In-vitro assessment of geometric characteristics in canal preparation using nickel-titanium files used for minimal invasiveness: an experimental study
Article information

Abstract
Objectives
This study aimed to assess geometric characteristics in canal preparation using nickel-titanium (NiTi) files used for minimal invasiveness.
Methods
Thirty J-shaped simulated canals in resin blocks were instrumented with either TruNatomy (TR; Dentsply Sirona), EndoRoad (ER; Maruchi), or ProTaper Ultimate (PTU; Dentsply Sirona). The simulated canal blocks were scanned using microcomputed tomography before and after instrumentation. The scanned images were reconstructed, and the canal surface area was measured from 0.5 to 6.5 mm from the apex. Three-dimensional representative models of each group were rendered. The data were statistically analyzed using one-way analysis of variance and Kruskal-Wallis test at 95% significance level.
Results
TR showed a superior ability to maintain the canal’s center. TR demonstrated comparable apical preparation to PTU. ER showed a smaller and limited apical preparation than other systems, with a tendency for canal preparation toward the inner side of the curvature. PTU featured the largest prepared apical size among the file groups and tended to straighten the curvature by preparing the canal more towards the outward side. The surface area instrumented using each NiTi file showed statistically significant differences among the three groups at all levels except 0.5, 2.0, and 3.5 mm from the apex (p < 0.05). There was no statistically significant difference between TR and PTU at a level of 0.5 mm from the apex (p > 0.05).
Conclusions
While PTU is suitable for general canal preparation to facilitate irrigation and intracanal medication, TR and ER excel in preserving canal centering with minimal concern for canal transportation by minimally invasive preparation.
INTRODUCTION
Proper cleaning and shaping of the root canal system are fundamental aspects of successful endodontic treatment. The primary goal of root canal preparation is to eliminate microorganisms, necrotic tissue, and infected dentin that may lead to pulp and periapical infections [1]. Nickel-titanium (NiTi) instruments have revolutionized root canal preparation due to their unique metallurgical properties, including superelasticity and shape memory, offering superior performance compared to traditional stainless-steel files while minimizing preparation-related complications such as canal transportation, ledge or zip formation, and other aberrations [2]. Recent generations of heat-treated NiTi instruments exhibit increased flexibility, fatigue resistance, and improved canal centering, allowing effective cleaning and shaping with minimal deviation from the original canal anatomy [3].
Current trends in endodontics emphasize a conservative approach to treatment. Modern advancements such as dental operating microscopes, ultrasonic instruments, heat-treated NiTi files, and supplemental irrigating systems have contributed to the shift toward minimally invasive endodontics (MIE). In this context, a conservative treatment approach refers to preserving pericervical and radicular dentin through conservative access cavity design, anatomically centered canal preparation with minimal taper enlargement, and reliance on enhanced irrigation and disinfection rather than excessive mechanical instrumentation [3,4]. MIE aims to preserve tooth structure, enhancing the long-term prognosis of endodontically treated teeth [3,4].
NiTi files with reduced taper and shaft diameter enable effective apical canal enlargement while minimizing file stress and reducing debris extrusion [5]. These design modifications allow for efficient preparation and disinfection up to the apical region without compromising the integrity of the canal or increasing the risk of procedural errors [6].
A critical consideration in assessing file performance is the ability to maintain the instrument’s central positioning within the canal, minimizing canal transportation. Especially, the instrumentation of the apical region is considered an essential component for achieving thorough cleaning and shaping. When considering transportation and apical preparation, it is challenging to determine which is more crucial, as there is a potential for conflicting aspects between these two values [2,7].
Manufacturers develop instrument systems to apply the MIE concept to mechanical shaping procedures. Among them, the TruNatomy rotary system (Dentsply Sirona, Ballaigues, Switzerland) features heat-treated instruments with an off-centered rectangular cross-section, regressive taper, and a maximum fluted diameter of 0.8 mm. The instruments have variable tapers, ranging from 0.02 for larger instruments to 0.04 for smaller ones. Previous studies highlight its high cyclic fatigue resistance and ability to preserve the original canal anatomy, attributed to enhanced flexibility from advanced heat treatment during the post-manufacturing process [4,8].
The ProTaper Ultimate (PTU) rotary system (Dentsply Sirona) is the latest addition to this kind of instrument system, utilizing a specialized heat treatment technology to achieve optimal flexibility and strength. Its parallelogram cross-section with distinctive acute angles, a partially off-centered design, and a maximal flute diameter of 1.0 mm allows for conservative dentin removal in critical areas, such as the cementoenamel junction [9,10].
