
Search
- Page Path
- HOME > Search
Research Articles
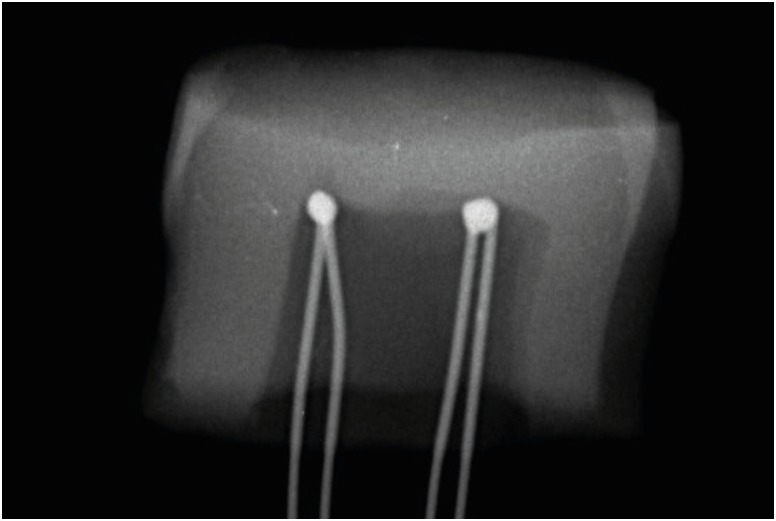
- Effect of cooling water temperature on the temperature changes in pulp chamber and at handpiece head during high-speed tooth preparation
- Ra'fat I. Farah
- Restor Dent Endod 2019;44(1):e3. Published online December 24, 2018
- DOI: https://doi.org/10.5395/rde.2019.44.e3
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub Objectives It was the aim of this study to evaluate the effect of cooling water temperature on the temperature changes in the pulp chamber and at the handpiece head during high-speed tooth preparation using an electric handpiece.
Materials and Methods Twenty-eight intact human molars received a standardized occlusal preparation for 60 seconds using a diamond bur in an electric handpiece, and one of four treatments were applied that varied in the temperature of cooling water applied (control, with no cooling water, 10°C, 23°C, and 35°C). The temperature changes in the pulp chamber and at the handpiece head were recorded using K-type thermocouples connected to a digital thermometer.
Results The average temperature changes within the pulp chamber and at the handpiece head during preparation increased substantially when no cooling water was applied (6.8°C and 11.0°C, respectively), but decreased significantly when cooling water was added. The most substantial drop in temperature occurred with 10°C water (−16.3°C and −10.2ºC), but reductions were also seen at 23°C (−8.6°C and −4.9°C). With 35°C cooling water, temperatures increased slightly, but still remained lower than the no cooling water group (1.6°C and 6.7ºC).
Conclusions The temperature changes in the pulp chamber and at the handpiece head were above harmful thresholds when tooth preparation was performed without cooling water. However, cooling water of all temperatures prevented harmful critical temperature changes even though water at 35°C raised temperatures slightly above baseline.
-
Citations
Citations to this article as recorded by
- Efficacy Assessment of a Novel Device for Dental Aerosol Capture and Inactivation: An In Vitro Study
Yan Sun, Jia-Chun Li, Yu-Gang Li, Xiao-Yan Yu, Jie Hu, Zhe Li, Ji-Chao Cao
International Dental Journal.2026; 76(2): 109331. CrossRef - Comparison of Two Fiber Post Removal Techniques Evaluating Dentin Removal, Efficiency, and Heat Production
Matthew Fenigstein, Mazin Askar, Ahmad Maalhagh-Fard, Susan Paurazas
Dentistry Journal.2025; 13(6): 234. CrossRef - Polymethyl Methacrylate (PMMA): An Overview of Its Biological Activities, Properties, Polymerization, Modifications, and Dental and Industrial Applications
Great Iruoghene Edo, Emad Yousif, Mohammed H. Al-Mashhadani
Regenerative Engineering and Translational Medicine.2025;[Epub] CrossRef - The Effect of Water Coolant and Bur Type on Pulp Temperature When Removing Tooth Structure and Restorative Dental Materials
C Mafrici, M Kingston, R Grice, PV Abbott
Operative Dentistry.2024; 49(1): 91. CrossRef - A Finite Element Method Study on a Simulation of the Thermal Behaviour of Four Methods for the Restoration of Class II Cavities
Adela Nicoleta Staicu, Mihaela Jana Țuculină, Cristian Niky Cumpătă, Ana Maria Rîcă, Maria Cristina Beznă, Dragoș Laurențiu Popa, Alexandru Dan Popescu, Oana Andreea Diaconu
Journal of Functional Biomaterials.2024; 15(4): 86. CrossRef - In vitro comparison of guide planes for removable partial dentures prepared with CAD-CAM-assisted templates, guiding rod templates, and freehand
Ni Cheng, Hai Yu, Wenxi Shan, Jiang Wu
