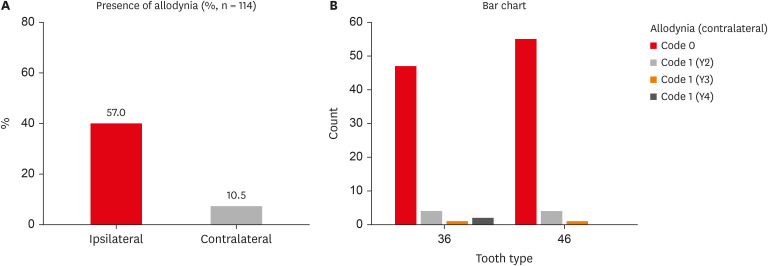
ePub Objectives The present study investigated the prevalence of mechanical allodynia (MA) in healthy teeth adjacent and contralateral to endodontically diseased teeth.
Materials and Methods This cross-sectional study included 114 patients with symptomatic irreversible pulpitis and apical periodontitis in permanent mandibular first molars who possessed healthy teeth adjacent and contralateral to the endodontically diseased tooth. The mechanical sensitivity of the teeth was determined by percussion testing. The presence or absence of pain on percussion in the teeth adjacent and contralateral to the endodontically diseased tooth and the tooth distal to the contralateral symmetrical tooth was recorded according to coding criteria. The prevalence of MA was computed as a percentage, and binary logistic regression analysis was done. The Fisher exact test and Mann-Whitney
U test were used for binary and ordinal data.Results Age and sex did not influence the prevalence of MA. An increased prevalence of MA was found in patients with higher levels of spontaneous pain (
p < 0.001). The prevalence of allodynia was 57% in teeth adjacent to endodontically diseased teeth and 10.5% in teeth contralateral to endodontically diseased teeth. In addition, on the ipsilateral side, there were more painful sensations distal to the diseased tooth than mesially.Conclusions Despite being disease-free, teeth adjacent and contralateral to endodontically diseased teeth exhibited pain on percussion. There was a direct association between the severity of the patient’s pain and the presence of MA.
-
Citations
Citations to this article as recorded by
- Incidence and assessment of mechanical allodynia and its association with dental anxiety in endodontic pain: A clinical study
Manduwada Vishal, Sowmya Padala, E. Soujanya, Mamta Kaushik
Journal of Conservative Dentistry and Endodontics.2026; 29(5): 514. CrossRef
- Incidence and assessment of mechanical allodynia and its association with dental anxiety in endodontic pain: A clinical study
- 4,145 View
- 111 Download
- 1 Crossref

- Radiographic patterns of periosteal bone reactions associated with endodontic lesions
- Poorya Jalali, Jessica Riccobono, Robert A. Augsburger, Mehrnaz Tahmasbi-Arashlow
- Restor Dent Endod 2023;48(3):e23. Published online June 8, 2023
- DOI: https://doi.org/10.5395/rde.2023.48.e23
-
Abstract
PDFPubReaderePub
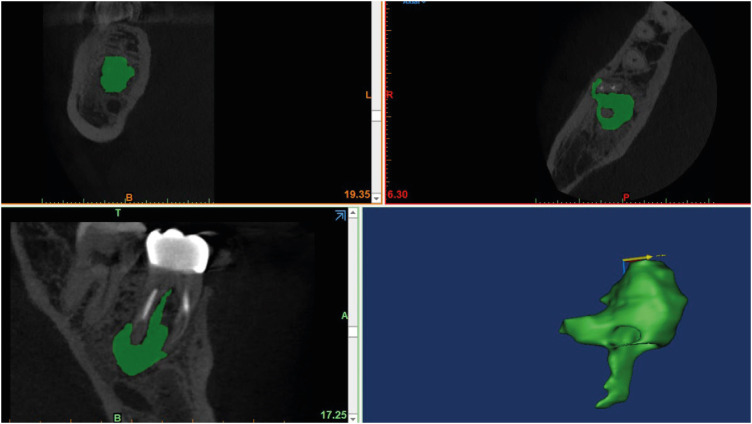
Objectives The formation of new bone by periosteum due to an insult is called periosteal bone reaction (PBR). This study assessed the cone beam computed tomography (CBCT) patterns of periosteal bone reactions associated with periapical inflammatory lesion (apical periodontitis/periapical rarefying osteitis).
