
Search
- Page Path
- HOME > Search
Research Article
- Influence of adjacent restorative material and distance on the accuracy of inlay cavity impressions with intraoral scanner: an in vitro study
- So-Yeon Lee, Sung-Ae Son, Jae-Hoon Kim, Deog-Gyu Seo, Jeong-Kil Park
- Restor Dent Endod 2026;51(1):e6. Published online January 23, 2026
- DOI: https://doi.org/10.5395/rde.2026.51.e6
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub - Objectives
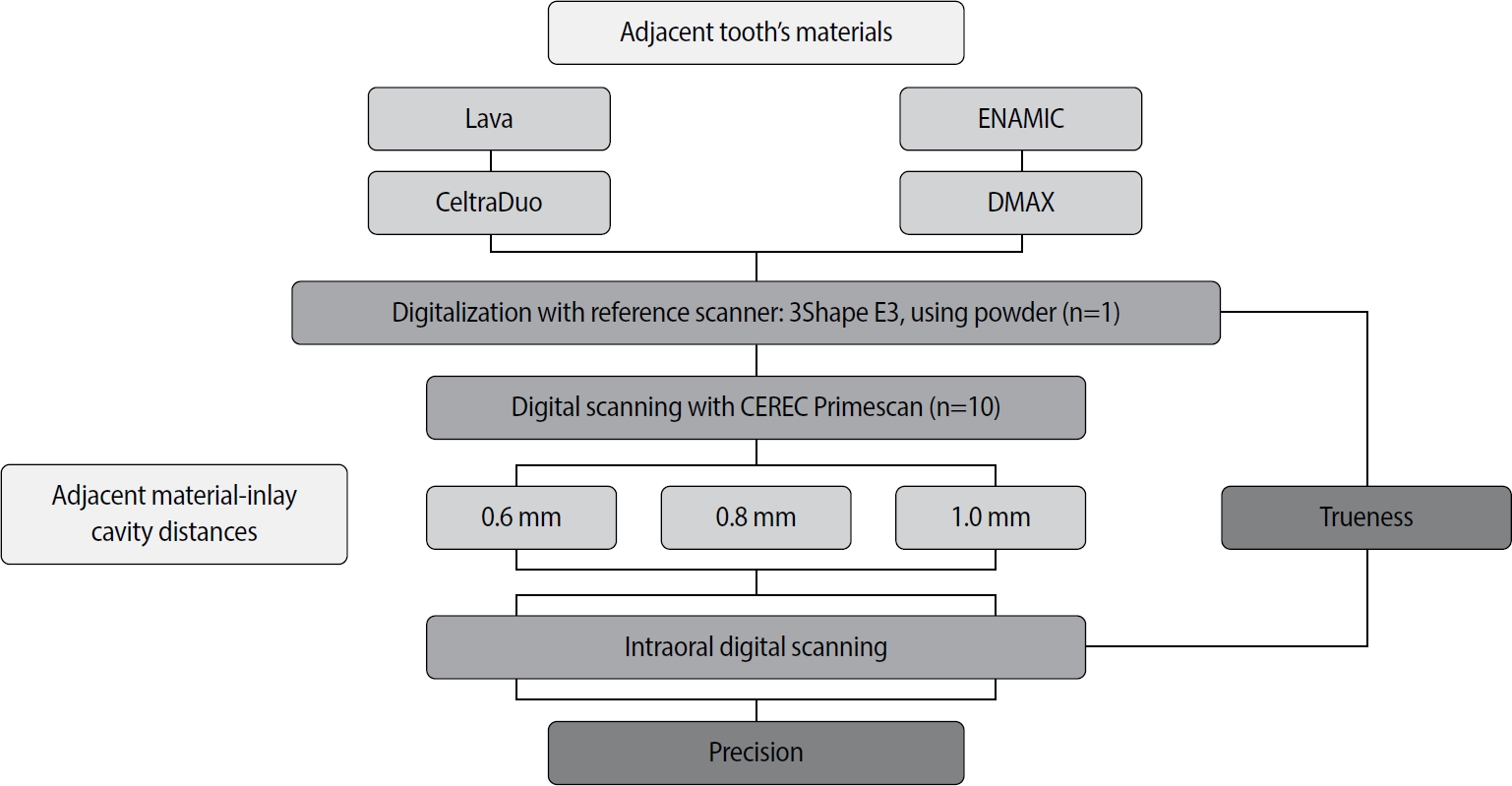
This study aimed to evaluate the influence of adjacent restorative material and interproximal distance on the accuracy of digital impressions of inlay cavities obtained using an intraoral scanner.
Methods
A disto-occlusal inlay cavity was prepared on a mandibular right first molar model, and digital scans were performed using a CEREC Primescan (Dentsply Sirona). The adjacent restorative materials used were Lava (3M ESPE), ENAMIC (VITA Zahnfabrik), Celtra Duo (Dentsply Sirona), and DMAX (DMAX), and the interproximal distances were set to 0.6 mm, 0.8 mm, and 1.0 mm. The obtained scan data were analyzed using GOM Inspect software (GOM GmbH).
Results
Trueness, maximum positive and negative deviations, and precision were significantly influenced by both the adjacent restorative material and the interproximal distance, while their interaction showed a significant effect only on precision. Celtra Duo demonstrated the highest trueness, with mean deviation values decreasing from 7.8 μm at a 0.6 mm interproximal distance to 7.3 μm at 1.0 mm. ENAMIC showed the best precision, presenting mean deviations of 2.6 μm at 0.6 mm, 2.9 μm at 0.8 mm, and 2.4 μm at 1.0 mm. A narrow interproximal distance of 0.6 mm resulted in lower trueness, measured at 8.3 μm, and the highest precision deviation of 3.4 μm. In contrast, an interproximal distance of 1.0 mm yielded improved scan accuracy, with increased trueness and reduced precision variation.
Conclusions
Digital impression accuracy of inlay cavities was influenced by adjacent restorative material and interproximal distance, suggesting clinical consideration is needed in CAD/CAM workflows to optimize restoration fit. -
Citations
Citations to this article as recorded by
- 3D-SCANNING IN PROSTHETIC DENTISTRY: ADVANTAGES, DISADVANTAGES, AND DEVELOPMENT PROSPECTS
V. S. Kuz, O. I. Teslenko, H. M. Kuz, H. M. Balia, Yu. S. Lunkova, O. V. Shemetov, I. M. Martynenko
Bulletin of Problems Biology and Medicine.2026; 1(1): 98. CrossRef
- 3D-SCANNING IN PROSTHETIC DENTISTRY: ADVANTAGES, DISADVANTAGES, AND DEVELOPMENT PROSPECTS
- 2,207 View
- 125 Download
- 1 Crossref

Review Article
- Epigenetics: general characteristics and implications for oral health
- Ji-Yun Seo, Yoon-Jung Park, Young-Ah Yi, Ji-Yun Hwang, In-Bog Lee, Byeong-Hoon Cho, Ho-Hyun Son, Deog-Gyu Seo
- Restor Dent Endod 2015;40(1):14-22. Published online November 13, 2014
- DOI: https://doi.org/10.5395/rde.2015.40.1.14
-
Abstract
PDFPubReaderePub
Genetic information such as DNA sequences has been limited to fully explain mechanisms of gene regulation and disease process. Epigenetic mechanisms, which include DNA methylation, histone modification and non-coding RNAs, can regulate gene expression and affect progression of disease. Although studies focused on epigenetics are being actively investigated in the field of medicine and biology, epigenetics in dental research is at the early stages. However, studies on epigenetics in dentistry deserve attention because epigenetic mechanisms play important roles in gene expression during tooth development and may affect oral diseases. In addition, understanding of epigenetic alteration is important for developing new therapeutic methods. This review article aims to outline the general features of epigenetic mechanisms and describe its future implications in the field of dentistry.
