
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(3); 2021 > Article
- Research Article Which factors related to apical radiolucency may influence its radiographic detection? A study using CBCT as reference standard
-
Rocharles Cavalcante Fontenele1
 , Eduarda Helena Leandro Nascimento2, Hugo Gaêta-Araujo3, Laís Oliveira de Araujo Cardelli1, Deborah Queiroz Freitas1
, Eduarda Helena Leandro Nascimento2, Hugo Gaêta-Araujo3, Laís Oliveira de Araujo Cardelli1, Deborah Queiroz Freitas1 -
Restor Dent Endod 2021;46(3):e43.
DOI: https://doi.org/10.5395/rde.2021.46.e43
Published online: July 21, 2021
1Department of Oral Diagnosis, Division of Oral Radiology, Piracicaba Dental School, University of Campinas, São Paulo, Brazil.
2Department of Dentistry, Oral Radiology area, Federal University of Sergipe, Sergipe, Brazil.
3Oral Radiology section, School of Dentistry, Federal University of Alfenas, Minas Gerais, Brazil.
- Correspondence to Rocharles Cavalcante Fontenele, DDS, MSc. PhD Student, Department of Oral Diagnosis, Division of Oral Radiology, Piracicaba Dental School, University of Campinas, Av. Limeira, 901, Piracicaba, São Paulo 13414-903, Brazil. rocharlesf@gmail.com
• Received: October 26, 2020 • Revised: January 6, 2021 • Accepted: February 2, 2021
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to evaluate the detection rate of apical radiolucencies in 2-dimensional images using cone-beam computed tomography (CBCT) as the reference standard, and to determine which factors related to the apical radiolucencies and the teeth could influence its detection.
-
Materials and Methods The sample consisted of exams of patients who had panoramic (PAN) and/or periapical (PERI) radiography and CBCT. The exams were assessed by 2 oral radiologists and divided into PAN+CBCT (227 teeth–285 roots) and PERI+CBCT (94 teeth–115 roots). Radiographic images were evaluated for the presence of apical radiolucency, while CBCT images were assessed for presence, size, location, and involvement of the cortical bone (thinning, expansion, and destruction). Diagnostic values were obtained for PERI and PAN.
-
Results PERI and PAN presented high accuracy (0.83 and 0.77, respectively) and specificity (0.89 and 0.91, respectively), but low sensitivity, especially for PAN (0.40 vs. 0.65 of PERI). The size of the apical radiolucency was positively correlated with its detection in PERI and PAN (p < 0.001). For PAN, apical radiolucencies were 3.93 times more frequently detected when related to single-rooted teeth (p = 0.038). The other factors did not influence apical radiolucency detection (p > 0.05).
-
Conclusions PERI presents slightly better accuracy than PAN for the detection of apical radiolucency. The size is the only factor related to radiolucency that influences its detection, for both radiographic exams. For PAN, apical radiolucency is most often detected in single-rooted teeth.
INTRODUCTION
Periapical (PERI) and panoramic radiographs (PAN) are routinely indicated by professionals as an initial imaging method for the endodontic diagnosis of apical radiolucency (AR), as these modalities can provide information on the progression, regression and/or persistence of periapical bone changes resulting from pulp inflammatory processes [1]. However, the superposition of anatomical structures is an inherent factor of 2-dimensional (2D) examinations that may impair the detection of AR [2].
Three-dimensional (3D) examination, especially cone-beam computed tomography (CBCT), is an important tool in endodontic diagnosis since it provides high-quality images and allows periapical tissue evaluation without superposition of structures [3]. Despite the advantages of radiographic images, as the use of lower radiation dose and lower cost, previous studies have shown that CBCT images are superior in the detection of periapical lesions [1,4,5,6,7]. In addition, several factors may influence radiographic interpretation, as morphological variations, surrounding bone density, location and size of periapical lesions [2].
Previous studies suggest the use of a periapical index (PAI) as a scoring method for the radiographic assessment of apical periodontitis [2,8,9,10]. However, due to limitations in detecting AR in 2D images and the increasing use of the 3D exams in dentistry, a new periapical index based on CBCT images (CBCT-PAI) was developed [1]. This new index consists of a 6-level scoring system considering lesion size, expansion, and destruction of cortical bone. Thus, the use of the CBCT-PAI supports the reliability of epidemiological studies, mainly those that assess the prevalence and severity of periapical lesions [1].