Materials and Methods Twenty-two small field of view CBCT images of patients with PBR were selected from a database of a private practice limited to endodontics. The volume of the periapical inflammatory lesion, the presence of cortical fenestration, the distance of the root apices to the affected cortex, and the location, pattern, and longest diameter of the periosteal reaction were recorded. Statistical analysis was performed using Wilcoxon Ranksum, Fischer’s exact, Spearman Correlation Coefficient, and paired
t -test.Results In all cases, periosteal bone reaction manifested as either parallel (90.9%) or irregular (9.1%). No correlation was found between periapical inflammatory lesion volume and the periosteal reaction's longest diameter (
p > 0.05). Cortical fenestration was noted in 72.7% of the cases. In addition, the findings showed that periosteal reactions were located mostly on the buccal and were present 53.8% and 100% of the time in the mandible and maxilla, respectively.Conclusions The periosteal reactions of endodontic origin had a nonaggressive form (
i.e ., parallel or irregular), and none of the lesions resulted in a periosteal reaction with an ominous Codman’s triangle or spicule pattern.-
Citations
Citations to this article as recorded by- ENDODONTIA E INTERCORRÊNCIAS: COMPREENDENDO OS ACIDENTES E OTIMIZANDO O PROGNÓSTICO
Ana Paula Oliveira Rocha, Flávia Cordeiro Antunes , Millena Alberto Luna , Raissa Danielle Muniz Da Silva , Gustavo Henrique Palma Durães , Juliano Magno de Valadares Bicalho , Lorena Miranda Lima , Barbara Quadros Tonelli
REMUNOM.2026; 2(03): 1. CrossRef - Endodontic Intervention in Chronic Osteomyelitis With Proliferative Periostitis: A Rare Case Report and Scoping Review
Gabriel Lima Braz, Ana Paula Neutzling Gomes, Lisandrea Rocha Schardosim, Nadia de Souza Ferreira, Jose Francisco Gomez-Sosa
Case Reports in Dentistry.2026;[Epub] CrossRef - The influence of endodontic treatment quality on periapical lesions' architecture in cone‐beam computed tomography
Ewa Mackiewicz, Tobias Bonsmann, Krzysztof Safranow, Patrycja Nowicka, Janusz Kołecki, Alicja Nowicka
Australian Endodontic Journal.2025; 51(1): 36. CrossRef - Novel radiographic pattern of maxillary periostitis induced by endodontic inflammation: A case report
Pai-Chun Huang, I-Hao Su, Meng-Ling Chiang, Jyh-Kwei Chen
Journal of Dental Sciences.2025; 20(3): 1982. CrossRef - Garre’s osteomyelitis of the mandible managed by nonsurgical re-endodontic treatment
Heegyun Kim, Jiyoung Kwon, Hyun-Jung Kim, Soram Oh, Duck-Su Kim, Ji-Hyun Jang
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef
- ENDODONTIA E INTERCORRÊNCIAS: COMPREENDENDO OS ACIDENTES E OTIMIZANDO O PROGNÓSTICO
- 6,842 View
- 105 Download
- 4 Web of Science
- 5 Crossref
Case Report
- Revitalization of necrotic mature permanent incisors with apical periodontitis: a case report
- Emre Nagas, M. Ozgur Uyanik, Zafer C. Cehreli
- Restor Dent Endod 2018;43(3):e31. Published online July 5, 2018
- DOI: https://doi.org/10.5395/rde.2018.43.e31
-
Abstract
PDFPubReaderePub
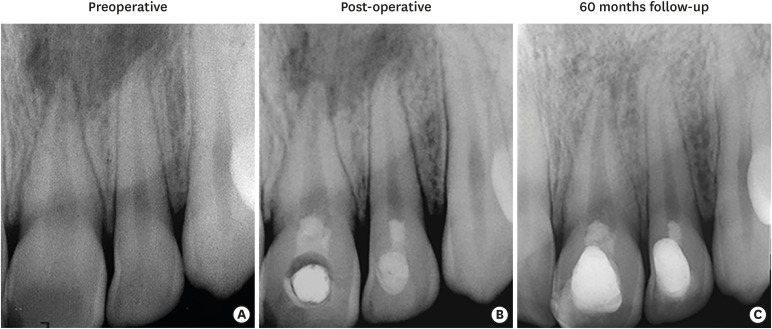
Despite considerable focus on the regenerative endodontic treatment of immature teeth with necrotic infected pulps and apical periodontitis, little data exist with regard to its possible implementation in necrotic permanent teeth with complete apical and radicular development. The present report describes the procedures and outcome of a regenerative endodontic treatment approach in 2 previously-traumatized incisors with closed apex with apical periodontitis. A 2-visit treatment procedure was employed. At initial visit, the root canals were copiously irrigated, followed by placement of a triple antibiotic paste containing ciprofloxacin, metronidazole, and clindamycin into the root canals. After 4 weeks, the antibiotic paste was removed, and apical bleeding was initiated with size 10 hand files beyond the apices. The root canals were coronally sealed with mineral trioxide aggregate, and the access cavities were restored with bonded resin composite. At post-operative 60 months, both teeth were remained asymptomatic, with the recall radiographs showing complete resolution of apical radiolucency and reestablishment of periradicular tissues. In both teeth, the dimensions of root space remained unchanged as verified by image analysis. The revitalization protocol utilizing root canal disinfection and induced apical bleeding in necrotic, closed-apex incisors may offer a clinically acceptable alternative to conventional root canal treatment.
