Effectiveness of silver diamine fluoride in managing hypersensitivity of molar-incisor hypomineralization affected molars: a scoping review
Article information

Abstract
Objectives
This study aimed to evaluate the efficacy of dentinal hypersensitivity treatment with silver diamine fluoride (SDF) in molar-incisor hypomineralization (MIH)-affected molars.
Methods
This scoping review was designed and structured according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses and its extension for scoping reviews. A search strategy was conducted across PubMed, The Cochrane Library, ScienceDirect, and Google Scholar to identify articles related to the topic. Two authors screened titles, abstracts, and full texts for review.
Results
Five studies met the eligibility criteria, comprising four randomized controlled trials and one case report, with sample sizes ranging from four to 200 participants. All included studies reported improvements in clinical outcomes, including reduced hypersensitivity following SDF application, as indicated by lower Schiff cold air sensitivity scale scores.
Conclusions
SDF is a promising treatment strategy for reducing hypersensitivity in MIH-affected molars; however, further research using SDF alone is needed to evaluate its exact effectiveness.
INTRODUCTION
The first study regarding molar-incisor hypomineralization (MIH) was reported in the late 1970s. However, the first official definition of MIH was established in 2001 by Weerheijm [1] as a systemic-origin syndrome presenting as demarcated, qualitative enamel defects in one to four first permanent molars (FPMs), frequently associated with affected incisors.
Clinically, MIH lesions are demarcated as creamy white to yellow-brown defects, occasionally accompanied by surface enamel breakdown [1–3]. The enamel of MIH-affected teeth is often porous like “pollen” with a 15 times higher proportion of amelogenin proteins, reducing mechanical properties, hardness, and elastic modulus compared to normal teeth, which could contribute to its inability to withstand the forces encountered during mastication [4,5], and leading to post-eruptive enamel breakdown (PEB) that could lead to early exposure of porous subsurface enamel or dentine and exacerbate hypersensitivity [6,7]. As a result, the prevalence of patients who experienced frequent hypersensitivity due to MIH-affected molars was relatively high [6], and the need to manage hypersensitivity among this population was rising [8].
The hydrodynamic theory of dentin hypersensitivity, proposed by Brännström [9], posits that “stimuli like cold, heat, or pressure cause fluid movement within exposed dentinal tubules, activating nerve endings and resulting in pain”. The often-exposed dentinal tubules, especially in MIH-affected teeth, can lead to pain and prolonged dentin sensitivity when exposed to hot or cold foods or to mechanical stimulation [7,10]. Efforts to overcome dentin hypersensitivity over the decades have agreed on two mechanisms to reduce dentin hypersensitivity, which are (1) disruption of nerve impulse transmission, and (2) occlusion of the exposed dentinal tubules [11,12].
Silver diamine fluoride (SDF) is a colorless preparation of Ag+ ions and fluoride (F–), forming a complex in ammonia, with a pH of approximately 8 to 9, and a commonly used concentration of 38% [13,14]. The mechanism of managing sensitivity with SDF is that the solution forms a mineral-rich precipitate layer that covers the exposed dentin, partially blocking dentinal tubules and eventually reducing fluid shifts within them, thereby diminishing neural stimulation and pain perception [13]. Moreover, a high fluoride concentration of 44,800 ppm can remineralize tooth enamel. The Ag+ ion is considered to have antibacterial properties, and the addition of diamine groups enhances mineral precipitation [14,15], which could reduce hypersensitivity in MIH-affected teeth [16]. These mechanisms propose a potential role for SDF in reducing hypersensitivity in MIH-affected molar populations [17], whereas the retention rate of restorations or crowns in MIH-affected teeth is low due to their low mineral content and high porosity [7].
Although the efficacy of SDF in treating caries has been widely studied, the evidence that SDF can reduce dentin hypersensitivity, particularly in molars affected by MIH, remains limited and inconclusive. Existing articles varied in their methods, outcome measures, and follow-up durations, leading to inconsistent conclusions across studies. Previous systematic reviews and meta-analyses have primarily focused on the caries-arresting effect of SDF or its general desensitizing efficacy in non-MIH teeth or MIH-affected teeth [16,18]. However, none have specifically examined its role in MIH-affected molars, where structural hypomineralization and hypersensitivity pose unique management challenges.