Nevertheless, factors as the tooth location (anterior or posterior region), tooth anatomy (multi- or single-rooted teeth), and the presence of thinning of the cortical bone could influence the detection of periapical lesions in 2D images, but those have not been considered in the CBCT-PAI. As the radiographic detection of AR may be related to these tooth and AR characteristics, the knowledge of which factors could contribute to its early diagnosis is clinically important for the prognosis of the endodontic treatment.
Therefore, the present study aimed to evaluate the detection rate of the AR in 2D images (PAN and PERI) using CBCT images as the reference standard, as well as to investigate which factors related to the AR, such as those used in the CBCT-PAI index, thinning of cortical bone and tooth characteristics could influence on its detection. The null hypothesis considered that the factors under study would not influence the detection of AR.
MATERIALS AND METHODS
After approval by the local Research Ethics Committee (protocol No. 91199018.5.0000.5418), sets of 2D (PERI and/or PAN) and CBCT exams were retrospectively collected from patients referred to the Oral Radiology service of the Department of Oral Diagnosis of the Piracicaba Dental School, University of Campinas, Brazil, over a 2-year period. Those patients were referred for imaging exams for various indications regardless of the present study (e.g., endodontics, surgery, and prosthetic indications). The inclusion criteria consisted of patients who underwent PAN and/or PERI, and CBCT within a maximum interval of 15 days, with the same regions of interest being visualized in both exams. Fully edentulous patients, presence of bone pathologies other than apical pathologies involving the evaluated tooth, and CBCT images with low quality for diagnosis (e.g., exams with beam-hardening and motion-related artifacts) were excluded.
PAN images were acquired using the Orthopantomograph OP100D unit (Instrumentarium Corp., Tuusula, Finland). PERI images were acquired with the Express digital radiographic system (Instrumentarium Corp.) and CBCT images were acquired in the Picasso trio unit (E-WOO Technology, Yongin, Korea), with 0.2 mm voxel. Exposure protocols for all examinations, as well as the size and location of the field of view (FOV) for CBCT exams, varied according to the specific indications for each patient.
After applying the inclusion criteria, the exams were divided into 2 groups (Figure 1): PAN+CBCT, composed of panoramic radiographs and CBCT images from the same patients, accounting for 227 teeth (285 dental roots); and PERI+CBCT, composed of PERIs and CBCT images from the same patients, totaling 94 teeth (115 dental roots). The distribution of the teeth by group and dental arch is shown in Table 1.
Figure 1
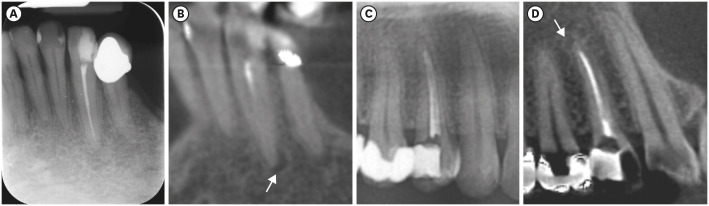
Images of PERI+CBCT and PAN+CBCT groups evaluated. Lower left canine in PERI (A) and CBCT coronal reconstruction (B). An upper right first premolar observed in cropped PAN (C) and CBCT sagittal reconstruction (D). Arrows indicate the apical radiolucencies detected in CBCT reconstructions.
CBCT, cone-beam computed tomography; PAN, panoramic radiograph; PERI, periapical radiograph.
Table 1
Distribution of the study sample according to each image group
The teeth that were present in both 2D and 3D imaging modalities (PAN+CBCT or PERI+CBCT) were recorded in an Excel spreadsheet (Microsoft Corporation, Redmond, WA, USA) for further evaluation by the examiners. For multi-rooted teeth, each root was assessed individually.
Initially, the 2D images (PAN and PERI) were evaluated for the presence or absence of AR using the ImageJ software (National Institutes of Health, Bethesda, MD, USA). AR was considered present when a well delimited radiolucent image was observed in the periapical region, more than 1 mm in width or twice the size of the periodontal ligament space.