-
Citations
Citations to this article as recorded by- Embracing change: Chemical modifications of nucleic acid bases as epigenetic marks
Nishu Nain, Shoaib Khan, Priyanka Phogat, Aparna Bansal, Shrikant Kukreti
Next Research.2026; 5: 101292. CrossRef - Holobiontic Intercellular Relationships Between the Oral Cavity and the Rest of the Human Organism: A Narrative Review
Vasile Burlui, Daniela Luminița Ichim, Daniela Ivona Tomița, Malina Visternicu, Alin Ciobica, Mihaela Diana Gheban
Medicina.2026; 62(7): 1365. CrossRef - Conversation between skin microbiota and the host: from early life to adulthood
Jimin Cha, Tae-Gyun Kim, Ji-Hwan Ryu
Experimental & Molecular Medicine.2025; 57(4): 703. CrossRef - Identification of two novel variants in homeodomain of
MSX1 associated with oligodontia
Ting Zeng, Xiuyou Wang, Li Xu, Xin Dong, Xili Qiu, Zhiyuan Deng, Saimin Pei, Rong Lei, Yuehong Wang, Ling Peng
Oral Science and Homeostatic Medicine.2025; 1(2): 9610029. CrossRef - DNA Methylation of COX‐2, IFN‐γ, TNF‐α, and LINE‐1 in Clinically Stable Periodontal Tissues Following Periodontal Therapy
Giulio Rasperini, Koki Yoshida, Alessandro Martinotti, Valentina Bollati, Letizia Tarantini, Farah Asa'ad
Clinical and Experimental Dental Research.2025;[Epub] CrossRef - Effect of Long Non-coding RNA and DNA Methylation on Gene Expression in Dental Fluorosis
Xiaoyan Hu, Huiru Li, Minzhi Yang, Yujiong Chen, Ailin Zeng, Jiayuan Wu, Jian Zhang, Yuan Tian, Jing Tang, Shengyan Qian, Mingsong Wu
Biological Trace Element Research.2024; 202(1): 221. CrossRef - MicroRNAs: Mighty Mite RNAs in Oral Diseases
Devapriya Appukuttan, P. S. G. Prakash
Journal of Interdisciplinary Dentistry.2024; 14(3): 145. CrossRef - Role of epigenetics in OSCC: an understanding above genetics
Priyanka P. Vatsa, Yogita Jindal, Janhavi Bhadwalkar, Ambika Chamoli, Vinal Upadhyay, Amit Mandoli
Medical Oncology.2023;[Epub] CrossRef - Downregulation of miRNA‐26 in chronic periodontitis interferes with innate immune responses and cell migration by targeting phospholipase C beta 1
Juhi R. Uttamani, Afsar R. Naqvi, Araceli Maria Valverde Estepa, Varun Kulkarni, Maria F. Brambila, Gloria Martínez, Gabriela Chapa, Christine D. Wu, Wei Li, Sona Rivas‐Tumanyan, Salvador Nares
Journal of Clinical Periodontology.2023; 50(1): 102. CrossRef - The Potential Role of Epigenetic Modifications on Different Facets in the Periodontal Pathogenesis
Samuel Laberge, Daniel Akoum, Piotr Wlodarczyk, Jean-Daniel Massé, Dominique Fournier, Abdelhabib Semlali
Genes.2023; 14(6): 1202. CrossRef - The Role of Histone Acetylation Modification in Dental Tissue-Derived Mesenchymal Stem Cells and Odontogenesis
Haoling Chen, Zijing Huang, Chuxiao Chen
Cellular Reprogramming.2023; 25(1): 11. CrossRef - Your health is in your mouth: A comprehensive view to promote general wellness
Antonia Barranca-Enríquez, Tania Romo-González
Frontiers in Oral Health.2022;[Epub] CrossRef - A Brief Landscape of Epigenetic Mechanisms in Dental Pathologies
Wojciech Tynior, Joanna Katarzyna Strzelczyk
Cytology and Genetics.2022; 56(5): 475. CrossRef - Influence of epigenetics on periodontitis and peri‐implantitis pathogenesis
Lena Larsson, Nolan M. Kavanagh, Trang V. N. Nguyen, Rogerio M. Castilho, Tord Berglundh, William V. Giannobile
Periodontology 2000.2022; 90(1): 125. CrossRef - DNA methylation alterations and their potential influence on macrophage in periodontitis
Yiyang Jiang, Jingfei Fu, Juan Du, Zhenhua Luo, Lijia Guo, Junji Xu, Yi Liu
Oral Diseases.2022; 28(2): 249. CrossRef - Stabilizing and Anti-Repressor Elements Effectively Increases Transgene Expression in Transfected CHO Cells
Qin Li, Rui-Fang Yan, Yong-Xiao Yang, Chun-liu Mi, Yan-long Jia, Tian-Yun Wang
Frontiers in Bioengineering and Biotechnology.2022;[Epub] CrossRef - Synthesis and Anticancer Potential of New Hydroxamic Acid Derivatives as Chemotherapeutic Agents
Işıl Nihan Korkmaz, Hasan Özdemir
Applied Biochemistry and Biotechnology.2022; 194(12): 6349. CrossRef - Impact of Epigenetic Alterations in the Development of Oral Diseases
Rodopi Emfietzoglou, Evangelos Pachymanolis, Christina Piperi
Current Medicinal Chemistry.2021; 28(6): 1091. CrossRef - Basics of Epigenetics and Role of Epigenetics in Diabetic Complications
Andamuthu Yamunadevi, Ramani Pratibha, Muthusamy Rajmohan, Sengottaiyan Mahendraperumal, Nalliappan Ganapathy
Journal of Pharmacy and Bioallied Sciences.2021; 13(Suppl 1): S336. CrossRef - Effects of Epigenetic Regulation on Cancer
Muhammet Mesut Nezir ENGİN, Esra ÖZEN ENGİN, Recep ERÖZ, Gorkem DULGER, Hüseyin YÜCE
Journal of Biotechnology and Strategic Health Research.2021; 5(1): 1. CrossRef - Photobiomodulation therapy improves human dental pulp stem cell viability and migration in vitro associated to upregulation of histone acetylation
Ivana M. Zaccara, Letícia B. Mestieri, Emily F. S. Pilar, Maria S. Moreira, Fabiana S. Grecca, Manoela D. Martins, Patrícia Maria Poli Kopper
Lasers in Medical Science.2020; 35(3): 741. CrossRef - The Biology of Social Adversity Applied to Oral Health
N. Gomaa, H. Tenenbaum, M. Glogauer, C. Quiñonez
Journal of Dental Research.2019; 98(13): 1442. CrossRef - The effect of DNA methylation on the miRNA expression pattern in lipopolysaccharide-induced inflammatory responses in human dental pulp cells
Zehuan Mo, Qimeng Li, Luhui Cai, Minkang Zhan, Qiong Xu
Molecular Immunology.2019; 111: 11. CrossRef - One-Carbon Metabolism Links Nutrition Intake to Embryonic Development via Epigenetic Mechanisms
Si Wu, Jun Zhang, Feifei Li, Wei Du, Xin Zhou, Mian Wan, Yi Fan, Xin Xu, Xuedong Zhou, Liwei Zheng, Yachuan Zhou
Stem Cells International.2019; 2019: 1. CrossRef - Epigenetic regulation in dental pulp inflammation
T Hui, C Wang, D Chen, L Zheng, D Huang, L Ye
Oral Diseases.2017; 23(1): 22. CrossRef - Current Concepts of Epigenetics and Its Role in Periodontitis
Lena Larsson
Current Oral Health Reports.2017; 4(4): 286. CrossRef - The periodontal war: microbes and immunity
Jeffrey L. Ebersole, Dolph Dawson, Pinar Emecen‐Huja, Radhakrishnan Nagarajan, Katherine Howard, Martha E. Grady, Katherine Thompson, Rebecca Peyyala, Ahmad Al‐Attar, Kathryn Lethbridge, Sreenatha Kirakodu, Octavio A. Gonzalez
Periodontology 2000.2017; 75(1): 52. CrossRef - Epigenetic regulatory elements: Recent advances in understanding their mode of action and use for recombinant protein production in mammalian cells