The EndoRoad file system (Maruchi, Wonju, Korea) incorporates an innovative heat treatment known as “memory-triple heat treatment.” This process induces the R-phase within the range of body temperature. This leads to a symmetric presence of the R-phase at body temperature, yielding a substantial enhancement in flexibility and cyclic fatigue resistance of the files compared to earlier heat treatment technologies [11,12].
However, despite these advancements, the efficacy and geometric characteristics of these modern NiTi files during canal preparation remain inadequately studied.
The objective of this study was to evaluate the geometric characteristics of canal preparation using three NiTi file systems designed for the minimal invasiveness concept. The null hypothesis was that there would be no significant differences in canal preparation among the tested file systems.
METHODS
The flow of this study is summarized in Figure 1. A total of 30 simulated J-shaped root canals in transparent resin blocks (Dentsply Sirona) were used in this study. Each resin block measured 16 mm in length, with a curvature radius of 3.5 mm and an angle of 53º, as measured according to the method described by Pruett et al. [13]. The point of maximum flexure was located 3.5 mm from the apical end, and the apical foramen communicated with the exterior of the resin block.
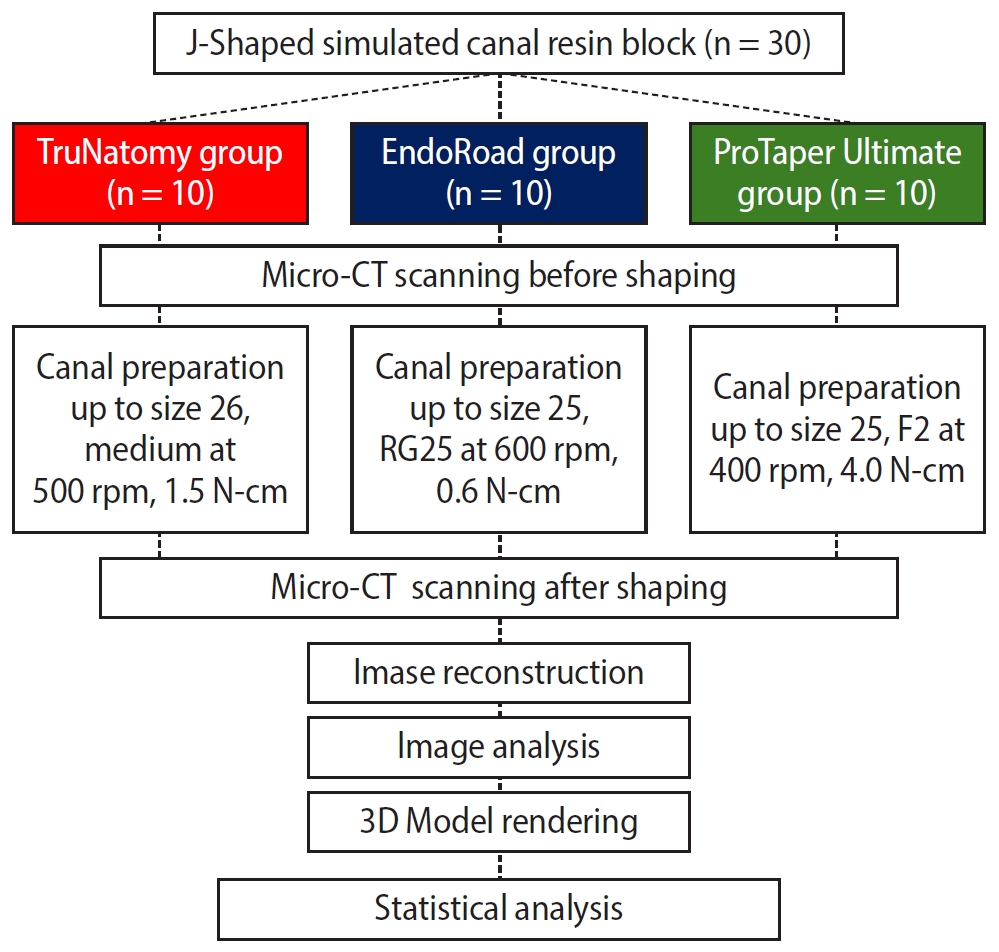
Experimental flow of this study. Micro-CT, micro-computed tomography; 3D, three-dimensional. TruNatomy: Dentsply Sirona, Ballaigues, Switzerland. ProTaper Ultimate: Dentsply Sirona. EndoRoad: Maruchi, Wonju, Korea.