Subsequently, the CBCT images, which acted as a reference standard, were evaluated using OnDemand3D software (Cybermed, Irvine, CA, USA) in a quiet and dimly lightroom. The periapical status was assessed according to the modified periapical CBCT-PAI index in which the images were analyzed in the buccolingual, mesiodistal and corono-apical dimensions to determine the presence and size of the periapical lesions. Score 0 was assigned for healthy periapex (periodontal ligament space up to 1 mm) and the scores 1, 2 and 3 for AR with diameters of 1 to 2 mm, 2 to 4 mm, > 4 mm, respectively, based on the highest measure observed among all the plans [1,11]. The presence of bone cortical expansion and destruction were also recorded. In addition, the location of the tooth (anterior/posterior and maxilla/mandible), if the tooth was single or multi-rooted, and the presence and degree of cortical thinning at the AR site were recorded. When present, the degree of cortical thinning was classified as mild, moderate or severe thinning when the remaining cortical thickness was 2/3, 1/2, and 1/4 of the maximum cortical thickness, respectively [12].
The images were evaluated simultaneously by 2 blinded examiners in a darkened environment, using a 21-inch LCD monitor with a screen resolution of 1,280 × 1,024. The brightness and contrast of the images and the zoom tool could be used at the discretion of the examiners.
Statistical analysis was performed with SPSS software version 23.0 (SPSS, Inc, Chicago, IL, USA). Pearson's χ2 test compared the detection of AR between 2D and 3D imaging modalities. Accuracy, sensitivity, specificity, positive and negative predictive values were obtained for PERI and PAN images, using CBCT as the reference standard. Binomial logistic regression tested which factors related to AR interfere with its detection in 2D images. The significance level was set at 0.05.
RESULTS
According to CBCT reference standard (whose detection rate was considered to be 100% in data analysis), in the PERI+CBCT and PAN+CBCT groups, AR was present in 22.6% (26 out of 115) and 27.4% (78 out of 285) of the dental roots, respectively. Table 2 details the detection rate of AR in PERI and PAN compared to CBCT. PERI had a higher detection rate (65.4%, or 17 out of 26) than PAN images (39.7%, or 31 out of 78) (Figure 2). However, both radiographic modalities differed significantly from the CBCT findings (p < 0.001).
Table 2
Detection of apical radiolucency on PERI and PAN images compared with CBCT images (reference standard)
Figure 2
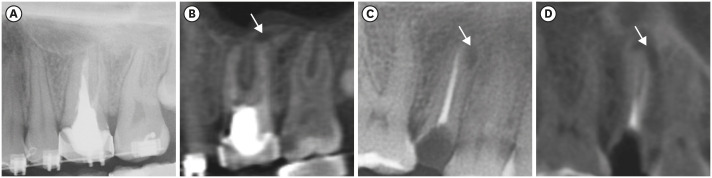
An apical radiolucency in a multi-rooted tooth that was not detected in PAN (A), but detected in the CBCT sagittal reconstruction, indicated by the arrow (B). The arrows are indicating an apical radiolucency detected on both PAN (C) and CBCT sagittal reconstruction (D) of a single-root tooth.
CBCT, cone-beam computed tomography; PAN, panoramic radiograph.
Diagnostic values of the 2D radiographic modalities evaluated are shown in Table 3. Although PERI and PAN presented high values of accuracy (0.83 and 0.77, respectively) and specificity (0.89 and 0.91, respectively), there was a low sensitivity in the detection of AR, especially for PAN images (0.40 vs. 0.65 of PERI). Also, high negative predictive values and low positive predictive values were related to both imaging modalities.
Table 3
Diagnostic tests of accuracy, sensitivity, specificity, PPV and NPV for PERI and PAN images
| Variables | Accuracy | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| PERI | 0.83 | 0.65 | 0.89 | 0.63 | 0.90 |
| PAN | 0.77 | 0.40 | 0.91 | 0.63 | 0.80 |
Regarding the factors that could influence the detection of AR in 2D images, the binomial logistic regression showed that radiolucency size (in all scores) was significantly related to its detection in both PERI and PAN radiographs (p < 0.05) (Table 4). In addition, in the PAN images, AR has 3.93 times more chances of being detected when they were related to single-rooted teeth than to multi-rooted teeth (p = 0.038). On the other hand, the factors ‘location’ (anterior/posterior and maxilla/mandible), ‘presence and degree of bone cortical thinning,’ ‘cortical expansion,’ and ‘cortical destruction’ did not influence AR detection in any of the radiographic modalities (p > 0.05).