Niamh Harraghy, David Calabrese, Igor Fisch, Pierre‐Alain Girod, Valérie LeFourn, Alexandre Regamey, Nicolas Mermod
Biotechnology Journal.2015; 10(7): 967. CrossRef - Protocol for assessing maternal, environmental and epigenetic risk factors for dental caries in children
Surani Fernando, David J. Speicher, Mahmoud M. Bakr, Miles C. Benton, Rodney A. Lea, Paul A. Scuffham, Gabor Mihala, Newell W. Johnson
BMC Oral Health.2015;[Epub] CrossRef
- Embracing change: Chemical modifications of nucleic acid bases as epigenetic marks
- 3,573 View
- 32 Download
- 29 Crossref
Readers' Forum
- Zirconia surface treatment for successful bonding
- Deog-Gyu Seo
- Restor Dent Endod 2014;39(4):333-333. Published online August 25, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.4.333
-
PDFPubReaderePub
-
Citations
Citations to this article as recorded by- Comparative effect of Zircos‐E and airborne‐particle abrasion on zirconia surface treatment: A meta‐analysis
Osayd Alawawda, Husam Altalla, Funda Bayindir
Journal of Prosthodontics.2025;[Epub] CrossRef - Shear bond strength of metallic orthodontic brackets to zirconium crowns treated by sandblasting compared to enamel using a universal adhesive: An in vitro study
Fatemeh Namvar, Mansoure Zarmehi Shahrebabak, Sepideh Arab, Maryam Abdoh Tabrizi, Amir Ghasemi, Fatemeh Safari
International Orthodontics.2022; 20(2): 100640. CrossRef - The effect of fusion sputtering surface treatment on microshear bond strength of zirconia and MDP-containing resin cement
Nesma Ali, Ahmed Safwat, Moustafa Aboushelib
Dental Materials.2019; 35(6): e107. CrossRef - Effects of air-abrasion pressure on the resin bond strength to zirconia: a combined cyclic loading and thermocycling aging study
Eman Z. Al-Shehri, Afnan O. Al-Zain, Alaa H. Sabrah, Sarah S. Al-Angari, Laila Al Dehailan, George J. Eckert, Mutlu Özcan, Jeffrey A. Platt, Marco C. Bottino
Restorative Dentistry & Endodontics.2017; 42(3): 206. CrossRef - Shear Bond Strength of MDP-Containing Self-Adhesive Resin Cement and Y-TZP Ceramics: Effect of Phosphate Monomer-Containing Primers
Jin-Soo Ahn, Young-Ah Yi, Yoon Lee, Deog-Gyu Seo
BioMed Research International.2015; 2015: 1. CrossRef - Preliminary studies on the effects of in situ synthesized polycrystalline particulates on the bonding strength of resin to zirconia ceramic surface
Yueming Tian, Lingling Zhang, Zutai Zhang, Ning Ding, Yan Liu, Guozhong Tian
Applied Surface Science.2015; 357: 961. CrossRef
- Comparative effect of Zircos‐E and airborne‐particle abrasion on zirconia surface treatment: A meta‐analysis
- 2,242 View
- 9 Download
- 6 Crossref
Review Article
- Thermal irritation of teeth during dental treatment procedures
- Su-Jung Kwon, Yoon-Jung Park, Sang-Ho Jun, Jin-Soo Ahn, In-Bog Lee, Byeong-Hoon Cho, Ho-Hyun Son, Deog-Gyu Seo
- Restor Dent Endod 2013;38(3):105-112. Published online August 23, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.3.105
-
Abstract
PDFPubReaderePub
While it is reasonably well known that certain dental procedures increase the temperature of the tooth's surface, of greater interest is their potential damaging effect on the pulp and tooth-supporting tissues. Previous studies have investigated the responses of the pulp, periodontal ligament, and alveolar bone to thermal irritation and the temperature at which thermal damage is initiated. There are also many
in vitro studies that have measured the temperature increase of the pulp and tooth-supporting tissues during restorative and endodontic procedures. This review article provides an overview of studies measuring temperature increases in tooth structures during several restorative and endodontic procedures, and proposes clinical guidelines for reducing potential thermal hazards to the pulp and supporting tissues.-
Citations
Citations to this article as recorded by- Impact of Various Sleeve Materials on Temperature Variations During Guided Endodontic Access Cavity Preparation Utilizing Finite‐Element Analysis
Anna Muryani, Wandi Prasetia, Dudi Aripin, Hendra Dian Adhita Dharsono, Zainul Ahmad Rajion, Satrio Wicaksono
Clinical and Experimental Dental Research.2026;[Epub] CrossRef - Comparative evaluation of microcrack formation and fracture resistance of root dentin with the use of three different rotary files: An in vitro study
Paridhi Maheshwari, Sayantan Mukherjee, Ipsita Maity, Paromita Mazumdar
Journal of Oral Research and Review.2026; 18(1): 59. CrossRef - Infrared thermographic evaluation of root surface during warm vertical compaction technique
Aysenur Oncu, Ecem Ozgur, Merve Sarı, Pelin Tufenkci, Berkan Celikten
European Journal of Oral Sciences.2026;[Epub] CrossRef - Effects of voltage reduction on changes of shear bond strength and fracture mode of resin-modified glass-ionomer cements after current application
Ryouhei WADA, Emi TAKEGAWA-UYAMA, Shinya HORIUCHI, Kazumitsu SEKINE, Eiji TANAKA, Kenichi HAMADA
Dental Materials Journal.2026; 45(3): 284. CrossRef - Inverse Heat Conduction Estimation of Heat Flux in Human Dentin from Dental Curing Lights Using the Conjugate Gradient Method
Ahmad Soori, Farshad Kowsary, Shadab Safarzadeh Khosroshahi, Mohammad Vahedi
International Journal of Thermophysics.2026;[Epub] CrossRef - Temperature Variations on the External Root Surface During Warm Injectable Gutta-Percha Obturation at Different Thermo-Plasticization Settings: An In Vitro Study
Mihai Paven, Adrian-George Marinescu, Osama Abuabboud, Laura-Elena Cîrligeriu, Luminița-Maria Nica, Bianca Georgiana Cărăbiș, Izabella Maria Kovacs, Oana-Alexandra Velea-Barta, Roxana Oancea
Medicina.2026; 62(6): 1159. CrossRef - Deviation analysis of guided fiber post removal using an assembled sleeveless guide system: A case series
Jingqi Zhu, Siyi Mo, Yuan Li, Yaojun Zhang, Xutong Song, Jingwen Liu, Ye Cao, Xiaoxiang Xu
The Journal of Prosthetic Dentistry.2026;[Epub] CrossRef - External Root Temperature and Its Relationship With Dentin Thickness During Gutta-Percha Removal Procedures With Ultrasound. An Ex Vivo Study
Juan Ramon Salazar-Silva, Carlos Emilio Paschoal, Daniela de Fatima Teixeira da Silva, Denise Maria Zezell, Fábio Luiz Cunha D'Assuncao, Celso Luiz Caldeira