-
Citations
Citations to this article as recorded by- Effect of chitosan medicaments loaded with green-synthesized silver nanoparticles on basic fibroblast growth factor release from infected dentin
Dilek Hancerliogullari, Zehra Gun Gok, Nebahat Aytuna Cerci, Eray Ceylanoglu, Bengisu Ozturk, Ozum Hekim Harput, Sevda Durust Baris, Filiz Kiper, Ali Erdemir
Odontology.2026; 114(3): 1593. CrossRef - The Role and Efficacy of Scaffolds in Regenerative Endodontics: A Survey of Current Practices and Perspective among Clinicians: A Questionnaire-based Study
Minusha Mohanan, Shabna Moyin, Shamsheer Thayyil, Anju Balachandran, Mary Elizabeth Nellickapalley Jacob, Koroth Valappil Harsha
Conservative Dentistry and Endodontic Journal.2026; 8(1): 10. CrossRef - Evaluation of Regenerative Endodontic Therapy in Young Permanent Teeth with Pulp Necrosis: A Retrospective Study
Işıl Özgül Kalyoncu, Ayşe Nur Sadıkoğlu, Figen Eren Giray, Betul Kargul
Current Research in Dental Sciences.2026; 36(2): 163. CrossRef - Regeneration Versus Granulation Tissue Healing in a Hopeless Mature Mandibular Molar Post-Endodontic Management: A 40-Month Follow-Up Case Report
Elhassan Hassanein, Petra Gierthmuehlen, Almaha S. Algazlan, Dalia Kaisarly, Moataz Elgezawi
Dentistry Journal.2026; 14(4): 243. CrossRef - The outcome of pulp revascularization of necrotic mature permanent teeth with periapical lesions using platelet-rich fibrin versus induced bleeding: a prospective preliminary randomized clinical trial
Lama Awawdeh, Bushra Almesleh, Hanan Hammouri, Aladdin Al-Qudah
Clinical Oral Investigations.2026;[Epub] CrossRef - Regenerative potential of concentrated growth factor compared to platelet-rich fibrin in treatment of necrotic mature teeth: a randomized clinical trial
Taghreed Salah, Wael Hussein, Heba Abdelkafy
BDJ Open.2025;[Epub] CrossRef - Efficacy of Pulp Revascularization in the Treatment of Apical Periodontitis in Mature Necrotic Teeth: An Umbrella Review
Wanderson Limeira de Sousa Barbosa, Luiz Renato Paranhos, Márcia Valente de Brito Dantas, Rômulo Dias Jesuino, João Marcos da Costa Ribeiro, Walbert A. Vieira, Felipe de Souza Matos
Australian Endodontic Journal.2025; 51(2): 495. CrossRef - Clinical and radiographic outcomes of non-surgical retreatment of mature maxillary incisors using two regenerative endodontic techniques in adolescents: a 24-month randomized clinical trial
Ahmad Abdel Hamid Elheeny, Sherif Shafik EL Bahnasy, Yassmin Mohamed ElMakawi, Mohammed Turky, Eman Farouk Ahmed, Norhan Khaled Omar Wahba
BDJ Open.2025;[Epub] CrossRef - Revolutionizing Endodontics: Innovative Approaches for Treating Mature Teeth With Closed Apices and Apical Lesions: A Report of Two Cases
Claudia Brizuela, Gastón Meza, Maroun Khoury
Journal of Endodontics.2024; 50(5): 596. CrossRef - Current Aspects of Regenerative Endodontics: A Systematic Review
A. V. Mitronin, K. A. Archakov, D. A. Ostanina, Yu. A. Mitronin, T. V. Khizrieva
Endodontics Today.2024; 21(4): 287. CrossRef - Correlation between pulp sensibility and magnetic resonance signal intensity following regenerative endodontic procedures in mature necrotic teeth- a retrospective cohort study
Noha Mohamed El-Kateb, Amr Mohamed Abdallah, Rania Noaman ElBackly
BMC Oral Health.2024;[Epub] CrossRef - Influence of periapical lesion size on healing outcome following regenerative endodontic procedures: a clinical investigation
Noha Mohamed El Kateb, Mahmoud Mostafa Fata
Oral Radiology.2022; 38(4): 480. CrossRef - Do alternative scaffolds used in regenerative endodontics promote better root development than that achieved with blood clots?