Therefore, a scoping review is suitable for mapping these gaps in the literature, identifying the proper scope and nature of evidence before conducting focused investigations or systematic reviews and meta-analyses when the scientific data are sufficient. As a result, this scoping review was conducted, regarding the research question as “What is the effectiveness of using SDF alone or in combination with restorative treatment in preventing hypersensitivity of teeth affected by MIH?” and aimed to evaluate current evidence on the effectiveness of SDF in the management of dentin hypersensitivity on MIH-affected molars.
METHODS
This scoping review was designed and structured according to the guidelines of the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses and its extension for scoping reviews) [19].
Research question
A primary research question was formulated for the research: “Evaluate the effectiveness of using SDF alone or in combination with restorative treatment in preventing hypersensitivity of teeth affected by MIH.” Also, the PICO (Population, Intervention, Comparison, and Outcomes) strategy was: population: MIH-affected molar undergoing hypersensitive treatment; intervention: SDF alone or in combination with restorative treatment, such as SDF-modified atraumatic restorative technique (SMART); comparison: teeth not undergoing treatment using SDF; outcomes: Schiff cold air sensitivity scale (SCASS).
Search strategy
A comprehensive search strategy was conducted from 14th to 16th October 2025, using Boolean operators (AND, OR, and NOT) to combine phrases with the scientific keywords and related synonyms based on the key concepts: (1) hypersensitivity, (2) SDF, and (3) MIH across four search databases: PubMed, The Cochrane Library, and ScienceDirect as the principal databases and Google Scholar (first 50 to 100 results) as a supplementary database by two authors to determine the eligibility of papers for a full review with the search strings was developed as in Table 1.
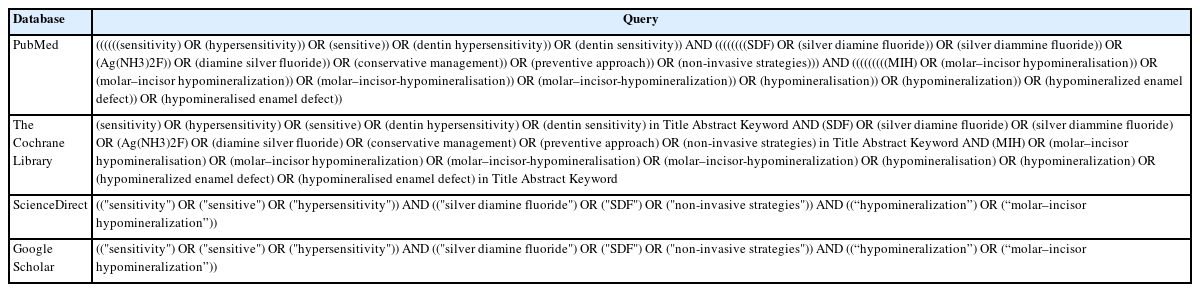
Searching strings
Eligibility criteria
For a paper to be considered for review, it must meet the following inclusion criteria and not meet the exclusion criteria in Table 2.
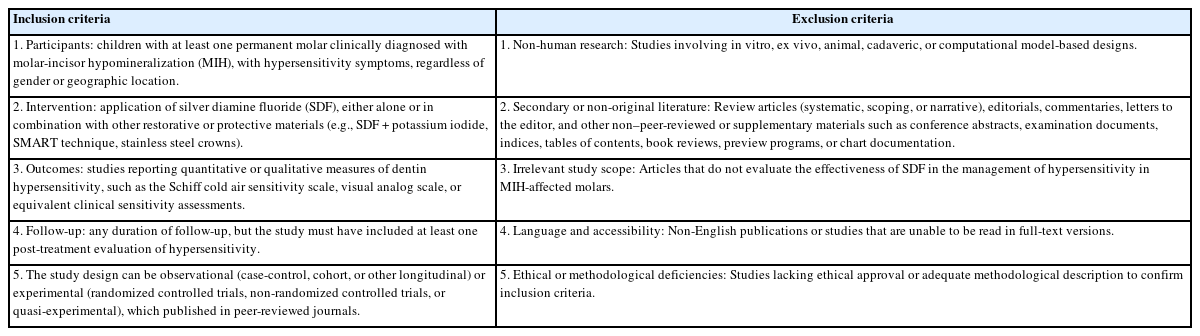
Eligibility criteria of articles used for review
Study selection
The research uses Covidence software [20] to manage and simplify data from four databases. First, the primary author imported all references into the Covidence software, which automatically removed duplicate records. After duplicates were removed, two independent reviewers screened the titles and abstracts against the predefined inclusion and exclusion criteria. In cases of disagreement, a third reviewer was consulted to resolve the conflicts. The same procedure was applied during the full-text review to identify the final set of eligible articles.