Group designation and Specimen preparation
The specimens were divided into three groups (n = 10 per group). The sample size was determined using pilot data from a preliminary micro-CT analysis and G*Power 3.1.9.2 software (Heinrich-Heine-Universität Düsseldorf, Germany), with an α level of 0.05 and a power of 0.80. This analysis indicated that a minimum of nine specimens per group would be required to detect significant differences in canal geometry among the file systems; therefore, 10 specimens per group were used in the present study. This sample size is also in line with a previous micro-CT study evaluating canal shaping outcomes using standardized models [7].
All canal preparations were performed by a single experienced operator (over 6-year experienced postgraduate student). The preparation followed the instructions of the manufacturer with minor modifications where unnecessary steps were omitted, are omitted. The final instrumentation size of all systems was standardized to approximately #25.
1. TruNatomy group (n = 10)
Working length was measured using a #10 K file, and patency was confirmed. Instrumentation was performed with the TruNatomy system at a speed of 500 rpm and a torque setting of 1.5 N•cm. All instrumentation was performed in the presence of a lubricant (RC prep; Premier Dental, Plymouth Meeting, PA, USA). Initial instrumentation was performed using the TruNatomy Glider file (#17/.02) until the working length was reached. The canal was irrigated with saline, and patency was reconfirmed. As the simulated canal is made of resin material, there was no organic tissue, bacteria, or dentinal tubules. So, only saline was used to clean out the resin debris after instrumentation. Final instrumentation was performed using the TruNatomy Prime file (#26/.04) to the working length. Irrigation with saline and patency checks were repeated throughout the process.
2. ProTaper Ultimate group (n = 10)
Working length was measured with a #10 K file, and patency was confirmed. Instrumentation was performed with the PTU system at a speed of 400 rpm and a torque setting of 4.0 N•cm. The same lubricant was used during all steps. Initial instrumentation was performed with the PTU Slider file (#16/.02v) to confirm the patency. The same saline irrigation protocol was used, followed by the instrumentation with the PTU Shaper file (#20/.04v), with the patency maintained. The instrumentation process continued with the PTU F1 file (#20/.07v) and, subsequently, the PTU F2 file (#25/.08v), both to the working length. The working length was maintained throughout instrumentation. Saline irrigation and patency checks were repeated at each step.
3. EndoRoad group (n = 10)
Working length was measured with a #10 K file, and patency was confirmed. Instrumentation was performed with the EndoRoad system at a speed of 600 rpm and a torque setting of 0.6 N•cm. The same lubricant was used during all steps. Initial instrumentation was performed using the EndoRoad RP15 file (#15/.02) to confirm the patency. The canal was irrigated with saline, followed by instrumentation with the EndoRoad RP20 file (#15/.03) until the patency was confirmed. Final instrumentation was performed using the EndoRoad RG25 file (#25, variable taper of 0.6 at less than 3 mm from the tip, and 0.2 at more than 3 mm from the tip) to the working length. Saline irrigation and patency checks were repeated throughout the process.
Before the experimental tests, all instruments were inspected under a dental operating microscope to confirm the absence of deformation, unwinding, or other defects. All files used in this study for canal preparation showed a normal morphology.
Micro-computed tomography scanning and three-dimensional reconstruction
The resin blocks were scanned before and after canal instrumentation using a micro-computed tomography (micro-CT, SkyScan 1273; Bruker micro-CT, Kontich, Belgium). Each specimen was secured in a cylindrical holder using Parafilm (Sigma-Aldrich, St. Louis, MO, USA), with the access cavity positioned at the top. The holder was placed in the micro-CT scanner, where parameters, file prefixes, and data directories were manually configured. Scanning was conducted individually for each specimen, with 21 minutes and 46 seconds per scan, at 70 kV, 214 μA, with 360° rotation and a 0.3° rotation step. The scans produced images with a voxel size of 24 μm.
Image reconstruction was performed using NRecon software (Bruker micro-CT, ver. 1.7.4.2) with beam hardening correction set at 40% and ring artifact correction at 1, generating 972 cross-sectional images per specimen. The reconstructed datasets were coregistered using DataViewer software (ver. 1.5.6.2, Bruker micro-CT). CTAn software (ver. 1.18.4.1, Bruker micro-CT) was employed to measure the cross-sectional areas of canals. Using CTvol software (ver. 2.3.2.0, Bruker micro-CT), three-dimensional (3D) models of the canals before and after instrumentation were rendered to evaluate the geometrical characteristics of the prepared canals.