Journal of Dentistry.2024; 149: 105322. CrossRef - Comparison of antimicrobial efficacy of different disinfectants on the biofilm formation in dental unit water systems using dip slide and conventional methods: A pilot study
Pelin Özmen, Hilal Erdoğan, Aslıhan Güngördü, Bülent Pişkin, Funda Kont Çobankara, Serdar Sütcü, Nesrin Şahin
Microscopy Research and Technique.2024; 87(6): 1241. CrossRef - Analysis of the Pulpal Blood Flow Microdynamics during Prosthetic Tooth Preparation Using Diamond Burs with Different Degrees of Wear
Edmond Ciora, Mariana Miron, Diana Lungeanu, Andreea Igna, Anca Jivanescu
Dentistry Journal.2024; 12(6): 178. CrossRef - Bacterial contamination potential of personal protective equipment itself in dental aerosol-producing treatments
Madline Priska Gund, Jusef Naim, Stefan Rupf, Barbara Gärtner, Matthias Hannig
Odontology.2024; 112(2): 309. CrossRef - Patient satisfaction before and after occlusal adjustment using a visual analog scale
Ha-Rim Lee, Sun-Haeng Lee, Gyeong-Je Lee
Oral Biology Research.2023; 47(1): 8. CrossRef - Heat generated during dental treatments affecting intrapulpal temperature: a review
Xin Er Lau, Xiaoyun Liu, Helene Chua, Wendy Jingwen Wang, Maykon Dias, Joanne Jung Eun Choi
Clinical Oral Investigations.2023; 27(5): 2277. CrossRef - “The effect of diode laser 940 nm and 445 nm on the rise in temperature of a pulp simulating material: in vitro study”
Basant Bahaaeldin, Ola Ibrahim Fahmy, Amira Zoghaby, Rene Franzen
Lasers in Dental Science.2023; 7(3): 147. CrossRef - Evaluation of the Pulp Chamber Temperature during Tooth Veneer Preparation Using Burs with Different Degrees of Wear—A Preliminary In Vitro Study
Edmond Ciora, Mariana Miron, Daliana Bojoga, Diana Lungeanu, Anca Jivanescu
Dentistry Journal.2023; 11(8): 197. CrossRef - Effect of spray air settings of speed-increasing contra-angle handpieces on intrapulpal temperatures, drilling times, and coolant spray pattern
Edina Lempel, József Szalma
Clinical Oral Investigations.2022; 26(1): 523. CrossRef - Preparing guiding planes for removable partial dentures: an in vitro comparison between assisted CAD-CAM template procedure and freehand preparation
Hefei Bai, Hongqiang Ye, Hu Chen, Yong Wang, Yongsheng Zhou, Yuchun Sun
Journal of Dentistry.2022; 123: 104166. CrossRef - Yeni Tip Koronavirüs (COVID-19) Salgınının Diş Hekimlerinin Tedavi Kliniği Düzeni Üzerine Etkisi
Onur Altuğ SAKALLI, Sedanur SAKALLI, Aleyna Öykü AKBAŞAK, Selim ERKUT
ADO Klinik Bilimler Dergisi.2022; 11(2): 140. CrossRef - Aerosol suppression from a handpiece using viscoelastic solution in confined dental office
Yong Il Kim, Seongpil An, Jungwoo Huh, Yang-Soo Kim, Jihye Heo, In-Seok Song, Alexander L. Yarin, Sam S. Yoon
Physics of Fluids.2022;[Epub] CrossRef - Coronavirus Disease (COVID-19) Transmission through Aerosols in Restorative and Endodontic Practice
Ambar W. Raut, Priyatama V. Meshram, Radha A. Raut
Annals of African Medicine.2022; 21(1): 1. CrossRef - Redefining aerosol in dentistry during COVID-19 pandemic
Kanupriya Rathore, HarshvardhanSingh Rathore, Pranshu Singh, Pravin Kumar
Dental Research Journal.2022; 19(1): 53. CrossRef - Different grinding speeds affect induced regeneration capacity of human treated dentin matrix
Min Li, Sen Yang, Jinlin Song, Tiwei Fu, Panpan Liang, Zhi Gao, Jing Tang, Lijuan Guo
Journal of Biomedical Materials Research Part B: Applied Biomaterials.2022; 110(4): 755. CrossRef -
In Vivo Pulp Temperature Changes During Class V Cavity Preparation and Resin Composite Restoration in Premolars
DC Zarpellon, P Runnacles, C Maucoski, DJ Gross, U Coelho, FA Rueggeberg, CAG Arrais
