
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 47(3); 2022 > Article
- Research Article Effects of different topical anesthetics on pain from needle insertion and injection, and the influence of anxiety in patients awaiting endodontic treatment
-
Fatih Aksoy1
 , Samet Tosun2
, Samet Tosun2 -
Restor Dent Endod 2022;47(3):e25.
DOI: https://doi.org/10.5395/rde.2022.47.e25
Published online: June 7, 2022
1Department of Endodontics, Faculty of Dentistry, Adıyaman University, Adıyaman, Turkey.
2Department of Endodontics, Faculty of Dentistry, Pamukkale University, Denizli, Turkey.
- Correspondence to Fatih Aksoy, DDS, PhD. Associate Professor, Department of Endodontics, Faculty of Dentistry, Adıyaman University, No:411, 02200, Adıyaman, Turkey. dr.f.aksoy@gmail.com
• Received: October 6, 2021 • Revised: December 9, 2021 • Accepted: January 10, 2022
Copyright © 2022. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to evaluate the effects of 5% lidocaine and 2.5% lidocaine/2.5% prilocaine topical anesthetic on pain during needle insertion and infiltration injection in the labial mucosa of anterior maxillary teeth, and to assess the relationship between patients’ anxiety and pain scores.
-
Materials and Methods The Modified Dental Anxiety Scale questionnaire was applied and recorded. Patients were randomly divided into 4 groups (n = 30), as follows: G1 group: 5% lidocaine and placebo for 1 minute, G2 group: 2.5% lidocaine/2.5% prilocaine and placebo for 1 minute, G3 group: 5% lidocaine and placebo for 3 minutes, and G4 group: 2.5% lidocaine/2.5% prilocaine and placebo for 3 minutes. Before the application of topical anesthesia, one side was randomly selected as the topical anesthesia and the contralateral side as the placebo. The pain levels were measured with Visual Analog Scale (VAS) immediately after needle insertion and injection and were compared. The correlation between anxiety and pain scores was analyzed.
-
Results Administration of 5% lidocaine for 1 minute had significantly higher pain scores for both insertion and infiltration injection than the other groups (p < 0.05). There was a significant moderate positive correlation between dental anxiety and the injection-induced VAS pain score in the placebo side in all groups (p < 0.05).
-
Conclusions Topical anesthetics significantly reduced the pain caused by both needle insertion and injection pain in comparison to the placebo side. The pain scores of patients with dental anxiety were lower on the topical anesthesia compared to the placebo side.
-
Trial Registration Thai Clinical Trials Registry Identifier: TCTR20201217002
INTRODUCTION
Intraoral local anesthesia is one of the most widely used strategies for managing pain during dental treatments, especially endodontic treatments, but is also feared by many patients [1,2,3,4]. In dental practice, injections into the mouth often cause patients serious anxiety [5]. Psychological factors, such as anxiety and fear, play important roles in pain perception. A previous study reported more intense and prolonged pain in highly anxious than normal subjects [6]. Therefore, evaluations should be made in the former group.
Two types of pain are associated with the administration of local anesthesia, namely at needle insertion and during injection of anesthetic solution [4]. Some patients may consider the anesthetic injection to be as worrisome as the dental treatment itself [7]. Therefore, dentists should try to make injections as painless as possible. Topical anesthetic agents have long been used in dentistry to reduce the pain that occurs during infiltration injections [8].
The topical anesthetic agents routinely used worldwide are 5% lidocaine and a mixture of 2.5% lidocaine/2.5% prilocaine [9,10]. These are classified as amide-type anesthetics, and are also used as gel, solution, ointment, and spray formulations [11]. In previous studies, topical anesthesia was applied to the oral mucosa for varying amounts of time [10,12]. However, there is no consensus on the optimum application time for local anesthetics. In addition, the permeability of the oral mucosal epithelium can be affected by the application method and time [13].
Clinical research is still lacking considering the role of the aforementioned factors in topical anesthesia. Here, we evaluated the effects of topical anesthesia at the needle insertion and injection site (in the labial mucosa of anterior maxillary teeth) according to application time, and assessed the effects of dental anxiety on patient pain levels.
MATERIALS AND METHODS
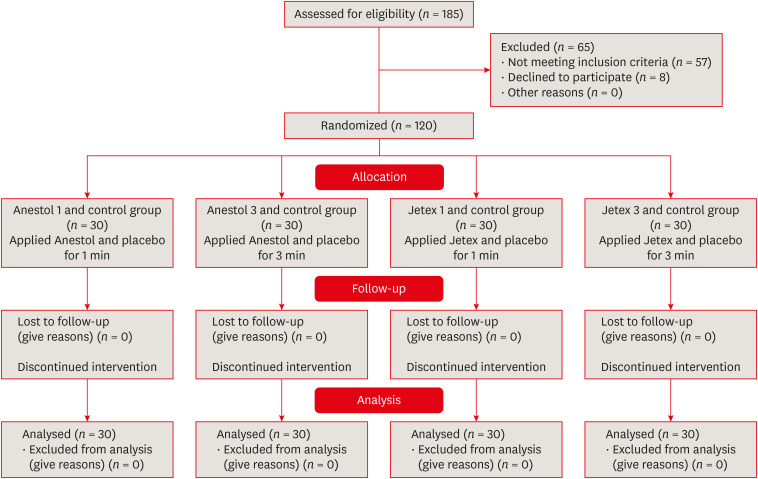
This split-mouth placebo-controlled double-blind clinical study was performed to examine the efficacy of different topical anesthetics for the control of pain, and the influence of anxiety, in patients awaiting endodontic treatment (Figure 1 for a flow diagram).
