
Search
- Page Path
- HOME > Search
Case Report
- Periodontal healing following non-surgical repair of an old perforation with pocket formation and oral communication
- Saeed Asgary, Prashant Verma, Ali Nosrat
- Restor Dent Endod 2018;43(2):e17. Published online April 13, 2018
- DOI: https://doi.org/10.5395/rde.2018.43.e17
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
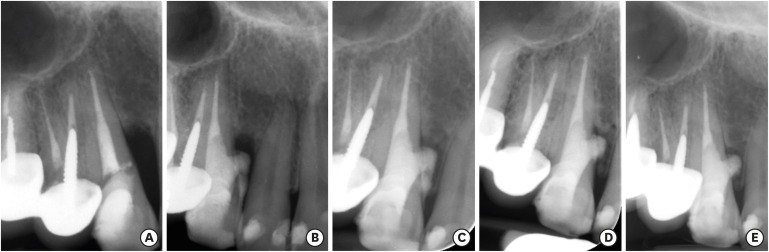
ePub Iatrogenic perforations negatively impact the outcome of endodontic treatments. Studies on prognostic factors showed that perforations in the coronal third of the root with periodontal pocket formation have an unfavorable prognosis. A 36-year-old female was referred for endodontic evaluation of tooth #13 with a history of an iatrogenic perforation, happened 3 years ago. There was a sinus tract associated with perforation, 10 mm probing on the mesial and mesio-palatal, bleeding on probing, radiolucent lesion adjacent to the perforation and complete resorption of the interdental bone between teeth #13 and #12. After the treatment options were discussed, she chose to save the tooth. The tooth was accessed under rubber dam isolation, the perforation site was cleaned and disinfected using 0.5% sodium hypochlorite and sealed with calcium-enriched mixture cement. Eighteen months after treatment the tooth was functional and asymptomatic. The probing depths were normal without bleeding on probing. Radiographically, the interdental crestal bone formed between teeth #13 and #12. Despite all negative prognostic factors in this case (
i.e. , perforations in the coronal third, pocket formation, and radiolucent lesion), healing was unexpectedly achieved via non-surgical repair of the perforation. Further research on biological aspects of healing in the periodontium following iatrogenic perforations are recommended.-
Citations
Citations to this article as recorded by
- Factors Influencing the Outcome of Iatrogenic Perforation Repair in Permanent Teeth—A Narrative Review
Saravanan Poorni, Srividhya Srinivasan, Thomas Clauder, Manali Ramakrishnan Srinivasan, Paul M. H. Dummer, Venkateshbabu Nagendrababu
Australian Endodontic Journal.2026;[Epub] CrossRef - Managing Internal Inflammatory Root Resorption and Perforation of a Mandibular Primary Molar: A Case Report With 15 Months Follow‐Up
Mana Mowji, Motahareh Khosrojerdi
Clinical Case Reports.2025;[Epub] CrossRef - Nonsurgical Management of Furcation Defects Using Cervical Sealing With Calcium–Silicate Cements: A Clinical Case Series
Saeed Asgary, Shamimul Hasan
Case Reports in Medicine.2025;[Epub] CrossRef - Nonsurgical Management of Simultaneous Double Lateral Root Perforations in Adjacent Teeth Using CBCT and MTA: A Case Report
Beyhan Başkan, Hatice Kübra Başkan, Beyza Güler, Ricardo Faria Ribeiro
Case Reports in Dentistry.2025;[Epub] CrossRef - Comprehensive review of composition, properties, clinical applications, and future perspectives of calcium-enriched mixture (CEM) cement: a systematic analysis
Saeed Asgary, Mahtab Aram, Mahta Fazlyab
BioMedical Engineering OnLine.2024;[Epub] CrossRef - External Cervical Resorption: A Volumetric Analysis on Evolution of Defects over Time
Ali Nosrat, Omid Dianat, Prashant Verma, Martin D. Levin, Jeffery B. Price, Anita Aminoshariae, Fabio Antonio Piola Rizzante
Journal of Endodontics.2023; 49(1): 36. CrossRef - Comparative evaluation of mineral trioxide aggregate, endoseal, and biodentine in furcation perforation repair
Udita Khare Baralay, Srinidhi Surya Raghavendra
Endodontology.2022; 34(1): 22. CrossRef - Calcium Silicate Cements Application in Lateral Root Perforation Repair: A Case Report with 16-Month Follow-Up
Juan G. Robledo, Pablo A. Rodríguez
Open Journal of Stomatology.2021; 11(08): 317. CrossRef - Vital Pulp Therapy as a Conservative Approach for Management of Invasive Cervical Root Resorption: A Case Series
Saeed Asgary, Mahdieh Nourzadeh, Prashant Verma, M. Lamar Hicks, Ali Nosrat
Journal of Endodontics.2019; 45(9): 1161. CrossRef
- Factors Influencing the Outcome of Iatrogenic Perforation Repair in Permanent Teeth—A Narrative Review
- 3,800 View
- 17 Download
- 9 Crossref

Review Article
- Current perspectives of bio-ceramic technology in endodontics: calcium enriched mixture cement - review of its composition, properties and applications
- Shivani Utneja, Ruchika Roongta Nawal, Sangeeta Talwar, Mahesh Verma
- Restor Dent Endod 2015;40(1):1-13. Published online November 3, 2014
- DOI: https://doi.org/10.5395/rde.2015.40.1.1
-
Abstract
PDFPubReaderePub
Advancements in bio-ceramic technology has revolutionised endodontic material science by enhancing the treatment outcome for patients. This class of dental materials conciliates excellent biocompatibility with high osseoconductivity that render them ideal for endodontic care. Few recently introduced bio-ceramic materials have shown considerable clinical success over their early generations in terms of good handling characteristics. Calcium enriched mixture (CEM) cement, Endosequence sealer, and root repair materials, Biodentine and BioAggregate are the new classes of bio-ceramic materials. The aim of this literature review is to present investigations regarding properties and applications of CEM cement in endodontics. A review of the existing literature was performed by using electronic and hand searching methods for CEM cement from January 2006 to December 2013. CEM cement has a different chemical composition from that of mineral trioxide aggregate (MTA) but has similar clinical applications. It combines the biocompatibility of MTA with more efficient characteristics, such as significantly shorter setting time, good handling characteristics, no staining of tooth and effective seal against bacterial leakage.