Data extraction and analysis
Two independent reviewers (TAT and VNM) conjointly determined which variables to extract, and a standardized data-charting form was automatically built by Covidence software to ensure methodological consistency. Data were retrieved independently by the two reviewers using the software. The extracted data from the selected articles includes: author name, publication year, country, study design, sample characteristics (number of participants and teeth, age, and gender), severity of MIH, intervention and comparison details, follow-up duration, and outcome measures related to dentin hypersensitivity (e.g., SCASS).
In case of disagreement between the reviewers regarding data extraction or study inclusion, the issue was first discussed to reach consensus. If consensus could not be achieved, a third reviewer (DTH) adjudicated the final decision. The process ensured that all included studies met the eligibility criteria. Agreement between the two reviewers during screening and data extraction was continuously monitored within Covidence. The level of agreement was assessed qualitatively through verification of screening logs and consensus discussions.
Due to the heterogeneity of study designs, sample sizes, follow-up durations, and outcome measures, a narrative synthesis was conducted. Extracted data were descriptively summarized in tabular and textual form to map key study characteristics and findings. Quantitative pooling or meta-analysis was not performed, consistent with the exploratory purpose of a scoping review.
As this review aimed to map and summarize the existing evidence rather than to evaluate the methodological quality of studies, no formal risk-of-bias or critical appraisal is required, according to PRISMA-ScR guidelines [19].
Ethical approval
Ethical approval was not required due to the study design. In this review, we conducted a thorough analysis of the current literature on the effectiveness of SDF and/or its combination with restorative treatment in preventing hypersensitivity of MIH-affected molars.
RESULTS
Study selection
After a thorough search, 199 records were identified (Figure 1). Titles and abstracts were used to screen the 171 papers remaining after 28 duplicate studies were removed. Following the exclusion of 155 records, a full-text screening procedure was conducted on the remaining 16 studies. 11 articles were eliminated from consideration for the following reasons: (1) wrong outcomes; (2) wrong intervention; (3) unable to read full-text; (4) not peer-reviewed or published; and (5) non-English articles. This approach produced a final of five articles. From the records that were included for examination, the authors subsequently retrieved both quantitative and qualitative data.