According to the reference study Visual Analog Scale (VAS) results; they had a large effect size (f = 0.604) [14]. Assuming we can achieve a lower effect size level (f = 0.35), a power analysis (G*Power 3.1 software, Heinrich-Heine-Universität Düsseldorf, Dusseldorf, Germany) was performed before the present study. Accordingly, when at least 96 participants (at least 24 participants for each therapy) were included in the study, that would result in 80% power with 95% confidence level (5% type 1 error rate). We included 120 participants in the present study (30 participants for each group). For VAS results, we had a large effect size (f = 0.518) and with this result, we reached 99.8% power with 95% confidence.
The commercial topical formulations used in this study were 5% lidocaine (Anestol® 5%, Sandoz, Kocaeli, Turkey) and 2.5% lidocaine/2.5% prilocaine mixture (Jetex® 5%, Pharmet, Istanbul, Turkey). As a placebo for each topical anesthetics, a topical gel with the same appearance and color that consists of polyethylene glycol 1500, polyethylene glycol 6000, propylene glycol, methyl paraben, and propyl paraben was prepared by a pharmacologist.
A total of 120 patients volunteered to participate in this split-mouth double-blind clinical trial. All patients provided written informed consent prior to participating in the study. The eligibility criteria were as follows: aged 18–65 years, American Society of Anesthesiologists category I or II, able to read the informed consent form and willing to participate, and no intolerance and/or allergies to the ingredients of the drugs used in the study. Vital teeth were selected that were clinically asymptomatic without spontaneous, prolonged, severe pain, and radiographic pathology and none had received apical surgery. None of the patients had used sedative analgesics or anxiety medications in the 12 hours prior to the study, and pregnant and breastfeeding women were excluded.
Initially, the Modified Dental Anxiety Scale (MDAS) of Humphris et al. [15], consisting of 5 questions each rated from 1 to 5, was used to determine the level of dental anxiety of each patient. MDAS scores were recorded.
To determine the efficacy of topical anesthetics relative to each other and the placebo, 5% lidocaine, 2.5% lidocaine/2.5% prilocaine mixture and placebo creams were placed in identical boxes, which were numbered using a random number table by a clinical nurse. The similar appearance of the boxes ensured that the clinician, patients and study authors were all blinded to the treatment. The nurse placed equal amounts of topical anesthetic and placebo treatment on sterile gauze (2 × 2 inches), and then passed the gauze to the clinician. Prior to the administration of agents (topical anesthesia or placebo), one side of the anterior maxillary region was randomly selected as the topical anesthetic side, with the contralateral side serving as the control (placebo) in each group. The sides to which the substances were applied were systematically alternated. In total, 120 patients were randomly divided into 4 groups (n = 30) using the Research Randomizer program (version 4.0, Urbaniak G.C. and Plous S., Lancaster, PA, USA; accessed at www.randomizer.org). It was implemented as follows: G1 group: 5% lidocaine and placebo cream for 1 minute; G2 group: 2.5% lidocaine/2.5% prilocaine mixture and placebo cream for 1 minute; G3 group: 5% lidocaine and placebo cream for 3 minutes; and G4 group: 2.5% lidocaine/2.5% prilocaine mixture and placebo cream for 3 minutes. In each group, one of the topical anesthetic creams was applied to the labial mucosa of the anterior maxillary tooth for 1 or 3 minutes; placebo creams were also applied for 1 or 3 minutes, to the contralateral side of the same patient.
The patients were instructed to score their pain during needle insertion and injection on a 100-mm horizontal non-graded VAS. In all groups, the same clinician inserted a 27-gauge needle (Ayset, Adana, Turkey) into the labial mucosa of the anterior maxillary tooth on the anesthetic side to a depth of 5 mm and then the patient was asked to provide a VAS score [8]. This was followed immediately by an injection of 0.9 mL of the anesthetic solution (1.8 mL articaine 4% with 1: 100,000 epinephrine) over a period of 30 seconds., and then then the patient was asked again to provide a VAS score. The needle was withdrawn and inserted 5 mm into the labial mucosa of the anterior maxillary tooth on the placebo side, and the patient was then asked to give a VAS pain score again. This was immediately followed by an injection of 0.9 mL of anesthetic solution (1.8 mL of articaine 4% to 1:100,000 epinephrine) over a period of 30 seconds, after which the patient was again asked to give a VAS score. VAS scores were recorded. The means of VAS score for insertion or injection was compared within the group between (the topical anesthetic side and the contralateral side [placebo]), and between all groups.