-
Citations
Citations to this article as recorded by- CBCT‐Assisted Microsurgical Management of Dual Periapical Lesions Involving Vital and Previously Endodontically Treated Maxillary Molars: A Case Report
Saeed Asgary
Clinical Case Reports.2026;[Epub] CrossRef - Comparative evaluation of calcium-enriched mixture and mineral trioxide aggregate in vital pulp therapy of molars: A systematic review
Aarti Ravishankar Lamb, Sheetal Ghivari, Rishikesh Meshram, Ambar Raut, Maithilee Sapkal, Saniya Rege
Journal of Conservative Dentistry and Endodontics.2026; 29(2): 127. CrossRef - Management of Furcal Perforation/Involvement in a Primary Molar With Irreversible Pulpitis Using Tampon Pulpotomy: A 18‐Month Healing Case Report
Saeed Asgary, Fatemeh Shekarchi
Clinical Case Reports.2026;[Epub] CrossRef - Modifications of Biodentine and Their Influence on Endodontic Properties: A Scoping Review
Rumesa Batul, Abdul Habeeb Adil, Niher Tabassum Snigdha, Ankita Mathur, Sushma Bommanavar, Mohmed Isaqali Karobari, Hannah Wesley
International Journal of Dentistry.2026;[Epub] CrossRef - Antibacterial Efficacy of Graphene Nanoparticles against Enterococcus faecalis: In Vitro Study
Omer Sheriff Sultan, Preena Sidhu, Kiran Rehman, Thiagrajan Madheswaran, Amalraj Fabian Davamani
European Journal of Dentistry.2025; 19(01): 103. CrossRef - Biomineralization reaction from nanosized calcium silicate: A new method for reducing dentin hypersensitivity
Mi-Jeong Jeon, Yu-Sung Choi, Jeong-Kil Park, Jin-Soo Ahn, Yu-Chih Chiang, Deog-Gyu Seo
Journal of Dental Sciences.2025; 20(1): 428. CrossRef - How to Deal with Pulpitis: An Overview of New Approaches
Jakub Fiegler-Rudol, Wojciech Niemczyk, Katarzyna Janik, Anna Zawilska, Małgorzata Kępa, Marta Tanasiewicz
Dentistry Journal.2025; 13(1): 25. CrossRef - Effect of Manipulation Methods and Storage Environments on the Microstructural, Chemical, and Mechanical Properties of Calcium‐Enriched Mixture Cement
Leyla Roghanizadeh, Hassan Torabzadeh, Ardavan Parhizkar, Alireza Akbarzadeh Baghban, Saeed Asgary, Luca Fiorillo
International Journal of Biomaterials.2025;[Epub] CrossRef - Advances in 3D Bioprinting of Scaffolds for Dental Tissue Engineering and Regeneration
Senyao Chen, Jianwei Sun, Wenzhi Wu, Zhuo Chen
Advanced Functional Materials.2025;[Epub] CrossRef - Effect of Vital Pulp Therapy Biomaterials on Tooth Discolouration: A Review of the Literature
Maedeh Gilvari Sarshari, Kiana Shakeri, Ardavan Parhizkar, Naresh Kasoju
International Journal of Biomaterials.2025;[Epub] CrossRef - Vital Pulpa Tedavilerinde Biyoseramik Materyallerin Kullanımı: Sistematik Derleme
Duygu Bal, Gül Keskin
Türk Diş Hekimliği Araştırma Dergisi.2025; 4(2): 103. CrossRef - Bioactive Materials in Pediatric Endodontics: Current Applications and Future Directions
Abdulrahman S Alshalan, Fai A Almutiri, Ali H Al-battat, Abdulrahman M Alqahtani, Khalid A Binzamil, Reem M Alabdan, Khalidah K Alrabghi, Asma M Aldohailan, Eman A Alshammari, Abdulrahman S Khurayniq, Mazen T Alshahrani
Cureus.2025;[Epub] CrossRef - Comparative clinical success of direct pulp capping materials: A network meta-regression of randomized clinical trials
Ömer Hatipoğlu, Elif Varlı Tekingür, Fatma Pertek Hatipoğlu
Journal of Dentistry.2025; 162: 106073. CrossRef - Pharmacopée intracanalaire
J. Davril, R. Balthazard, R. Giess, M. Vincent, E. Mortier
EMC - Odontologie.2025; 41(4): 1. CrossRef - Comparative evaluation of four different calcium-based medicaments as an indirect pulp capping agent: An in vivo study
Ray Anuja Awadhesh, Nitin Kararia, Deepak Kumar Sharma, Shyam Agrawal, Rachit Mathur, Jyotirmoyee Bhanja
Journal of Conservative Dentistry and Endodontics.2025; 28(10): 1013. CrossRef - Calcium Phosphate Incorporated Polymeric Fibrous Scaffolds for Bone Tissue Engineering: A Comprehensive Review
Parvathy GH, Nidhish Kumar P, Swapna YV, Mathew CT, Jijimon K Thomas
Journal of Macromolecular Science, Part B.2025; : 1. CrossRef - Investigation of the crystal formation from calcium silicate in human dentinal tubules and the effect of phosphate buffer saline concentration
Mi-Jeong Jeon, Jin-Soo Ahn, Jeong-Kil Park, Deog-Gyu Seo
Journal of Dental Sciences.2024; 19(4): 2278. CrossRef - Comprehensive review of composition, properties, clinical applications, and future perspectives of calcium-enriched mixture (CEM) cement: a systematic analysis
Saeed Asgary, Mahtab Aram, Mahta Fazlyab
BioMedical Engineering OnLine.2024;[Epub] CrossRef - Dentinal tubule penetration following ultrasonic, sonic, and single-cone technique of a biosealer: An ex vivo study
Dina Abdellatif, Massimo Pisano, Renato Gullà, Giuseppe Sangiovanni, Shishir Singh, Francesco Giordano, Alessio Buonavoglia, Alfredo Iandolo
Journal of Conservative Dentistry and Endodontics.2024; 27(3): 331. CrossRef - Physicochemical properties of silicate tricalcium-based cement for use as pulp capping or repair material
Suyane Maria LUNA-CRUZ, Bernardo Almeida AGUIAR, Pierre Basílio Almeida FECHINE, Marco Antônio Húngaro DUARTE, Bruno Carvalho de VASCONCELOS, Juliano Sartori MENDONÇA
Brazilian Oral Research.2024;[Epub] CrossRef - Successful Tampon Pulpotomy in a Molar With an Endodontic Lesion: A Case Report
Saeed Asgary
Cureus.2024;[Epub] CrossRef - Comparative evaluations of shear bond strength of mineral trioxide aggregate, Biodentine, and calcium-enriched mixture to bulk-fill flowable composite using three different adhesive systems: An in vitro study
Asmat Fatima, Huma İftekhar, Sharique Alam, Rajendra Kumar Tewari, Mukhtar Un Nisar Andrabi
Journal of Conservative Dentistry and Endodontics.2024; 27(7): 706. CrossRef - Comparative in vitro analysis of the antifungal activity of different calcium silicate-based endodontic sealers
Luiz Felipe Nunes Moreira, Fernando Peña-Bengoa, Sven Eric Niklander, Carlos Eduardo da Silveira Bueno, Alexandre Sigrist de Martin, Daniel Guimarães Pedro Rocha
Brazilian Journal of Oral Sciences.2024; 23: e243355. CrossRef - Enhancing pH Modulation and Calcium Ions Release in External Resorption Artificial Defects
Azadeh Kheradyar, Mamak Adel, Majid Sirati-Sabet, Alireza Kolahdouzan, Sahar Shafagh, Lucas da Fonseca Roberti Garcia
International Journal of Dentistry.2024;[Epub] CrossRef - Efficacy of pulpotomy for permanent teeth with carious pulp exposure: A systematic review and meta-analysis of randomized controlled trials
Wenjun Li, Bo Yang, Jing Shi, Carlos Alberto Antunes Viegas
PLOS ONE.2024; 19(7): e0305218. CrossRef - Comparative evaluation of cervical pulpotomy and pulpectomy for primary molars with irreversible pulpitis: a multicentre randomised controlled trial