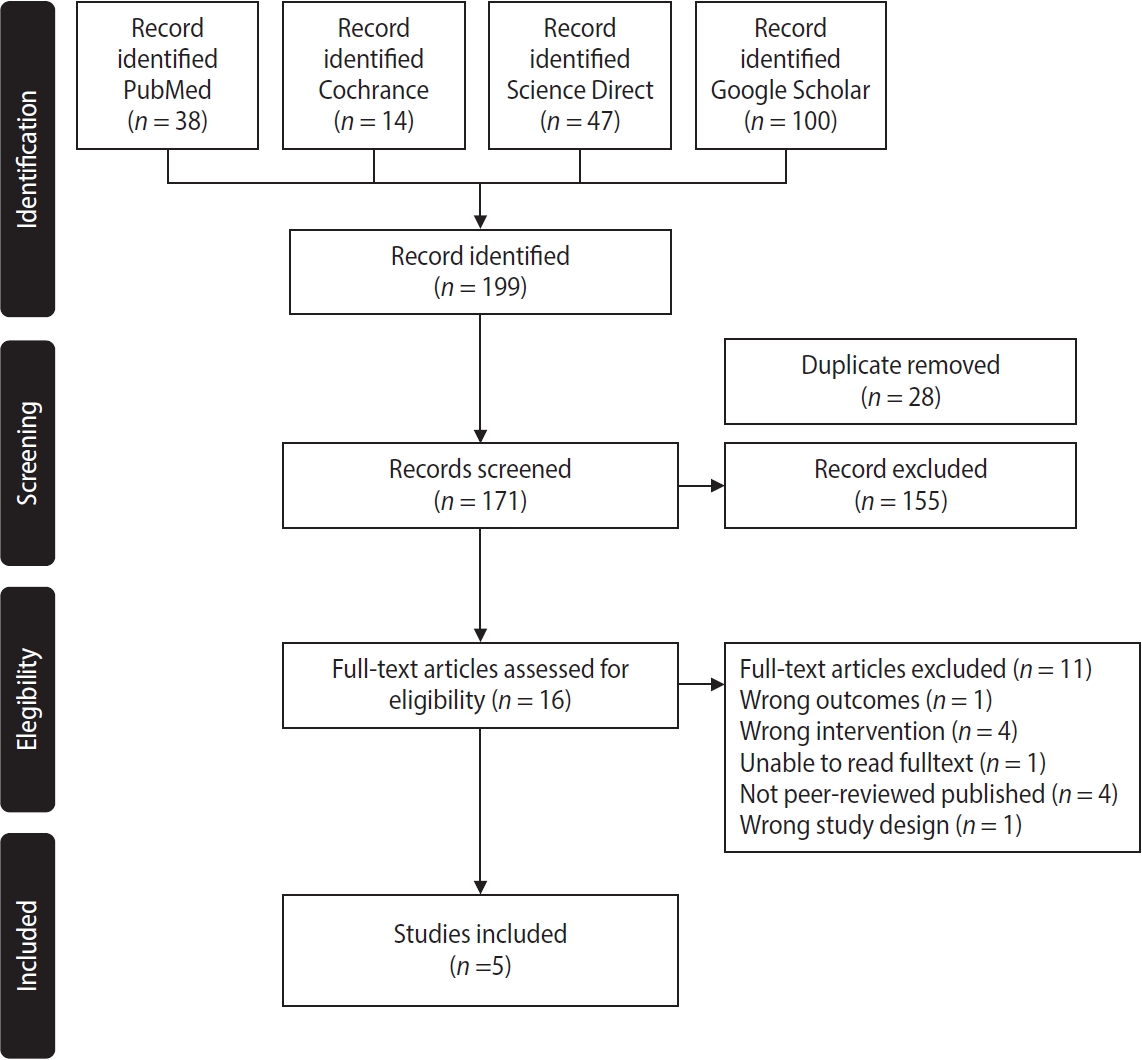
Flow diagram of literature search and study selection.
Study characteristics
The characteristics of the included studies and their main findings are summarized in Table 3. In total, five studies were analyzed, with sample sizes ranging from 4 to 200 teeth. 4 out of five were randomized clinical trials (RCTs), while the remaining study was a case report. At the tooth level, the RCTs have sample sizes ranging from 56 to 200 teeth [17,21–23], whereas only four molars were reported in the case report [24]. At the patient level, only one patient was recorded in the case report [24], whereas the RCTs reported sample sizes ranging from 28 to 100 patients across four studies [17,21–23]. Regarding sample severity, the article from Syria focused solely on molars affected by mild MIH [21], while the article from Egypt included a wider range, from moderate to severe, for research [22], and a case report from India reported on four severe-level molars [24]. In contrast, two studies from Türkiye did not mention the severity of the samples [17,23]. Despite variation in sample sizes, which highlights methodological diversity, all studies shared a common inclusion criterion: hypersensitive MIH-affected molars, allowing cross-study comparison.
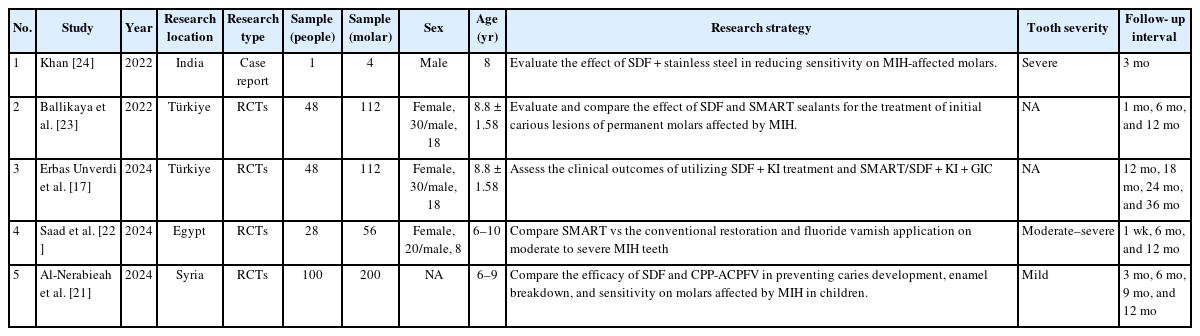
Descriptive characteristics of included articles
1. Demographics of participants
The age of participants was relatively similar across the studies, ranging from 6 to 12 years, which corresponds to the mixed dentition period when hypersensitivity symptoms are most prevalent. In research in Türkiye, one original study had a 12-month follow-up [23], while a subsequent study extended the follow-up period to 36 months, with a reported mean age of 8.8 ± 1.58 years [17]. The remaining two studies, conducted in Egypt (6–10 years) and Syria (6–9 years), also included participants within the mixed dentition stage [21,22]. Moreover, a case report from India focused on a single 8-year-old male participant [24]. While the study from Syria did not specify the gender distribution of participants, the studies from Türkiye (30 females and 18 males) and Egypt (20 females and eight males) provided clear details, showing a predominance of female participants.