Operative Dentistry.2021; 46(4): 374. CrossRef - In vivo evaluation of the virucidal efficacy of chlorhexidine and povidone-iodine mouthwashes against salivary SARS-CoV-2. A randomized-controlled clinical trial
Rola Elzein, Fadi Abdel-Sater, Soha Fakhreddine, Pierre Abi Hanna, Rita Feghali, Hassan Hamad, Fouad Ayoub
Journal of Evidence Based Dental Practice.2021; 21(3): 101584. CrossRef - Possible transmission of Covid-19 & precautions in a dental setting: A review
Sonali Gholap, Amit Mani, Shubhangi Mani, Shivani Sachdeva, Jasleen Kaur Sodhi, Hiral Vora
IP International Journal of Periodontology and Implantology.2021; 6(2): 98. CrossRef - An Evaluation of Two Systems for the Management of the Microbiological Quality of Water in Dental Unit Waterlines: Hygowater® and IGN Calbénium®
Damien Offner, Anne-Marie Musset
International Journal of Environmental Research and Public Health.2021; 18(10): 5477. CrossRef - Restoration of dental services after COVID-19: The fallow time determination with laser light scattering
Xiujie Li, Cheuk Ming Mak, Kuen Wai Ma, Hai Ming Wong
Sustainable Cities and Society.2021; 74: 103134. CrossRef - Possible aerosol transmission of COVID-19 and special precautions in dentistry
Zi-yu Ge, Lu-ming Yang, Jia-jia Xia, Xiao-hui Fu, Yan-zhen Zhang
Journal of Zhejiang University-SCIENCE B.2020; 21(5): 361. CrossRef - Yeni Koronavirüs Salgını ve Diş Hekimliği Tedavileri Üzerine Etkileri
Elif Ballıkaya, Gülce Esentürk, Gizem Erbaş Ünverdi, Zafer Cehreli
Hacettepe University Faculty of Health Sciences Journal.2020; 7(2): 92. CrossRef - Dentistry: its Role in the Transmission of SARS-CoV-2 Through Bioaerosols
Reinaldo Rodríguez Aguilar
Odovtos - International Journal of Dental Sciences.2020; 22(3): 103. CrossRef
- Efficacy Assessment of a Novel Device for Dental Aerosol Capture and Inactivation: An In Vitro Study
- 6,540 View
- 57 Download
- 28 Crossref

- Finishing and polishing effects of multiblade burs on the surface texture of 5 resin composites: microhardness and roughness testing
- Elodie Ehrmann, Etienne Medioni, Nathalie Brulat-Bouchard
- Restor Dent Endod 2019;44(1):e1. Published online November 26, 2018
- DOI: https://doi.org/10.5395/rde.2019.44.e1

-
Abstract
PDFPubReaderePub
Objectives The aim of this
in vitro study was to test the effect of 2 finishing–polishing sequences (QB, combining a 12/15-fluted finishing bur and an EVO-Light polisher; QWB, adding a 30-fluted polishing bur after the 12/15-fluted finishing bur used in the QB sequence) on 5 nanotech-based resin composites (Filtek Z500, Ceram X Mono, Ceram X Duo, Tetric Evoceram, and Tetric Evoceram Bulk Fill) by comparing their final surface roughness and hardness values to those of a Mylar strip control group (MS).Materials and Methods Twelve specimens of each nanocomposite were prepared in Teflon moulds. The surface of each resin composite was finished with QB (5 samples), QWB (5 samples), or MS (2 samples), and then evaluated (60 samples). Roughness was analysed with an optical profilometer, microhardness was tested with a Vickers indenter, and the surfaces were examined by optical and scanning electron microscopy. Data were analysed using the Kruskal-Wallis test (
p < 0.05) followed by the Dunn test.Results For the hardness and roughness of nanocomposite resin, the QWB sequence was significantly more effective than QB (
p < 0.05). The Filtek Z500 showed significantly harder surfaces regardless of the finishing–polishing sequence (p < 0.05).Conclusions QWB yielded the best values of surface roughness and hardness. The hardness and roughness of the 5 nanocomposites presented less significant differences when QWB was used.