S. Sabbagh, Z. Bahrololoomi, A. Sarraf Shirazi, F. Zarebidoki, S. Salajegheh, F. Fotouhi, A. Akbarzadeh Baghban, S. Asgary
European Archives of Paediatric Dentistry.2024; 25(2): 255. CrossRef - Bioceramic Materials: A Boon in Pediatric Dentistry: A Literature Review
Sheenam Ayub, Sonal Gupta, Menia Gumro
Journal of Primary Care Dentistry and Oral Health.2024; 5(1): 3. CrossRef - Peptide KN-17-Loaded Supramolecular Hydrogel Induces the Regeneration of the Pulp-Dentin Complex
Borui Zhao, Qian Zhang, Houzhi Yang, Shuipeng Yu, Rui Fu, Shurui Shi, Yuanyuan Wang, Wei Zhou, Yange Cui, Qingxiang Guo, Xi Zhang
ACS Biomaterials Science & Engineering.2024; 10(4): 2523. CrossRef - Cimentos biocerâmicos na endodontia: atualizações sobre as propriedades regenerativas e antibacterianas
Víctor Lucas Ribeiro Lopes, Even Herlany Pereira Alves, Hélio Mateus Silva Nascimento, Maria de Fátima Leal de Sousa, Daniel Fernando Pereira Vasconcelos, Francisca Meire Soares de Freitas Portela
Cuadernos de Educación y Desarrollo.2024; 16(8): e5259. CrossRef - ZrO2 and ZnO nanoparticles effect on setting time, microhardness, and compressive strength of calcium-enriched-mixture cement
Faezeh Sadat Razavi, Fatemeh Mahmoudi Afsah, Alireza Akbarzadeh Baghban, Hasan Torabzadeh, Saeed Asgary
Brazilian Journal of Oral Sciences.2024; 23: e244482. CrossRef - Radiographic Evaluation of Periapical Healing Rates Between Bio-Ceramic Sealer and AH+ Sealer: A Retrospective Study
Dalia Nayil Alharith, Iman T. Mansi, YoumnaElsaid Abdulmotalib, HebaFuad Amous, TagreedSuliman Aljulban, Haifa Mohammed Al Aiban, Sali Mohamad Haffar
Annals of Dental Specialty.2023; 11(2): 124. CrossRef - Bioceramics in endodontics – A review
Chris Cherian Geogi, Ananya Rawat, Sandeep Dubey, Palak Singh
IP Indian Journal of Conservative and Endodontics.2023; 7(4): 163. CrossRef - Exploring the Most Effective Apical Seal for Contemporary Bioceramic and Conventional Endodontic Sealers Using Three Obturation Techniques
Hira Akhtar, Farah Naz, Arshad Hasan, Anum Tanwir, Danish Shahnawaz, Umair Wahid, Fariha Irfan, Muhammad Adeel Ahmed, Khalid H. Almadi, Mazen F. Alkahtany, Tariq Abduljabbar, Fahim Vohra
Medicina.2023; 59(3): 567. CrossRef - Tissue Response to a Heat Resistant Silicate-Based and an Epoxy Resin-Based Endodontic Sealer Implanted in Rat Tibias
Osvaldo Zmener, Cornelis H. Pameijer, Roberto Della Porta, Romina de Lucca
Applied Sciences.2023; 13(18): 10075. CrossRef - Autotransplantation of a Third Molar to Replace an Adjacent Unrestorable Tooth: A Case Report
Saeed Asgary
Cureus.2023;[Epub] CrossRef - Fracture Resistance of Molars With Simulated Strip Perforation Repaired With Different Calcium Silicate-Based Cements
Alaa Kabtoleh, Ossama Aljabban, Yasser Alsayed Tolibah
Cureus.2023;[Epub] CrossRef - Outcomes of Endodontic-Treated Teeth Obturated with Bioceramic Sealers in Combination with Warm Gutta-Percha Obturation Techniques: A Prospective Clinical Study
Denise Irene Karin Pontoriero, Edoardo Ferrari Cagidiaco, Valerio Maccagnola, Daniele Manfredini, Marco Ferrari
Journal of Clinical Medicine.2023; 12(8): 2867. CrossRef - An in vitro comparative evaluation of the effect of three intracanal medicaments – chlorhexidine gel, triple antibiotic paste, and calcium hydroxide paste on the push-out bond strength of MTA Plus, Biodentine, and calcium-enriched mixture
Gouthami Datta, Ramya Raghu, Ashish Shetty, Gautham P Manjunath, Dishant Patel, Subhashini Rajasekhara
Endodontology.2023; 35(1): 60. CrossRef - Effects of CEM cement and emdogain on proliferation and differentiation of human stem cells from the apical papilla: a comparative in vitro study
Elham Khoshbin, Leila Ghasemi, Rezvan Najafi, Hamed Karkehabadi
Biotechnology Letters.2023; 45(1): 69. CrossRef - Ceramic nanomaterials: Preparation and applications in osteoporosis and bone tissue regeneration
Anish John, Apurva M. Shetty, Kshema Salian, Samantha Neha Sequeria, P. R. Sumukh, Dewi Sukmawati, Gowtham Menon, Shajan Abraham, Jayachandran Venkatesan, V. Anoop Narayanan
Journal of Materials Research.2023; 38(17): 4023. CrossRef - Recent Advances in Endodontic Diagnosis and Modern Treatment Plans
Alfredo Iandolo
Diagnostics.2023; 13(17): 2786. CrossRef - Outcome of pulpotomy in permanent teeth with irreversible pulpitis: a systematic review and meta-analysis
Amber Ather, Biraj Patel, Jonathan A. L. Gelfond, Nikita B. Ruparel
Scientific Reports.2022;[Epub] CrossRef - Comparison of Coronal Discoloration Induced by White MTA and CEM Cement
Mamak Adel, Sareh Aflaki, Mohammad Jafar Eghbal, Alireza Darvish, Amanda Mandana Golshiri, Nima Moradi Majd, Rodolfo Reda, Maryam Tofangchiha, Alessio Zanza, Luca Testarelli
Journal of Composites Science.2022; 6(12): 371. CrossRef - Current trends and future perspectives on dental nanomaterials – An overview of nanotechnology strategies in dentistry
Vidhya Rekha Umapathy, Prabhu Manickam Natarajan, C. SumathiJones, Bhuminathan Swamikannu, W.M.S. Johnson, V. Alagarsamy, Ashequr Rahman Milon
Journal of King Saud University - Science.2022; 34(7): 102231. CrossRef - Evaluation of the Sealing Ability and Bond Strength of Two Endodontic Root Canal Sealers: An In Vitro Study
Manuel Marques Ferreira, José Pedro Martinho, Inês Duarte, Diogo Mendonça, Ana Catarina Craveiro, Maria Filomena Botelho, Eunice Carrilho, Carlos Miguel Marto, Ana Coelho, Anabela Paula, Siri Paulo, Nuno Chichorro, Ana Margarida Abrantes
Dentistry Journal.2022; 10(11): 201. CrossRef - Outcomes of root canal therapy or full pulpotomy using two endodontic biomaterials in mature permanent teeth: a randomized controlled trial
Saeed Asgary, Mohammad Jafar Eghbal, Arash Shahravan, Eshaghali Saberi, Alireza Akbarzadeh Baghban, Ardavan Parhizkar
Clinical Oral Investigations.2022; 26(3): 3287. CrossRef - Trends of calcium silicate biomaterials in medical research and applications: A bibliometric analysis from 1990 to 2020
Hua Yin, Xiaoli Yang, Lisi Peng, Chuanchao Xia, Deyu Zhang, Fang Cui, Haojie Huang, Zhaoshen Li
Frontiers in Pharmacology.2022;[Epub] CrossRef - Different types of bioceramics as dental pulp capping materials: A systematic review
Sotoudeh Davaie, Tabassom Hooshmand, Sajjad Ansarifard
Ceramics International.2021; 47(15): 20781. CrossRef - Effect of MTA versus CEM apical plugs on fracture resistance of endodontically treated simulated immature teeth restored with cast metal posts: an in-vitro study
Ensieh Grayli, Abbas Dashtban, Leyla Shadan, Naser Behnampour, Elham Afshari