2. Study locations and treatment methods
The five studies originated from four different countries worldwide. While two of the five studies were conducted in Türkiye [17,23], the remaining studies were conducted in India [24], Egypt [22], and Syria [21]. The treatment methods were different across studies.
Treatment methods were diverse across the five included studies, with all studies utilizing SDF as the primary intervention. Two RCTs investigated the effectiveness of SDF-only in managing hypersensitivity in MIH-affected molars [21,23]. Four out of five studies used a combination of SDF with other materials, such as potassium iodide (KI), glass ionomer cement (GIC), or stainless steel crowns, in their research [17,22–24]. Additionally, only two studies assessed the efficacy of treatment strategies that did not contain SDF, such as casein phosphopeptide-amorphous calcium phosphate (CPP-ACPFV) fluoride varnish and the combination of conventional restorative treatment with fluoride varnish [21,22].
3. Follow-up periods
The included studies showed variability in follow-up durations. Among the RCTs, follow-up periods ranged from 1 week to 36 months. Two studies from Türkiye assessed outcomes over extended periods, with follow-ups at 12, 18, 24, and 36 months in one study [17] and at 1, 6, and 12 months in another [23]. The trial conducted in Egypt reported follow-ups at 1 week, 6 months, and 12 months [22], whereas the Syrian study evaluated outcomes at 3, 6, 9, and 12 months [21]. In contrast, the case report from India had a shorter follow-up period of 3 months [24].
Results of individual studies
A comprehensive description of the variables related to treatment effectiveness is available in Tables 4 and 5. All five studies reported measurable decreases in dentin hypersensitivity following SDF application. However, the magnitude and duration of improvement varied by intervention type and study design.
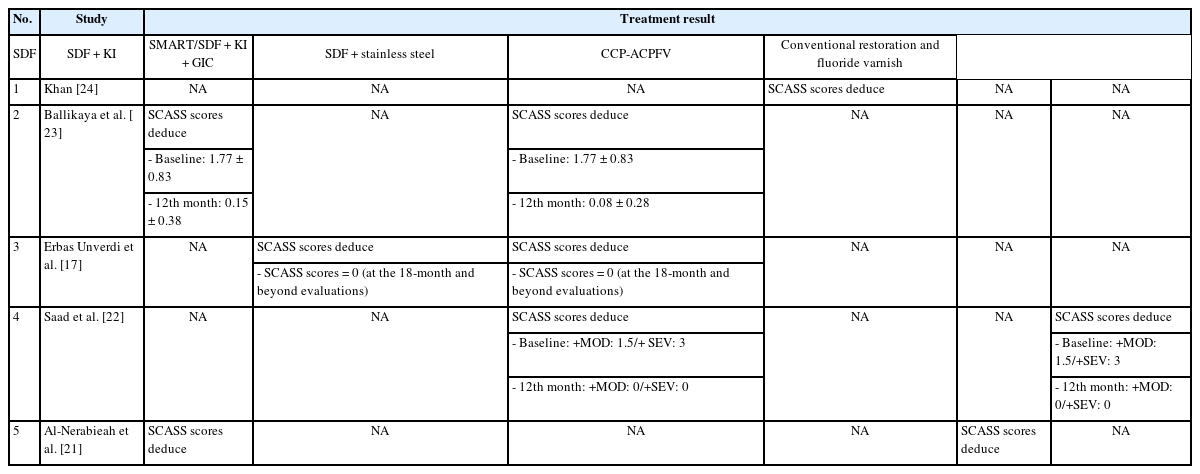
Effectiveness of different strategies in reducing the sensitivity of MIH-affected teeth in the included articles
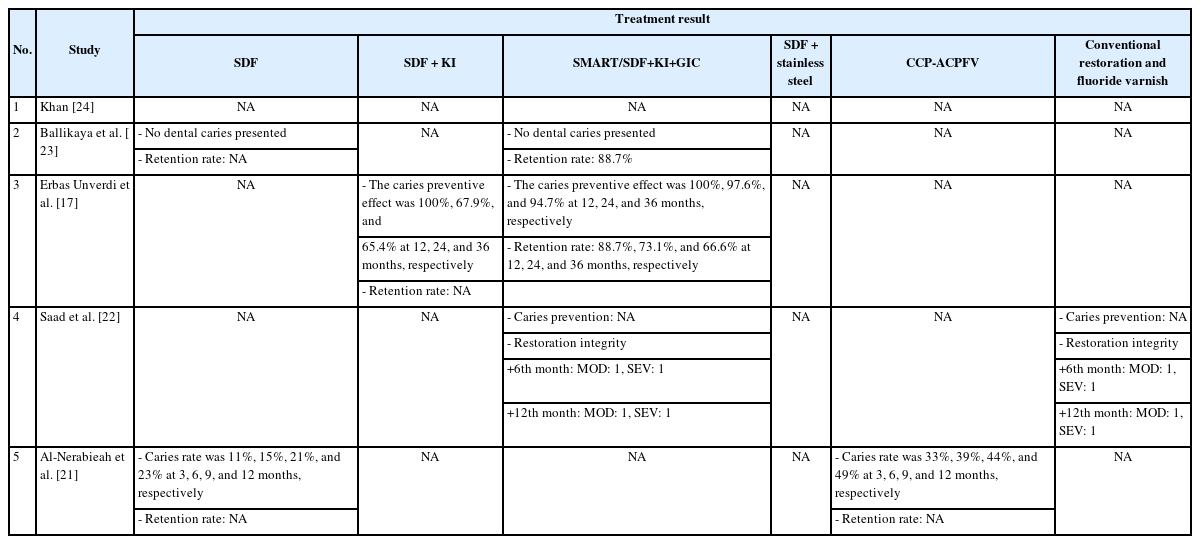
Effectiveness of different strategies in caries prevention and retention rate/restoration integrity of MIH-affected teeth in the included articles