Canal levels from 0.5 mm to 6.5 mm from the apex were subdivided into increments of 1.0 mm. The cross-sectional surface areas (mm2) were measured at the seven levels at each 1-mm incremental level from 0.5 mm to 6.5 mm.
Statistical analysis
The Shapiro-Wilk test was used to assess the normality of the data distribution for all three groups at each measurement level. When the assumptions of normality and homogeneity of variance were satisfied, one-way analysis of variance was used to determine significant differences among the groups, followed by appropriate post hoc pairwise comparisons with Bonferroni adjustment. For data that did not meet normality assumptions, the nonparametric Kruskal-Wallis test was applied instead. All statistical analyses were performed using IBM SPSS Statistics software (ver. 26; IBM Corp., Armonk, NY, USA), with a confidence interval of 95% and a significance level set at 0.05.
RESULTS
During instrumentation, no procedural complications, such as instrument fracture, loss of working length, or ledge formation, were observed in any specimen.
In the 3D models, the TruNatomy group showed superior ability in maintaining the center of the canal (Figure 2). The TruNatomy group also demonstrated comparable apical preparation to that of the PTU group. The EndoRoad group, in contrast, showed a more limited apical preparation compared to the other NiTi file systems, with a tendency for canal preparation toward the inner side of the canal curvature (Figure 2). However, this tendency was consistent and presented with minimal aberrations. The PTU group featured the largest apical preparation among the file groups, with a notable tendency to straighten the canal curvature by preparing more toward the outward side.
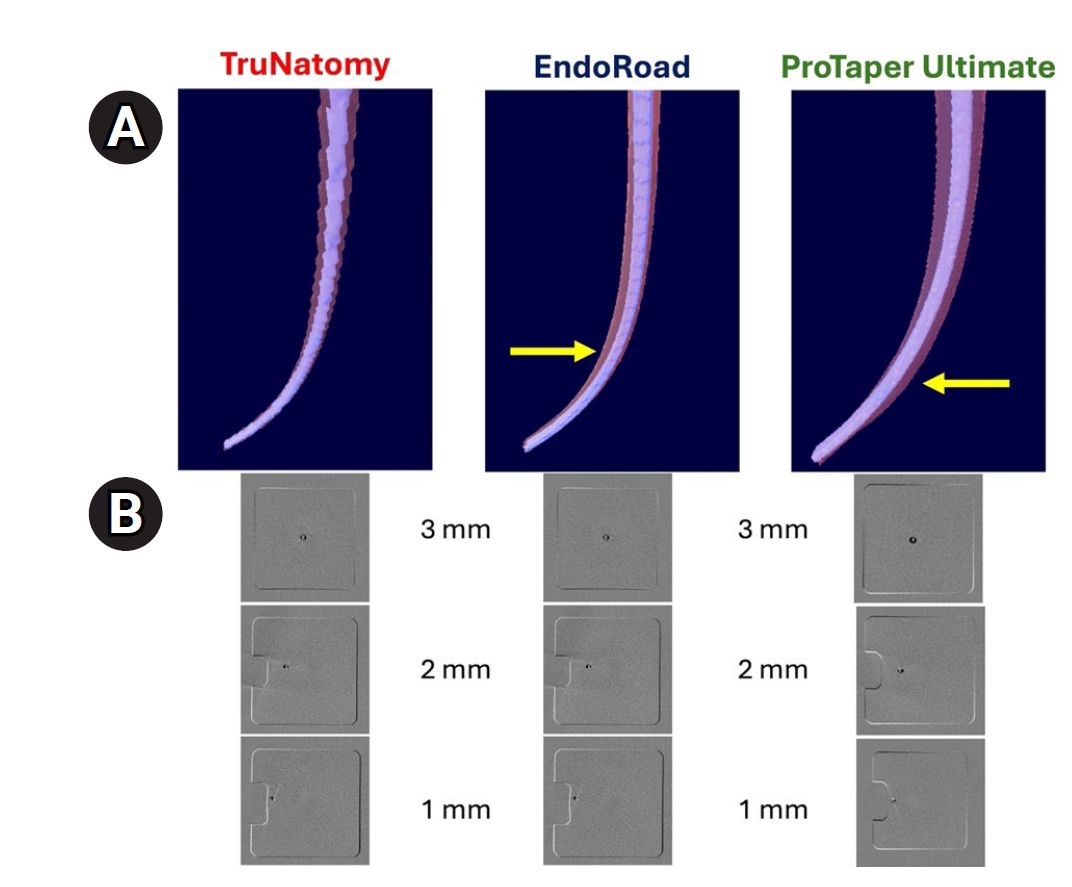
Representative superimposed images show maintaining the center of the canals after instrumentation. (A) Longitudinal superimposed images. The EndoRoad group shows inner side deviation to the canal curvature, while the ProTaper Ultimate group shows outward side deviation apically (yellow arrows). (B) Cross-sectional superimposed images at the 1 mm, 2 mm, and 3 mm levels. TruNatomy: Dentsply Sirona, Ballaigues, Switzerland. ProTaper Ultimate: Dentsply Sirona. EndoRoad: Maruchi, Wonju, Korea.