BMC Oral Health.2021;[Epub] CrossRef - Effectiveness of Direct Pulp Capping Bioactive Materials in Dentin Regeneration: A Systematic Review
Ermin Nie, Jiali Yu, Rui Jiang, Xiangzhen Liu, Xiang Li, Rafiqul Islam, Mohammad Khursheed Alam
Materials.2021; 14(22): 6811. CrossRef - Pediatric Endodontic Treatment of Adolescent Patients
Adriana Modesto Vieira, Herbert L. Ray
Dental Clinics of North America.2021; 65(4): 775. CrossRef - Management of primary molars with irreversible pulpitis employing tampon pulpotomy: Report of three cases with 34‐month mean follow‐up
Saeed Asgary, Alireza Sarraf Shirazi, Sedigheh Sabbagh
Clinical Case Reports.2021; 9(4): 2289. CrossRef - Effects of various liquid-to-powder ratios on the compressive strength of calcium enriched mixture: Original research
Mohammad Forough Reyhani, Sheida Hosseinian Ahangarnezhad, Negin Ghasemi, Amin Salem Milani
Journal of Dental Research, Dental Clinics, Dental Prospects.2021; 15(2): 129. CrossRef - Evaluation of the Use of Bioceramics in Endodontic Management, Literature Review
Wejdan Ali Alkaabinah, Bashayr Faisal Alanazi, Amlak Munahi Albaqami, Bashayer Mohammed Almutiry, Maram Saleh A Alkhamis, Ali Abdullah Alhejailan, Ibrahim Owaidh M Almutairi, Bassel Hamad Aldahman, Alhanoof Falah Alanazi
Pharmacophore.2021; 12(3): 87. CrossRef - Bioactive Glass Modified Calcium Phosphate Cement with Improved Bioactive Properties: A Potential Material for Dental Pulp-Capping Approaches
Sotoudeh Davaie, Sima Shahabi, Marjan Behroozibakhsh, Sanaz Vali, Farhood Najafi
Journal of Biomimetics, Biomaterials and Biomedical Engineering.2021; 51: 1. CrossRef - Intratubular penetration of endodontic sealers depends on the fluorophore used for CLSM assessment
Taiane Correa Furtado, Igor Abreu de Bem, Lucas Silveira Machado, Jefferson Ricardo Pereira, Marcus Vinícius Reis Só, Ricardo Abreu da Rosa
Microscopy Research and Technique.2021; 84(2): 305. CrossRef - From the Desk of the Editor: The New-Age Bioceramic Root Canal Sealers
Shishir Singh
Journal of Conservative Dentistry.2021; 24(5): 413. CrossRef - Influence of Blood Contamination on Push-Out Bond Strength of Three Calcium Silicate-Based Materials to Root Dentin
Cristina Rodrigues Paulo, Joana A. Marques, Diana B. Sequeira, Patrícia Diogo, Rui Paiva, Paulo J. Palma, João Miguel Santos
Applied Sciences.2021; 11(15): 6849. CrossRef - Comparison of the Success Rate of Mineral Trioxide Aggregate, Endosequence Bioceramic Root Repair Material, and Calcium Hydroxide for Apexification of Immature Permanent Teeth: Systematic Review and Meta-Analysis
Izaz Shaik, Bhargavi Dasari, Rashmi Kolichala, Mina Doos, Fida Qadri, Jenefer Loveline Arokiyasamy, Rahul Vinay Chandra Tiwari
Journal of Pharmacy and Bioallied Sciences.2021; 13(Suppl 1): S43. CrossRef - Local Drug Delivery Systems for Vital Pulp Therapy: A New Hope
Ardavan Parhizkar, Saeed Asgary, Carlo Galli
International Journal of Biomaterials.2021; 2021: 1. CrossRef - Toughening of Bioceramic Composites for Bone Regeneration
Zahid Abbas, Massimiliano Dapporto, Anna Tampieri, Simone Sprio
Journal of Composites Science.2021; 5(10): 259. CrossRef - Performance of Bioceramic-based Root Filling Material with Artifact Reduction Properties in the Detection of Vertical Root Fractures Using Cone-beam Computed Tomography
Ali Bahmani, Hamed Karkehabadi, Abbas Shokri, Maryam Farhadian
The Open Dentistry Journal.2021; 15(1): 170. CrossRef - The effect of partial pulpotomy with iRoot BP Plus in traumatized immature permanent teeth: A randomized prospective controlled trial
YingTing Yang, Bin Xia, Zheng Xu, Guili Dou, Yue Lei, Wei Yong
Dental Traumatology.2020; 36(5): 518. CrossRef - Effect of ultrasonic cleaning on the bond strength of fiber posts in oval canals filled with a premixed bioceramic root canal sealer
Fernando Peña Bengoa, Maria Consuelo Magasich Arze, Cristobal Macchiavello Noguera, Luiz Felipe Nunes Moreira, Augusto Shoji Kato, Carlos Eduardo Da Silveira Bueno
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - Silico-Aluminophosphate and Alkali-Aluminosilicate Geopolymers: A Comparative Review
Yan-Shuai Wang, Yazan Alrefaei, Jian-Guo Dai
Frontiers in Materials.2019;[Epub] CrossRef - Combination of mineral trioxide aggregate and propolis promotes odontoblastic differentiation of human dental pulp stem cells through ERK signaling pathway
Jae-Hwan Kim, Soo-Yung Kim, Su-Mi Woo, Ha-Na Jeong, Ji-Yeon Jung, Seon-Mi Kim, Hae-Soon Lim
Food Science and Biotechnology.2019; 28(6): 1801. CrossRef - Effectiveness of a Novel Calcium-enriched Mixture Root Cement to Decelerate Replacement Resorption in Replanted Teeth: A Case Report
Nasil Sakkir, Tony Francis, Sonal B Joshi
World Journal of Dentistry.2019; 10(6): 457. CrossRef - Which procedures and materials could be applied for full pulpotomy in permanent mature teeth? A systematic review
M. Zanini, M. Hennequin, PY. Cousson
Acta Odontologica Scandinavica.2019; 77(7): 541. CrossRef - Microstructure and chemical analysis of four calcium silicate-based cements in different environmental conditions
K. Ashofteh Yazdi, Sh. Ghabraei, B. Bolhari, M. Kafili, N. Meraji, M. H. Nekoofar, P. M. H. Dummer
Clinical Oral Investigations.2019; 23(1): 43. CrossRef - Treatment Outcomes of 4 Vital Pulp Therapies in Mature Molars
Saeed Asgary, Raheleh Hassanizadeh, Hassan Torabzadeh, Mohammad Jafar Eghbal
Journal of Endodontics.2018; 44(4): 529. CrossRef - Sectional Fixed Orthodontic Extrusion Technique in Management of Teeth with Complicated Crown-Root Fractures: Report of Two Cases
S. Nagarajan M. P. Sockalingam, Katherine Kong Loh Seu, Halimah Mohamed Noor, Ahmad Shuhud Irfani Zakaria
Case Reports in Dentistry.2018; 2018: 1. CrossRef - Evaluation of Physicochemical Properties of New Calcium Silicate-Based Sealer
Aline Teixeira Mendes, Paula Barcellos da Silva, Bruna Barcelos Só, Lina Naomi Hashizume, Rodrigo Ricci Vivan, Ricardo Abreu da Rosa, Marco Antonio Húngaro Duarte, Marcus Vinícius Reis Só
Brazilian Dental Journal.2018; 29(6): 536. CrossRef - Periodontal healing following non-surgical repair of an old perforation with pocket formation and oral communication
Saeed Asgary, Prashant Verma, Ali Nosrat
Restorative Dentistry & Endodontics.2018;[Epub] CrossRef - Nonsurgical Management and 2-year Follow-up by means of Cone Beam Computed Tomography of an Invasive Cervical Resorption in a Molar
Esam Halboub, Hemant R Chourasia, Rafael A Roges
The Journal of Contemporary Dental Practice.2018; 19(9): 1152. CrossRef - Management of merged external/internal root resorption using CEM cement: a case report.
