
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 38(4); 2013 > Article
- Case Report Conservative approach of a symptomatic carious immature permanent tooth using a tricalcium silicate cement (Biodentine): a case report
- Cyril Villat1, Brigitte Grosgogeat2, Dominique Seux3, Pierre Farge3
-
2013;38(4):-262.
DOI: https://doi.org/10.5395/rde.2013.38.4.258
Published online: November 12, 2013
1Laboratoire des Multimatériaux et Interfaces, UMR CNRS 5615, Department of Conservative Dentistry and Endodontics, Faculté d'Odontologie, Université de Lyon, Hospices Civils de Lyon, Lyon, France.
2Laboratoire des Multimatériaux et Interfaces, UMR CNRS 5615, Department of Biomaterials, Faculté d'Odontologie, Université de Lyon, Hospices Civils de Lyon, Lyon, France.
3Department of Conservative Dentistry and Endodontics, Faculté d'Odontologie, Université de Lyon, Hospices Civils de Lyon, France.
- Correspondence to: Cyril Villat, DDS, PhD. Associate Professor, Department of Conservative Dentistry and Endodontics, Université Lyon 1, Faculté d'Odontologie, 11 rue Guillaume Paradin 69365 Lyon Cedex 08 France. TEL, +33(0)4 78 77 86 89; FAX, +33(0)4 78 77 87 12; cyril.villat@univlyon1.fr
• Received: July 19, 2013 • Revised: September 15, 2013 • Accepted: September 25, 2013
©Copyights 2013. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 254 Views
- 1 Download
- 26 Crossref
Abstract
- The restorative management of deep carious lesions and the preservation of pulp vitality of immature teeth present real challenges for dental practitioners. New tricalcium silicate cements are of interest in the treatment of such cases. This case describes the immediate management and the follow-up of an extensive carious lesion on an immature second right mandibular premolar. Following anesthesia and rubber dam isolation, the carious lesion was removed and a partial pulpotomy was performed. After obtaining hemostasis, the exposed pulp was covered with a tricalcium silicate cement (Biodentine, Septodont) and a glass ionomer cement (Fuji IX extra, GC Corp.) restoration was placed over the tricalcium silicate cement. A review appointment was arranged after seven days, where the tooth was asymptomatic with the patient reporting no pain during the intervening period. At both 3 and 6 mon follow up, it was noted that the tooth was vital, with normal responses to thermal tests. Radiographic examination of the tooth indicated dentin-bridge formation in the pulp chamber and the continuous root formation. This case report demonstrates a fast tissue response both at the pulpal and root dentin level. The use of tricalcium silicate cement should be considered as a conservative intervention in the treatment of symptomatic immature teeth.
Introduction
Preserving dental pulp vitality is a significant clinical challenge in restorative dentistry, especially with regard to the management of permanent immature teeth.1 According to the consensus report of the European Society of Endodontology, when the pulp of a tooth with incomplete root formation is exposed, the therapeutic procedure should preserve the vitality of the remaining part of the pulp.2 After removing the damaged pulpal tissue, it is recommended that materials that protect the underlying healthy pulpal tissues should be used to allow and promote healing and repair.2 Indicators for successful management are a normal response to pulp sensitivity tests and the absence of pain, the radiological evidence of a dentin-bridge formation, and the continuing root formation in immature teeth. In addition, there should be no evidence of clinical or radiographic signs of internal root resorption or apical periodontitis.2
Calcium hydroxide is described as the material of choice for direct pulp capping and partial or coronal pulpotomy.3 However, recent clinical studies question the predictability of the results with calcium hydroxide. In addition, the use of calcium hydroxide has been shown to be time-consuming with iterative clinical applications of the medication often required.4 Mineral Trioxide Aggregate (MTA), a tricalcium silicate cement arising from the Portland cement, was developed in the mid 1990's, initially for endodontic treatment procedures (root perforation and surgical endodontics). This material was shown to have good physico-chemical and biological properties and secondary properties preventing bacterial leakage, which are better than other current restorative materials.5-10 MTA also demonstrated additional dentin mineralization properties when used as a pulp capping agent.8,10,11 However, its handling properties remain relatively poor compared to that of calcium hydroxide.11,12
In 2009, a synthetic tricalcium silicate cement (Biodentine, Septodont, Saint Maur-des-Fossées, France) became commercially available. This new tricalcium silicate cement has high mechanical properties for restorative dentistry and appears to induce an early dental pulp mineralization.13-15
In vitro studies have demonstrated ionic uptake and infiltration of minerals at the dentinmaterial interface, which is associated with a porous internal hydrogel formation allowing for ion exchange.16-18 Although Biodentine was initially developed for endodontic applications, preliminary results with Biodentine demonstrated a successful and quick positive outcome with respect to direct pulp capping. Tricalcium silicate cements could be indicated as restorative materials for direct pulp capping with regard to their dentin-mineralizing properties.19 Indeed, the chemical setting reaction of the two main components (tricalcium silicate = Ca3SiO5 and dicalcium silicate = Ca2SiO4) of these cements leads to the release of calcium hydroxide.20
In this case report, the authors report on a clinical case where a tricalcium silicate cement (Biodentine) was used as a pulpotomy agent in the treatment of a pulpitis in permanent immature premolar.