A 12-month follow-up study conducted in Türkiye comparing SDF and the SMART technique found no significant difference in hypersensitivity scores between the groups at 1, 6, and 12 months after repeated SDF applications. Both treatments contributed to the reduction of hypersensitivity, as reflected in the SCASS scores, with both studies showing a reduction from 1.77 ± 0.83 at baseline to 0.15 ± 0.38 with SDF alone and to 0.08 ± 0.28 with the SMART technique after a 12-month follow-up period. Moreover, this study, which employed SDF alone, demonstrated immediate symptom relief and a significant reduction in SCASS scores. Moreover, no caries were detected, and the retention rate within the SMART technique group was 88.7% [23].
Another Turkish study with a 36-month follow-up compared the effects of SDF combined with KI (SDF + KI) with those of the SMART technique. There was a significant reduction in SCASS scores at all evaluation periods relative to baseline, with both interventions showing SCASS scores of 0 from the 18-month follow-up onward. The caries-preventive effect was 100%, 67.9%, and 65.4% for SDF + KI-treated teeth; and 100%, 97.6%, and 94.7% for SMART (SDF + KI + GIC)-treated teeth at 12, 24, and 36 months, respectively. The clinical retention rate of SMART sealants at 12, 24, and 36 months was 88.7%, 73.1%, and 66.6%, respectively [17].
A study in Egypt comparing the SMART technique with a combination of conventional restorations and fluoride varnish application found a significant reduction in SCASS scores across four evaluation intervals. In both interventions, the moderate hypomineralized molar severity (MOD) group (with a 1.5-point SCASS score) and the severe hypomineralized molar severity (SEV) group (with a 3-point SCASS score) showed reductions to 0. This result suggests that these approaches are effective in reducing dentin hypersensitivity in molars affected by MIH. There was no difference between 6 and 12 months in each of the four subgroups [22].
In Syria, a study assessing the effectiveness of SDF and CPP-ACPFV found no significant differences in SCASS scores between treatment groups throughout the study. The caries rates were 11%, 15%, 21%, and 23% for SDF-treated teeth, and 33%, 39%, 44%, and 49% for CCP-ACPFV-treated teeth at 3, 6, 9, and 12 months, respectively [21].
A case report from India evaluating the combined effect of SDF and stainless steel crowns showed a reduction in SCASS scores, suggesting decreased hypersensitivity [24].
DISCUSSION
This scoping review is the first article to collect, analyze, and provide a comprehensive evaluation of the effectiveness of SDF treatment in reducing dentin hypersensitivity on molars affected by MIH.