Hesam Mirmohammadi, Saeed Asgary
Journal of Oral Research.2018; 7(8): 318. CrossRef - Maturogenesis of an Immature Dens Evaginatus Nonvital Premolar with an Apically Placed Bioceramic Material (EndoSequence Root Repair Material®): An Unexpected Finding
S. Nagarajan M. P. Sockalingam, Mohd Safwani Affan Alli Awang Talip, Ahmad Shuhud Irfani Zakaria
Case Reports in Dentistry.2018; 2018: 1. CrossRef - The implications and applications of nanotechnology in dentistry: A review
Rawan N. AlKahtani
The Saudi Dental Journal.2018; 30(2): 107. CrossRef - Calcium silicate‐based cements: composition, properties, and clinical applications
Alaa E. Dawood, Peter Parashos, Rebecca H.K. Wong, Eric C. Reynolds, David J. Manton
Journal of Investigative and Clinical Dentistry.2017;[Epub] CrossRef - Biocompatibility of three new calcium silicate‐based endodontic sealers on human periodontal ligament stem cells
M. Collado‐González, D. García‐Bernal, R. E. Oñate‐Sánchez, P. S. Ortolani‐Seltenerich, A. Lozano, L. Forner, C. Llena, F. J. Rodríguez‐Lozano
International Endodontic Journal.2017; 50(9): 875. CrossRef - Cytotoxicity and bioactivity of various pulpotomy materials on stem cells from human exfoliated primary teeth
M. Collado‐González, D. García‐Bernal, R. E. Oñate‐Sánchez, P. S. Ortolani‐Seltenerich, T. Álvarez‐Muro, A. Lozano, L. Forner, C. Llena, J. M. Moraleda, F. J. Rodríguez‐Lozano
International Endodontic Journal.2017;[Epub] CrossRef - The Effect of Three Different Biomaterials on Proliferation and Viability of Human Dental Pulp Stem Cells (In-vitro Study)
Dalia A. Mohamed, Maha I. Abdelfattah, Eman H. A. Aboulezz
Open Access Macedonian Journal of Medical Sciences.2017; 5(5): 657. CrossRef - Bioactive-glass in Endodontic Therapy and Associated Microsurgery
Andrea Corrado Profeta, Gian Marco Prucher
The Open Dentistry Journal.2017; 11(1): 164. CrossRef - Comparison of mineral trioxide aggregate and calcium hydroxide for apexification of immature permanent teeth: A systematic review and meta-analysis
Jia-Cheng Lin, Jia-Xuan Lu, Qian Zeng, Wei Zhao, Wen-Qing Li, Jun-Qi Ling
Journal of the Formosan Medical Association.2016; 115(7): 523. CrossRef - Cytotoxic effects of mineral trioxide aggregate, calcium enrichedmixture cement, Biodentine and octacalcium pohosphate onhuman gingival fibroblasts
Eshagh A. Saberi, Narges Farhadmollashahi, Faroogh Ghotbi, Hamed Karkeabadi, Roholla Havaei
Journal of Dental Research, Dental Clinics, Dental Prospects.2016; 10(2): 75. CrossRef - Influence of Biodentine® - A Dentine Substitute - On Collagen Type I Synthesis in Pulp Fibroblasts In Vitro
Frangis Nikfarjam, Kim Beyer, Anke König, Matthias Hofmann, Manuel Butting, Eva Valesky, Stefan Kippenberger, Roland Kaufmann, Detlef Heidemann, August Bernd, Nadja Nicole Zöller, Dimitrios Karamichos
PLOS ONE.2016; 11(12): e0167633. CrossRef - Challenges in developing valid techniques for equine endodontic treatment of apically infected cheek teeth
R. M. Baratt
Equine Veterinary Education.2016; 28(11): 609. CrossRef - Regenerative Endodontic Procedure in Korean Children and Adolescents: A Case Report
So-Youn An, Jin-Kyoung Kim, Youn-Soo Shim
Journal of dental hygiene science.2016; 16(4): 317. CrossRef
- CBCT‐Assisted Microsurgical Management of Dual Periapical Lesions Involving Vital and Previously Endodontically Treated Maxillary Molars: A Case Report
- 5,232 View
- 47 Download
- 87 Crossref
Research Article
-
In vitro cytotoxicity of four calcium silicate-based endodontic cements on human monocytes, a colorimetric MTT assay - Sedigheh Khedmat, Somayyeh Dehghan, Jamshid Hadjati, Farimah Masoumi, Mohammad Hossein Nekoofar, Paul Michael Howell Dummer
- Restor Dent Endod 2014;39(3):149-154. Published online April 30, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.3.149
-
Abstract
PDFPubReaderePub
Objectives This study was performed to evaluate the cytotoxicity of four calcium silicate-based endodontic cements at different storage times after mixing.
Materials and Methods Capillary tubes were filled with Biodentine (Septodont), Calcium Enriched Mixture (CEM cement, BioniqueDent), Tech Biosealer Endo (Tech Biosealer) and ProRoot MTA (Dentsply Tulsa Dental). Empty tubes and tubes containing Dycal were used as negative and positive control groups respectively. Filled capillary tubes were kept in 0.2 mL microtubes and incubated at 37℃. Each material was divided into 3 groups for testing at intervals of 24 hr, 7 day and 28 day after mixing. Human monocytes were isolated from peripheral blood mononuclear cells and cocultered with 24 hr, 7 day and 28 day samples of different materials for 24 and 48 hr. Cell viability was evaluated using an MTT assay.
Results In all groups, the viability of monocytes significantly improved with increasing storage time regardless of the incubation time (
p < 0.001). After 24 hr of incubation, there was no significant difference between the materials regarding monocyte viability. However, at 48 hr of incubation, ProRoot MTA and Biodentine were less cytotoxic than CEM cement and Biosealer (p < 0.01).Conclusions Biodentine and ProRoot MTA had similar biocompatibility. Mixing ProRoot MTA with PBS in place of distilled water had no effect on its biocompatibility. Biosealer and CEM cement after 48 hr of incubation were significantly more cytotoxic to on monocyte cells compared to ProRoot MTA and Biodentine.