Case report
A 12 year-old girl presented at the emergency dental clinic, Hospices Civils de Lyon, Lyon, France, for an acute, spontaneous and lasting referred pain in the right posterior mandibular quadrant. Clinical and radiographic examinations revealed extensive occlusal caries invading the pulp on the second right lower premolar, an immature permanent tooth with incomplete root formation (Figure 1a). The diagnosis was acute pulpitis (#45).
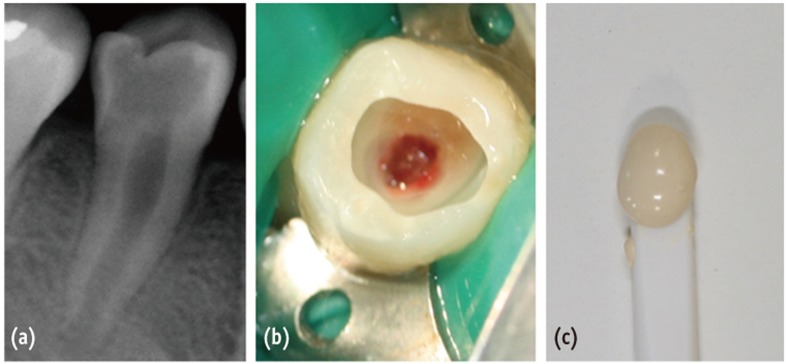 Figure 1
Figure 1 
Figure 1 (a) Preoperative radiograph of tooth #45 demonstrating an extensive occlusal caries close to the pulp chamber and incomplete root maturation; (b) Clinical view following caries removal and partial pulpotomy; (c) Color and texture of Biodentine before application.
Download Figure After taking the informed consent of her parents due to the young age of the patient, a conservative pulpal treatment option was adopted in order to allow for further root formation and to preserve the growing potential of the root and the healing potential of the pulp. Accordingly, #45 was anesthetized by a peri-apical injection with 1.5 mL of a 2% articaine and 1/200,000 epinephrine solution (Primacaine Adrenaline 1/200,000, Acteon Pierre Rolland, Merignac, France) and isolated under rubber-dam.
Following caries removal, a partial pulpotomy was performed using a round low-speed carbide bur (H1.204.021, Komet France, Paris, France) under constant irrigation until a normal bleeding was obtained (Figure 1b). The hemostasis was obtained by irrigation with saline solution and application of sterile cotton pellets. Biodentine was processed according to the manufacturer's instruction by mixing a single-unit powder part (tricalcium silicate-dicalcium silicate-zircon dioxide) and 5 drops of a single-unit liquid part (calcium chloride-distilled water) for 30 seconds (Figure 1c). Figure 2a displays the immediate post treatment X-ray which shows the pulp capping material located at the roof of the pulp chamber. Direct pulp capping was performed with a 2 mm-thickness layer of the tricalcium silicate cement (Biodentine). The tooth #45 was restored with conventional glass ionomer cement (Fuji IX extra, GC Corp., Tokyo, Japan) and checked for centric occlusion. At a postoperative phone call the following day, the patient reported complete cessation of the painful episode within 12 hours after completion of the treatment. At seven day follow-up, a clinical examination found responses to thermal pulpal tests within normal limits for a non-inflammatory pulp (hot and cold were discriminated and the response did not exceed the stimulus duration). At a three months recall, a clinical examination showed a normal pulpal sensitivity. There were no clinical or radiographic signs of root resorption or apical periodontitis. A radiograph showed morpho-differentiation of a dentin bridge immediately under the tricalcium silicate cement. (Figures 2b and 2c). Root formation had occurred and a thickening of the root dentin walls was noted. At 6 month recall, the bevel-shaped ends of the dentin at 3 months appeared to change to thicker round-shaped root-dentin walls.
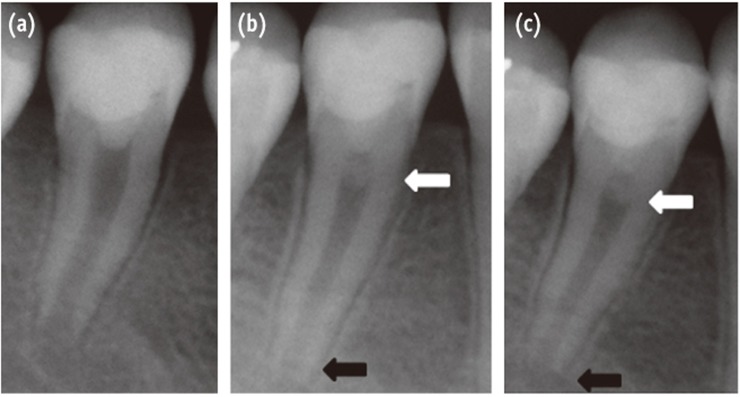 Figure 2
Figure 2
Figure 2 (a) Immediate post-operative radiograph following silicate cement (Biodentine) placement and glass ionomer cement (Fuji IX) restoration; (b) Three months follow-up radiograph: formation of pulpal roof dentin bridge (white arrow) and root edification (black arrow); (c) Six months follow-up radiograph.