Journal of Endodontics.2025; 51(3): 340. CrossRef - Temperature Changes of NaOCl after Irrigation Using Passive Ultrasonic Irrigation, Easy Clean, and XP-Endo Finisher: A Randomized Crossover Clinical Trial
Geraldo Edson Freitas Athayde de Moraes, Daniel Guimarães Pedro Rocha, Carlos Eduardo Fontana, Rina Andréa Pelegrine, Alexandre Sigrist de Martin, Índia Olinta De Azevedo Queiroz, Carlos Eduardo da Silveira Bueno
European Journal of Dentistry.2025; 19(03): 660. CrossRef - Real‐Time Analysis of Changes in Internal and External Root Temperatures Using Different Systems for Activating the Irrigation Solution
Maria Eduarda Paz Dotto, Julia Menezes Savaris, Luiz Carlos de Lima Dias-Junior, Tamer Ferreira Schmidt, Lucas da Fonseca Roberti Garcia, Cleonice da Silveira Teixeira, Eduardo Antunes Bortoluzzi, Paolo Francesco Manicone
International Journal of Dentistry.2025;[Epub] CrossRef - Thermal Behaviour of Teeth With Internal Root Resorption During Obturation and Enhancing Thermal Simulations: A Finite-Element Analysis
Alper Kabakci, Ayca Yilmaz, Dilek Helvacioglu-Yigit, Nawar Naguib Nawar, Hyeon-Cheol Kim
International Dental Journal.2025; 75(6): 103903. CrossRef - Determination of a safe protocol for using laser ablation with indocyanine green dye in endodontic treatment. In vitro, in vivo and human study
Renato de Toledo Leonardo, Mirtha Perdomo, Marcelo Costa Perdomo, María Betania Acevedo Giménez, Celso Kenji Nishiyama, Fernando Accorsi Orosco, Arturo Javier Aranda Garcia, Carolina Sayuri Wajima, Cristiane Cantiga-Silva, Ana Maria Veiga Vasques, Flávio
Lasers in Medical Science.2025;[Epub] CrossRef - Antibacterial PEEK-Ag Surfaces: Development and In Vitro Evaluation Against Staphylococcus aureus and Pseudomonas aeruginosa
Flávio Rodrigues, Mariana Fernandes, Filipe Samuel Silva, Óscar Carvalho, Sara Madeira
Journal of Functional Biomaterials.2025; 16(10): 388. CrossRef - The effect of di̇fferent preheati̇ng methods on the intrapulpal temperature of bulk-fi̇ll composi̇te resi̇ns
Hilal Ateş, Merve İşcan Yapar
BMC Oral Health.2025;[Epub] CrossRef - Comparative evaluation of increase in temperature on the external root surface of teeth during retrieval of broken NiTi instrument using two ultrasonic tips and two power settings: An in vitro study
Ashish K. Jain, Rishabhkumar Jain, Rahul Rao, Prajakta Rao, Pooja Yadav, Vinayak Thorat
Journal of Conservative Dentistry and Endodontics.2024; 27(6): 634. CrossRef - Dental health concerns for patients suffering from facial, peri-oral burns, and inhalation injury: A persistent yet underappreciated challenge
Hans-Oliver Rennekampff, Isabelle Rennekampff, Mayer Tenenhaus
Burns.2024; 50(9): 107224. CrossRef - Recent advances in the pathogenesis and prevention strategies of dental calculus
Yu Wei, Gao-peng Dang, Zhao-yang Ren, Mei-chen Wan, Chen-yu Wang, Hong-bo Li, Tong Zhang, Franklin R. Tay, Li-na Niu
npj Biofilms and Microbiomes.2024;[Epub] CrossRef - In Vitro Evaluation of Root Surface Temperature Using Different Endodontic Filling Techniques
Lea Külzer, Theresia Saban, Andreas Braun, Johannes-S. Wenzler
Applied Sciences.2024; 14(21): 9830. CrossRef - Accuracy comparison of single- and double-sleeve endodontic guides for fiber post removal
Omid Dianat, Mandana Naseri, Yaser Safi, Ali Modaberi, Nazanin Zargar, Ove A. Peters, Mehran Farajollahi
BMC Oral Health.2024;[Epub] CrossRef - The Effect of Water Coolant and Bur Type on Pulp Temperature When Removing Tooth Structure and Restorative Dental Materials
C Mafrici, M Kingston, R Grice, PV Abbott
Operative Dentistry.2024; 49(1): 91. CrossRef - A Comparative Study of Temperature Variations in Incisor Root Surfaces During Root Canal Preparation Using Various Rotary Systems and Irrigation Protocols
Mihai Paven, Adrian-George Marinescu, Osama Abuabboud, Laura-Elena Cirligeriu, Luminita Maria Nica, Vlad Tiberiu Alexa, Ruxandra Sava Rosianu, Atena Galuscan, Roxana Oancea
Journal of Clinical Medicine.2024; 13(23): 7484. CrossRef - The Effect of Restoration Polymerization and Residual Dentine Thickness on Thermal Changes of Pulp Chamber of Immature Permanent Teeth
Kevser Kolçakoğlu, Merve Aksoy, Cenkhan Bal, Akif Demirel, Firdevs Tulga Öz
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2024;[Epub] CrossRef - Efficacy of pulpotomy in managing irreversible pulpitis in mature permanent teeth: A systematic review and meta-analysis
Yuanyuan Li, Wenying Wang, Qian Zeng, Michelle Tang, Joshua Massey, Brian E. Bergeron, Lisha Gu, Franklin R. Tay
Journal of Dentistry.2024; 144: 104923. CrossRef - Evaluation of diamond rotary instruments marketed for removing zirconia restorations
Severin Hunziker, Lea Thorpe, Nicola U. Zitzmann, Nadja Rohr
The Journal of Prosthetic Dentistry.2024; 131(5): 895. CrossRef - Influence of different cutting instruments and rotational speeds on heat generation and cutting efficiency when sectioning different types of zirconia
Lisa Türp, Frank Lehmann, Sebastian Wille, Matthias Kern
Journal of the Mechanical Behavior of Biomedical Materials.2024; 160: 106715. CrossRef - Loss of pulp vitality correlated with the duration of the interim restoration and the experience of the dentist: A retrospective study
Göran Nilsson, Stefan Ellner, Liselott Arnebrant, Lars Brudin, Christel Larsson
The Journal of Prosthetic Dentistry.2023; 130(6): 833. CrossRef - Thermal Sensing of Photo-Activated Dental Resin Composites Using Infrared Thermography
Turki A. Bakhsh, Abdulaziz Alfaifi, Yousef Alghamdi, Mohannad Nassar, Roaa A. Abuljadyel
Polymers.2023; 15(20): 4117. CrossRef - Effect of irrigation acid solutions on cleaning and bond strength to post‐space dentin
C. de Melo Alencar, J. Ferrari Zaniboni, J. Felipe Besegato, A. Patricia Oliveira Barros, M. Bena Gélio, L Garcia Belizário, E. Maximiliano Fernandez Godoy, M. Carlos Kuga
European Journal of Oral Sciences.2023;[Epub] CrossRef - Effect of Intermediate Irrigation on Temperature Rise during Broken NiTi File Removal Using Ultrasonic Device
László Pintér, Károly Krajczár, Fanni Őry, József Szalma, Edina Lempel
Applied Sciences.2023; 13(17): 9761. CrossRef - Top tips for improving crown preparations
James Baker, Ewen McColl, Christopher Tredwin
British Dental Journal.2023; 234(1): 16. CrossRef - Evaluation of knowledge and awareness of pediatric oral health among school teachers of Hazaribag before and after oral health education.