-
Citations
Citations to this article as recorded by- Comprehensive review of composition, properties, clinical applications, and future perspectives of calcium-enriched mixture (CEM) cement: a systematic analysis
Saeed Asgary, Mahtab Aram, Mahta Fazlyab
BioMedical Engineering OnLine.2024;[Epub] CrossRef - Biocompatibility of mineral trioxide aggregate and biodentine as root-end filling materials: an in vivo study
Mohamed Nabeel, Ashraf M. Abu-Seida, Abeer A. Elgendy, Hossam M. Tawfik
Scientific Reports.2024;[Epub] CrossRef - Apoptotic effects of biodentine, calcium-enriched mixture (CEM) cement, ferric sulfate, and mineral trioxide aggregate (MTA) on human mesenchymal stem cells isolated from the human pulp of exfoliated deciduous teeth
Bahareh NAZEMI SALMAN, Mahshid MOHEBBI RAD, Ehsan SABURI
Minerva Dental and Oral Science.2024;[Epub] CrossRef - Evaluation of the Effects of Retro-Cavity Preconditioning with or Without Ethylenediaminetetraacetic Acid on Root Surface pH and Dislodgement Resistance of NeoMTA2 and Mineral Trioxide Aggregate Flow Retro-Fills: An Ex Vivo Investigation
Sedigheh Khedmat, Seyyed Ali Abaee, Hadi Assadian, Antonio Signore, Stefano Benedicenti
Journal of Functional Biomaterials.2024; 16(1): 3. CrossRef - Bone morphogenetic proteins in biomineralization of two endodontic restorative cements
Tamara A. Souza, Mirna M. Bezerra, Paulo G. B. Silva, José J. N. Costa, Rayssa F. L. A. Carneiro, Janice O. F. Barcelos, Bruno C. Vasconcelos, Hellíada V. Chaves
Journal of Biomedical Materials Research Part B: Applied Biomaterials.2021; 109(3): 348. CrossRef - Cytotoxicity and Bioactivity of Mineral Trioxide Aggregate and Bioactive Endodontic Type Cements: A Systematic Review
Uma Dixit, Rucha Shivajirao Bhise Patil, Rupanshi Parekh
International Journal of Clinical Pediatric Dentistry.2021; 14(1): 30. CrossRef - Physicochemical and Biological Properties of Mg-Doped Calcium Silicate Endodontic Cement
Kyung-Hyeon Yoo, Yong-Il Kim, Seog-Young Yoon
Materials.2021; 14(8): 1843. CrossRef - Comparative evaluation of the effect of cold ceramic and MTA-Angelus on cell viability, attachment and differentiation of dental pulp stem cells and periodontal ligament fibroblasts: an in vitro study
Sedigheh Khedmat, Pegah Sarraf, Ehsan Seyedjafari, Parisa Sanaei-rad, Faranak Noori
BMC Oral Health.2021;[Epub] CrossRef - Cytotoxicity of universal dental adhesive systems: Assessment in vitro assays on human gingival fibroblasts
Stefano Pagano, Guido Lombardo, Stefania Balloni, Maria Bodo, Stefano Cianetti, Antonella Barbati, Azadeh Montaseri, Lorella Marinucci
Toxicology in Vitro.2019; 60: 252. CrossRef - The effect of desiccation on water sorption, solubility and hygroscopic volumetric expansion of dentine replacement materials
Ruba Mustafa, Ruwaida Z. Alshali, Nick Silikas
Dental Materials.2018; 34(8): e205. CrossRef - Evaluation of the Viability of Rat Periodontal Ligament Cells after Storing at 0℃/2 MPa Condition up to One Week: In Vivo MTT Method
Sun Mi Jang, Sin-Yeon Cho, Eui-Seong Kim, Il-Young Jung, Seung Jong Lee
Journal of Korean Dental Science.2016; 9(1): 1. CrossRef - Cytotoxic effects of one‐step self‐etching adhesives on an odontoblast cell line
Yoon Lee, So‐Youn An, Yoon‐Jung Park, Frank H. Yu, Joo‐Cheol Park, Deog‐Gyu Seo
Scanning.2016; 38(1): 36. CrossRef - Influence of Biodentine® - A Dentine Substitute - On Collagen Type I Synthesis in Pulp Fibroblasts In Vitro
Frangis Nikfarjam, Kim Beyer, Anke König, Matthias Hofmann, Manuel Butting, Eva Valesky, Stefan Kippenberger, Roland Kaufmann, Detlef Heidemann, August Bernd, Nadja Nicole Zöller, Dimitrios Karamichos
PLOS ONE.2016; 11(12): e0167633. CrossRef - Evaluation of cytotoxicity and gelatinases activity in 3T3 fibroblast cell by root repair materials
Varol Basak, Tuna Elif Bahar, Karsli Emine, Kasimoglu Yelda, Koruyucu Mine, Seymen Figen, Nurten Rustem
Biotechnology & Biotechnological Equipment.2016; 30(5): 984. CrossRef - In VitroCytotoxicity of Calcium Silicate-Based Endodontic Cement as Root-End Filling Materials
Selen Küçükkaya, Mehmet Ömer Görduysus, Naciye Dilara Zeybek, Sevda Fatma Müftüoğlu
Scientifica.2016; 2016: 1. CrossRef - Cytotoxic effects of mineral trioxide aggregate, calcium enrichedmixture cement, Biodentine and octacalcium pohosphate onhuman gingival fibroblasts
Eshagh A. Saberi, Narges Farhadmollashahi, Faroogh Ghotbi, Hamed Karkeabadi, Roholla Havaei
Journal of Dental Research, Dental Clinics, Dental Prospects.2016; 10(2): 75. CrossRef - Cytotoxicity and Initial Biocompatibility of Endodontic Biomaterials (MTA and Biodentine™) Used as Root-End Filling Materials
Diana María Escobar-García, Eva Aguirre-López, Verónica Méndez-González, Amaury Pozos-Guillén
BioMed Research International.2016; 2016: 1. CrossRef - Cytotoxicity and osteogenic potential of silicate calcium cements as potential protective materials for pulpal revascularization
Eduardo A. Bortoluzzi, Li-na Niu, Chithra D. Palani, Ahmed R. El-Awady, Barry D. Hammond, Dan-dan Pei, Fu-cong Tian, Christopher W. Cutler, David H. Pashley, Franklin R. Tay
Dental Materials.2015; 31(12): 1510. CrossRef
- Comprehensive review of composition, properties, clinical applications, and future perspectives of calcium-enriched mixture (CEM) cement: a systematic analysis
- 2,919 View
- 6 Download
- 18 Crossref
Case Report
- Surgical management of a failed internal root resorption treatment: a histological and clinical report
- Saeed Asgary, Mohammad Jafar Eghbal, Leili Mehrdad, Sanam Kheirieh, Ali Nosrat
- Restor Dent Endod 2014;39(2):137-142. Published online March 21, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.2.137
-
Abstract
PDFPubReaderePub
This article presents the successful surgical management of a failed mineral trioxide aggregate (MTA) orthograde obturation of a tooth with a history of impact trauma and perforated internal root resorption. A symptomatic maxillary lateral incisor with a history of perforation due to internal root resorption and nonsurgical repair using MTA was referred. Unintentional overfill of the defect with MTA had occurred 4 yr before the initial visit. The excess MTA had since disappeared, and a radiolucent lesion adjacent to the perforation site was evident radiographically. Surgical endodontic retreatment was performed using calcium enriched mixture (CEM) cement as a repair material. Histological examination of the lesion revealed granulation tissue with chronic inflammation, and small fragments of MTA encapsulated within fibroconnective tissue. At the one and two year follow up exams, all signs and symptoms of disease had resolved and the tooth was functional. Complete radiographic healing of the lesion was observed two years after the initial visit. This case report illustrates how the selection of an appropriate approach to treatment of a perforation can affect the long term prognosis of a tooth. In addition, extrusion of MTA into a periradicular lesion should be avoided.