Download Figure Discussion
Studies have shown that the partial pulpotomy technique obtains good clinical outcomes independent of the material used. However, the main discriminative factor between materials is the speed and quality of the dentin bridge formation.21,22 The literature cites calcium hydroxide as the gold standard for pulp capping. It is acknowledged to have many biological properties including antibacterial, antifungal and dentinogenetic effects. However, its high solubility leads to leakage and requires an additional high quality coronal sealing. Although calcium hydroxide allows for the formation of a dentin bridge, studies have shown that the resulting dentin contains tunnels, which could favour infection or necrosis of the pulp.3 In addition, the resulting root dentin is weaker than the original tissue and a higher occurrence of late root canal fracture has been reported.23
In order to overcome these deficits, researchers have looked to develop new materials with a higher sealing ability and enhanced biological properties, with one example being hard-setting calcium hydroxide. More recent developments belonging to the family of tricalcium silicate cements have seen improved biological and clinical effects. ProRoot MTA (Dentsply, Johnson City, TN, USA) was the first of a new generation biomaterials to be commercially available.
At the present time, this category of dental materials can be divided into two main groups:
- Portland-derived cements like ProRoot MTA, MTA Angelus (Angelus Soluções Odontológicas, Londrina, Brazil) or MMMTA (MicroMega, Besançon, France)
- Synthetic tricalcium silicate cements which result in an industrial mixing of tricalcium silicate and dicalcium silicate clusters like Biodentine.
The clinical interest of tricalcium silicate cements has been reported both in endodontic and restorative treatment.4,6,8,11,21,24-28 Among the tricalcium silicate cements, Biodentine has a short setting time, good mechanical properties and an effective sealing capacity (to mineralized tissues), which enables its use as a direct pulp capping and restorative material.13,17
Some authors have suggested that the favorable biological properties of tricalcium silicate cements make them valuable for preserving the vitality of the pulp in immature permanent teeth with irreversible pulpitis.19,29 Such a conservative approach using tricalcium silicate cements, as opposed to pulpectomy and root canal therapy or apexification with a standard therapy, would allow for the growth in length and thickness of the root-walls.23 Moreover, in vitro and in vivo studies have shown that the dentin bridge formation is more homogeneous and root dentin formation occurs earlier with tricalcium silicate than with calcium hydroxide based materials.4,11,22,24,28-31 These features (increased speed and quality of dentin bridge formation and root dentin formation) were observed in our case report and support the conservative approach adopted to treating this case of an irreversible pulpitis.
Conclusions
Biodentine tricalcium silicate cement appears to offer a valuable alternative therapeutic intervention to maintain pulp vitality for immature permanent teeth. Moreover, its handling and mechanical properties, as well as its short setting time allow for its clinical use as a conventional dentine substitute. It will be important to conduct more clinical studies to validate these observations. Conservative techniques that improve treatment outcomes in immature permanent teeth with inflammatory and infectious pulpal diseases should be encouraged.
Figure 1
(a) Preoperative radiograph of tooth #45 demonstrating an extensive occlusal caries close to the pulp chamber and incomplete root maturation; (b) Clinical view following caries removal and partial pulpotomy; (c) Color and texture of Biodentine before application.
Figure 2
(a) Immediate post-operative radiograph following silicate cement (Biodentine) placement and glass ionomer cement (Fuji IX) restoration; (b) Three months follow-up radiograph: formation of pulpal roof dentin bridge (white arrow) and root edification (black arrow); (c) Six months follow-up radiograph.
- 1. Witherspoon DE, Small JC, Harris GZ. Mineral trioxide aggregate pulpotomies: a case series outcomes assessment. J Am Dent Assoc 2006;137:610-618.PubMed
- 2. European Society of Endodontology. Quality guidelines for endodontic treatments: consensus report of the European Society of Endodontology. Int Endod J 2006;39:921-930.PubMed
- 3. Mohammadi Z, Dummer PM. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int Endod J 2011;44:697-730.ArticlePubMed
- 4. Nair PN, Duncan HF, Pitt Ford TR, Luder HU. Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: a randomized controlled trial. Int Endod J 2008;41:128-150.ArticlePubMed
- 5. Camilleri J, Pitt Ford TR. Mineral trioxide aggregate: a review of the constituents and biological properties of the material. Int Endod J 2006;39:747-754.ArticlePubMed
- 6. Yun YR, Yang IS, Hwang YC, Hwang IN, Choi HR, Yoon SJ, Kim SH, Oh WM. Pulp response of mineral trioxide aggregate, calcium sulfate or calcium hydrate. J Korean Acad Conserv Dent 2007;32:95-101.