Table 4
Binomial logistic regression detailing the possible factors that influence the detection of apical radiolucency on PERI and PAN images
DISCUSSION
The periapical status of a tooth is an important factor to be detected by the clinician to advise the patient about treatment options and their success rates [13,14]. It is known that radiographic exams may underestimate the detection of periapical lesions when compared to CBCT [2,8,9,10,13,15,16,17]. Our findings confirm a lower accuracy of PERI (83%) and PAN (77%) when compared to CBCT for this diagnostic task. To make it possible to evaluate the accuracy of PERI and PAN in detecting AR, we used CBCT as a reference standard since no other method could be applied to determine the presence of apical lesions in an in vivo study. Therefore, in data analysis, the rate of detection of CBCT was considered 100%. Additionally, the present study investigated which morphological factors associated with AR could influence its detection in 2D radiographic examinations. According to our results, the size of AR was the factor that most influenced its detection for both radiographic modalities investigated. For PAN, root morphology was an additional factor that influenced AR detection, as in single-rooted tooth there was higher AR detection.
Although imaging exams are indispensable to assess the periapical tissues, the most conclusive method to detect apical periodontitis is the histopathological evaluation [18]. However, this procedure is invasive and not ethically acceptable for clinical studies. Thus, the CBCT evaluation was considered the reference standard, since this imaging modality allows a dynamic assessment of the scanned volume in the three dimensions with high resolution. A previous ex vivo study investigated the accuracy of PERI and CBCT in apical periodontitis detection, using histopathological examination as a reference standard [16]. The high diagnostic values (sensitivity, 0.89; specificity, 1.0; area under the receiver operating characteristic curve, 0.943; positive predictive value, 1.0; and negative predictive value, 0.81) obtained by the CBCT evaluation endorse the choice of this imaging modality as a reference standard for clinical studies.
Regarding the methodology, this study investigated the relationship between the factors considered in the CBCT-PAI index and the detection of AR in radiographic images. This classification system has advantages over the PAI, since it is based on a 3D evaluation, allowing precise analysis of AR dimension [1,8]. Moreover, this classification may be considered more complex, since it evaluates the presence of sequelae resulting from apical periodontitis, such as the expansion of cortical bone and the presence of cortical bone destruction. As in a previous study [8], aiming the simplification of this method, in the present study it was done an adaptation regarding the lesion size classification, reducing from 6 to 4 possible scores for this variable.
The present study is novel in evaluating 2 groups of radiographic exams (periapical and/or panoramic) and CBCT exams of the same patient, both acquired in a short time interval. The lower sensitivity found for 2D images was expected due to the inherent limitations of the radiographic technique, such as superposition of anatomical structures [8,9,10,17,19]. Another important radiographic limitation is the time-lapse between a bone change and its radiographic appearance, since a 30%–50% bone demineralization threshold is required for radiographic identification [2,9].
First, we hypothesized that some factors related to the cortical bone (e.g., thinning and perforation) could influence the radiographic detection of the AR, as reported in previous ex vivo studies [20,21]. However, the main factor that influenced the radiographic detection of AR was its size. This might have occurred due to the lower incidence of cases with complications related to the integrity of the cortical bone (e.g., thinning and perforation) in the vicinity of the periapical regions in the present retrospective study. Additionally, root morphology influenced PAN evaluation, since the lesions were more easily detected in single-rooted teeth. We believe that this result is related to the greater difficulty in the evaluation of the periapical region of multi-rooted teeth, especially those located in the maxilla. The maxilla region has a large superposition of anatomical structures and higher buccolingual bone thickness, which could explain this finding. Previous studies aimed to evaluate the diagnostic accuracy of PAN for the detection of apical periodontitis in teeth with and without endodontic treatment, using CBCT images as the reference standard [9,10]. Corroborating to our hypothesis, the results presented by those authors show that in the posterior maxilla there is a lower detection of apical periodontitis when compared to other regions, such as canines, premolars, and lower molars [9,10].