-
Citations
Citations to this article as recorded by- Multidisciplinary Management of Severe Iatrogenic Injury to the Maxillary Incisors Following Mesiodens Extraction
Prabhleen Brar, Sudhir Bhandari, Raj K Verma
Cureus.2026;[Epub] CrossRef - Managing Internal Inflammatory Root Resorption and Perforation of a Mandibular Primary Molar: A Case Report With 15 Months Follow‐Up
Mana Mowji, Motahareh Khosrojerdi
Clinical Case Reports.2025;[Epub] CrossRef - Endodontic management of internal replacement resorption of two maxillary central incisors with the aid of cone-beam computed tomography as the diagnostic tool: a case report and review of literature
Fatemeh Eskandari, Safoora Sahebi, Negar Ghorbani Jahandizi, Hossein Mofidi
Journal of Medical Case Reports.2025;[Epub] CrossRef - Removal of AH Plus Bioceramic Sealer from Artificial Internal Resorption Cavities Using Different Irrigation Activation Systems
Mine Büker, Meltem Sümbüllü, Emine Şimşek, Fadime Sena Sezer
Cumhuriyet Dental Journal.2025; 28(3): 383. CrossRef - Evaluation of the effectiveness of different supplemental cleaning techniques in the retreatment of roots with small simulated internal resorption cavities: an in vitro comparative study
Sine Güngör Us, Özgür Uzun, Nazlı Merve Güngör
BMC Oral Health.2025;[Epub] CrossRef - Comprehensive review of composition, properties, clinical applications, and future perspectives of calcium-enriched mixture (CEM) cement: a systematic analysis
Saeed Asgary, Mahtab Aram, Mahta Fazlyab
BioMedical Engineering OnLine.2024;[Epub] CrossRef - The various forms of tooth resorption
Jordan Samuel Blum
Australian Endodontic Journal.2024; 50(2): 191. CrossRef - Bioceramics in Endodontics: Updates and Future Perspectives
Xu Dong, Xin Xu
Bioengineering.2023; 10(3): 354. CrossRef - Imaging techniques and various treatment modalities used in the management of internal root resorption: A systematic review
R. S Digholkar, S D Aggarwal, P S Kurtarkar, P. B Dhatavkar, V L Neil, D N Agarwal
Endodontology.2023; 35(2): 85. CrossRef - Treatment of Teeth with Root Resorptions: A Case Report and Systematic Review
Damla Erkal, Abdullah Başoğlu, Damla Kırıcı, Nezahat Arzu Kayar, Simay Koç, Kürşat Er
Galician Medical Journal.2023;[Epub] CrossRef - Effects of calcium silicate cements on neuronal conductivity
Derya Deniz-Sungur, Mehmet Ali Onur, Esin Akbay, Gamze Tan, Fügen Daglı-Comert, Taner Cem Sayın
Restorative Dentistry & Endodontics.2022;[Epub] CrossRef - Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part II: other clinical applications and complications
M. Torabinejad, M. Parirokh, P. M. H. Dummer
International Endodontic Journal.2018; 51(3): 284. CrossRef - Periodontal healing following non-surgical repair of an old perforation with pocket formation and oral communication
Saeed Asgary, Prashant Verma, Ali Nosrat
Restorative Dentistry & Endodontics.2018;[Epub] CrossRef - Conservative Management of Class 4 Invasive Cervical Root Resorption Using Calcium-enriched Mixture Cement
Saeed Asgary, Ali Nosrat
Journal of Endodontics.2016; 42(8): 1291. CrossRef - Importance of CBCT in the management plan of upper canine with internal resorption
Roberto Fornara, Dario Re Cecconi
Giornale Italiano di Endodonzia.2015; 29(2): 70. CrossRef
- Multidisciplinary Management of Severe Iatrogenic Injury to the Maxillary Incisors Following Mesiodens Extraction
- 3,324 View
- 24 Download
- 15 Crossref
Research Article
- A preliminary report on histological outcome of pulpotomy with endodontic biomaterials vs calcium hydroxide
- Ali Nosrat, Ali Peimani, Saeed Asgary
- Restor Dent Endod 2013;38(4):227-233. Published online November 12, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.4.227
-
Abstract
PDFPubReaderePub
Objectives The purpose of the study was to evaluate human dental pulp response to pulpotomy with calcium hydroxide (CH), mineral trioxide aggregate (MTA), and calcium enriched mixture (CEM) cement.
Materials and Methods A total of nine erupted third molars were randomly assigned to each pulpotomy group. The same clinician performed full pulpotomies and coronal restorations. The patients were followed clinically for six months; the teeth were then extracted and prepared for histological assessments. The samples were blindly assessed by an independent observer for pulp vitality, pulp inflammation, and calcified bridge formation.
Results All patients were free of clinical signs/symptoms of pulpal/periradicular diseases during the follow up period. In CH group, one tooth had necrotic radicular pulp; other two teeth in this group had vital uninflamed pulps with complete dentinal bridge formation. In CEM cement and MTA groups all teeth had vital uninflamed radicular pulps. A complete dentinal bridge was formed beneath CEM cement and MTA in all roots. Odontoblast-like cells were present beneath CEM cement and MTA in all samples.
Conclusions This study revealed that CEM cement and MTA were reliable endodontic biomaterials in full pulpotomy treatment. In contrast, the human dental pulp response to CH might be unpredictable.