- 7. Chang SW, Yoo HM, Park DS, Oh TS, Bae KS. Ingredients and cytotoxicity of MTA and 3 kinds of Protland cements. J Korean Acad Conserv Dent 2008;33:369-376.Article
- 8. Roberts HW, Toth JM, Berzins DW, Charlton DG. Mineral trioxide aggregate material use in endodontic treatment: a review of the literature. Dent Mater 2008;24:149-164.ArticlePubMed
- 9. Torabinejad M, Parirokh M. Mineral trioxide aggregate: a comprehensive literature review-part II: leakage and biocompatibility investigations. J Endod 2010;36:190-202.ArticlePubMed
- 10. Chang SW. Chemical characteristics of mineral trioxide aggregate and its hydration reaction. Restor Dent Endod 2012;37:188-193.ArticlePubMedPMC
- 11. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review-part III: clinical applications, drawbacks and mechanism of action. J Endod 2010;36:400-413.ArticlePubMed
- 12. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review-part I: chemical, physical, and antibacterial properties. J Endod 2010;36:16-27.ArticlePubMed
- 13. Koubi G, Colon P, Franquin JC, Hartmann A, Richard G, Faure MO, Lambert G. Clinical evaluation of the performance and safety of a new dentine substitute, Biodentine, in the restoration of posterior teeth-a prospective study. Clin Oral Investig 2013;17:243-249.ArticlePubMed
- 14. Darvell BW, WU RC. 'MTA'-an hydraulic silicate cement: review update and setting reaction. Dent Mater 2011;27:407-422.ArticlePubMed
- 15. Laurent P, Camps J, About I. Biodentine induces TGF-β 1 release from human pulp cells and early dental pulp mineralization. Int Endod J 2012;45:439-448.PubMed
- 16. Han L, Okiji T. Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J 2011;44:1081-1087.ArticlePubMed
- 17. Villat C, Tran XV, Pradelle-Plasse N, Ponthiaux P, Wenger F, Grosgogeat B, Colon P. Impedance methodology. A new way to characterize the setting reaction of dental cements. Dent Mater 2010;26:1127-1132.ArticlePubMed
- 18. Atmeh AR, Chong EZ, Richard G, Festy F, Watson TF. Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. J Dent Res 2012;91:454-459.ArticlePubMedPMCPDF
- 19. Eghbal MJ, Asgary S, Baglue RA, Parirokh M, Ghoddusi J. MTA pulpotomy of human permanent molars with irreversible pulpitis. Aust Endod J 2009;35:4-8.ArticlePubMed
- 20. Camilleri J. Characterization and hydration kinetics of tricalcium silicate cement use as a dental biomaterial. Dent Mater 2011;27:836-844.PubMed
- 21. Accorinte Mde L, Holland R, Reis A, Bortoluzzi MC, Murata SS, Dezan E Jr, Souza V, Alessandro LD. Evaluation of mineral trioxide aggregate and calcium hydroxide cement as pulp-capping agents in human teeth. J Endod 2008;34:1-6.ArticlePubMed
- 22. Leye Benoist F, Gaye Ndiaye F, Kane AW, Benoist HM, Farge P. Evaluation of mineral trioxide aggregate (MTA) versus calcium hydroxide cement (Dycal) in the formation of a dentine bridge: a randomized controlled trial. Int Dent J 2012;62:33-39.PubMed
- 23. Huang GT. Apexification: the beginning of its end. Int Endod J 2009;42:855-866.ArticlePubMed
- 24. Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: a preliminary report. Int Endod J 2003;36:225-231.ArticlePubMedPDF
- 25. Iwamoto CE, Adachi E, Pameijer CH, Barnes D, Romberg EE, Jefferies S. Clinical and histological evaluation of white ProRoot MTA in direct pulp capping. Am J Dent 2006;19:85-90.PubMed
- 26. Witherspoon DE. Vital pulp therapy with new materials: new directions and treatment perspectives-permanent teeth. Pediatr Dent 2008;30:220-224.ArticlePubMed
- 27. Accorinte ML, Loguercio AD, Reis A, Bauer JR, Grande RH, Murata SS, Souza V, Holland R. Evaluation of two mineral trioxide aggregate compounds as pulp-capping agents in human teeth. Int Endod J 2009;42:122-128.ArticlePubMed
- 28. Bakland LK, Andreasen JO. Will mineral trioxide aggregate replace calcium hydroxide in treating pulpal and periodontal healing complications subsequent to dental trauma? A review. Dent Traumatol 2012;28:25-32.ArticlePubMed
- 29. Asgary S, Eghbal MJ, Ghoddusi J, Yazdani S. One-year of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter, randomized, noinferiority clinical trial. Clin Oral Investig 2013;17:431-439.PubMed
- 30. El-Meligy OA, Avery DR. Comparison of mineral trioxide aggregate and calcium hydroxide as pulpotomy agents in young permanent teeth (apexogenesis). Pediatr Dent 2006;28:399-404.PubMed
- 31. Tran XV, Gorin C, Willig C, Baroukh B, Pellat B, Decup F, Opsahl Vital S, Chaussain C, Boukpessi T. Effect of a calcium-silicate-based restorative cement on pulp repair. J Dent Res 2012;91:1166-1171.ArticlePubMedPDF
REFERENCES
Tables & Figures
Figure 1 (a) Preoperative radiograph of tooth #45 demonstrating an extensive occlusal caries close to the pulp chamber and incomplete root maturation; (b) Clinical view following caries removal and partial pulpotomy; (c) Color and texture of Biodentine before application.