Letícia de Araújo, Taynara Santos Goulart, Ana Clara Kuerten Gil, Daniela Peressoni Vieira Schuldt, Beatriz Serrato Coelho, Daniela de Rossi Figueiredo, Lucas da Fonseca Roberti Garcia, Josiane de Almeida
Brazilian Dental Journal.2022; 33(2): 22. CrossRef - Endodontic Regenerative Procedures in Necrotic Adult Teeth
Sara Garrido-Parada, Pablo Castelo-Baz, Nancy Feijoo-Pato, José Gaviño-Orduña, Benjamín Martín-Biedma
Applied Sciences.2022; 12(9): 4212. CrossRef - Combined conventional and regenerative treatment in molars with coexistent closed and open apices: A case series
Zafer C. Cehreli, Gizem Erbas Unverdi, Pinar Eymirli, Irem Mergen, Ezgihan Arslan, Gulce Esenturk
Australian Endodontic Journal.2022; 48(1): 197. CrossRef - Regenerative Endodontic Procedures for the Treatment of Necrotic Mature Teeth with Apical Periodontitis: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Antonios Glynis, Federico Foschi, Ismini Kefalou, Despina Koletsi, Giorgos N. Tzanetakis
Journal of Endodontics.2021; 47(6): 873. CrossRef - Different Approaches to the Regeneration of Dental Tissues in Regenerative Endodontics
Anna M. Krupińska, Katarzyna Skośkiewicz-Malinowska, Tomasz Staniowski
Applied Sciences.2021; 11(4): 1699. CrossRef - Quantitative Assessment of Intracanal Regenerated Tissues after Regenerative Endodontic Procedures in Mature Teeth Using Magnetic Resonance Imaging: A Randomized Controlled Clinical Trial
Noha Mohamed El-Kateb, Rania Noaman El-Backly, Wessam Mohamed Amin, Amr Mohamed Abdalla
Journal of Endodontics.2020; 46(5): 563. CrossRef
- Effect of chitosan medicaments loaded with green-synthesized silver nanoparticles on basic fibroblast growth factor release from infected dentin
- 3,369 View
- 34 Download
- 18 Crossref
Research Article
- Effects of canal enlargement and irrigation needle depth on the cleaning of the root canal system at 3 mm from the apex
- Ho-Jin Moon, Chan-Ui Hong
- Restor Dent Endod 2012;37(1):24-28. Published online March 2, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.1.24
-
Abstract
PDFPubReaderePub
Objectives The aim of this study was to test the hypothesis, that the effectiveness of irrigation in removing smear layer in the apical third of root canal system is dependent on the depth of placement of the irrigation needle into the root canal and the enlargement size of the canal.
Materials and Methods Eighty sound human lower incisors were divided into eight groups according to the enlargement size (#25, #30, #35 and #40) and the needle penetration depth (3 mm from working length, WL-3 mm and 9 mm from working length, WL-9 mm). Each canal was enlarged to working length with Profile.06 Rotary Ni-Ti files and irrigated with 5.25% NaOCl. Then, each canal received a final irrigation with 3 mL of 3% EDTA for 4 min, followed by 5 mL of 5.25% NaOCl at different level (WL-3 mm and WL-9 mm) from working length. Each specimen was prepared for the scanning electron microscope (SEM). Photographs of the 3mm area from the apical constriction of each canal with a magnification of ×250, ×500, ×1,000, ×2,500 were taken for the final evaluation.
Results Removal of smear layer in WL-3 mm group showed a significantly different effect when the canal was enlarged to larger than #30. There was a significant difference in removing apical smear layer between the needle penetration depth of WL-3 mm and WL-9 mm.
Conclusions Removal of smear layer from the apical portion of root canals was effectively accomplished with apical instrumentation to #35/40 06 taper file and 3 mm needle penetration from the working length.
-
Citations
Citations to this article as recorded by- Numerical Evaluation of Flow Pattern for Root Canal Irrigation Including icrobubbles
Joon Hyun Kim, Chan U Lee, Inwhan Lee, Jaeyong Sung
Journal of the Korean Society of Manufacturing Technology Engineers.2023; 32(5): 251. CrossRef
- Numerical Evaluation of Flow Pattern for Root Canal Irrigation Including icrobubbles
- 1,786 View
- 6 Download
- 1 Crossref
 First
First Prev
Prev