-
Citations
Citations to this article as recorded by- Long-term Outcome of Vital Pulp Therapy and Regenerative Endodontic Procedures in Immature Permanent Maxillary Incisors: A 7-year Follow-up Case Report
Mulham Almaliki, Motaz Almaghraby, Abdulaziz Bakhsh
International Journal of Clinical Pediatric Dentistry.2026; 19(3): 403. CrossRef - A meta‐analysis of calcium silicate‐based cements and calcium hydroxide as promoters of hard tissue bridge formation
Emmanuel J. N. L. Silva, Karem P. Pinto, Fernanda N. S. J. Riche, Maristela G. H. Carestiato, Jorge N. R. Martins, Henry F. Duncan, Marco A. Versiani, Gustavo De‐Deus
International Endodontic Journal.2025; 58(5): 685. CrossRef - Clinical and radiographic outcomes of pulpotomy materials in permanent teeth: a systematic review of calcium hydroxide, MTA, biodentine, and iRoot BP plus
Anggi Putri Riandani, Arief Cahyanto, Rana Abdelbaset Lotfy Diab, Ratih Widyasari, Atia Nurul Sidiqa, Hendra Dian Adhita Dharsono, Myrna Nurlatifah Zakaria
BMC Oral Health.2025;[Epub] CrossRef - Comprehensive review of composition, properties, clinical applications, and future perspectives of calcium-enriched mixture (CEM) cement: a systematic analysis
Saeed Asgary, Mahtab Aram, Mahta Fazlyab
BioMedical Engineering OnLine.2024;[Epub] CrossRef - Hard tissue formation in pulpotomized primary teeth in dogs with nanomaterials MCM-48 and MCM-48/hydroxyapatite: an in vivo animal study
Sahar Talebi, Nosrat Nourbakhsh, Ardeshir Talebi, Amir Abbas Nourbakhsh, Abbas Haghighat, Maziar Manshayi, Hamid Reza Bakhsheshi, Razieh Karimi, Rahman Nazeri, Kenneth J.D. Mackenzie
BMC Oral Health.2024;[Epub] CrossRef - The Role of Growth Factor Delivery Systems on Cellular Activities of Dental
Stem Cells: A Systematic Review (Part II)
Sayna Shamszadeh, Armin Shirvani, Saeed Asgary
Current Stem Cell Research & Therapy.2024; 19(4): 587. CrossRef - Calcium Silicate-Based Cements in Restorative Dentistry: Vital Pulp Therapy Clinical, Radiographic, and Histological Outcomes on Deciduous and Permanent Dentition—A Systematic Review and Meta-Analysis
Maria Teresa Xavier, Ana Luísa Costa, João Carlos Ramos, João Caramês, Duarte Marques, Jorge N. R. Martins
Materials.2024; 17(17): 4264. CrossRef - Pulpotomy: An alternative treatment modality to conventional root canal treatment
Günther Streit, Martin Vorster, Peet J Van der Vyver
South African Dental Journal.2023; 78(06): 309. CrossRef - A Comparative Histological Analysis of Human Pulp Following Direct Pulp Capping with Propolis or Biodentine
Nehad A Ahmad, Nevin A. Gad, Marwa H. Abdulmonaem
Journal of Nature and Science of Medicine.2022; 5(3): 281. CrossRef - Expression of Matrix Metalloproteinases-8 and Myeloperoxidase in Pulp Tissue after Pulpotomy with Calcium Silicate Cements
Nayara Nery de Oliveira Cunha, Marina Azevedo Junqueira, Leopoldo Cosme-Silva, Laís da Silveira Terra Santos, George Augusto Veloso de Oliveira, Rafael Tobias Moretti Neto, Denismar Alves Nogueira, Maísa Ribeiro Pereira Lima Brigagão, Ana Beatriz da Silve
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2021;[Epub] CrossRef - Long-term Outcomes of Full Pulpotomy in Permanent Molars for Patients Treated in a Single, Short Session under Special Conditions
Natacha Linas, Nicolas Decerle, Marie-Laure Munoz-Sanchez, Denise Faulks, Valérie Collado, Emmanuel Nicolas, Martine Hennequin, Pierre-Yves Cousson
Journal of Endodontics.2020; 46(11): 1597. CrossRef - Quantitative Assessment of Root Development after Regenerative Endodontic Therapy: A Systematic Review and Meta-Analysis
Teng Kai Ong, Ghee Seong Lim, Maharaj Singh, Alissa V. Fial
Journal of Endodontics.2020; 46(12): 1856. CrossRef - Dexamethasone- loaded polymeric porous sponge as a direct pulp capping agent
Amjad Alagha, Abdulwahab Nourallah, Sahar Alhariri
Journal of Biomaterials Science, Polymer Edition.2020; 31(13): 1689. CrossRef - Postendodontic Pain after Pulpotomy or Root Canal Treatment in Mature Teeth with Carious Pulp Exposure: A Multicenter Randomized Controlled Trial
Mohammad Jafar Eghbal, Ali Haeri, Arash Shahravan, Ali Kazemi, Fariborz Moazami, Mohammad Ali Mozayeni, Eshaghali Saberi, Mohammad Samiei, Mehdi Vatanpour, Alireza Akbarzade Baghban, Mahta Fazlyab, Ardavan Parhizkar, Mahboobe Ahmadi, Nazila Akbarian Rad,
Pain Research and Management.2020; 2020: 1. CrossRef - Vital Pulp Therapy as a Conservative Approach for Management of Invasive Cervical Root Resorption: A Case Series
Saeed Asgary, Mahdieh Nourzadeh, Prashant Verma, M. Lamar Hicks, Ali Nosrat
Journal of Endodontics.2019; 45(9): 1161. CrossRef - Which procedures and materials could be applied for full pulpotomy in permanent mature teeth? A systematic review
M. Zanini, M. Hennequin, PY. Cousson
Acta Odontologica Scandinavica.2019; 77(7): 541. CrossRef - Periodontal healing following non-surgical repair of an old perforation with pocket formation and oral communication
Saeed Asgary, Prashant Verma, Ali Nosrat
Restorative Dentistry & Endodontics.2018;[Epub] CrossRef - Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part I: vital pulp therapy
M. Parirokh, M. Torabinejad, P. M. H. Dummer
International Endodontic Journal.2018; 51(2): 177. CrossRef - Treatment Outcomes of 4 Vital Pulp Therapies in Mature Molars
Saeed Asgary, Raheleh Hassanizadeh, Hassan Torabzadeh, Mohammad Jafar Eghbal
Journal of Endodontics.2018; 44(4): 529. CrossRef - A Review of Criteria for the Evaluation of Pulpotomy Outcomes in Mature Permanent Teeth
Marjorie Zanini, Martine Hennequin, Pierre-Yves Cousson
Journal of Endodontics.2016; 42(8): 1167. CrossRef - Calcium-Enriched Mixture Pulpotomy of Primary Molar Teeth with Irreversible Pulpitis. A Clinical Study
Mahtab Memarpour, Soleiman Fijan, Saeed Asgary, Marzieh Keikhaee
The Open Dentistry Journal.2016; 10(1): 43. CrossRef - Endodontie in der unreifen bleibenden Dentition — Maßnahmen zur Vitalerhaltung, Apexifikation und Regeneration der Pulpa
Martin Jung
Oralprophylaxe & Kinderzahnheilkunde.2016; 38(1): 29. CrossRef - Conservative Management of Class 4 Invasive Cervical Root Resorption Using Calcium-enriched Mixture Cement
Saeed Asgary, Ali Nosrat
Journal of Endodontics.2016; 42(8): 1291. CrossRef - Permanent teeth pulpotomy survival analysis: retrospective follow-up
Gustavo Golgo Kunert, Itaborai Revoredo Kunert, Luiz Cesar da Costa Filho, José Antônio Poli de Figueiredo
Journal of Dentistry.2015; 43(9): 1125. CrossRef - Cytocompatibility and Antibacterial Properties of Capping Materials
Claudio Poggio, Carla Renata Arciola, Riccardo Beltrami, Annachiara Monaco, Alberto Dagna, Marco Lombardini, Livia Visai
The Scientific World Journal.2014; 2014: 1. CrossRef - Surgical management of a failed internal root resorption treatment: a histological and clinical report
Saeed Asgary, Mohammad Jafar Eghbal, Leili Mehrdad, Sanam Kheirieh, Ali Nosrat
Restorative Dentistry & Endodontics.2014; 39(2): 137. CrossRef - Effect of Mineral Trioxide Aggregate Surface Treatments on Morphology and Bond Strength to Composite Resin
Joo-Hee Shin, Ji-Hyun Jang, Sang Hyuk Park, Euiseong Kim
Journal of Endodontics.2014; 40(8): 1210. CrossRef
- Long-term Outcome of Vital Pulp Therapy and Regenerative Endodontic Procedures in Immature Permanent Maxillary Incisors: A 7-year Follow-up Case Report
- 3,059 View
- 18 Download
- 27 Crossref
 First
First Prev
Prev