-
Citations
Citations to this article as recorded by- The Influence of Different Polishing Systems on the Gloss and Surface Roughness of Two Distinct Nano‐Filled Composites
Abdulrahman Alghamdi, Hanan Filemban
Journal of Esthetic and Restorative Dentistry.2026; 38(7): 1448. CrossRef - The effect of reduced-step finishing and polishing protocols on roughness, gloss, and surface quality of bulk-fill resin-based composites
Rawan N. AlKahtani, Ghada Alharbi, Hala Aly Maher Ragab, Reem Abdullah AlKhalaf, Abrar Nasser Bin Nooh, Sarah Alghamdi
BMC Oral Health.2026;[Epub] CrossRef - Effect of modeling liquid application on color stability and surface roughness of single-shade composites
Melek Güven Bekdaş, Ihsan Hubbezoglu
BMC Oral Health.2025;[Epub] CrossRef - Effects of different charcoal-containing whitening toothpastes on color and surface roughness of a supra-nanofilled composite resin
Meltem Nermin Polan, Sevil Gurgan
BMC Oral Health.2025;[Epub] CrossRef - Impact of different polishing techniques on surface roughness, gloss, and microhardness of zirconium oxide reinforced flowable bulk-fill resin composite: an in vitro study
Amr Elsayed Elnahas, Mohamed Elshirbeny Elawsya, Abeer ElSayed ElEmbaby
BMC Oral Health.2025;[Epub] CrossRef - Tek Renkli Monokromatik Kompozit Rezinlerle İlgili Bir Durum Değerlendirmesi
Kubra Nur Yeşilova, Sebnem Turkun
Selcuk Dental Journal.2025; 12(2): 331. CrossRef - Effect of different finishing and polishing systems on surface properties of universal single shade resin-based composites
Ghada Alharbi, Hend NA Al Nahedh, Loulwa M. Al-Saud, Nourah Shono, Ahmed Maawadh
BMC Oral Health.2024;[Epub] CrossRef - A comparative study of polishing systems on optical properties and surface roughness of additively manufactured and conventional resin based composites
Ayse Tugba Erturk-Avunduk, Sevim Atılan-Yavuz, Hande Filiz, Esra Cengiz-Yanardag
Scientific Reports.2024;[Epub] CrossRef - Effect of Instrument Lubricant on Mechanical Properties of Restorative Composite
G Pippin, D Tantbirojn, M Wolfgang, JS Nordin, A Versluis
Operative Dentistry.2024; 49(4): 475. CrossRef - An In Vitro Study regarding the Wear of Composite Materials Following the Use of Dental Bleaching Protocols
Alexandru Dan Popescu, Mihaela Jana Ţuculină, Lelia Mihaela Gheorghiță, Andrei Osman, Claudiu Nicolicescu, Smaranda Adelina Bugălă, Mihaela Ionescu, Jaqueline Abdul-Razzak, Oana Andreea Diaconu, Bogdan Dimitriu
Journal of Functional Biomaterials.2023; 14(10): 532. CrossRef - Akıllı Kromatik Teknolojili Kompozit Rezinlerin Farklı pH Değerlerindeki Sıvılarda Bekletilmesi Sonrası Oluşan Yüzey Pürüzlülüğü ve Renk Değişimlerinin Değerlendirilmesi
Fatih ÖZNURHAN, Aylin ÖZEL
Farabi Tıp Dergisi.2023; 2(4): 17. CrossRef - Enamel surface roughness evaluation after debonding and residual resin removal using four different burs
Rapeti Madhu Vanya, Anil Chirla, Uday Kumar Digumarthi, Tarakesh Karri, Bommareddy Radhika, Sanapala Manojna
Journal of Contemporary Orthodontics.2023; 7(3): 173. CrossRef - Finishing and Polishing of Composite Restoration: Assessment of Knowledge, Attitude and Practice Among Various Dental Professionals in India
Sankar Vishwanath, Sadasiva Kadandale, Senthil kumar Kumarappan, Anupama Ramachandran, Manu Unnikrishnan, Honap manjiri Nagesh
Cureus.2022;[Epub] CrossRef - Evaluation of different composite resin finishing and polishing protocols by confocal laser scan microscopy
Kayo Matheus Rodrigues de Souza, Roberto Victor de Melo Silva, Marlon Ferreira Dias, Paulo Cardoso Lins-Filho, Claudio Heliomar Vicente da Silva, Renata Pedrosa Guimarães
Brazilian Journal of Oral Sciences.2022; 21: e225334. CrossRef - Laboratory methods to simulate the mechanical degradation of resin composite restorations
Veronica P. Lima, Jaqueline B. Machado, Yu Zhang, Bas A.C. Loomans, Rafael R. Moraes
Dental Materials.2022; 38(1): 214. CrossRef - FARKLI POLİSAJ SİSTEMLERİNİN POSTERİOR BÖLGEDE KULLANILAN KOMPOZİT REZİNLERİN YÜZEY PÜRÜZLÜLÜĞÜ ÜZERİNE ETKİSİ
Meltem Nermin DURSUN, Cansu ATALAY
Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi.2022; : 1. CrossRef - The Effect of Additional Finishing and Polishing Sequences on Hardness and Roughness of Two Different Dental Composites: An In Vitro Study
Kıvanç Dülger
Journal of Advanced Oral Research.2022; 13(2): 216. CrossRef - Effect of immediate and delayed finishing and polishing procedure on Streptococcal mutans adhesion and micro-hardness of composite resin surface: An in-vitro study
Tushar Kanti Majumdar, Moumita Khatua, Paromita Mazumdar, Sayantan Mukherjee
International Dental Journal of Student's Research.2022; 10(1): 5. CrossRef - Comparison of Polishing Systems on the Surface Roughness of Resin Based Composites Containing Different Monomers