Statistical analysis of the instrumented surface area revealed differences among the three groups at all levels (Figure 3), except at 0.5 mm, 2.0 mm, and 3.5 mm from the apex. The PTU group shows much bigger areas than other groups at all levels, while the EndoRoad group shows generally a smaller surface area, especially over the 3.5 mm level. The TruNatomy group shows a significantly larger area at the 1 mm level. In comparison, there was no difference between the TruNatomy and EndoRoad groups at 2.0 mm and 3.5 mm levels from the apex.
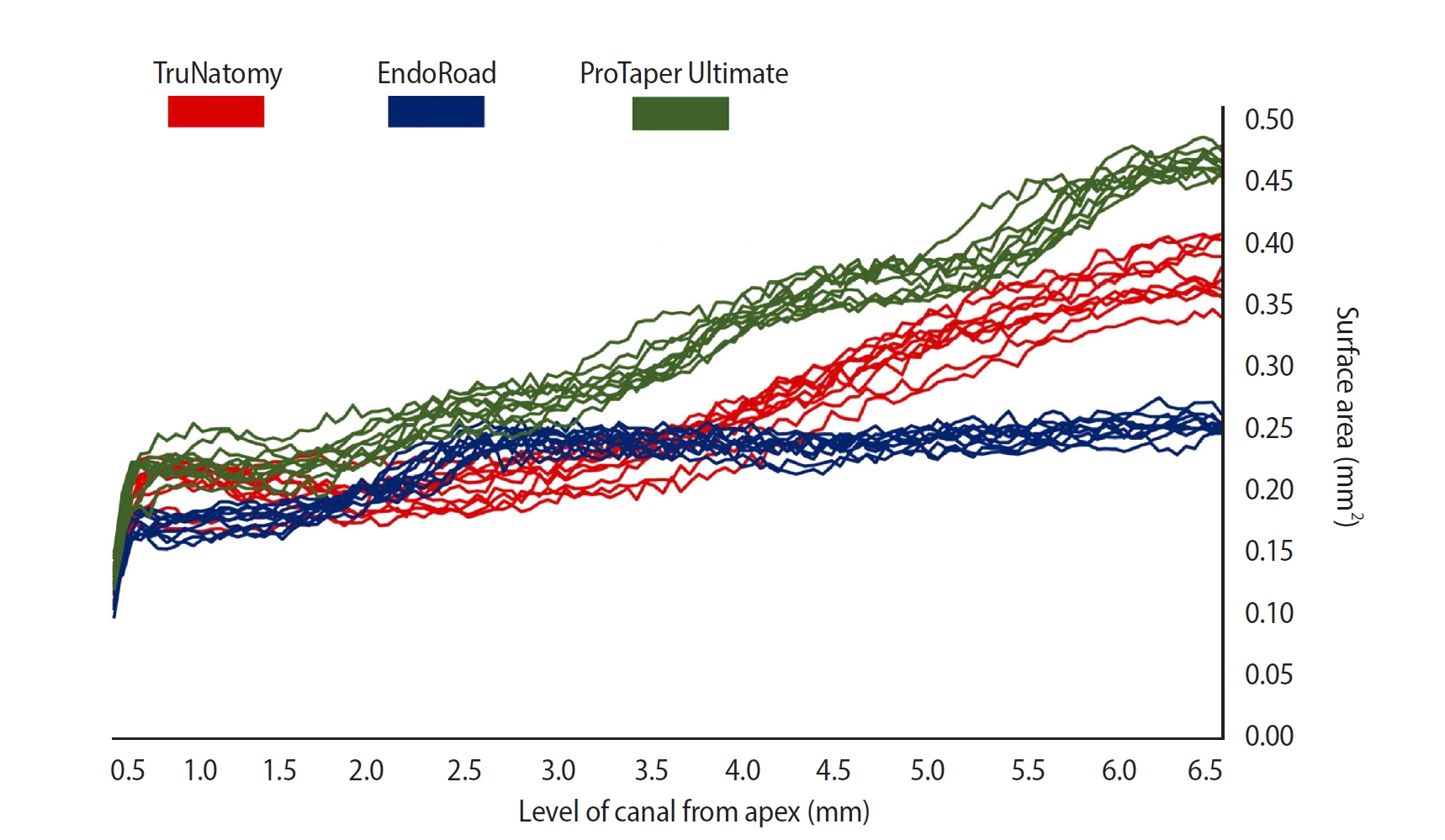
Line graphs of the instrumented surface areas for all specimens of the three groups at levels from 0.5 mm to 6.5 mm from the apex. The ProTaper Ultimate group (green) shows much bigger areas than other groups in all levels, while the EndoRoad group (blue) shows generally a smaller surface area, especially over the 3.5 mm level. The TruNatomy group (red) shows a significantly larger area at the 1 mm level (p < 0.05). In comparison, there was no difference between the TruNatomy and EndoRoad