As is known, sensitivity and specificity are, respectively, the ability of a test to correctly identify those with (true positives) and without (true negatives) the condition evaluated (e.g., detection of periapical radiolucency); while the positive and negative predictive values represent the probability of the test result being correct, both when the condition tested is present (positive predictive value) and when the condition tested is absent (negative predictive value). Accuracy, in turn, represents the overall percentage of correct answers of the test in relation to the total number of cases. The low sensitivity values and high specificity values obtained in the present study suggest that there is an increase in the number of false-negatives and true-positives AR detected in the radiographic evaluation. The findings obtained by previous studies are in accordance with our results [2,9,16]. On the other hand, these previous studies show lower negative predictable value, higher positive predictable value, and lower accuracy values when compared to our results, which may be explained by the sample composed of a larger number of teeth without the presence of AR (i.e., control). Thus, these results are expected due to the greater ability of radiographic exams to detect teeth without the presence of an AR.
The present study used a convenience sample from patients that acquired radiographic and tomographic exams in a short period between each other. The sample used for this study showed a lower incidence of teeth with periapical lesions, as well as complications resulting from these injuries (e.g., cortical interruption and expansion). This lower incidence probably occurred due the patients had been referred for imaging examination for several reasons, not necessarily for endodontic purposes.
CONCLUSIONS
In conclusion, the 2D images have moderate accuracy in the AR detection, with discrete better performance for periapical radiography examination. The main factor that influenced the radiographic detection of the AR is the size of the lesion, and larger lesions are easier detected in both radiographic examinations (periapical and panoramic radiographies). In addition, in panoramic radiography, AR related to single-rooted teeth may be easier detected.
-
Funding: This study was financed in part by PIBIC/CNPq (National Council for Scientific and Technological Development) and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Fontenele RC, Nascimento EHL, Freitas DQ.
Data curation: Gaêta-Araujo H, Cardelli LOA.
Formal analysis: Fontenele RC, Nascimento EHL, Freitas DQ.
Funding acquisition: Fontenele RC, Nascimento EHL, Gaêta-Araujo H, Freitas DQ.
Investigation: Fontenele RC, Nascimento EHL, Gaêta-Araujo H, Freitas DQ.
Methodology: Fontenele RC, Nascimento EHL, Freitas DQ.
Project administration: Fontenele RC, Nascimento EHL, Freitas DQ.
Resources: Fontenele RC, Freitas DQ.
Software: Gaêta-Araujo H, Cardelli LOA, Freitas DQ.
Supervision: Freitas DQ.
Validation: Fontenele RC, Nascimento EHL, Freitas DQ.
Visualization: Fontenele RC, Nascimento EHL, Gaêta-Araujo H, Freitas DQ.
Writing - original draft: Fontenele RC, Nascimento EHL, Gaêta-Araujo H, Cardelli LOA, Freitas DQ.
Writing - review & editing: Freitas DQ.
- 1. Estrela C, Bueno MR, Azevedo BC, Azevedo JR, Pécora JD. A new periapical index based on cone beam computed tomography. J Endod 2008;34:1325-1331.ArticlePubMed
- 2. Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod 2008;34:273-279.ArticlePubMed
- 3. de Freitas JV, Baratto-Filho F, Coelho BS, Tomazinho FSF, Crozeta BM, de Sousa Neto MD, Gabardo MCL. Efficacy of different cone-beam computed tomographic protocols in the identification of mesiobuccal canals of maxillary first molars: a tomographic and ex vivo study. J Endod 2017;43:810-815.ArticlePubMed