Moreover, MDAS scores < 12 and ≥ 12 were considered to indicate low and high levels of dental anxiety level, respectively [8]. The means of VAS score for the insertion or the injection was compared to patients with lower MDAS scores and those with higher MDAS scores.
All statistical analyses were performed using SPSS 25.0 software (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) and categorical variables as number and percent. Shapiro-Wilk test was used for testing normality. If parametric test conditions were satisfied, independent samples t-test was used for comparisons among groups. If parametric test conditions were not satisfied, Mann-Whitney U test and Kruskal-Wallis variance was used for comparisons among groups. The post hoc Mann-Whitney U test with Bonferroni correction was used when Kruskal-Wallis variance analysis determined a significant difference. For pairwise comparisons; if parametric test conditions were satisfied paired samples t-test; and if parametric test conditions were not satisfied Wilcoxon signed rank test was used. Chi-square test was used to compare the categorical variables. Spearman correlation coefficient was used for determining the correlation between continuous variables. In all analyses, p < 0.05 was taken to indicate statistical significance.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the version 2008 of Helsinki declaration and registered at Thai Clinical Trials Registry (www.clinicaltrials.in.th; Thai Clinical Trial Registry identification number TCTR20201217002). The present study was approved by the Clinical Researches Ethics Committee of Adiyaman University (Adiyaman/Turkey, Approval No: 13-1/2019). Informed consent Informed consent was obtained from all individual participants included in the study.
RESULTS
A total of 120 patients (61 men and 59 women aged 20–63 years) participated in this study. The sex ratio and mean age were comparable between groups (Table 1). Sex and age were not significant factors among the groups (p > 0.05). The mean VAS pain scores are presented in Figure 2 and Table 2. Topical anesthetics significantly reduced both the insertion and injection pain in comparison to placebo. The administration of 5% lidocaine for 1 minute had significantly higher levels of insertion and injection pain on the topical anesthetic side than all other groups (p < 0.05). Assessment of pain scores at the time of needle insertion indicated that the administration of 2.5% lidocaine/2.5% prilocaine for 1 minute had significantly better results than the administration of 5% lidocaine for 1 minute. Furthermore, the administration of 5% lidocaine for 1 minute also showed significantly higher pain scores than the administration of 5% lidocaine for 3 minutes (p < 0.05).
Table 1
Demographic data of the patients; MDAS scores of the all groups
Figure 2
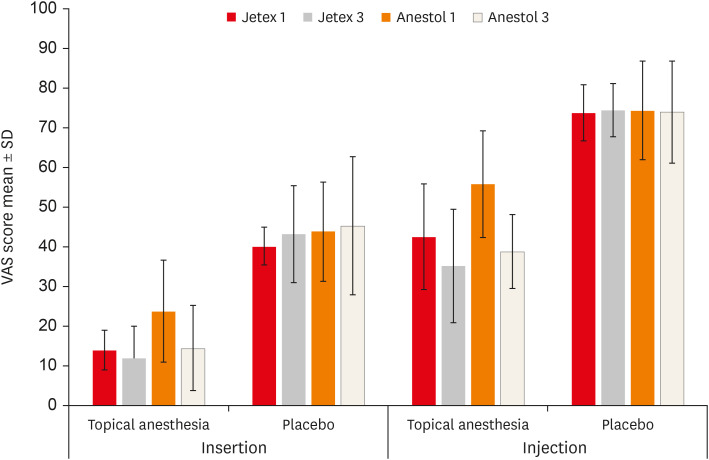
The needle insertion and injection VAS scores of the groups.
VAS, Visual Analog Scale; SD, standard deviation.
Table 2
Comparison of Visual Analog Scale scores (mm) between placebo and anesthesia after both the needle insertion and injection in all group
The MDAS scores of the patients ranged from 5 to 18 in the present study. There was no statistically significant difference in mean MDAS scores among the groups (p > 0.05) (Table 1). Besides, the mean and SD VAS scores of all groups are shown in Table 3 according to dental anxiety level. Patients with higher or lower MDAS scores showed significantly higher insertion and injection pain scores on the placebo side than on the topical anesthetic side (p < 0.05). In the G1 group, patients with high anxiety after, the administration of 5% lidocaine for 1 minute showed significantly higher pain scores during needle insertion than patients with low anxiety (p < 0.05).
Table 3
Comparison of the Visual Analog Scale scores according to Modified Dental Anxiety Scale anxiety levels in all group
Patients with high anxiety showed significantly higher pain scores during injections on the placebo side in all groups than patients with low anxiety (p < 0.05). Furthermore, we found a significant moderate correlation between dental anxiety and pain scores on the placebo side in all groups (p < 0.05). Age did not have a significant correlation with VAS pain scores in either the topical anesthetic side or the placebo side (p > 0.05).