Vipin Ahuja, Annapurna Ahuja, Nilima Thosar
F1000Research.2023; 12: 1292. CrossRef - Applications of single laser pulse from Nd:doped lasers for cleaning of small diameter carious lesions. Modelling and analytical study
T Uzunov, M Deneva, P Uzunova, M Nenchev
Journal of Physics: Conference Series.2023; 2487(1): 012022. CrossRef - Accuracy of a 3D printed sleeveless guide system used for fiber post removal: An in vitro study
Siyi Mo, Yongwei Xu, Lei Zhang, Ye Cao, Yongsheng Zhou, Xiaoxiang Xu
Journal of Dentistry.2023; 128: 104367. CrossRef - Heat generated during dental treatments affecting intrapulpal temperature: a review
Xin Er Lau, Xiaoyun Liu, Helene Chua, Wendy Jingwen Wang, Maykon Dias, Joanne Jung Eun Choi
Clinical Oral Investigations.2023; 27(5): 2277. CrossRef - Pulp chamber temperature rise in light-cure bonding of brackets with and without primer, in intact versus restored teeth
Gabriela Cenci SCHMITZ, Fernanda de Souza HENKIN, Mauricio MEZOMO, Mariana MARQUEZAN, Gabriela BONACINA, Maximiliano Schünke GOMES, Eduardo Martinelli Santayana de LIMA
Dental Press Journal of Orthodontics.2023;[Epub] CrossRef - Temperature Rise in Curing Modes of Two Different Dental Light-Curing Units: The Importance of Heating Rate
Ahmad Soori, Faezeh Soori, Farshad Kowsary, Shahin Kasraei
International Journal of Thermophysics.2023;[Epub] CrossRef - Effective application of suitable single pulse of Nd:doped lasers for cleaning of initial carious lesions of human teeth. Experimental study
T Uzunov, M Deneva, V Kazakov, P Uzunova, N Kaimakanova, M Nenchev
Journal of Physics: Conference Series.2023; 2487(1): 012021. CrossRef - Comparative Evaluation of Intrapulpal Thermal Changes during the Polymerization of Different Adhesive Resin Materials: An In Vitro Study
Pavithra K Ramanna, Suneel V Vadavadagi, Konsam Bidya Devi, Pawankumar Kamalapurkar, Shreeshail Indi, Vineetha Chakravarthy Srinivas
The Journal of Contemporary Dental Practice.2022; 23(5): 539. CrossRef - Anesthetic-, irrigation- and pain-free dentistry? The case for a femtosecond laser enabled intraoral robotic device
Ludovic Rapp, Steve Madden, Andrei V. Rode, Laurence J. Walsh, Heiko Spallek, Quan Nguyen, Van Dau, Peter Woodfield, Dzung Dao, Omar Zuaiter, Alaa Habeb, Timothy R. Hirst
Frontiers in Dental Medicine.2022;[Epub] CrossRef - 4D Printing of Shape‐Memory Semi‐Interpenetrating Polymer Networks Based On Aromatic Heterochain Polymers
Kseniia N. Bardakova, Bato Ch. Kholkhoev, Ivan A. Farion, Evgenii O. Epifanov, Olga S. Korkunova, Yuri M. Efremov, Nikita V. Minaev, Anna B. Solovieva, Peter S. Timashev, Vitaliy F. Burdukovskii
Advanced Materials Technologies.2022;[Epub] CrossRef - How does indirect air-cooling influence pulp chamber temperature in different volume teeth and absence/presence of resin-based composite during light curing?
Mathieu Mouhat, Lina Stangvaltaite-Mouhat, Emil Finnäs, Amani Andersen, Anneli Lirhus Evertsen, Bo W. Nilsen
BMC Oral Health.2022;[Epub] CrossRef - Intrapulpal temperature changes during the cementation of ceramic veneers
Edina Lempel, Dóra Kincses, Donát Szebeni, Dóra Jordáki, Bálint Viktor Lovász, József Szalma
Scientific Reports.2022;[Epub] CrossRef - Femtosecond laser dentistry for precise and efficient cavity preparation in teeth
Ludovic Rapp, Steve Madden, Julia Brand, Laurence J. Walsh, Heiko Spallek, Omar Zuaiter, Alaa Habeb, Timothy R. Hirst, Andrei V. Rode
Biomedical Optics Express.2022; 13(9): 4559. CrossRef - Three Dimensional mapping of the root apex: distances between apexes and anatomical structures and external cortical plates
Carlos Henrique FERRARI, Amjad ABU HASNA, Frederico Canato MARTINHO
Brazilian Oral Research.2021;[Epub] CrossRef - Effects of 9,300 nm Carbon Dioxide Laser on Dental Hard Tissue: A Concise Review
Vicky Wenqing Xue, Irene Shuping Zhao, Iris Xiaoxue Yin, John Yun Niu, Edward Chin Man Lo, Chun Hung Chu
Clinical, Cosmetic and Investigational Dentistry.2021; Volume 13: 155. CrossRef - PHOTOPOLYMERIZED COMPOSITIONS AND LIGHT SOURCES FOR DENTAL PRACTICE (REVIEW)
A. M. Lalatovich, M. A. Vaniev, N. V. Sidorenko, Y. A. Makedonova, D. Yu. Dyachenko, S. V. Dyachenko
IZVESTIA VOLGOGRAD STATE TECHNICAL UNIVERSITY.2021; (12(259)): 7. CrossRef - Spray mist reduction by means of a high-volume evacuation system—Results of an experimental study
Martin Koch, Christian Graetz, Essam Al-Moraissi
PLOS ONE.2021; 16(9): e0257137. CrossRef - Pulp chamber temperature changes during orthodontic bonding – an in vitro study
Aysegul Ayhan Bani, Burcu Balos Tuncer, Cumhur Tuncer
Australasian Orthodontic Journal.2021; 37(2): 157. CrossRef - Thermal Behavior of Teeth During Restoration Procedure With Composite: Experimental Tests and Numerical Simulation
M. Potenza, P. Coppa, L. Cerroni, G. Bovesecchi
Journal of Heat Transfer.2021;[Epub] CrossRef - Comparative Evaluation of Thermal Alterations on External Root Surface during Mechanical Instrumentation and Thermoplasticized Gutta-percha Obturation: An Ex Vivo Study
Rohit Sharma, Atul Jain, Madhurima Sharma, Shivani Chauhan, Abhinay Agarwal
World Journal of Dentistry.2021; 12(5): 367. CrossRef - Degree of conversion and in vitro temperature rise of pulp chamber during polymerization of flowable and sculptable conventional, bulk-fill and short-fibre reinforced resin composites
Edina Lempel, Zsuzsanna Őri, Dóra Kincses, Bálint Viktor Lovász, Sándor Kunsági-Máté, József Szalma
Dental Materials.2021; 37(6): 983. CrossRef - Pulp chamber temperature changes during orthodontic bonding – an in vitro study
Aysegul Ayhan Bani, Burcu Balos Tuncer, Cumhur Tuncer
Australasian Orthodontic Journal.2021; 37(2): 157. CrossRef - Shot peening increases resistance to cyclic fatigue fracture of endodontic files
Javier Nino-Barrera, Jose Sanchez-Aleman, Manuel Acosta-Humanez, Luis Gamboa-Martinez, Carlos Cortes-Rodriguez
Scientific Reports.2021;[Epub] CrossRef - Temperature Dependence of Specific Heat of Human Enamel and Dentin: An Experimental Study
Ahmad Soori, Farshad Kowsary, Shahin Kasraei
International Journal of Thermophysics.2021;[Epub] CrossRef - Prosthodontic Applications of Polymethyl Methacrylate (PMMA): An Update
Muhammad Sohail Zafar
Polymers.2020; 12(10): 2299. CrossRef - The effect of halogen bulb and light-emitting diode light curing units on temperature increase and fibroblast viability