- 4. Patel S. New dimensions in endodontic imaging: part 2. Cone beam computed tomography. Int Endod J 2009;42:463-475.ArticlePubMed
- 5. Moura MS, Guedes OA, De Alencar AH, Azevedo BC, Estrela C. Influence of length of root canal obturation on apical periodontitis detected by periapical radiography and cone beam computed tomography. J Endod 2009;35:805-809.ArticlePubMed
- 6. Durack C, Patel S. Cone beam computed tomography in endodontics. Braz Dent J 2012;23:179-191.ArticlePubMed
- 7. Patel S, Brown J, Pimentel T, Kelly RD, Abella F, Durack C. Cone beam computed tomography in endodontics - a review of the literature. Int Endod J 2019;52:1138-1152.ArticlePubMedPDF
- 8. Pope O, Sathorn C, Parashos P. A comparative investigation of cone-beam computed tomography and periapical radiography in the diagnosis of a healthy periapex. J Endod 2014;40:360-365.ArticlePubMed
- 9. Nardi C, Calistri L, Pradella S, Desideri I, Lorini C, Colagrande S. Accuracy of orthopantomography for apical periodontitis without endodontic treatment. J Endod 2017;43:1640-1646.ArticlePubMed
- 10. Nardi C, Calistri L, Grazzini G, Desideri I, Lorini C, Occhipinti M, Mungai F, Colagrande S. Is panoramic radiography an accurate imaging technique for the detection of endodontically treated asymptomatic apical periodontitis? J Endod 2018;44:1500-1508.ArticlePubMed
- 11. Esposito S, Cardaropoli M, Cotti E. A suggested technique for the application of the cone beam computed tomography periapical index. Dentomaxillofac Radiol 2011;40:506-512.ArticlePubMedPMC
- 12. Kapila R, Harada N, Araki K, Sano T, Goto TK. Evaluation of juxta-apical radiolucency in cone beam CT images. Dentomaxillofac Radiol 2014;43:20130402.ArticlePubMedPMC
- 13. Patel S, Wilson R, Dawood A, Foschi F, Mannocci F. The detection of periapical pathosis using digital periapical radiography and cone beam computed tomography - part 2: a 1-year post-treatment follow-up. Int Endod J 2012;45:711-723.ArticlePubMed
- 14. Davies A, Mannocci F, Mitchell P, Andiappan M, Patel S. The detection of periapical pathoses in root filled teeth using single and parallax periapical radiographs versus cone beam computed tomography - a clinical study. Int Endod J 2015;48:582-592.ArticlePubMed
- 15. López FU, Kopper PM, Cucco C, Della Bona A, de Figueiredo JA, Vier-Pelisser FV. Accuracy of cone-beam computed tomography and periapical radiography in apical periodontitis diagnosis. J Endod 2014;40:2057-2060.ArticlePubMed
- 16. Kanagasingam S, Lim CX, Yong CP, Mannocci F, Patel S. Diagnostic accuracy of periapical radiography and cone beam computed tomography in detecting apical periodontitis using histopathological findings as a reference standard. Int Endod J 2017;50:417-426.ArticlePubMedPDF
- 17. Abella F, Patel S, Durán-Sindreu F, Mercadé M, Bueno R, Roig M. An evaluation of the periapical status of teeth with necrotic pulps using periapical radiography and cone-beam computed tomography. Int Endod J 2014;47:387-396.ArticlePubMed
- 18. Kanagasingam S, Hussaini HM, Soo I, Baharin S, Ashar A, Patel S. Accuracy of single and parallax film and digital periapical radiographs in diagnosing apical periodontitis - a cadaver study. Int Endod J 2017;50:427-436.ArticlePubMedPDF
- 19. Kruse C, Spin-Neto R, Wenzel A, Kirkevang LL. Cone beam computed tomography and periapical lesions: a systematic review analysing studies on diagnostic efficacy by a hierarchical model. Int Endod J 2015;48:815-828.ArticlePubMed
- 20. Bender IB. Factors influencing the radiographic appearance of bony lesions. J Endod 1997;23:5-14.ArticlePubMed