Marina Gullo Augusto, Guilherme Schmitt de Andrade, Ingrid Fernandes Mathias-Santamaria, Amanda Maria de Oliveira Dal Piva, João Paulo Mendes Tribst
Journal of Composites Science.2022; 6(5): 146. CrossRef - THE EFFECT OF PH-CYCLING AND TOOTHBRUSHING SIMULATIONS ON SURFACE ROUGHNESS OF BULK-FILL COMPOSITES
Tuğba MİSİLLİ, Nihan GONULOL, Özge Gizem CABADAĞ, Lena ALMASIFAR, Derya DİNÇ
Clinical and Experimental Health Sciences.2021; 11(3): 487. CrossRef - A three-year randomized clinical trial evaluating direct posterior composite restorations placed with three self-etch adhesives
Joseph Sabbagh, Layal El Masri, Jean Claude Fahd, Paul Nahas
Biomaterial Investigations in Dentistry.2021; 8(1): 92. CrossRef - Press-On Force Effect on the Efficiency of Composite Restorations Final Polishing—Preliminary In Vitro Study
Anna Lehmann, Kacper Nijakowski, Natalia Potempa, Paweł Sieradzki, Mateusz Król, Olaf Czyż, Agnieszka Radziszewska, Anna Surdacka
Coatings.2021; 11(6): 705. CrossRef - Surface evaluations of a nanocomposite after different finishing and polishing systems for anterior and posterior restorations
Riccardo Monterubbianesi, Vincenzo Tosco, Giulia Orilisi, Simone Grandini, Giovanna Orsini, Angelo Putignano
Microscopy Research and Technique.2021; 84(12): 2922. CrossRef - Wear, roughness and microhardness analyses of single increment restorative materials submitted to different challenges in vitro
L. C. Oliveira, P. H. dos Santos, F. S. S. Ramos, M. D. Moda, A. L. F. Briso, T. C. Fagundes
European Archives of Paediatric Dentistry.2021; 22(2): 247. CrossRef - Neurotic personality trait as a predictor in the prognosis of composite restorations: A 24-month clinical follow up study
Sulthan Ibrahim Raja Khan, Dinesh Rao, Anupama Ramachandran, Bhaskaran Veni Ashok, Jagan Kumar Baskaradoss
Scientific Reports.2021;[Epub] CrossRef - The Effect of Finishing and Polishing Sequences on The Surface Roughness of Three Different Nanocomposites and Composite/Enamel and Composite/Cementum Interfaces
Ksenia Babina, Maria Polyakova, Inna Sokhova, Vladlena Doroshina, Marianna Arakelyan, Nina Novozhilova
Nanomaterials.2020; 10(7): 1339. CrossRef - Surface Geometry of Four Conventional Nanohybrid Resin‐Based Composites and Four Regular Viscosity Bulk Fill Resin‐Based Composites after Two‐Step Polishing Procedure
Mateusz Granat, Janusz Cieloszyk, Urszula Kowalska, Jadwiga Buczkowska-Radlińska, Ryta Łagocka, Ali Nokhodchi
BioMed Research International.2020;[Epub] CrossRef - Effect of Polishing Systems on Fluoride Release and Surface Roughness of Different Restorative Materials
Soner Şişmanoğlu DDS, PhD, Burak Gümüştaş DDS, PhD, Zuhal Yıldırım-Bilmez DDS, PhD
Odovtos - International Journal of Dental Sciences.2019; 22(1): 81. CrossRef
- The Influence of Different Polishing Systems on the Gloss and Surface Roughness of Two Distinct Nano‐Filled Composites
- 3,240 View
- 27 Download
- 28 Crossref
- Enamel pretreatment with Er:YAG laser: effects on the microleakage of fissure sealant in fluorosed teeth
- Mahtab Memarpour, Nasrin Kianimanesh, Bahareh Shayeghi
- Restor Dent Endod 2014;39(3):180-186. Published online May 22, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.3.180
-
Abstract
PDFPubReaderePub
Objectives The purpose of this
in vitro study was to evaluate the microleakage and penetration of fissure sealant in permanent molar teeth with fluorosis after pretreatment of the occlusal surface.Materials and Methods A total of 120 third molars with mild dental fluorosis were randomly divided into 6 groups (
n = 20). The tooth surfaces were sealed with an unfilled resin fissure sealant (FS) material. The experimental groups included: 1) phosphoric acid etching (AE) + FS (control); 2) AE + One-Step Plus (OS, Bisco) + FS; 3) bur + AE + FS; 4) bur + AE + OS + FS; 5) Er:YAG laser + AE + FS; and 6) Er:YAG laser + AE + OS + FS. After thermocycling, the teeth were immersed in 0.5% fuchsin and sectioned. Proportions of mircoleakage (PM) and unfilled area (PUA) were measured by digital microscope.Results Overall, there were significant differences among all groups in the PM (
p = 0.00). Group 3 showed the greatest PM, and was significantly different from groups 2 to 6 (p < 0.05). Group 6 showed the lowest PM. Pretreatment with Er:YAG with or without adhesive led to less PM than bur pretreatment. There were no significant differences among groups in PUA.Conclusions Conventional acid etching provided a similar degree of occlusal seal in teeth with fluorosis compared to those pretreated with a bur or Er:YAG laser. Pretreatment of pits and fissures with Er:YAG in teeth with fluorosis may be an alternative method before fissure sealant application.