Georgia Memari Trava, Juliane Almeida Santos, Lucas Paula Ramos, Pamela Beatriz Rosário Estevam dos Santos, Amjad Abu Hasna, Karen Cristina Yui, Adriano Bressane, Luciane Dias de Oliveira, Marianne Spalding
F1000Research.2020; 9: 1369. CrossRef - A Study on Temperature Changes during Bone Scaling and Cutting of Dental Ultrasonic Scaling/Surgery System
Min-Woo Sa, Tae-Jo Ko, Jong Young Kim
Journal of the Korean Society of Manufacturing Process Engineers.2020; 19(2): 1. CrossRef - Controlling In Vivo, Human Pulp Temperature Rise Caused by LED Curing Light Exposure
DC Zarpellon, P Runnacles, C Maucoski, U Coelho, FA Rueggeberg, CAG Arrais
Operative Dentistry.2019; 44(3): 235. CrossRef - Pulp Temperature Rise Induced by Light-Emitting Diode Light-Curing Units Using an Ex Vivo Model
Alexandra Vinagre, João Ramos, Clara Rebelo, José Basto, Ana Messias, Nélia Alberto, Rogério Nogueira
Materials.2019; 12(3): 411. CrossRef - The cooling efficiency of different dental high-speed handpiece coolant port designs
Helene Chua, Joanne Jung Eun Choi, Rishi Sanjay Ramani, Ritu Ganjigatti, John Neil Waddell
Heliyon.2019; 5(8): e02185. CrossRef - Polymerisation Shrinkage Profiling of Dental Composites using Optical Fibre Sensing and their Correlation with Degree of Conversion and Curing Rate
Ginu Rajan, Raju Raju, Sagar Jinachandran, Paul Farrar, Jiangtao Xi, B. Gangadhara Prusty
Scientific Reports.2019;[Epub] CrossRef - Tooth sectioning for coronectomy: how to perform?
József Szalma, László Vajta, Lajos Olasz, Edina Lempel
Clinical Oral Investigations.2019; 23(2): 519. CrossRef - Dentistry Applications of Fiber Bragg Gratings: Irradiation Protocols for Bulk Fill Flow Dental Composites
Ana Paula Gebert de Oliveira Franco, Manoella Maria Machado Costa, Leandro Zen Karam, Osnara Maria Mongruel Gomes, Hypolito Jose Kalinowski
Journal of Lightwave Technology.2019; 37(18): 4881. CrossRef - In Vitro Analysis of Techniques that Alter the Surface Hardness of a Glass Ionomer Restorative Material
Riaan Mulder, Naeemah Noordien, Shaun Rossouw, Luzaan van Zyl
The Journal of Contemporary Dental Practice.2019; 20(12): 1362. CrossRef - Changes in the radicular pulp-dentine complex in healthy intact teeth and in response to deep caries or restorations: A histological and histobacteriological study
Domenico Ricucci, Simona Loghin, Li-na Niu, Franklin R. Tay
Journal of Dentistry.2018; 73: 76. CrossRef - Effect of Irradiance and Exposure Duration on Temperature and Degree of Conversion of Dual-Cure Resin Cement for Ceramic Restorations
JS Shim, SH Han, N Jha, ST Hwang, W Ahn, JY Lee, JJ Ryu
Operative Dentistry.2018; 43(6): E280. CrossRef - Protective Effects of Base Cements against Intrapulpal Temperature Rise during Curing of Composite Resins: An In Vitro Study by Pulpal Blood Microcirculation Model
Ihsan F Ertugrul, Basak Yazkan, Ceylan Ç Ertugrul
International Journal of Experimental Dental Science.2018; 7(2): 85. CrossRef - Thermal imaging of the pulp during residual adhesive removal
Gökmen Kurt, Nisa Gül, Özgür Er, Gülşen Çakmak, Emre Bendeş, Veysel Aslantaş
Journal of Orofacial Orthopedics / Fortschritte der Kieferorthopädie.2017; 78(4): 330. CrossRef - Influence of the material for preformed moulds on the polymerization temperature of resin materials for temporary FPDs
Philipp-Cornelius Pott, Hans Schmitz-Wätjen, Meike Stiesch, Michael Eisenburger
The Journal of Advanced Prosthodontics.2017; 9(4): 294. CrossRef - Light curing in dentistry and clinical implications: a literature review
Frederick Allen RUEGGEBERG, Marcelo GIANNINI, Cesar Augusto Galvão ARRAIS, Richard Bengt Thomas PRICE
Brazilian Oral Research.2017;[Epub] CrossRef - Intrapulpal temperature changes during curing of different bulk-fill restorative materials
Elif YASA, Cigdem ATALAYIN, Gamze KARACOLAK, Tugrul SARI, L. Sebnem TURKUN
Dental Materials Journal.2017; 36(5): 566. CrossRef - Can Mineral Trioxide Aggregate and Nanoparticulate EndoSequence Root Repair Material Produce Injurious Effects to Rat Subcutaneous Tissues?
Wafaa A. Khalil, Siham K. Abunasef
Journal of Endodontics.2015; 41(7): 1151. CrossRef - Comparison of photopolymerization temperature increases in internal and external positions of composite and tooth cavities in real time: Incremental fillings of microhybrid composite vs. bulk filling of bulk fill composite
Ryan Jin-Young Kim, Sung-Ae Son, Ji-Yun Hwang, In-Bog Lee, Deog-Gyu Seo
Journal of Dentistry.2015; 43(9): 1093. CrossRef - Real-Time Analysis of Temperature Changes in Composite Increments and Pulp Chamber during Photopolymerization
Ryan Jin-Young Kim, In-Bog Lee, Jin-Young Yoo, Su-Jung Park, Sin-Young Kim, Young-Ah Yi, Ji-Yun Hwang, Deog-Gyu Seo
BioMed Research International.2015; 2015: 1. CrossRef - Temperature changes under demineralized dentin during polymerization of three resin-based restorative materials using QTH and LED units
Sayed-Mostafa Mousavinasab, Maryam Khoroushi, Mohammadreza Moharreri, Mohammad Atai
Restorative Dentistry & Endodontics.2014; 39(3): 155. CrossRef - Comparison of Exothermic Release during the Polymerization of Four Materials used to fabricate Provisional Restorations
Minu Raju
International Journal of Prosthodontics and Restorative Dentistry.2014; 4(1): 1. CrossRef
- Impact of Various Sleeve Materials on Temperature Variations During Guided Endodontic Access Cavity Preparation Utilizing Finite‐Element Analysis
- 7,638 View
- 52 Download
- 76 Crossref
Basic Research
- A new method to measure the linear polymerization shrinkage of composites using a particle tracking method with computer vision
- In-Bog Lee, Sun-Hong Min, Deog-Gyu Seo, Sun-Young Kim, Youngchul Kwon
- J Korean Acad Conserv Dent 2010;35(3):180-187. Published online May 31, 2010
- DOI: https://doi.org/10.5395/JKACD.2010.35.3.180
-
Abstract
PDFPubReaderePub
Since the introduction of restorative dental composites, their physical properties have been significantly improved. However, polymerization shrinkage is still a major drawback. Many efforts have been made to develop a low shrinking composite, and silorane-based composites have recently been introduced into the market. In addition, many different methods have been developed to measure the polymerization shrinkage.