groups at 2.0 mm and 3.5 mm levels from the apex. TruNatomy: Dentsply Sirona, Ballaigues, Switzerland. ProTaper Ultimate: Dentsply Sirona. EndoRoad: Maruchi, Wonju, Korea.
All groups show significant differences among the groups at the 1 mm and 3 mm levels (p < 0.05, Figure 4). The PTU group shows significantly bigger areas than the other groups at the 2 mm level (p < 0.05). The TruNatomy and EndoRoad groups do not have a significant difference. All groups show significant differences among the groups at the 1 mm level (p < 0.05).
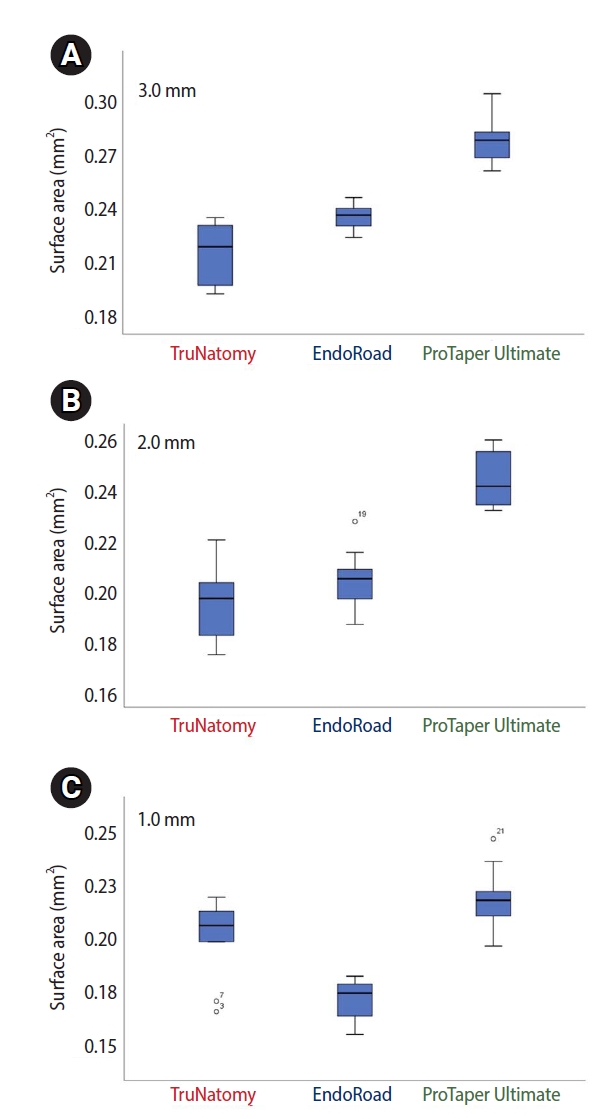
Instrumented surface areas at three levels. (A) All groups show significant differences among the groups at the 1 mm and 3 mm levels. (B) The ProTaper Ultimate group shows significantly bigger areas than the other groups at the 2 mm level. TruNatomy and EndoRoad do not have a significant difference. (C) All groups show significant differences among the groups at the 1 mm level. TruNatomy: Dentsply Sirona, Ballaigues, Switzerland. ProTaper Ultimate: Dentsply Sirona. EndoRoad: Maruchi, Wonju, Korea.