DISCUSSION
According to some studies, topical anesthesia is highly effective for reducing pain during dental procedures; however, others have reported contradictory results [1,16,17,18]. In this study, there were significant differences in pain caused by insertion and injection between the topical anesthetic and placebo-treated sides, as shown in Table 2. These findings are consistent with the results of previous studies using 5% lidocaine and a 2.5% lidocaine/2.5% prilocaine mixture [19,20]. Therefore, we suggest the use of topical anesthesia to reduce pain during needle insertion and infiltration injection for maxillary anterior teeth.
A more realistic reaction to pain may express in actual patients than in healthy volunteers [21]. In the present study, the effects of placebo treatment and topical anesthetic were compared in the same patients, to avoid bias associated with interindividual differences. The design also avoided bias associated with temporal differences, where the discrepancy in pain scores between visits can be quite large if there are changes in emotional, psychological, or physical variables [21]. Many previous studies have compared the efficacy of topical anesthetics to placebo, with varying results [1,8,19,22]. The discrepant results may have been due to methodological differences among the studies.
We used a VAS pain score in this study, which is one of the most commonly used methods for assessing pain perception. Previous studies showed that the VAS pain score is a repeatable and highly sensitive method [23,24].
Different parts of the mouth have been used as injection regions in studies [17,18]. In some studies, the labial mucosa of the maxillary anterior region was the preferred injection site [4,8,25]. In the present study, we preferred the labial mucosa of the maxillary anterior region. Another previous study reported that this was one of the most painful areas in the body in which to receive an injection, and that the severity of pain from needle insertion or injection was not associated with different anterior maxillary teeth to be anesthetized [26]. This area, which is suitable for a bilateral application, is therefore a representative sensitive area [27].
Most of the previous studies provided little information on the application time of topical anesthesia [28]. The main reason for an ineffectual anesthetic solution may be a short application time [22]. In the present study, we compared the effects of 1- and 3-minute topical anesthetic application times. One-minute application of 5% lidocaine was not as effective as 2.5% lidocaine/2.5% prilocaine mixture during needle insertion. However, there was no significant difference in efficacy with regard to needle insertion or injection pain between the 2 anesthetics with the 3-minute application time. In this study, the positive effect of 1-minute application of 2.5% lidocaine/2.5% prilocaine mixture with respect to the pain associated with needle insertion may have been due to its composition, i.e., a eutectic mixture of local anesthetics; such mixtures have a lower melting point, so are more easily absorbed through the oral mucous membrane [29].
A previous study reported that 5% lidocaine was as effective as 20% benzocaine if applied for at least 3 minutes [30]. In the present study, 5% lidocaine applied for 3 minutes was as effective as 2.5% lidocaine/2.5% prilocaine mixture applied for 1 minute. Moreover, similar efficacy was observed between 5% lidocaine and 2.5% lidocaine/2.5% prilocaine mixture applied for 3 minutes. In addition, 5% lidocaine applied for 3 minutes reduced pain more effectively than 5% lidocaine applied for 1 minute. In summary, these observations indicated that 5% lidocaine should be applied for at least 3 minutes to ensure a sufficient topical anesthetic effect. Thus, the optimum application time can differ according to both the concentration and type of topical anesthetic used.
Whether patients have anxiety and concerns regarding anesthesia can be determined using specific scales, which are convenient for the physician and aid treatment planning. In the present study, we used the MDAS questionnaire, which is known to be reliable when applied to Turkish populations, and using it alone does not increase the level of anxiety [31,32]. Some studies have shown that female patients have higher dental anxiety levels than male patients, while other studies found no sex difference [31,33,34,35]. In the present study, no relationship was found between sex and dental anxiety; the differences among the reports may have been due to cultural factors.
It is known that there is a relationship between dental anxiety and pain [34]. In addition, there are studies reporting that patients with dental anxiety suffer from significantly impaired oral health–related quality of life [36]. A systematic review reported that patients’ quality of life improved after endodontic treatment [37]. However, dental anxiety can be a serious obstacle to dental treatments. In patients awaiting endodontic treatment, anticipatory anxiety regarding the pain that may occur before or during treatment procedures can be distressing to patients. Despite the availability of a variety of pain management strategies, effective pain control is still difficult [38,39]. However, it may be concluded that successfully managing dental anxiety individuals is achievable for clinicians but requires a phased treatment approach and good communication [38]. For the dentist, the gains in successfully managing both the patient's oral health and dental anxiety can be counted as job satisfaction and minimizing clinical time loss [38]. In the present study, topical anesthesia was associated with significantly lower pain scores in highly anxious patients compared to placebo. We found a significant relationship between MDAS and VAS scores; patients with higher MDAS scores also had higher VAS scores during infiltration injection on the placebo side. These findings indicated that topical anesthesia reduced the effect of dental anxiety on increasing pain, consistent with results reported previously [8].
CONCLUSIONS
In conclusion, topical anesthetics facilitate the control of pain caused by both needle insertion and infiltration anesthesia in the anterior maxillary region. The 5% lidocaine was more effective when applied for 3 minutes than for 1 minute, while pain due to insertion and injection did not differ significantly by 2.5% lidocaine/2.5% prilocaine mixture application time. The presence of anxiety during infiltration injection into the anterior maxillary region had a significant effect on pain scores independent of the topical anesthetic application.
