
Search
- Page Path
- HOME > Search
Research Article
- Clinical and radiographic outcomes of regenerative endodontic treatment performed by endodontic postgraduate students: a retrospective study
- Hadi Rajeh Alfahadi, Saad Al-Nazhan, Fawaz Hamad Alkazman, Nassr Al-Maflehi, Nada Al-Nazhan
- Restor Dent Endod 2022;47(2):e24. Published online May 9, 2022
- DOI: https://doi.org/10.5395/rde.2022.47.e24
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub Objectives Regenerative endodontic treatment is a clinical procedure aimed at biologically regenerating damaged root canal tissue of immature permanent teeth. This study aimed to report the outcomes of regenerative endodontic treatment performed by endodontic postgraduate students.
Materials and Methods Clinical and radiographic data of 27 patients, aged 10–22 years, who underwent regenerative treatment of immature permanent teeth from 2015 to 2019 were followed up, wherein clinical and radiographic examinations were performed for each patient. Postoperative success rate and tooth survival were analyzed, and the postoperative radiographic root area changes were quantified.
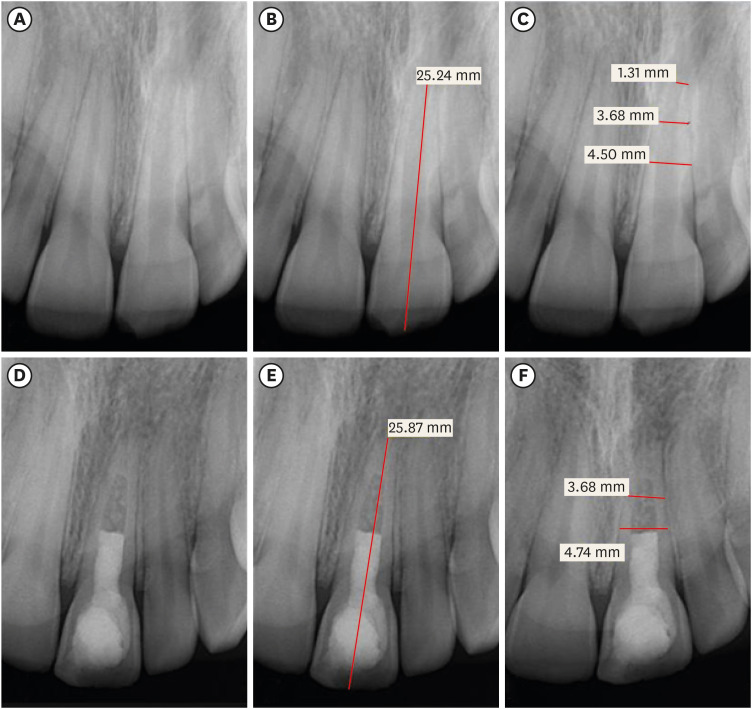
Results A total of 23 patients attended the dental appointments, showing that all teeth survived and were asymptomatic. Specifically, 7 periapical pathosis cases were completely healed, 12 were incompletely healed, and 4 cases failed. Moreover, significant differences were found between discolored and non-discolored teeth, and between the presence or absence of periapical radiolucency. Additionally, 3 anterior teeth showed complete closure of the apical foramen, while the apical foramen width was reduced in 17 teeth and failed in 3 teeth. Root length was also found to have been increased in 7 anterior and 4 posterior teeth, and the average length ranged from 4.00–0.63 mm in the anterior teeth, 2.85–1.48 mm of the mesial root, and 2.73–2.16 mm of the molar teeth distal root. Furthermore, calcified tissue deposition was observed in 7 teeth.
Conclusions A favorable outcome of regenerative endodontic treatment of immature permanent teeth with necrotic pulp was achieved with a high survival rate.