- 21. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: II. 1961. J Endod 2003;29:707-712.PubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Radiomics-based classification of pediatric dental trauma in periapical radiographs: a preliminary study
Mengtian Peng, Bin Yu, Juan Hu, Xiaoxin Xie, Jihong He
BMC Medical Imaging.2025;[Epub] CrossRef - Increasing Diagnostic Acumen in Endodontics
Shilpa Thakkar, Dana Mominkhan
Dental Clinics of North America.2025; 69(4): 479. CrossRef - Three-dimensional clinical assessment for MRONJ risk in oncologic patients following tooth extractions
Catalina Moreno Rabie, Rocharles Cavalcante Fontenele, Nicolly Oliveira Santos, Fernanda Nogueira Reis, Tim Van den Wyngaert, Reinhilde Jacobs
Dentomaxillofacial Radiology.2023;[Epub] CrossRef - Quality of techniques used to assess clinical outcomes of regenerative endodontic treatment in necrotic mature teeth
Roy George
Evidence-Based Dentistry.2022; 23(3): 98. CrossRef
 ePub Link
ePub Link Cite
CiteWhich factors related to apical radiolucency may influence its radiographic detection? A study using CBCT as reference standard
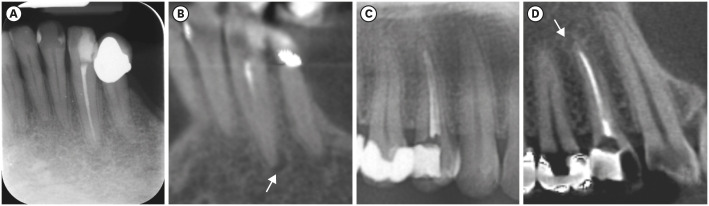
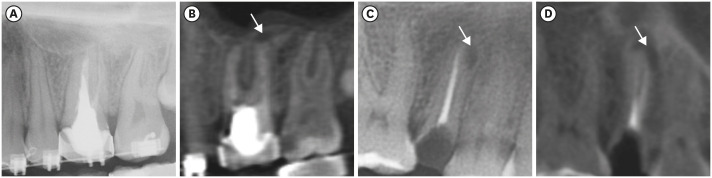
Figure 1 Images of PERI+CBCT and PAN+CBCT groups evaluated. Lower left canine in PERI (A) and CBCT coronal reconstruction (B). An upper right first premolar observed in cropped PAN (C) and CBCT sagittal reconstruction (D). Arrows indicate the apical radiolucencies detected in CBCT reconstructions.CBCT, cone-beam computed tomography; PAN, panoramic radiograph; PERI, periapical radiograph.
Figure 2 An apical radiolucency in a multi-rooted tooth that was not detected in PAN (A), but detected in the CBCT sagittal reconstruction, indicated by the arrow (B). The arrows are indicating an apical radiolucency detected on both PAN (C) and CBCT sagittal reconstruction (D) of a single-root tooth.CBCT, cone-beam computed tomography; PAN, panoramic radiograph.
Figure 1
Figure 2
Which factors related to apical radiolucency may influence its radiographic detection? A study using CBCT as reference standard
Distribution of the study sample according to each image group
| Image group | Dental arch | Region | Number of teeth (%) |
|---|---|---|---|
| PERI+CBCT | Maxilla | Anterior | 28 (29.8) |
| Posterior | 19 (20.2) | ||
| Mandible | Anterior | 28 (29.8) | |
| Posterior | 19 (20.2) | ||
| PAN+CBCT | Maxilla | Anterior | 47 (20.7) |
| Posterior | 63 (27.8) | ||
| Mandible | Anterior | 47 (20.7) | |
| Posterior | 70 (30.8) |
CBCT, cone-beam computed tomography; PAN, panoramic radiograph; PERI, periapical radiograph.
Detection of apical radiolucency on PERI and PAN images compared with CBCT images (reference standard)
| Variables | CBCT | p value* | |||
|---|---|---|---|---|---|
| Absence | Present | Total | |||
| PERI | |||||
| Absence | 79 (88.8) | 9 (34.6) | 88 (76.5) | < 0.001 | |
| Presence | 10 (11.2) | 17 (65.4) | 27 (23.5) | ||
| Total | 89 (77.4) | 26 (22.6) | 115 (100.0) | ||
| PAN | |||||
| Absence | 189 (91.3) | 47 (60.3) | 236 (82.8) | < 0.001 | |
| Presence | 18 (8.7) | 31 (39.7) | 49 (17.2) | ||
| Total | 207 (72.6) | 78 (27.4) | 285 (100.0) | ||
Bold numbers indicate agreement between imaging modalities.
CBCT, cone-beam computed tomography; PAN, panoramic radiograph; PERI, periapical radiograph.
*According to Pearson's χ2 test.
Diagnostic tests of accuracy, sensitivity, specificity, PPV and NPV for PERI and PAN images
| Variables | Accuracy | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| PERI | 0.83 | 0.65 | 0.89 | 0.63 | 0.90 |
| PAN | 0.77 | 0.40 | 0.91 | 0.63 | 0.80 |
NPV, negative predictive value; PAN, panoramic radiograph; PERI, periapical radiograph; PPV, positive predictive value.