ACKNOWLEDGEMENTS
The authors are grateful to Hande Şenol for her assistance as statistical analyzer and Miray Ege as a pharmacologist.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Tosun S.
Data curation: Aksoy F.
Formal analysis: Aksoy F, Tosun S.
Investigation: Tosun S.
Methodology: Aksoy F.
Project administration: Aksoy F.
Supervision: Tosun S.
Validation: Tosun S.
Visualization: Tosun S.
Writing - original draft: Aksoy F, Tosun S.
Writing - review & editing: Aksoy F, Tosun S.
- 1. Parirokh M, Sadeghi AS, Nakhaee N, Pardakhty A, Abbott PV, Yosefi MH. Effect of topical anesthesia on pain during infiltration injection and success of anesthesia for maxillary central incisors. J Endod 2012;38:1553-1556.ArticlePubMed
- 2. Singh P. An emphasis on the wide usage and important role of local anesthesia in dentistry: a strategic review. Dent Res J (Isfahan) 2012;9:127-132.ArticlePubMedPMC
- 3. Leopold A, Wilson S, Weaver JS, Moursi AM. Pharmacokinetics of lidocaine delivered from a transmucosal patch in children. Anesth Prog 2002;49:82-87.PubMedPMC
- 4. Nakamura S, Matsuura N, Ichinohe T. A new method of topical anesthesia by using anesthetic solution in a patch. J Endod 2013;39:1369-1373.ArticlePubMed
- 5. Reader AW, Nusstein JM, Hargreaves KM. Local anesthesia in endodontics. Cohen’s pathways of the pulp. 10th ed. St Louis, MO: Mosby Elsevier; 2011. p. 691-719.
- 6. van Wijk AJ, Hoogstraten J. Anxiety and pain during dental injections. J Dent 2009;37:700-704.ArticlePubMed
- 7. van Wijk AJ, Makkes PC. Highly anxious dental patients report more pain during dental injections. Br Dent J 2008;205:E7.ArticlePubMedPDF
- 8. Cho SY, Kim E, Park SH, Roh BD, Lee CY, Lee SJ, Jung IY. Effect of topical anesthesia on pain from needle insertion and injection and its relationship with anxiety in patients awaiting apical surgery: a randomized double-blind clinical trial. J Endod 2017;43:364-369.ArticlePubMed
- 9. Bågesund M, Tabrizi P. Lidocaine 20% patch vs lidocaine 5% gel for topical anaesthesia of oral mucosa. Int J Paediatr Dent 2008;18:452-460.ArticlePubMed
- 10. Weilbach C, Hoppe C, Karst M, Winterhalter M, Raymondos K, Schultz A, Rahe-Meyer N. Effectiveness of various formulations of local anesthetics and additives for topical anesthesia - a prospective, randomized, double-blind, placebo-controlled study. J Pain Res 2017;10:1105-1109.PubMedPMC
- 11. Lee HS. Recent advances in topical anesthesia. J Dent Anesth Pain Med 2016;16:237-244.ArticlePubMedPMCPDF
- 12. Bhalla J, Meechan JG, Lawrence HP, Grad HA, Haas DA. Effect of time on clinical efficacy of topical anesthesia. Anesth Prog 2009;56:36-41.ArticlePubMedPMCPDF
- 13. Sanz R, Calpena AC, Mallandrich M, Clares B. Enhancing topical analgesic administration: review and prospect for transdermal and transbuccal drug delivery systems. Curr Pharm Des 2015;21:2867-2882.ArticlePubMed
- 14. Vickers ER, Punnia-Moorthy A. A clinical evaluation of three topical anaesthetic agents. Aust Dent J 1992;37:266-270.Article
- 15. Humphris GM, Morrison T, Lindsay SJ. The Modified Dental Anxiety Scale: validation and United Kingdom norms. Community Dent Health 1995;12:143-150.PubMed
- 16. Malamed SF. Handbook of local anesthesia-e-book. 7th ed. St Louis, MO: Elsevier Health Sciences; 2019.
- 17. Franz-Montan M, de Paula E, Groppo FC, Silva AL, Ranali J, Volpato MC. Liposomal delivery system for topical anaesthesia of the palatal mucosa. Br J Oral Maxillofac Surg 2012;50:60-64.ArticlePubMed
- 18. Drum M, Reader A, Beck M. Long buccal nerve block injection pain in patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:e51-e54.ArticlePubMed
- 19. Rosa AL, Sverzut CE, Xavier SP, Lavrador MA. Clinical effectiveness of lidocaine and benzocaine for topical anesthesia. Anesth Prog 1999;46:97-99.PubMedPMC
- 20. Svensson P, Petersen JK. Anesthetic effect of EMLA occluded with Orahesive oral bandages on oral mucosa. A placebo-controlled study. Anesth Prog 1992;39:79-82.PubMedPMC
- 21. Kincheloe JE, Mealiea WL Jr, Mattison GD, Seib K. Psychophysical measurement on pain perception after administration of a topical anesthetic. Quintessence Int 1991;22:311-315.PubMed
- 22. de Freiras GC, Pozzobon RT, Blaya DS, Moreira CH. Efficacy of benzocaine 20% topical anesthetic compared to placebo prior to administration of local anesthesia in the oral cavity: a randomized controlled trial. Anesth Prog 2015;62:46-50.ArticlePubMedPMCPDF
- 23. Revill SI, Robinson JO, Rosen M, Hogg MI. The reliability of a linear analogue for evaluating pain. Anaesthesia 1976;31:1191-1198.ArticlePubMed
- 24. McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales: a critical review. Psychol Med 1988;18:1007-1019.ArticlePubMed
- 25. Sharifi R, Salehian S, Sadeghi M, Mozaffari HR. Effect of topical anesthetics on pain during needle insertion of maxillary infiltration anesthesia: a systematic review and meta-analysis study. Sch Acad J Pharm 2017;6:16-26.