-
Citations
Citations to this article as recorded by
- Regenerative Endodontics and Stem Cell-Based Therapies – A Systematic Review
Wjoud Ahmed Alshamrani, Sarah Sulaiman Alzarea, Joud Khalid Alabbas, Ayah Khalid Alabbas, Mawiyah Ibrahim Aljaddua, Osama Khattak, Rakhi Issrani
Journal of Pharmacy and Bioallied Sciences.2026; 18(Suppl 1): S29. CrossRef - Treatment outcomes and prognostic factors of regenerative endodontic procedures in immature permanent teeth
Gülsen Kiraz, Salihanur Sarı, Sümeyra Akkoç, Arzu Kaya Mumcu
BMC Oral Health.2026;[Epub] CrossRef - Pre‐Operative Factors on Prognosis of Regenerative Endodontic Procedures: A Systematic Review and Meta‐Analysis
Filipe Colombo Vitali, Alexandre Henrique dos Reis‐Prado, Pablo Silveira Santos, Ana Paula Portes Zeno, Patrícia de Andrade de Risso, Lucianne Cople Maia, Francine Benetti, Cleonice da Silveira da Teixeira
International Endodontic Journal.2025; 58(12): 1814. CrossRef - Clinical, radiographic, and biomarker perspectives of low-level laser therapy during regenerative endodontic procedures in necrotic immature young teeth: a randomized clinical study
Pragya Pandey, Neha Jasrasaria, Ramesh Bharti, Rakesh Kumar Yadav, Monika Kumari, Abinia Vaishnavi, Rahul Pandey
Lasers in Medical Science.2025;[Epub] CrossRef - Allogeneic Bone Marrow Mesenchymal Stromal Cell Transplantation Induces Dentin Pulp Complex-like Formation in Immature Teeth with Pulp Necrosis and Apical Periodontitis
Jose Francisco Gomez-Sosa, José E. Cardier, Olga Wittig, Dylana Díaz-Solano, Eloisa Lara, Kharelys Duque, Giselle Ramos-González
Journal of Endodontics.2024; 50(4): 483. CrossRef - Radiographic assessment of dental post and core placement at different educational levels in an undergraduate student clinic: a 4-year retrospective study
Turki Alshehri, Nourhan M. Aly, Raand Altayyar, Deena Alghamdi, Shahad Alotaibi, Passent Ellakany
F1000Research.2024; 12: 976. CrossRef - Evaluation of the efficacy of injectable platelet‐rich fibrin versus platelet‐rich plasma in the regeneration of traumatized necrotic immature maxillary anterior teeth: A randomized clinical trial
Maha Mohamed Abo‐Heikal, Jealan M. El‐Shafei, Samia A. Shouman, Nehal N. Roshdy
Dental Traumatology.2024; 40(1): 61. CrossRef - Radiographical assessment of post and core placement errors encountered by Saudi dental students at different educational levels
Turki Alshehri, Nourhan M. Aly, Raand Altayyar, Deena Alghamdi, Shahad Alotaibi, Passent Ellakany
F1000Research.2023; 12: 976. CrossRef
- Regenerative Endodontics and Stem Cell-Based Therapies – A Systematic Review
- 5,835 View
- 113 Download
- 8 Web of Science
- 8 Crossref

Case Report
- Treatment of non-vital immature teeth with amoxicillin-containing triple antibiotic paste resulting in apexification
- Hyon-Beom Park, Bin-Na Lee, Yun-Chan Hwang, In-Nam Hwang, Won-Mann Oh, Hoon-Sang Chang
- Restor Dent Endod 2015;40(4):322-327. Published online August 28, 2015
- DOI: https://doi.org/10.5395/rde.2015.40.4.322
-
Abstract
PDFPubReaderePub
A recent treatment option for non-vital immature teeth in young patients is revascularization with triple antibiotic paste (TAP). However, tooth discoloration was reported with the use of conventional minocycline-containing TAP. In this case report, amoxicillin-containing TAP was used for revascularization of non-vital immature teeth to prevent tooth discoloration. At the 1 yr follow up, the teeth were asymptomatic on clinical examination and showed slight discoloration of the crown due to mineral trioxide aggregate (MTA) filling rather than amoxicillin-containing TAP. Radiographic examination revealed complete resolution of the periapical radiolucency, and closed apex with obvious periodontal ligament space. However, the root growth was limited, and the treatment outcome was more like apexification rather than revascularization. These results may be due to unstable blood clot formation which could not resist the condensation force of MTA filling, whether or not a collagen matrix was in place. These cases showed that although revascularization was not successful, apexification could be expected, resulting in the resolution of the periapical radiolucency and the closure of the apex. Therefore, it is worthwhile attempting revascularization of non-vital immature teeth in young patients.