Download Figure
Figure 2 (a) Immediate post-operative radiograph following silicate cement (Biodentine) placement and glass ionomer cement (Fuji IX) restoration; (b) Three months follow-up radiograph: formation of pulpal roof dentin bridge (white arrow) and root edification (black arrow); (c) Six months follow-up radiograph.
Download Figure
Figure 1
(a) Preoperative radiograph of tooth #45 demonstrating an extensive occlusal caries close to the pulp chamber and incomplete root maturation; (b) Clinical view following caries removal and partial pulpotomy; (c) Color and texture of Biodentine before application.
Figure 2
(a) Immediate post-operative radiograph following silicate cement (Biodentine) placement and glass ionomer cement (Fuji IX) restoration; (b) Three months follow-up radiograph: formation of pulpal roof dentin bridge (white arrow) and root edification (black arrow); (c) Six months follow-up radiograph.
REFERENCES
- 1. Witherspoon DE, Small JC, Harris GZ. Mineral trioxide aggregate pulpotomies: a case series outcomes assessment. J Am Dent Assoc 2006;137:610-618.PubMed
- 2. European Society of Endodontology. Quality guidelines for endodontic treatments: consensus report of the European Society of Endodontology. Int Endod J 2006;39:921-930.PubMed
- 3. Mohammadi Z, Dummer PM. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int Endod J 2011;44:697-730.ArticlePubMed
- 4. Nair PN, Duncan HF, Pitt Ford TR, Luder HU. Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: a randomized controlled trial. Int Endod J 2008;41:128-150.ArticlePubMed
- 5. Camilleri J, Pitt Ford TR. Mineral trioxide aggregate: a review of the constituents and biological properties of the material. Int Endod J 2006;39:747-754.ArticlePubMed
- 6. Yun YR, Yang IS, Hwang YC, Hwang IN, Choi HR, Yoon SJ, Kim SH, Oh WM. Pulp response of mineral trioxide aggregate, calcium sulfate or calcium hydrate. J Korean Acad Conserv Dent 2007;32:95-101.
- 7. Chang SW, Yoo HM, Park DS, Oh TS, Bae KS. Ingredients and cytotoxicity of MTA and 3 kinds of Protland cements. J Korean Acad Conserv Dent 2008;33:369-376.Article
- 8. Roberts HW, Toth JM, Berzins DW, Charlton DG. Mineral trioxide aggregate material use in endodontic treatment: a review of the literature. Dent Mater 2008;24:149-164.ArticlePubMed
- 9. Torabinejad M, Parirokh M. Mineral trioxide aggregate: a comprehensive literature review-part II: leakage and biocompatibility investigations. J Endod 2010;36:190-202.ArticlePubMed
- 10. Chang SW. Chemical characteristics of mineral trioxide aggregate and its hydration reaction. Restor Dent Endod 2012;37:188-193.ArticlePubMedPMC
- 11. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review-part III: clinical applications, drawbacks and mechanism of action. J Endod 2010;36:400-413.ArticlePubMed
- 12. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review-part I: chemical, physical, and antibacterial properties. J Endod 2010;36:16-27.ArticlePubMed
- 13. Koubi G, Colon P, Franquin JC, Hartmann A, Richard G, Faure MO, Lambert G. Clinical evaluation of the performance and safety of a new dentine substitute, Biodentine, in the restoration of posterior teeth-a prospective study. Clin Oral Investig 2013;17:243-249.ArticlePubMed
- 14. Darvell BW, WU RC. 'MTA'-an hydraulic silicate cement: review update and setting reaction. Dent Mater 2011;27:407-422.ArticlePubMed
- 15. Laurent P, Camps J, About I. Biodentine induces TGF-β 1 release from human pulp cells and early dental pulp mineralization. Int Endod J 2012;45:439-448.PubMed