- 26. Sharifi R, Nazari H, Bolourchi P, Khazaei S, Parirokh M. The most painful site of maxillary anterior infiltrations. Dent Res J (Isfahan) 2016;13:539-543.ArticlePubMedPMC
- 27. Yonchak T, Reader A, Beck M, Clark K, Meyers WJ. Anesthetic efficacy of infiltrations in mandibular anterior teeth. Anesth Prog 2001;48:55-60.PubMedPMC
- 28. Meechan JG. Intra-oral topical anaesthetics: a review. J Dent 2000;28:3-14.ArticlePubMed
- 29. Daneshkazemi A, Abrisham SM, Daneshkazemi P, Davoudi A. The efficacy of eutectic mixture of local anesthetics as a topical anesthetic agent used for dental procedures: a brief review. Anesth Essays Res 2016;10:383-387.ArticlePubMedPMC
- 30. Yaacob HB, Noor GM, Malek SN. The pharmacological effect of xylocaine topical anaesthetic--a comparison with a placebo. Singapore Dent J 1981;6:55-57.PubMed
- 31. Tunc EP, Firat D, Onur OD, Sar V. Reliability and validity of the Modified Dental Anxiety Scale (MDAS) in a Turkish population. Community Dent Oral Epidemiol 2005;33:357-362.ArticlePubMed
- 32. Humphris GM, Hull P. Do dental anxiety questionnaires raise anxiety in dentally anxious adult patients? A two-wave panel study. Prim Dent Care 2007;14:7-11.ArticlePubMedPDF
- 33. Sghaireen MG, Zwiri AM, Alzoubi IA, Qodceih SM, Al-Omiri MK. Anxiety due to dental treatment and procedures among university students and its correlation with their gender and field of study. Int J Dent 2013;2013:647436.ArticlePubMedPMCPDF
- 34. Dou L, Vanschaayk MM, Zhang Y, Fu X, Ji P, Yang D. The prevalence of dental anxiety and its association with pain and other variables among adult patients with irreversible pulpitis. BMC Oral Health 2018;18:101.ArticlePubMedPMCPDF
- 35. Economou GC. Dental anxiety and personality: investigating the relationship between dental anxiety and self-consciousness. J Dent Educ 2003;67:970-980.ArticlePubMedPDF
- 36. Mehrstedt M, John MT, Tönnies S, Micheelis W. Oral health-related quality of life in patients with dental anxiety. Community Dent Oral Epidemiol 2007;35:357-363.ArticlePubMed
- 37. Neelakantan P, Liu P, Dummer PM, McGrath C. Oral health-related quality of life (OHRQoL) before and after endodontic treatment: a systematic review. Clin Oral Investig 2020;24:25-36.ArticlePubMedPDF
- 38. Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J 2013;58:390-407.ArticlePubMed
- 39. Dou L, Luo J, Yang D. Anaesthetic efficacy of supplemental lingual infiltration of mandibular molars after inferior alveolar nerve block plus buccal infiltration in patients with irreversible pulpitis. Int Endod J 2013;46:660-665.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Rapid local anesthesia in children enhanced by STAR particles: a first-in-humans, randomized clinical trial
Andrew R. Tadros, Mark R. Prausnitz, Eric I. Felner