-
Citations
Citations to this article as recorded by- Comparative evaluation of effect of modified triple antibiotic paste and calcium hydroxide as intracanal medicament on microhardness of root dentin: An in vitro study
Aparna Palekar, Piyush Mantri, Minal Awinashe, Basawaraj Biradar, Mukund Singh
Endodontology.2024; 36(2): 143. CrossRef - Healing of Large Endodontic Lesions Using Long‐Term Application of a New Combination of Triple Antibiotics: A Series of Cases
Saeed Asgary, Ardavan Parhizkar, Maria Beatriz Duarte Gavião
Case Reports in Dentistry.2023;[Epub] CrossRef - Comparative Evaluation of Two Antibiotic Pastes for Root Canal Disinfection
Mridula Goswami, CP Baveja, Urvashi Bhushan, Sadhna Sharma
International Journal of Clinical Pediatric Dentistry.2022; 15(S1): S12. CrossRef - Regenerative Endodontics as the Future Treatment of Immature Permanent Teeth
Justyna Zbańska, Katarzyna Herman, Piotr Kuropka, Maciej Dobrzyński
Applied Sciences.2021; 11(13): 6211. CrossRef - Antimicrobial efficacy of triple antibiotic paste in teeth with primary endodontic infection: A systematic review
Rhythm Bains, Aseem P. Tikku, Promila Verma, Pragya Pandey
Asian Journal of Oral Health and Allied Sciences.2021; 11: 2. CrossRef - Effectiveness of MTA apical plug in dens evaginatus with open apices
Khoa Van Pham, Thu Anh Tran
BMC Oral Health.2021;[Epub] CrossRef - Lesion Sterilization and Tissue Repair: A Literature Review
Ankit Rawat, Jyoti Nagpal, Shreeya Mehta, Divya Vyas, Abhishek Kumar, Fathima Amal
Journal of Research and Advancement in Dentistry.2021; 12(3): 6. CrossRef - Spectrophotometric assessment of Tooth discoloration induced by various Antibiotic pastes
Ravi Gupta, Radhika Kewalramani, Dishant Patel
Research Journal of Pharmacy and Technology.2021; : 1979. CrossRef - Comparative evaluation of calcium release of the apical plugs formed by mineral trioxide aggregate, Biodentine, and EndoSequence root repair material with and without 2% triple antibiotic powder: An in vitro study
PoojaNitin Mapara, ND Shashikiran, Sachin Gugawad, Namrata Gaonkar, Savita Hadakar, Swapnil Taur, Dhanshri Khade
Journal of Indian Society of Pedodontics and Preventive Dentistry.2020; 38(2): 132. CrossRef - Effect of triple antibiotic loaded apatitic nanocarriers on Enterococcus faecalis biofilm – An In vitro study
S. Nagarathinam, V. Sujatha, K. Madhumathi, S. Mahalaxmi, P.Pranav Vanajassun, T.S.Sampath Kumar
Journal of Drug Delivery Science and Technology.2019; 51: 499. CrossRef - Coronal tooth discoloration induced by regenerative endodontic treatment using different scaffolds and intracanal coronal barriers: a 6-month ex vivo study
Noushin Shokouhinejad, Hassan Razmi, Maryam Farbod, Marzieh Alikhasi, Josette Camilleri
Restorative Dentistry & Endodontics.2019;[Epub] CrossRef - Triple antibiotic paste: momentous roles and applications in endodontics: a review
Ardavan Parhizkar, Hanieh Nojehdehian, Saeed Asgary
Restorative Dentistry & Endodontics.2018;[Epub] CrossRef - Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part II: other clinical applications and complications
M. Torabinejad, M. Parirokh, P. M. H. Dummer
International Endodontic Journal.2018; 51(3): 284. CrossRef - Alternative to Avoid Tooth Discoloration after Regenerative Endodontic Procedure: A Systematic Review
Luciane Geanini Pena dos Santos, Luiz Alexandre Chisini, Camila Guerner Springmann, Beatriz Dulcineia Mendes de Souza, Fernanda Geraldo Pappen, Flávio Fernando Demarco, Mara Cristina Santos Felippe, Wilson Tadeu Felippe
Brazilian Dental Journal.2018; 29(5): 409. CrossRef - Regenerative Endodontic Treatment or Mineral Trioxide Aggregate Apical Plug in Teeth with Necrotic Pulps and Open Apices: A Systematic Review and Meta-analysis
Mahmoud Torabinejad, Ali Nosrat, Prashant Verma, Oyoyo Udochukwu
Journal of Endodontics.2017; 43(11): 1806. CrossRef - Revascularization in Immature Permanent Teeth with Necrotic Pulp and Apical Pathology: Case Series
López Carmen, Mendoza Asunción, Solano Beatriz, Yáñez-Vico Rosa, Jiiang H. Jeng
Case Reports in Dentistry.2017;[Epub] CrossRef
- Comparative evaluation of effect of modified triple antibiotic paste and calcium hydroxide as intracanal medicament on microhardness of root dentin: An in vitro study
- 3,159 View
- 14 Download
- 16 Crossref
 First
First Prev
Prev