Binomial logistic regression detailing the possible factors that influence the detection of apical radiolucency on PERI and PAN images
| Variables | Estimate | SE | Wald χ2 | p value | OR | 95% CI (min–max) | ||
|---|---|---|---|---|---|---|---|---|
| PERI | ||||||||
| Localization and tooth morphology | ||||||||
| Maxillary or mandibular | 1.467 | 0.913 | 2.581 | 0.108 | 4.33 | (0.72–25.94) | ||
| Anterior or posterior | −1.503 | 1.093 | 1.89 | 0.169 | 0.22 | (0.26–1.89) | ||
| Single- or multi-rooted | 1.051 | 1.152 | 0.832 | 0.362 | 2.86 | (0.29–27.37) | ||
| Apical radiolucency size | 19.152 | < 0.001 | ||||||
| Score 1 | 3.18 | 1.262 | 6.352 | 0.012 | 24.05 | (2.03–285.27) | ||
| Score 2 | 2.377 | 0.761 | 9.744 | 0.002 | 10.77 | (2.42–47.92) | ||
| Score 3 | 3.68 | 1.393 | 6.981 | 0.008 | 39.64 | (2.59–607.44) | ||
| Cortical thinning | 0.00 | 1.000 | ||||||
| Score 1 | 42.033 | 46,176.01 | 0.00 | 0.999 | - | (0.00) | ||
| Score 3 | 62.95 | 61,218.45 | 0.00 | 0.999 | - | (0.00) | ||
| Cortical expansion | −20.410 | 27,670.73 | 0.00 | 0.999 | 0.00 | (0.00) | ||
| Cortical destruction | −20.092 | 22,732.18 | 0.00 | 0.999 | 0.00 | (0.00) | ||
| PAN | ||||||||
| Localization and tooth morphology | ||||||||
| Maxillary or mandibular | −0.632 | 0.383 | 2.718 | 0.099 | 0.53 | (0.25–1.13) | ||
| Anterior or posterior | 0.211 | 0.855 | 0.061 | 0.805 | 1.24 | (0.23–6.59) | ||
| Single- or multi-rooted | −1.641 | 0.791 | 4.3 | 0.038 | 3.93 | (0.04–0.91) | ||
| Apical radiolucency size | 9.092 | 0.028 | ||||||
| Score 1 | 1.495 | 0.716 | 4.356 | 0.037 | 4.46 | (1.1–18.14) | ||
| Score 2 | 2.607 | 0.886 | 8.668 | 0.003 | 13.6 | (2.39–76.92) | ||
| Score 3 | 1.768 | 0.83 | 4.538 | 0.033 | 5.86 | (1.15–29.8) | ||
| Cortical thinning | 1.114 | 0.774 | ||||||
| Score 1 | −0.456 | 1.281 | 0.127 | 0.722 | 0.63 | (0.51–7.81) | ||
| Score 2 | 1.008 | 1.674 | 0.362 | 0.547 | 2.74 | (0.1–72.94) | ||
| Score 3 | −21.969 | 17,416.11 | 0.00 | 0.999 | 0.00 | (0.00) | ||
| Cortical expansion | −21.119 | 22,939.57 | 0.00 | 0.999 | 0.00 | (0.00) | ||
| Cortical destruction | 0.819 | 1.176 | 0.485 | 0.486 | 2.27 | (0.23–22.72) | ||
OR, odds ratio; CI, confidence interval; PAN, panoramic radiograph; PERI, periapical radiograph; SE, standard error.
Table 1 Distribution of the study sample according to each image group
CBCT, cone-beam computed tomography; PAN, panoramic radiograph; PERI, periapical radiograph.
Table 2 Detection of apical radiolucency on PERI and PAN images compared with CBCT images (reference standard)
Bold numbers indicate agreement between imaging modalities.
CBCT, cone-beam computed tomography; PAN, panoramic radiograph; PERI, periapical radiograph.
*According to Pearson's χ2 test.
Table 3 Diagnostic tests of accuracy, sensitivity, specificity, PPV and NPV for PERI and PAN images
NPV, negative predictive value; PAN, panoramic radiograph; PERI, periapical radiograph; PPV, positive predictive value.
Table 4 Binomial logistic regression detailing the possible factors that influence the detection of apical radiolucency on PERI and PAN images
OR, odds ratio; CI, confidence interval; PAN, panoramic radiograph; PERI, periapical radiograph; SE, standard error.