-
Citations
Citations to this article as recorded by- Comparative Evaluation of the Retention Rates of Composite Resin Pit and Fissure Sealants Placed on Permanent Molars Treated with Air Abrasion and Acid Etching: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Vishal Raut, Deepak Sharma, Ashish K Jain, Rahul Rao, Laresh N Mistry, Supriya Solanke
International Journal of Clinical Pediatric Dentistry.2026; 19(2): 271. CrossRef - Effects of Er: YAG laser and acid etching on bond strength of clear aligner attachments to fluorotic enamel
Rui Xia, Jie Lei, Maoxuan Luo, Yao Xiao, Rawaa A. Faris
PLOS One.2025; 20(8): e0328937. CrossRef - Comparative Evaluation of Penetrative and Adaptive Properties of Unfilled and Filled Resin-Based Sealants When Placed using Conventional acid Etching, Lasing, and Fissurotomy Bur Technique of Enamel Preparation
Poonam Ramrao Shingare, Vishwas Chaugule, Neha Pankey, Pallavi Kakade
Contemporary Clinical Dentistry.2022; 13(4): 349. CrossRef - Laser Tooth Preparation for Pit and Fissure Sealing
Yair Schwimmer, Nurit Beyth, Diana Ram, Eitan Mijiritsky, Esti Davidovich
International Journal of Environmental Research and Public Health.2020; 17(21): 7813. CrossRef - The clinical effects of laser preparation of tooth surfaces for fissure sealants placement: a systematic review and meta-analysis
Yunhan Zhang, Yan Wang, Yandi Chen, Yang Chen, Qiong Zhang, Jing Zou
BMC Oral Health.2019;[Epub] CrossRef - Effect of laser preparation on adhesion of a self‐adhesive flowable composite resin to primary teeth
Mahtab Memarpour, Fereshteh Shafiei, Faranak Razmjoei, Nasrin Kianimanesh
Microscopy Research and Technique.2016; 79(4): 334. CrossRef
- Comparative Evaluation of the Retention Rates of Composite Resin Pit and Fissure Sealants Placed on Permanent Molars Treated with Air Abrasion and Acid Etching: A Systematic Review and Meta-analysis of Randomized Controlled Trials
- 2,430 View
- 14 Download
- 6 Crossref
Case Report
- Diagnostic challenges of nonodontogenic toothache
- Hyung-Ok Park, Jung-Hong Ha, Myoung-Uk Jin, Young-Kyung Kim, Sung-Kyo Kim
- Restor Dent Endod 2012;37(3):170-174. Published online August 29, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.3.170
-
Abstract
PDFPubReaderePub
The objective of this article was to present two nonodontogenic conditions that may mimic odontogenic toothache: trigeminal neuralgia and burning mouth syndrome. Two cases are presented in which one is related to the upper left second premolar and the other is related to the upper left first molar. Both showed pain when chewing. These two cases highlight the complexities involved in diagnosing nonodontogenic toothache. This article demonstrates the importance of having a thorough knowledge of both odontogenic and nonodontogenic toothache, as well as the need for careful evaluation of the nature of the pain and history, clinical and radiographic examinations.