All five included studies reported a reduction in dentin hypersensitivity with each treatment strategy, accompanied by a significant decrease in SCASS scores, particularly with SDF-only or SDF combined with other materials [17,21–24]. Previous studies also suggested that the application of silver ions significantly occludes dentinal tubules and reduces hypersensitivity [25–28]. Silver particles can deposit in the lumens and may form mechanical blockages along the length of the tubules, reducing fluid movement within the dentin tubules and thereby reducing dentin hypersensitivity [13,29]. A series of chemical reactions contributes to tooth desensitization by occluding dentinal tubules, facilitating remineralization of demineralized tooth structure, and inhibiting dentinal collagen degradation. However, these reactions result in a notable side effect—permanent black staining of carious lesions in both enamel and dentin, while sound enamel remains unaffected [30]. Additionally, studies that combined SDF with other treatment strategies, such as KI [17], SMART [17,22,23], or stainless steel crowns [24], also reported reductions in hypersensitivity. The combination of SDF with KI offers both hypersensitivity reduction and mitigates the common detrimental effect of black staining by forming silver iodide precipitates, which enhances patient satisfaction, particularly in aesthetic regions [31]. The SMART technique has been proven to the reduction of hypersensitivity. However, the long-term clinical efficacy of the SMART technique in managing MIH-affected cases remains unclear [32]. Furthermore, stainless steel crown placement offers desensitizing benefits while ensuring long-term mechanical coverage and pulpal protection, making it especially valuable in pediatric dentistry [24]. Ultimately, these findings suggest that SDF, when combined with other restorative or protective strategies, may offer significant benefits in managing hypersensitivity.
Several factors influenced the effectiveness of SDF treatment. The patient age range across the studies was relatively consistent, predominantly covering the mixed dentition period (6–10 years), which corresponds to the phase when enamel porosity and dentin exposure are greatest. This may be because, at the age of 8 years, as recommended by the European Academy of Paediatric Dentistry for MIH prevalence studies, the FPMs typically erupt intact, allowing clear visualization of enamel opacities for diagnosis. In older children, PEB and conservative treatment may obscure MIH characteristics, leading to potential underdiagnosis [33,34]. Younger individuals with MIH may experience greater hypersensitivity, as physiological reparative dentin deposition and exposure to desensitizing agents increase with age. Additionally, older individuals may develop greater awareness and improved ability to manage hypersensitivity symptoms [8]. All five studies demonstrated significant success in reducing dentinal hypersensitivity in MIH-affected molars. Treatment Needs Index or MIH severity scores were inconsistently reported, limiting the ability to stratify the results. However, the severity of MIH lesions still played a crucial role, with mild, moderate, and severe cases responding differently to treatment, with more severe lesions requiring combined restorative approaches (e.g., SMART or SDF + KI), which demonstrated complete hypersensitivity elimination and improved retention rates in the longer term [7].
The follow-up periods also varied significantly, ranging from 1 week to 36 months among the included studies, which may explain the variability in reported long-term effectiveness. Studies with longer observation periods, such as those conducted in Türkiye [17], demonstrated more stable and sustained reductions in hypersensitivity, suggesting that repeated SDF application or the adjunctive use of glass ionomer materials may contribute to prolonged tubule occlusion and mineral deposition. In contrast, shorter-term studies reported rapid symptom relief but lacked evidence of sustained benefit over time [21–24].
Interestingly, studies combining SDF with other agents, such as SDF + KI or SMART, have suggested potential advantages for maintaining long-term hypersensitivity control [17,22–24]. Some findings from the included articles require further discussion. The studies from Türkiye reported complete elimination of hypersensitivity from 18 months onward (SCASS score of 0), showing the potential for prolonged effectiveness of SDF, SDF combined with potassium iodide, and SMART technique in MIH-affected molars [17], similarly to the findings of the previous scientific review by Jayanti and Riyanti [35], which also highlighted the promising role of SDF and its combinations as a minimally invasive treatment option for teeth affected by MIH. However, while Jayanti and Riyanti [35] conducted a broad scoping review summarizing various noninvasive and restorative management strategies for MIH, our review focused specifically on the effectiveness of SDF in reducing dentin hypersensitivity in MIH-affected molars. Consequently, our synthesis provides a more targeted evaluation of SDF alone and its combined protocols (e.g., SDF + KI, SMART), whereas Jayanti and Riyanti’s work [35] emphasizes overall treatment modalities, including resin infiltration, GIC, and fluoride varnishes. Additionally, the article from Syria found that there was no difference between using SDF alone and using CPP-ACPFV in reducing hypersensitivity in molars affected by MIH [21]. Moreover, a case report from India also noted a reduction in hypersensitivity when using SDF prior to stainless steel crowns, providing physical protection against external agents [24]. Comparatively, studies using SDF alone generally reported a significant short-term reduction in SCASS scores [21,23], while combination techniques achieved earlier desensitization and longer maintenance of effect [17,22]. These findings support a potential synergistic benefit when SDF is combined with other bioactive restorative materials, though the small number of trials prevents definitive conclusions. These variations highlight the need for further analysis to establish a standardized treatment strategy for molars affected by MIH.