DISCUSSION
This study evaluated the geometric characteristics of canal preparation using three NiTi file systems designed according to the MIE concept. A designated file from each system was selected to standardize the apical tip ISO size of #25 (EndoRoad RG25 file and PTU F2) and #26 (TruNatomy Prime file). It might initially seem that the TruNatomy file, with its slender and narrow appearance, would result in insufficient canal preparation. However, the results showed that the instrumented area at the apical 0.5–3.0 mm prepared with the TruNatomy Prime file was comparable to that of the PTU F2 file [8,9].
The TruNatomy system was originally designed to achieve minimally invasive canal preparation and to preserve a larger portion of the tooth structure, particularly the root dentine [8,9]. The findings of this study partially support this concept, as the canal preparation in the coronal 3.0–6.5 mm region with the TruNatomy file was more limited compared to the larger-taper PTU file system. However, this minimal preparation could raise concerns about the prognosis of the overall treatment, as restricted canal shaping may reduce the accessibility of irrigants and intracanal medicaments. Despite these concerns, the results demonstrated that apical preparation from 0.5 mm to 3.0 mm using the TruNatomy file was comparable to that achieved by the PTU file. This suggests that the core function of instrumentation—removing debris and microorganisms—was not compromised, even with this smaller and more conservative file system [8,9,14,15].
Although the tip size (approximately #25) of the three NiTi file systems was standardized, the cross-sectional areas changed from 0.5 to 6.5 mm from the apex and differed significantly among the systems. The key characteristics of each file system can be summarized as follows: TruNatomy demonstrated apical preparation comparable to PTU, highlighting its effectiveness in shaping the apical region. PTU exhibited the most extensive preparation among the three groups, reflecting its large taper design. EndoRoad showed relatively limited apical preparation compared to the other systems; however, its low standard deviation indicated a consistent preparation trend across specimens [8,9].
Schilder [16] proposed that the final preparation should have a continuous taper with the smallest possible apical foramen. Similarly, Buchanan [17] suggested that apical preparation should be performed to the minimum size possible. However, current instrumentation and irrigation techniques remain insufficient for the complete elimination of debris and bacteria in the apical third [18]. The challenge of removing bacterial debris from this region is attributed to the narrow canal space, complex canal morphology, inadequate irrigant flushing, and variations in the diameter of the root canal [6]. Thus, the debate regarding the optimal extent of apical enlargement for successful endodontic treatment remains unresolved. Although randomized controlled trials are considered the gold standard in clinical research, no such study has been conducted in this regard to date.
The concept of significant apical enlargement is based on the premise that increasing the apical diameter enhances canal debridement [19]. This is justified by evidence that microorganisms can penetrate dentinal tubules to depths of 200–300 μm, where they are difficult to eliminate using conventional methods [20]. Studies by Falk and Sedgley [21] have demonstrated that larger apical preparation improves the efficacy of irrigation solutions and reduces bacterial growth in the apical region. Similarly, Brunson et al. [22] reported that larger apical preparation increases the volume of irrigation solution reaching the apical third, enhancing the removal of tissue debris.
Additionally, Fornari et al. [23] and Plotino et al. [24] observed that apical enlargement reduces the non-instrumented areas within the root canal, potentially improving overall cleanliness. Conversely, a study by Coldero et al. [25] found no significant difference in intracanal bacterial reduction with or without apical enlargement preparation. It concluded that removing additional dentine from the apical region is unnecessary when an adequate coronal taper is achieved, as this facilitates effective irrigation throughout the root canal system. Thus, apical enlargement remains controversial to date, and no study has ever shown a direct relationship between apical enlargement and clinical success or failure in endodontic treatment. Additionally, apical enlargement carries several drawbacks, including the risk of canal transportation, weakening of the root structure, and potential over-preparation of the canal [26].
Transportation is defined as the removal of the canal wall structure on the outer curve of the apical half of the canal. This occurs due to the natural tendency of files to return to their original linear shape during canal preparation, potentially resulting in ledge formation or even perforation [2]. Therefore, a more comprehensive definition of root canal transportation describes it as the deviation of the post-instrumentation canal center from its original position compared to the pre-instrumentation canal center.