- 16. Han L, Okiji T. Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J 2011;44:1081-1087.ArticlePubMed
- 17. Villat C, Tran XV, Pradelle-Plasse N, Ponthiaux P, Wenger F, Grosgogeat B, Colon P. Impedance methodology. A new way to characterize the setting reaction of dental cements. Dent Mater 2010;26:1127-1132.ArticlePubMed
- 18. Atmeh AR, Chong EZ, Richard G, Festy F, Watson TF. Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. J Dent Res 2012;91:454-459.ArticlePubMedPMCPDF
- 19. Eghbal MJ, Asgary S, Baglue RA, Parirokh M, Ghoddusi J. MTA pulpotomy of human permanent molars with irreversible pulpitis. Aust Endod J 2009;35:4-8.ArticlePubMed
- 20. Camilleri J. Characterization and hydration kinetics of tricalcium silicate cement use as a dental biomaterial. Dent Mater 2011;27:836-844.PubMed
- 21. Accorinte Mde L, Holland R, Reis A, Bortoluzzi MC, Murata SS, Dezan E Jr, Souza V, Alessandro LD. Evaluation of mineral trioxide aggregate and calcium hydroxide cement as pulp-capping agents in human teeth. J Endod 2008;34:1-6.ArticlePubMed
- 22. Leye Benoist F, Gaye Ndiaye F, Kane AW, Benoist HM, Farge P. Evaluation of mineral trioxide aggregate (MTA) versus calcium hydroxide cement (Dycal) in the formation of a dentine bridge: a randomized controlled trial. Int Dent J 2012;62:33-39.PubMed
- 23. Huang GT. Apexification: the beginning of its end. Int Endod J 2009;42:855-866.ArticlePubMed
- 24. Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: a preliminary report. Int Endod J 2003;36:225-231.ArticlePubMedPDF
- 25. Iwamoto CE, Adachi E, Pameijer CH, Barnes D, Romberg EE, Jefferies S. Clinical and histological evaluation of white ProRoot MTA in direct pulp capping. Am J Dent 2006;19:85-90.PubMed
- 26. Witherspoon DE. Vital pulp therapy with new materials: new directions and treatment perspectives-permanent teeth. Pediatr Dent 2008;30:220-224.ArticlePubMed
- 27. Accorinte ML, Loguercio AD, Reis A, Bauer JR, Grande RH, Murata SS, Souza V, Holland R. Evaluation of two mineral trioxide aggregate compounds as pulp-capping agents in human teeth. Int Endod J 2009;42:122-128.ArticlePubMed
- 28. Bakland LK, Andreasen JO. Will mineral trioxide aggregate replace calcium hydroxide in treating pulpal and periodontal healing complications subsequent to dental trauma? A review. Dent Traumatol 2012;28:25-32.ArticlePubMed
- 29. Asgary S, Eghbal MJ, Ghoddusi J, Yazdani S. One-year of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter, randomized, noinferiority clinical trial. Clin Oral Investig 2013;17:431-439.PubMed
- 30. El-Meligy OA, Avery DR. Comparison of mineral trioxide aggregate and calcium hydroxide as pulpotomy agents in young permanent teeth (apexogenesis). Pediatr Dent 2006;28:399-404.PubMed
- 31. Tran XV, Gorin C, Willig C, Baroukh B, Pellat B, Decup F, Opsahl Vital S, Chaussain C, Boukpessi T. Effect of a calcium-silicate-based restorative cement on pulp repair. J Dent Res 2012;91:1166-1171.ArticlePubMedPDF
Citations
Citations to this article as recorded by 
- How Does Ethylenediaminetetraacetic Acid Irrigation Affect Biodentine? A Multimethod Ex Vivo Study
Katarzyna Dąbrowska, Aleksandra Palatyńska-Ulatowska, Leszek Klimek
Materials.2024; 17(6): 1230. CrossRef - Evaluation of Biodentine Tricalcium Silicate-Based Cement after Chlorhexidine Irrigation
Katarzyna Dąbrowska, Aleksandra Palatyńska-Ulatowska, Leszek Klimek
Applied Sciences.2024; 14(19): 8702. CrossRef - Evaluation of the chemical, physical, and biological properties of a newly developed bioceramic cement derived from cockle shells: an in vitro study