Drug Delivery and Translational Research.2026; 16(2): 539. CrossRef - Evaluation of Articaine Infiltration Location on the Success Rate of Mandibular Lateral Incisor Anesthesia: A Prospective Crossover Randomized Clinical Trial Study
Alireza Adl, Fahime Alimardani, Fereshte Sobhnamayan
Journal of Endodontics.2026; 52(2): 175. CrossRef - Comparison of topical ethyl chloride spray and subcutaneous 1% mepivacaine for local anesthesia in single-rod etonogestrel implant insertion: an observational study
Rosana Garrido-Santamaría, Jesús Martínez-Tofé, Noelia Navas-Echazarreta, Antonio Rodríguez-Calvo, Michał Czapla, Ignacio Larrayoz-Roldán, Raúl Juárez-Vela, Antonio Martinez-Sabater, Regina Ruiz De Viñaspre-Hernandez
Frontiers in Medicine.2026;[Epub] CrossRef - The Case for Transdermal Lidocaine 7.5% in the Management of Localized Pain: A Biopharmaceutical Review
Alexandra LaStella
Scriptum Pharmacologia .2025;[Epub] CrossRef - A Framework for the Modulation and Alleviation of Pain Sensations: A Narrative Review
Rushita Dobariya, Niraj Kinariwala, Nirav Parekh, Dhruvi Gangani, Devshree Dave, Hasti Maru, Nandani Mangukiya, Siddhi Singh
Cureus.2025;[Epub] CrossRef - Phacoemulsification Techniques and Their Effects on Corneal Endothelial Cells and Visual Acuity: A Review of "Direct-Chop" and "Stop-and-Chop" Approaches Under Topical Anesthesia
Devwrath Upasani, Sachin Daigavane
Cureus.2024;[Epub] CrossRef - Local anaesthetics in pediatric dental practice (literature review)
E. V. Ekimov, G. I. Skripkina, A. Zh. Garifullina, N. V. Chumichkin
Pediatric dentistry and dental prophylaxis.2023; 23(3): 211. CrossRef
 ePub Link
ePub Link Cite
CiteEffects of different topical anesthetics on pain from needle insertion and injection, and the influence of anxiety in patients awaiting endodontic treatment
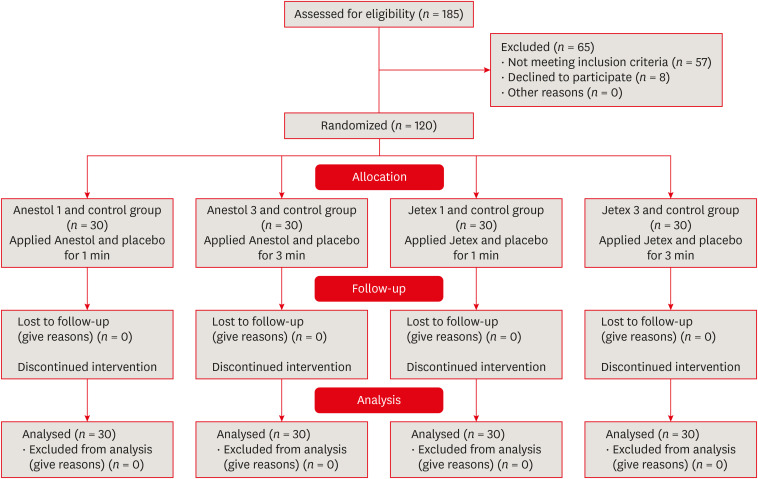
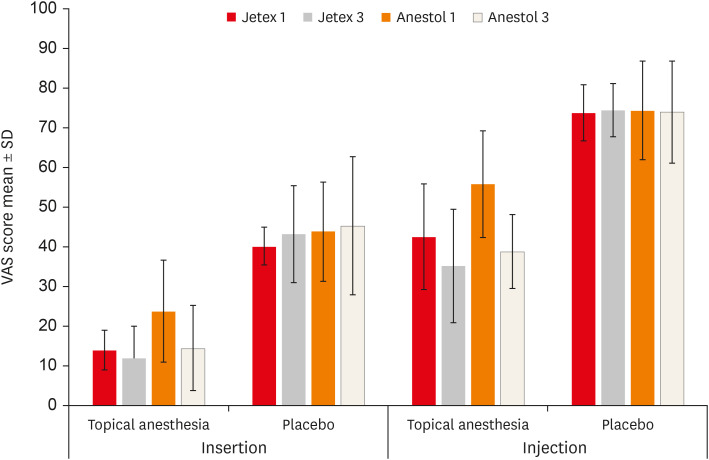
Figure 1 PRIRATE 2010 flowchart.
Figure 2 The needle insertion and injection VAS scores of the groups.VAS, Visual Analog Scale; SD, standard deviation.
Figure 1
Figure 2
Effects of different topical anesthetics on pain from needle insertion and injection, and the influence of anxiety in patients awaiting endodontic treatment
Demographic data of the patients; MDAS scores of the all groups
| Demographic data | G2 ( | G4 ( | G1 ( | G3 ( | Total ( | ||
|---|---|---|---|---|---|---|---|
| Age (yr) | 38.30 ± 12.77 | 38.63 ± 10.04 | 37.57 ± 12.84 | 37.60 ± 12.86 | 38.03 ± 12.06 | 0.959*a | |
| Sex (M/F) | 17/13 (56.7/43.3) | 14/16 (46.7/53.3) | 13/17 (43.3/56.7) | 17/13 (56.7/43.3) | 61/59 (50.8/49.2) | 0.698*b | |
| MDAS score | 12.17 ± 2.57 | 12.23 ± 2.76 | 12.13 ± 4.20 | 12.27 ± 3.62 | 0.970*a | ||
| ≥ 12 | 15 | 14 | 18 | 14 | 59 (49.2) | 0.637*b | |
| < 12 | 15 | 16 | 12 | 16 | 61 (50.8) | ||
Values are presented as number (%) or mean ± standard deviation.