In this study, we developed a new method to measure the linear polymerization shrinkage of composites without direct contact to a specimen using a particle tracking method with computer vision. The shrinkage kinetics of a commercial silorane-based composite (P90) and two conventional methacrylate-based composites (Z250 and Z350) were investigated and compared. The results were as follows:
The linear shrinkage of composites was 0.33-1.41%. Shrinkage was lowest for the silorane-based (P90) composite, and highest for the flowable Z350 composite.
The new instrument was able to measure the true linear shrinkage of composites in real time without sensitivity to the specimen preparation and geometry.
-
Citations
Citations to this article as recorded by- Effect of layering methods, composite type, and flowable liner on the polymerization shrinkage stress of light cured composites
Youngchul Kwon, Jack Ferracane, In-Bog Lee
Dental Materials.2012; 28(7): 801. CrossRef
- Effect of layering methods, composite type, and flowable liner on the polymerization shrinkage stress of light cured composites
- 1,998 View
- 5 Download
- 1 Crossref
Original Article
- Influence of three different preparation designs on the marginal and internal gaps of CEREC3 CAD/CAM inlays
- Deog-Gyu Seo, Young-Ah Yi, Yoon Lee, Byoung-Duck Roh
- J Korean Acad Conserv Dent 2009;34(3):177-183. Published online May 31, 2009
- DOI: https://doi.org/10.5395/JKACD.2009.34.3.177
-
Abstract
PDFPubReaderePub
The aim of this study was to evaluate the marginal and internal gaps in CEREC3 CAD/CAM inlays of three different preparation designs. CEREC3 Inlays of three different preparation designs (n = 10) were fabricated according to Group I-conventional functional cusp capping/shoulder preparation, Group II-horizontal reduction of cusps and Group III-complete reduction of cusps/shoulder preparation. After cementation of inlays, the bucco-lingual cross section was performed through the center of tooth. Cross section images of 20 magnifications were obtained through the stereomicroscope. The gaps were measured using the Leica application suite software at each reference point. Statistical analysis was performed using one-way ANOVA and Tukey's test (α<0.05).
The marginal gaps ranged from 80.0 to 97.8 µm for Group I, 42.0 to 194.8 µm for Group II, 51.0 to 80.2 µm for Group III. The internal gaps ranged from 90.5 to 304.1 µm for Group I, 80.0 to 274.8 µm for Group II, 79.7 to 296.7 µm for Group III. The gaps of each group were the smallest on the margin and the largest on the horizontal wall. For the CEREC3 CAD/CAM inlays, the simplified designs (groups II and III) did not demonstrate superior results compared to the traditional cusp capping design (group I).
-
Citations
Citations to this article as recorded by- Effect of axiopulpal line angle design and cement space settings on seating accuracy of CAD/CAM ceramic inlays: an in vitro study
Donghwan Kim, Mi-Jeong Jeon, Young Suk Kang, Yu-Sung Choi, Jeong-Kil Park, Deog-Gyu Seo
Journal of Dentistry.2026; 170: 106677. CrossRef - Influence of preparation design on fit and ceramic thickness of CEREC 3 partial ceramic crowns after cementation
Jae-Hoon Kim, Byeong-Hoon Cho, Jin-Hee Lee, Soo-Jung Kwon, Young-Ah Yi, Yooseok Shin, Byoung-Duck Roh, Deog-Gyu Seo
Acta Odontologica Scandinavica.2015; 73(2): 107. CrossRef
- Effect of axiopulpal line angle design and cement space settings on seating accuracy of CAD/CAM ceramic inlays: an in vitro study
- 2,049 View
- 5 Download
- 2 Crossref
Review Article
- The role of Type 2 Diabetes as a predisposing risk factor on the pulpo-periapical pathogenesis: review article
- Jin-Hee Kim, Kwang-shik Bae, Deog-Gyu Seo, Sung-Tae Hong, Yoon Lee, Sam-Pyo Hong, Kee-Yeon Kum
- J Korean Acad Conserv Dent 2009;34(3):169-176. Published online May 31, 2009
- DOI: https://doi.org/10.5395/JKACD.2009.34.3.169
-
Abstract
PDFPubReaderePub
Diabetes Mellitus (DM) is a syndrome accompanied with the abnormal secretion or function of insulin, a hormone that plays a vital role in controlling the blood glucose level (BGL). Type 1and 2 DM are most common form and the prevalence of the latter is recently increasing. The aim of this article was to assess whether Type 2 DM could act as a predisposing risk factor on the pulpo-periapical pathogenesis. Previous literature on the pathologic changes of blood vessels in DM was thoroughly reviewed. Furthermore, a histopathologic analysis of artificially-induced periapical specimens obtained from Type 2 diabetic and DM-resistant rats was compared. Histopathologic results demonstrate that the size of periapical bone destruction was larger and the degree of pulpal inflammation was more severe in diabetic rats, indicating that Type 2 DM itself can be a predisposing risk factor that makes the host more susceptible to pulpal infection. The possible reasons may be that in diabetic state the lumen of pulpal blood vessels are thickened by atheromatous deposits, and microcirculation is hindered. The function of polymorphonuclear leukocyte is also impaired and the migration of immune cells is blocked, leading to increased chance of pulpal infection. Also, lack of collateral circulation of pulpal blood vessels makes the pulp more susceptible to infection. These decrease the regeneration capacity of pulpal cells or tissues, delaying the healing process. Therefore, when restorative treatment is needed in Type 2 DM patients, dentists should minimize irritation to the pulpal tissue un der control of BGL.
-
Citations
Citations to this article as recorded by- Pulp necrosis following luxated injury to teeth in a patient with uncontrolled type II diabetes mellitus: a case report
Haneol Shin, Seung-Jong Lee, Il-Young Jung, Chan-Young Lee
Restorative Dentistry & Endodontics.2012; 37(1): 61. CrossRef
- Pulp necrosis following luxated injury to teeth in a patient with uncontrolled type II diabetes mellitus: a case report
- 1,893 View
- 12 Download
- 1 Crossref
Original Articles
- Effect of instrument compliance on the polymerization shrinkage stress measurements of dental resin composites
- Deog-Gyu Seo, Sun-Hong Min, In-Bog Lee
- J Korean Acad Conserv Dent 2009;34(2):145-153. Published online March 31, 2009
- DOI: https://doi.org/10.5395/JKACD.2009.34.2.145
-
Abstract
PDFPubReaderePub
The purpose of this study was to evaluate the effect of instrument compliance on the polymerization shrinkage stress measurements of dental composites. The contraction strain and stress of composites during light curing were measured by a custom made stress-strain analyzer, which consisted of a displacement sensor, a cantilever load cell and a negative feedback mechanism. The instrument can measure the polymerization stress by two modes: with compliance mode in which the instrument compliance is allowed, or without compliance mode in which the instrument compliance is not allowed.