Only a few studies have addressed both caries prevention and hypersensitivity reduction. The 12-month study in Türkiye reported no new caries development, but this study observed a significant reduction in hypersensitivity [23]. Meanwhile, the 36-month Turkish study found that the SMART technique provided superior caries prevention (94.7% after 36 months) compared with SDF + KI (65.4%), although both strategies reduced hypersensitivity [17]. Similarly, the study from Syria showed that SDF was more effective in preventing caries than CPP-ACPFV (23% vs 49% caries incidence after 12 months), but also no significant difference was observed between the two groups in terms of hypersensitivity reduction [21]. This suggests that hypersensitivity in MIH-affected molars is more likely due to MIH itself rather than to dental caries. However, further long-term follow-up research using SDF should be considered to determine the relationship among MIH-affected teeth, hypersensitivity, and dental caries.
The retention rate/integrity of restorations was reported in only a few studies. A 12-month study from Türkiye reported an 88.7% retention rate with the SMART technique [23], whereas a 36-month study from Türkiye showed a decline to 66.6% at 36 months [17]. Additionally, the study from Egypt evaluated the integrity of restorations and found no significant difference between the SMART technique and conventional restorations combined with fluoride varnish [22]. Despite these variations in restoration retention, all studies consistently reported a significant reduction in hypersensitivity. This suggests that improvements in hypersensitivity may not be directly related to restoration retention. However, further long-term follow-up research is needed to provide conclusive scientific evidence on this matter.
Despite this scoping review achieving its aim of evaluating the effectiveness of SDF in managing hypersensitivity of MIH, some important limitations should be acknowledged to provide proper guidance for future studies.
This scoping review is constrained by the limited number of eligible studies (n = 5), small sample sizes, and heterogeneity in study design, diagnostic criteria, intervention types, and follow-up durations. It is difficult to make direct comparisons, which could limit the accuracy of the evaluation. Moreover, the methodological rigor across studies was inconsistent, and one study included a case report, further limiting generalizability. Furthermore, in almost every study, the researcher's intervention involved combining SDF with other materials to manage dentin hypersensitivity in MIH-affected molars. This could be challenging to determine whether the reduction in dentin hypersensitivity was a direct effect of SDF or of the other materials. These factors reduce the overall certainty of the evidence and underscore the need for larger sample sizes, longer follow-up durations, systematic reporting of severity levels, use of SDF-only, and well-designed RCTs to verify the observed effects. Although a formal risk-of-bias assessment was not conducted, this aligns with the methodological framework of scoping reviews, which aim to provide an overview of available evidence rather than to appraise its quality.
Moreover, some of the exclusion criteria may limit this scoping review, as it included only English-language articles and research from the four mentioned scientific databases, due to language barriers and accessibility issues. The limited search of gray literature, such as conference proceedings, dissertations, or other non-peer-reviewed sources, might also lead to publication bias. Future reviews should adopt a more comprehensive, inclusive search strategy to improve results.
CONCLUSIONS
This scoping review identified a small but growing body of evidence suggesting that SDF, whether used alone or in combination with other restorative strategies, may effectively reduce dentin hypersensitivity in molars affected by MIH. However, the strength of this conclusion is limited due to the small number of available studies, their methodological heterogeneity, and the absence of standardized outcome measures.
Future well-designed randomized controlled trials with standardized diagnostic criteria and follow-up protocols are required to confirm these preliminary observations and determine optimal application. According to current evidence, SDF-based interventions are a promising, minimally invasive approach for managing hypersensitivity in molars affected by MIH.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING/SUPPORT
The authors have no financial relationships relevant to this article to disclose.
ACKNOWLEDGMENTS
During the preparation of this work, the authors used ChatGPT ver. 5.3 (OpenAI, San Francisco, CA, USA) in order to improve the readability and language of the manuscript during the writing process. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
AUTHOR CONTRIBUTIONS
Conceptualization, Methodology: all authors. Data curation, Formal analysis, Investigation: Tuan TA, Minh VN , Linh TK. Writing - original draft: Ngoc VTN, Hieu DT, Tuan TA, Minh VN. Writing - review & editing: all authors. All authors read and approved the final manuscript.
DATA SHARING STATEMENT
The data supporting this article can be made available by the corresponding author upon request.