MDAS, Modified Dental Anxiety Scale.
*
aKruskal-Wallis variance analysis; bChi-square test.
Comparison of Visual Analog Scale scores (mm) between placebo and anesthesia after both the needle insertion and injection in all group
| Group | G2 (1) | G4 (2) | G1 (3) | G3 (4) | Intergroup | |
|---|---|---|---|---|---|---|
| Insertion | ||||||
| Topical anesthesia | 14.00 ± 5.02 | 11.93 ± 8.17 | 23.80 ± 12.89 | 14.50 ± 10.71 | 0.0001*a (2–3, 3–4, 1–3) | |
| Placebo | 40.20 ± 4.79 | 43.20 ± 12.21 | 43.90 ± 12.47 | 45.30 ± 17.42 | 0.752a | |
| In-group | 0.0001*f | 0.0001*e | 0.0001*f | 0.0001*f | ||
| Injection | ||||||
| Topical anesthesia | 42.53 ± 13.35 | 35.23 ± 14.3 | 55.8 ± 13.44 | 38.83 ± 9.31 | 0.0001*a (2–3, 3–4, 1–3) | |
| Placebo | 73.77 ± 7.11 | 74.53 ± 6.71 | 74.43 ± 12.4 | 73.97 ± 12.87 | 0.960a | |
| In-group | 0.0001*f | 0.0001*e | 0.0001*e | 0.0001*f | ||
Values are expressed as mean ± standard deviation.
*
aKruskal-Wallis variance analysis; ePaired samples
Comparison of the Visual Analog Scale scores according to Modified Dental Anxiety Scale anxiety levels in all group
| Group | Anxiety | Intergroup | |||
|---|---|---|---|---|---|
| < 12 | ≥ 12 | ||||
| G2 | |||||
| Insertion | |||||
| Topical anesthesia | 14.07 ± 5.86 | 13.93 ± 4.23 | 0.775d | ||
| Placebo | 39.6 ± 4.79 | 40.8 ± 4.87 | 0.539d | ||
| In-group | 0.001*f | 0.0001*e | |||
| Injection | |||||
| Topical anesthesia | 38.67 ± 14.65 | 46.40 ± 11.06 | 0.187d | ||
| Placebo | 70.07 ± 6.17 | 77.47 ± 6.10 | 0.003*d | ||
| In-group | 0.001*f | 0.0001*e | |||
| G4 | |||||
| Insertion | |||||
| Topical anesthesia | 11.56 ± 5.21 | 12.36 ± 10.82 | 0.423d | ||
| Placebo | 40.25 ± 7.79 | 46.57 ± 15.48 | 0.294d | ||
| In-group | 0.0001*e | 0.0001*e | |||
| Injection | |||||
| Topical anesthesia | 33.75 ± 7.80 | 36.93 ± 19.50 | 0.886d | ||
| Placebo | 71.31 ± 4.19 | 78.21 ± 7.27 | 0.003*c | ||
| In-group | 0.0001*e | 0.0001*e | |||
| G1 | |||||
| Insertion | |||||
| Topical anesthesia | 17.17 ± 11.53 | 28.22 ± 12.06 | 0.022*d | ||
| Placebo | 36.17 ± 8.57 | 49.06 ± 12.15 | 0.003*d | ||
| In-group | 0.0001*e | 0.0001*e | |||
| Injection | |||||
| Topical anesthetic | 50.08 ± 14.11 | 59.61 ± 11.88 | 0.072d | ||
| Placebo | 65.83 ± 12.28 | 80.17 ± 8.82 | 0.001*d | ||
| In-group | 0.004*e | 0.0001*e | |||
| G3 | |||||
| Insertion | |||||
| Topical anesthesia | 11.06 ± 6.21 | 18.43 ± 13.43 | 0.334d | ||
| Placebo | 44.19 ± 16.8 | 46.57 ± 18.65 | 0.715c | ||
| In-group | 0.0001*e | 0.001*f | |||
| Injection | |||||
| Topical anesthesia | 39.38 ± 6.95 | 38.21 ± 11.71 | 0.728d | ||
| Placebo | 67.69 ± 10.74 | 81.14 ± 11.51 | 0.001*d | ||
| In-group | 0.0001*e | 0.001*f | |||
Values are expressed as mean ± standard deviation.
*
cIndependent samples
Table 1 Demographic data of the patients; MDAS scores of the all groups
Values are presented as number (%) or mean ± standard deviation.
MDAS, Modified Dental Anxiety Scale.
*
aKruskal-Wallis variance analysis; bChi-square test.
Table 2 Comparison of Visual Analog Scale scores (mm) between placebo and anesthesia after both the needle insertion and injection in all group
Values are expressed as mean ± standard deviation.
*
aKruskal-Wallis variance analysis; ePaired samples
Table 3 Comparison of the Visual Analog Scale scores according to Modified Dental Anxiety Scale anxiety levels in all group
Values are expressed as mean ± standard deviation.
*
cIndependent samples