Monthip Wannakajeepiboon, Chankhrit Sathorn, Chatvadee Kornsuthisopon, Busayarat Santiwong, Thanakorn Wasanapiarnpong, Pairoj Linsuwanont
BMC Oral Health.2023;[Epub] CrossRef - Protección pulpar directa y posterior apexogénesis. Informe de un caso clínico / Direct pulp capping followed by apexogenesis. A clinical case report
Osvaldo Zmener, Ana C. Boetto
Revista de la Asociación Odontológica Argentina.2022;[Epub] CrossRef - The Effect of Irrigation with Citric Acid on Biodentine Tricalcium Silicate-Based Cement: SEM-EDS In Vitro Study
Katarzyna Dąbrowska, Aleksandra Palatyńska-Ulatowska, Leszek Klimek
Materials.2022; 15(10): 3467. CrossRef - The Immunomodulatory and Regenerative Effect of Biodentine™ on Human THP‐1 Cells and Dental Pulp Stem Cells: In Vitro Study
Duaa Abuarqoub, Nazneen Aslam, Rand Zaza, Hanan Jafar, Suzan Zalloum, Renata Atoom, Walhan Alshaer, Mairvat Al-Mrahleh, Abdalla Awidi, Bruna Sinjari
BioMed Research International.2022;[Epub] CrossRef - Biodentine: Material of choice for apexification
Himanshu Aeran, Mahema Sharma, Avantika Tuli
International Journal of Oral Health Dentistry.2021; 7(1): 54. CrossRef - Minimal Intervention in Dentistry: A Literature Review on Biodentine as a Bioactive Pulp Capping Material
Naji Ziad Arandi, Mohammad Thabet, Mona Abbassy
BioMed Research International.2021;[Epub] CrossRef - Biodentine Pulpotomies on Permanent Traumatized Teeth with Complicated Crown Fractures
Léa Haikal, Beatriz Ferraz dos Santos, Duy-Dat Vu, Marina Braniste, Basma Dabbagh
Journal of Endodontics.2020; 46(9): 1204. CrossRef - Influence of sodium hypochlorite and ultrasounds on surface features and chemical composition of Biodentine tricalcium silicate-based material
Aleksandra PALATYŃSKA-ULATOWSKA, Katarzyna BUŁA, Leszek KLIMEK
Dental Materials Journal.2020; 39(4): 587. CrossRef - Effects of two fast-setting pulp-capping materials on cell viability and osteogenic differentiation in human dental pulp stem cells: An in vitro study
Yan Sun, Jun Liu, Tao Luo, Ya Shen, Ling Zou
Archives of Oral Biology.2019; 100: 100. CrossRef - Healing Capacity of Autologous Bone Marrow–derived Mesenchymal Stem Cells on Partially Pulpotomized Dogs' Teeth
Mona H. El-Zekrid, Salah H. Mahmoud, Fawzy A. Ali, Mohamed E. Helal, Mohammed E. Grawish
Journal of Endodontics.2019; 45(3): 287. CrossRef - Large Periapical or Cystic Lesions in Association with Roots Having Open Apices Managed Nonsurgically Using 1-step Apexification Based on Platelet-rich Fibrin Matrix and Biodentine Apical Barrier: A Case Series
Sarang Sharma, Vivek Sharma, Deepak Passi, Dhirendra Srivastava, Shibani Grover, Shubha Ranjan Dutta
Journal of Endodontics.2018; 44(1): 179. CrossRef - Microleakage and Shear Bond Strength of Biodentine at Different Setting Time
Yong Ho Song, Nanyoung Lee, Sangho Lee, Myeongkwan Jih
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2018; 45(3): 344. CrossRef - Biodentine™ material characteristics and clinical applications: a 3 year literature review and update
S. Rajasekharan, L. C. Martens, R. G. E. C. Cauwels, R. P. Anthonappa
European Archives of Paediatric Dentistry.2018; 19(1): 1. CrossRef - Case Report: Immediate pain relief after partial pulpotomy of cariously exposed young permanent molar using mineral trioxide aggregate and root maturation, with two years follow-up
Passant Nagi, Nevine Waly, Adel Elbardissy, Mohammed Khalifa
F1000Research.2018; 7: 1616. CrossRef - Factors affecting the outcomes of direct pulp capping using Biodentine