A flowable (Filtek Flow: FF) and two universal hybrid (Z100: Z1 and Z250: Z2) composites were studied. A silane treated metal rod with a diameter of 3.0 mm was fixed at free end of the load cell, and other metal rod was fixed on the base plate. Composite of 1.0 mm thickness was placed between the two rods and light cured. The axial shrinkage strain and stress of the composite were recorded for 10 minutes during polymerization, and the tensile modulus of the materials was also determined with the instrument. The statistical analysis was conducted by ANOVA, paired t-test and Tukey's test (α<0.05).
There were significant differences between the two measurement modes and among materials. With compliance mode, the contraction stress of FF was the highest: 3.11 (0.13), followed by Z1: 2.91 (0.10) and Z2: 1.94 (0.09) MPa. When the instrument compliance is not allowed, the contraction stress of Z1 was the highest: 17.08 (0.89), followed by FF: 10.11 (0.29) and Z2: 9.46 (1.63) MPa. The tensile modulus for Z1, Z2 and FF was 2.31 (0.18), 2.05 (0.20), 1.41 (0.11) GPa, respectively. With compliance mode, the measured stress correlated with the axial shrinkage strain of composite; while without compliance the elastic modulus of materials played a significant role in the stress measurement.
-
Citations
Citations to this article as recorded by- Effects of cuspal compliance and radiant emittance of LED light on the cuspal deflection of replicated tooth cavity
Chang-Ha LEE, In-Bog LEE
Dental Materials Journal.2021; 40(3): 827. CrossRef - Polymerization Shrinkage and Stress of Silorane-based Dental Restorative Composite
In-Bog Lee, Sung-Hwan Park, Hyun-Jeong Kweon, Ja-Uk Gu, Nak-Sam Choi
Composites Research.2013; 26(3): 182. CrossRef - Evaluation of polymerization shrinkage stress in silorane-based composites
Seung-Ji Ryu, Ji-Hoon Cheon, Jeong-Bum Min
Journal of Korean Academy of Conservative Dentistry.2011; 36(3): 188. CrossRef - The change of the initial dynamic visco-elastic modulus of composite resins during light polymerization
Min-Ho Kim, In-Bog Lee
Journal of Korean Academy of Conservative Dentistry.2009; 34(5): 450. CrossRef
- Effects of cuspal compliance and radiant emittance of LED light on the cuspal deflection of replicated tooth cavity
- 2,065 View
- 2 Download
- 4 Crossref
- The comparison of relative reliability on biaxial and three point flexural strength testing methods of light curing composite resin
- Deog-Gyu Seo, Byoung-Duck Roh
- J Korean Acad Conserv Dent 2006;31(1):58-65. Published online January 31, 2006
- DOI: https://doi.org/10.5395/JKACD.2006.31.1.058
-
Abstract
PDFPubReaderePub
The possibility of applying a bi-axial flexure strength test on composite resin was examined using three point and bi-axial flexure strength tests to measure the strength of the light-cured resin and to compare the relative reliability using the Weibull modulus.
The materials used in this study were light-curing restorative materials, MICRONEW™, RENEW® (Bisco, Schaumburg, USA). The bi-axial flexure strength measurements used the piston-on-3-ball test according to the regulations of the International Organization for Standardization (ISO) 6872 and were divided into 6 groups, where the radius of the specimens were 12 mm (radius connecting the 3-balls: 3.75 mm), 16 mm (radius connecting the 3-balls: 5 mm), and the thickness were 0.5 mm, 1 mm, 2 mm for each radius.
The bi-axial flexure strength of the MICRONEW™ and RENEW® were higher than the three point flexure strength and the Weibull modulus value were also higher in all of the bi-axial flexure strength groups, indicating that the bi-axial strength test is relatively less affected by experimental error.
In addition, the 2 mm thick specimens had the highest Weibull modulus values in the bi-axial flexure strength test, and the MICRONEW™ group showed no significant statistical difference (p > 0.05). Besides the 2 mm MICRONEW™ group, each group showed significant statistical differences (p < 0.05) according to the thickness of the specimen and the radius connecting the 3-balls.
The results indicate that for the 2 mm group, the bi-axial flexure strength test is a more reliable testing method than the three point flexure strength test.
-
Citations
Citations to this article as recorded by- Remineralization of demineralized teeth enamel with nHAp and nHAp-NaF-PEO nanocomposite
Nazifa Zaman Khan, S. Manjura Hoque, Harinarayan Das, Arup Kumar, Rafiqul Islam, Mozammal Hossain
Biomedical Engineering Advances.2025; 10: 100192. CrossRef - Mechanical properties of CAD/CAM polylactic acid as a material for interim restoration
Won-Il Choi, Lee-gang Yoo, Yu-ri Kim, Bock-Young Jung
Heliyon.2023; 9(4): e15314. CrossRef - The comparisons of layers and the effect of additional firings on flexural strength and translucency of 5Y-ZP
Hyung-Joon Kim, Soo-Yeon Shin
Journal of Dental Rehabilitation and Applied Science.2021; 37(3): 111. CrossRef - Effect of coloring liquids on biaxial flexural strength of monolithic zirconia
Chaeyul Jung, Min-Jeong Kim, Jae-Hyun Kim
The Journal of Korean Academy of Prosthodontics.2021; 59(2): 190. CrossRef - Mechanical Properties and Reliability of Sand Casting 3D Printing Materials
Hyeon Jin Son, Seongwan Jang, Hwan Jong Lee, Jeong Jik Yang, Yeong Geun Jeong, Chang-Jun Bae
Korean Journal of Materials Research.2020; 30(1): 38. CrossRef - Comparison analysis of fracture load and flexural strength of provisional restorative resins fabricated by different methods
Won-Tak Cho, Jae-Won Choi
The Journal of Korean Academy of Prosthodontics.2019; 57(3): 225. CrossRef - Effect of Two Polishing Systems on Surface Roughness, Topography, and Flexural Strength of a Monolithic Lithium Disilicate Ceramic
Mahshid Mohammadibassir, Mohammad Bagher Rezvani, Hossein Golzari, Elham Moravej Salehi, Mohammad Amin Fahimi, Mohammad Javad Kharazi Fard
Journal of Prosthodontics.2019;[Epub] CrossRef - Characteristics according to the Amount of HAp Added in Resin for Tooth Repair
Sungu Hwang, Jinhyuck Lim, Suchak Ryu
Journal of the Korean Ceramic Society.2019; 56(6): 521. CrossRef - Flexural strength and microstructure of two lithium disilicate glass ceramics for CAD/CAM restoration in the dental clinic
Suk-Ho Kang, Juhea Chang, Ho-Hyun Son
Restorative Dentistry & Endodontics.2013; 38(3): 134. CrossRef
- Remineralization of demineralized teeth enamel with nHAp and nHAp-NaF-PEO nanocomposite
- 1,837 View
- 6 Download
- 9 Crossref
 First
First Prev
Prev