-
Citations
Citations to this article as recorded by- Analysis of Final Diagnosis of Patients with Suspected Nonodontogenic Toothache: A Retrospective Study
Jeong Yeop Chun, Young Joo Shim
Journal of Oral Medicine and Pain.2024; 49(3): 57. CrossRef - Interactions of Acetyl-11-Keto-Beta-Boswellic Acid on Catechol-O-Methyltransferase in the Management of Masticatory Myofascial Pain Syndrome
Ramya Suresh, Pradeep Kumar Yadalam, Ramya Ramadoss, Karthikeyan Ramalingam, Arvind Muthukrishnan
Cureus.2024;[Epub] CrossRef - Assessment of Concordance between Chairside Ultrasonography and Digital Palpation in Detecting Myofascial Trigger Points in Masticatory Myofascial Pain Syndrome
Mohamed Elbarbary, Michael Goldberg, Howard C. Tenenbaum, David K. Lam, Bruce V. Freeman, David J. Pustaka, David Mock, Joseph Beyene, Amir Azarpazhooh
Journal of Endodontics.2023; 49(2): 129. CrossRef - Masticatory Myofascial Pain Syndrome: Implications for Endodontists
Mohamed Elbarbary, Ariel Oren, Michael Goldberg, Bruce V. Freeman, David Mock, Howard C. Tenenbaum, Amir Azarpazhooh
Journal of Endodontics.2022; 48(1): 55. CrossRef - PRICE 2020 guidelines for reporting case reports in Endodontics: explanation and elaboration
V. Nagendrababu, B. S. Chong, P. McCabe, P. K. Shah, E. Priya, J. Jayaraman, S. J. Pulikkotil, P. M. H. Dummer
International Endodontic Journal.2020; 53(7): 922. CrossRef - Clinical Outline of Oral Diseases
Arvind Babu Rajendra Santosh, Doryck Boyd, Kumaraswamy Kikeri Laxminarayana
Dental Clinics of North America.2020; 64(1): 1. CrossRef - Nonodontogenic Sources of Dental Pain
Scott E. Schames, Michael Jordan, Hila Robbins, Lenard Katz, Kaitlyn Tarbert
Journal of the California Dental Association.2016; 44(8): 507. CrossRef - Nonodontogenic toothaches
Edward F. Wright
The Journal of the American Dental Association.2015; 146(6): 406. CrossRef - Síndrome de boca ardiente: claves diagnósticas y terapéuticas
Eduardo Chimenos-Küstner, Cristina Arcos-Guerra, Maria Sueli Marques-Soares
Medicina Clínica.2014; 142(8): 370. CrossRef
- Analysis of Final Diagnosis of Patients with Suspected Nonodontogenic Toothache: A Retrospective Study
- 3,148 View
- 32 Download
- 9 Crossref
Basic Researchs
- Microshear bond strength of a self-etching primer adhesive to enamel according to the type of bur
- Jin-Ho Jeong, Young-Gon Cho, Myung-Seon Lee
- J Korean Acad Conserv Dent 2011;36(6):477-482. Published online November 30, 2011
- DOI: https://doi.org/10.5395/JKACD.2011.36.6.477
-
Abstract
PDFPubReaderePub
Objectives The purpose of this study was to compare the microshear bond strength (uSBS) to enamel prepared with different burs and to determine what type of bur were chosen when a self-etching primer adhesive was used.
Materials and Methods Enamel of forty-two human molars were used. They were divided into one of six groups (n = 7), Group 1, coarse (125 - 150 µm) diamond bur; Group 2, standard (106 - 125 µm) diamond bur; Group 3, fine (53 - 63 µm) diamond bur; Group 4, extrafine (20 - 30 µm) diamond bur; Group 5, plain-cut carbide bur (no. 245); Group 6, cross-cut carbide bur (no. 557). Clearfil SE Bond and Clearfil AP-X (Kuraray Medical Inc.) was bonded to enamel surface. The bonded specimens were subjected to uSBS testing.
Results The uSBS of Group 4 was the highest among groups and it was significantly higher than that of Groups 1, 2, 3, and 6 (
p < 0.05), but it was not significantly different from that of Group 5.Conclusions Different burs used on enamel surface affected the microshear bond strengths of a self-etching primer adhesive to the enamel surface. In the case of Clearfil SE Bond, extrafine diamond and plain-cut carbide bur are recommended for bonding to enamel.
-
Citations
Citations to this article as recorded by- Sixty-month follow up of three different universal adhesives used with a highly-filled flowable resin composite in the restoration of non-carious cervical lesion
Fatma Dilsad Oz, Canan Ozturk, Reza Soleimani, Sevil Gurgan
Clinical Oral Investigations.2022; 26(8): 5377. CrossRef
- Sixty-month follow up of three different universal adhesives used with a highly-filled flowable resin composite in the restoration of non-carious cervical lesion
- 1,611 View
- 5 Download
- 1 Crossref
- Effect of cutting instruments on the dentin bond strength of a self-etch adhesive
- Young-Gon Lee, So-Ra Moon, Young-Gon Cho
- J Korean Acad Conserv Dent 2010;35(1):13-19. Published online January 31, 2010
- DOI: https://doi.org/10.5395/JKACD.2010.35.1.013
-
Abstract
PDFPubReaderePub
The purpose of this study was to compare the microshear bond strength of a self-etching primer adhesive to dentin prepared with different diamond points, carbide burs and SiC papers, and also to determine which SiC paper yield similar strength to that of dentinal surface prepared with points or burs.