Mariusz Lipski, Alicja Nowicka, Katarzyna Kot, Lidia Postek-Stefańska, Iwona Wysoczańska-Jankowicz, Lech Borkowski, Paweł Andersz, Anna Jarząbek, Katarzyna Grocholewicz, Ewa Sobolewska, Krzysztof Woźniak, Agnieszka Droździk
Clinical Oral Investigations.2018; 22(5): 2021. CrossRef - Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part I: vital pulp therapy
M. Parirokh, M. Torabinejad, P. M. H. Dummer
International Endodontic Journal.2018; 51(2): 177. CrossRef - Effect of iRoot Fast Set root repair material on the proliferation, migration and differentiation of human dental pulp stem cells in vitro
Yan Sun, Tao Luo, Ya Shen, Markus Haapasalo, Ling Zou, Jun Liu, Gianpaolo Papaccio
PLOS ONE.2017; 12(10): e0186848. CrossRef - Dislodgement resistance of calcium silicate‐based materials from root canals with varying thickness of dentine
Ö. İ. Ulusoy, Y. N. Paltun, N. Güven, B. Çelik
International Endodontic Journal.2016; 49(12): 1188. CrossRef - Expression of Mineralization Markers during Pulp Response to Biodentine and Mineral Trioxide Aggregate
Mariana O. Daltoé, Francisco Wanderley G. Paula-Silva, Lúcia H. Faccioli, Patrícia M. Gatón-Hernández, Andiara De Rossi, Léa Assed Bezerra Silva
Journal of Endodontics.2016; 42(4): 596. CrossRef - Biodentine Reduces Tumor Necrosis Factor Alpha–induced TRPA1 Expression in Odontoblastlike Cells
Ikhlas A. El Karim, Maelíosa T.C. McCrudden, Mary K. McGahon, Tim M. Curtis, Charlotte Jeanneau, Thomas Giraud, Chris R. Irwin, Gerard J. Linden, Fionnuala T. Lundy, Imad About
Journal of Endodontics.2016; 42(4): 589. CrossRef - Coronal Pulpotomy Technique Analysis as an Alternative to Pulpectomy for Preserving the Tooth Vitality, in the Context of Tissue Regeneration: A Correlated Clinical Study across 4 Adult Permanent Molars
Raji Viola Solomon, Umrana Faizuddin, Parupalli Karunakar, Grandhala Deepthi Sarvani, Sevvana Sree Soumya
Case Reports in Dentistry.2015; 2015: 1. CrossRef - A Review on Biodentine, a Contemporary Dentine Replacement and Repair Material
Özlem Malkondu, Meriç Karapinar Kazandağ, Ender Kazazoğlu
BioMed Research International.2014; 2014: 1. CrossRef - The use of platelet rich plasma in the treatment of immature tooth with periapical lesion: a case report
Günseli Güven Polat, Ceren Yıldırım, Özlem Martı Akgün, Ceyhan Altun, Didem Dinçer, Cansel Köse Özkan
Restorative Dentistry & Endodontics.2014; 39(3): 230. CrossRef - Biodentine-a novel dentinal substitute for single visit apexification
Gurudutt Nayak, Mohammad Faiz Hasan
Restorative Dentistry & Endodontics.2014; 39(2): 120. CrossRef
 ePub Link
ePub Link Cite
CiteConservative approach of a symptomatic carious immature permanent tooth using a tricalcium silicate cement (Biodentine): a case report
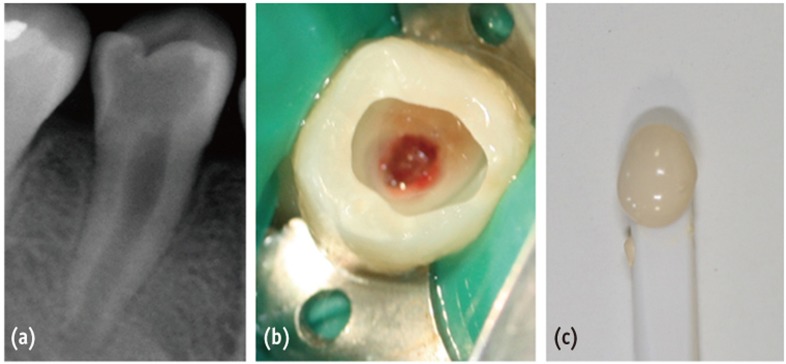
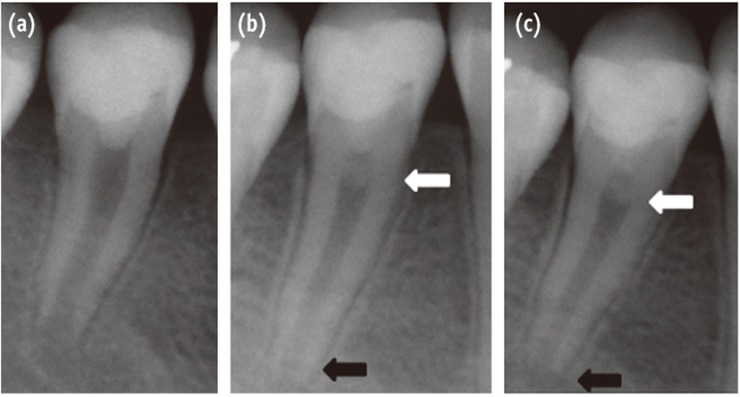
Figure 1 (a) Preoperative radiograph of tooth #45 demonstrating an extensive occlusal caries close to the pulp chamber and incomplete root maturation; (b) Clinical view following caries removal and partial pulpotomy; (c) Color and texture of Biodentine before application.
Figure 2 (a) Immediate post-operative radiograph following silicate cement (Biodentine) placement and glass ionomer cement (Fuji IX) restoration; (b) Three months follow-up radiograph: formation of pulpal roof dentin bridge (white arrow) and root edification (black arrow); (c) Six months follow-up radiograph.
Figure 1
Figure 2
Conservative approach of a symptomatic carious immature permanent tooth using a tricalcium silicate cement (Biodentine): a case report