Canal transportation during instrumentation most commonly occurs at different levels depending on the degree of root canal curvature. As a deviation of the prepared canal from its original path, root canal transportation is a critical factor influencing treatment outcomes [2,27]. Consequently, evaluating the ability of endodontic instruments to remain centered within the canal while minimizing iatrogenic defects is essential.
While small-tapered instruments are commonly believed to possess greater flexibility, allowing them to maintain the original axial direction of the root canal more effectively, recent studies using proper 3D analysis with micro-CT technology have demonstrated comparable canal transportation levels between the XP-endo Shaper (FKG Dentaire) and other systems in mesial canals of mandibular molars [27]. Previous meta-analysis research on the centering ability of NiTi instruments has identified the shaft taper as a significant factor influencing canal transportation. emphasizing the importance of taper selection in minimizing this issue during canal preparation [28].
This study utilized resin blocks simulating root canals as experimental samples, providing advantages and limitations. Using simulated root canals with standardized shapes and dimensions, such as round cross-sections, continuous tapers, and uniform sizes, allows for high reproducibility and a controlled environment to evaluate various instrumentation techniques. One of the primary benefits of using simulated resin blocks is the ability to visualize how canal preparation progresses during instrumentation. This feature is particularly valuable for assessing shaping outcomes, including apical stop formation, taper consistency, and the presence of aberrations such as zips, elbows, or perforations. Additionally, the high degree of standardization in simulated canal block anatomy eliminates anatomical variability, enabling researchers to focus solely on the performance of the instruments under investigation. Such evaluations provide insights into the efficacy and safety of different file systems under controlled conditions [29,30].
Despite their advantages, simulated resin block models have several significant limitations. One major drawback is their inability to evaluate root canal cleanliness, as the resin material does not replicate the biological presence of pulp tissue, debris, or microbial contamination. Moreover, the mechanical properties of resin differ substantially from those of human dentin, requiring lower forces for instrumentation and potentially underestimating straightening and the incidence of preparation errors, such as ledging or outer widening [30-32]. This discrepancy leads to differences in the forces required for instrumentation, with human dentin requiring approximately twice the force for preparation compared to resin blocks. While resin block models offer valuable insights into instrumentation performance, the results must be interpreted cautiously when extrapolating findings to clinical practice. The simplified anatomy and reduced hardness of resin blocks may underestimate the challenges of preparing natural root canals. Therefore, the findings of this study should be regarded as comparative data obtained under highly standardized in vitro conditions rather than as direct predictors of clinical outcomes.
In the present study, the primary objective was to compare subtle differences in shaping behavior and canal geometry among three NiTi file systems designed for MIE. To achieve this aim, it was essential to minimize anatomical variability and confounding factors. Simulated canals in resin blocks with identical curvature, length, and canal diameter were therefore selected, as they provide a highly standardized experimental environment in which the effects of the instruments themselves can be isolated more reliably. While this choice inevitably limits the direct clinical extrapolation of our results, it strengthens the internal validity of the comparison among the three systems.
This study used micro-CT technology, and this imaging technique enables noninvasive, nondestructive, and high-resolution 3D assessments, offering unparalleled insights into various aspects of canal instrumentation. Micro-CT provides the ability to precisely analyze the changes in root canal volume, monitoring changes in the structural integrity of the canal walls [7,32]. Especially as in this study, the assessment of shaping performance and maintaining the original anatomy would be effective. As a result, micro-CT findings are reliable only within experiments conducted under identical conditions and parameter settings.
CONCLUSIONS
Based on the results from the present study, the PTU would be an ideal selection when extensive canal preparation is needed to create sufficient space for irrigation and intracanal medication, with a low tendency for canal transportation under the conditions of this study. TruNatomy seems proper for maintaining canal centering, particularly in severely curved canals, with comparable apical preparation to that of PTU. EndoRoad is a reliable choice for negotiating highly calcified canals, enabling minimal preparation and glide path establishment with reduced risk of procedural accidents.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING/SUPPORT
This study was supported by the SNUDH Research Fund (grant No. 04-2022-0121).
AUTHOR CONTRIBUTIONS
Conceptualization, Funding acquisition, Supervision, Project administration: Lee W. Data curation, Software: Jang E. Formal analysis: Jang E, Lee W. Investigation, Visualization: Jang E, Kim HC. Methodology, Validation: Kim HC, Lee W. Writing - original draft: Jang E. Writing - review & editing: Kim HC, Lee W. All authors read and approved the final manuscript.
DATA SHARING STATEMENT
The datasets are not publicly available but are available from the corresponding author upon reasonable request.