Fifty-six human molar were sectioned to expose the occlusal dentinal surfaces of crowns and slabs of 1.2 mm thick were made. Dentinal surfaces were removed with three diamond points, two carbide burs, and three SiC papers. They were divided into one of eight equal groups (n = 7); Group 1: standard diamond point(TF-12), Group 2: fine diamond point (TF-12F), Group 3: extrafine diamond point (TF-12EF), Group 4: plain-cut carbide bur (no. 245), Group 5: cross-cut carbide bur (no. 557), Group 6 : P 120-grade SiC paper, Group 7: P 220-grade SiC paper, Group 8: P 800-grade SiC paper.
Clearfil SE Bond was applied on dentinal surface and Clearfil AP-X was placed on dentinal surface using Tygon tubes. After the bonded specimens were subjected to uSBS testing, the mean uSBS (n = 20 for each group) was statistically compared using one-way ANOVA and Tukey HSD test.
In conclusion, the use of extrafine diamond point is recommended for improved bonding of Clearfil SE Bond to dentin. Also the use of P 220-grade SiC paper in vitro will be yield the results closer to dentinal surface prepared with fine diamond point or carbide burs
in vivo .-
Citations
Citations to this article as recorded by- Evaluation of the flexural and repair bond strengths of 3D-printed temporary restorations
Nazmi Dinçer, Şafak Külünk, Seniha Kısakürek, Ibrahim Duran
BMC Oral Health.2025;[Epub] CrossRef - Comparison of shear bond strength between various temporary prostheses resin blocks fabricated by subtractive and additive manufacturing methods bonded to self-curing reline resin
Hyo-Min Ryu, Jin-Han Lee
The Journal of Korean Academy of Prosthodontics.2023; 61(3): 189. CrossRef - The Effect of Aging and Different Surface Treatments on Temporary Cement Bonding of Temporaray Crown Materials
Sebahat FINDIK AYDINER, Nuran YANIKOĞLU, Zeynep YEŞİL DUYMUŞ
Cumhuriyet Dental Journal.2023; 26(2): 144. CrossRef - Influence of surface treatments and repair materials on the shear bond strength of CAD/CAM provisional restorations
Ki-Won Jeong, Sung-Hun Kim
The Journal of Advanced Prosthodontics.2019; 11(2): 95. CrossRef - Shear bond strength of dental CAD-CAM hybrid restorative materials repaired with composite resin
Yun-Hee Moon, Jonghyuk Lee, Myung-Gu Lee
The Journal of Korean Academy of Prosthodontics.2016; 54(3): 193. CrossRef - Microshear bond strength of a self-etching primer adhesive to enamel according to the type of bur
Jin-Ho Jeong, Young-Gon Cho, Myung-Seon Lee
Journal of Korean Academy of Conservative Dentistry.2011; 36(6): 477. CrossRef
- Evaluation of the flexural and repair bond strengths of 3D-printed temporary restorations
- 1,828 View
- 15 Download
- 6 Crossref
Original Article
- Iatrogenic chemical burn on facial skin by 37% phosphoric acid etchant
- Jong-Hyun Park, Hye-Jin Shin, Se-Hee Park, Jin-Woo Kim, Kyung-Mo Cho
- J Korean Acad Conserv Dent 2009;34(1):38-41. Published online January 31, 2009
- DOI: https://doi.org/10.5395/JKACD.2009.34.1.038
-
Abstract
PDFPubReaderePub
When we use the total-etch dentin adhesive system for composite resin restorations, gel or liquid acid etchant such as 37% phosphoric acid is commonly used. Thirty seven percentage phosphoric acid is very powerful erosive agent, and can cause severe harmful effects when it contacts with an oral mucosa and facial skin.
This case describes iatrogenic chemical burn on facial skin caused by phosphoric acid which was happened during composite resin restorative procedure.
Chemical burn by acid etchant can be evoked by careless handling of remnant and syringe. In order to prevent these iatrogenic injuries, we should check the complete removal of the etching agent both in intra and extra-oral environments after etching and rinsing procedure and it is necessary to use of the rubber dam or isolation instruments.
If accidental burn were occurred, immediate wash with copious water. And bring the patient to the dermatologist as soon as possible.
-
Citations
Citations to this article as recorded by- Cytotoxicity of V-Prep Versus Phosphoric Acid Etchant on Oral Gingival Fibroblasts
Victor Ghoubril, Sylvie Changotade, Didier Lutomski, Joseph Ghoubril, Carole Chakar, Maher Abboud, Louis Hardan, Naji Kharouf, Elie Khoury
Journal of Functional Biomaterials.2022; 13(4): 266. CrossRef - Effects of dental acid etchants in oral epithelial cells
Do-kyeong Kim, Jae-won Kwak, Ryeong-mi Jo, Da-som Jung, Da-young Youn, Na-yeon Oh, Ji-hye Jang
Oral Biology Research.2019; 43(4): 299. CrossRef
- Cytotoxicity of V-Prep Versus Phosphoric Acid Etchant on Oral Gingival Fibroblasts
- 5,880 View
- 83 Download
- 2 Crossref
 First
First Prev
Prev

