Fiber-reinforced composite post removal using guided endodontics: a case report
Article information

Abstract
Although several techniques have been proposed to remove fiber-reinforced composite (FRC) post, no safe and efficient technique has been established. Recently, a guided endodontics technique has been introduced in cases of pulp canal obliteration. This study describes 2 cases of FRC post removal from maxillary anterior teeth using this guided endodontics technique with a dental operating microscope. Optically scanned data set from plaster cast model was superimposed with the data set of cone-beam computed tomography. By implant planning software, the path of a guide drill was selected. Based on them, a customized stent was fabricated and utilized to remove the FRC post. Employing guided endodontics, the FRC post was removed quickly and safely with minimizing the loss of the remaining tooth structure. The guided endodontics was a useful option for FRC post removal.
INTRODUCTION
The post and core build-up serves to reconstruct the lost tooth structure and provide sufficient retention and resistance for the final restoration [1]. If a periapical lesion develops on a previously endodontically treated tooth and a post is in place, post must be removed for successful nonsurgical root canal treatment. In some cases, the post needs to be removed to enhance the design, mechanics, or esthetics of a new restoration [2]. However, post removal is challenging for clinicians and could weaken or perforate the root structure.
A dentist may choose to place a fiber-reinforced composite (FRC) post with a composite resin core following root canal treatment due to less chance of root fracture and better esthetics [3]. FRC post removal pose some difficulties not encountered with metal post removal. Due to the lower modulus of elasticity of the FRC, the ultrasonic vibration is not adequate to disrupt the cement interface between the post and root dentin. In addition, the FRC post is difficult to distinguish from the root dentin deep in the canal even with the use of a dental operative microscope. Removal of a FRC post involves drilling it out in most cases. In order to minimize the loss of root structure while finding the interface between the root filled material and end of the post, initial targeting toward the interface is an important and difficult procedure.
Although several techniques have been proposed to remove a FRC post, such as the use of an ultrasonic tip, a round bur, or specially designed removal kit, the procedure of removing the FRC post is challenging for clinicians with risks of root perforation with the use of any technique [4567].
Recently a guided endodontics technique has been introduced for nonsurgical root canal treatment of a tooth with pulp canal obliteration that has shown a favorable clinical outcome without complications, such as extensive tooth structure removal and root perforation [8910]. The basic concept of this technique is identical to the procedure that uses a computer-aided design (CAD)/computer-aided manufacturing (CAM) stent for guiding the position and direction of the dental implant.
This report describes 2 cases of FRC post removal from maxillary anterior tooth safely and efficiently using guided endodontics with a dental operating microscope.
CASE REPORT
Case 1
1. Patient evaluation
A 19-year-old female patient visited the clinic with a fractured coronal restoration of the upper maxillary (right) central incisor (Figure 1). Ten years ago, the tooth was fractured with pulp involvement and was treated with root canal treatment and FRC post-resin core. There was no pain or tenderness on percussion. By cone beam computed tomography (CBCT) and periapical radiograph examination, there was neither periapical pathosis nor widening of periodontal ligament which was periapical index (PAI) score 0 [11]. Even though the tooth was diagnosed as previously endodontic treatment and normal periapex, the gap between the previous FRC post and root canal wall was assumed. Also, the post replacement was essential in order to improve the retention of the newly installed core.
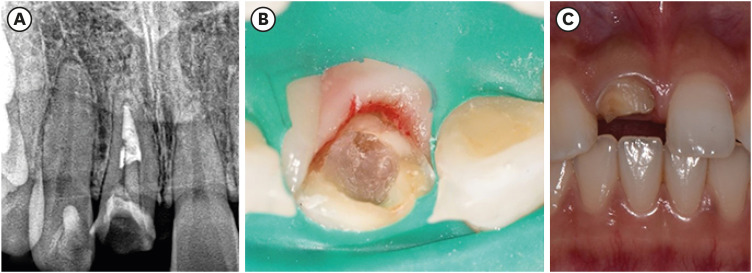
The initial periapical radiograph (A) and photography (B) shows that the fiber-reinforced composite post-resin core of upper maxillary (right) central incisor is partially broken.
Considering the configuration of post space of root canal, a cast post restoration was planned in hopes of achieving better retention. Therefore, the previously cemented FRC post needed to be removed. For this compromised tooth, it was important to minimize the loss of tooth structure during FRC post removal. Therefore, we decided to use the guided endodontics technique for this patient.
2. Procedure for making a customized stent
In order to make a customized stent, an alginate impression (Aroma fine plus normal set, GC Corporation, Tokyo, Japan) was taken of the maxillary anterior area, and a plaster cast model was made. The plaster model (Whip-Mix Silky-Rock yellow model stone, Whip-Mix corporation, Louisville, KY, USA) was optically scanned using a scanner (CS3600, Carestream Dental, Atlanta, GA, USA). Two 3D data sets consisting of CBCT and optical scanning data were input into the implant planning software (DDS-Pro, Digital Dental Service, Czestochowa, Poland). In the software, the path of a guide drill was set to follow the length of the FRC post seated in the tooth. A guide stent was also designed (Figure 2). The stent was fabricated using a 3D printer (BIO3D, Bio3D Ltd., Seoul, Korea). A metal sleeve was integrated inside, and Vaseline oil (White Petrolatum, Firson, Cheonan, Korea) was applied at the inner surface of the metal sleeve for lubrication. A guide drill with a diameter 1.0 mm (Steco System Technik, Hamburg, Germany) and a metal sleeve (Steco System Technik) with 1.0-mm inner diameter, a 3.5-mm outer diameter, and a 5.0-mm height were used in the present case.
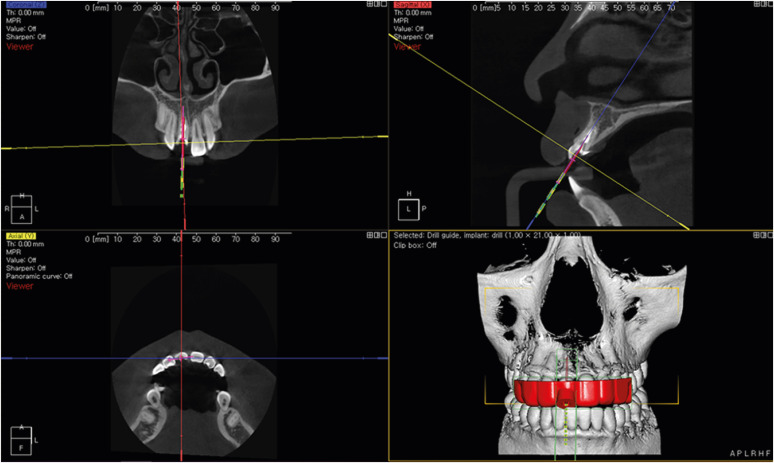
Planning of coronal, sagittal, and axial plane of the guide drill placement for removal of fiber-reinforced composite post using the implant planning software (DDS-Pro).
3. Treatment using a customized stent
After checking the fit of the stent, the stent was positioned in the mouth (Figure 3A). A guide drill (1.0 mm, Steco System Technik) with a rubber stop was used at 10,000 rpm with pecking motion through the metal sleeve of the stent. With each 2-mm apical advancement of the guide drill, the drilled cavity was irrigated with saline. The required amount of apical advancement of the guided drill was calculated as 8 mm using the implant planning software. After approximately 8.0 mm apical advancement of the guide drill, gutta-percha could be observed under the dental operating microscope (OPMI pico, Carl Zeiss, Oberkochen, Germany) (Figure 3B).
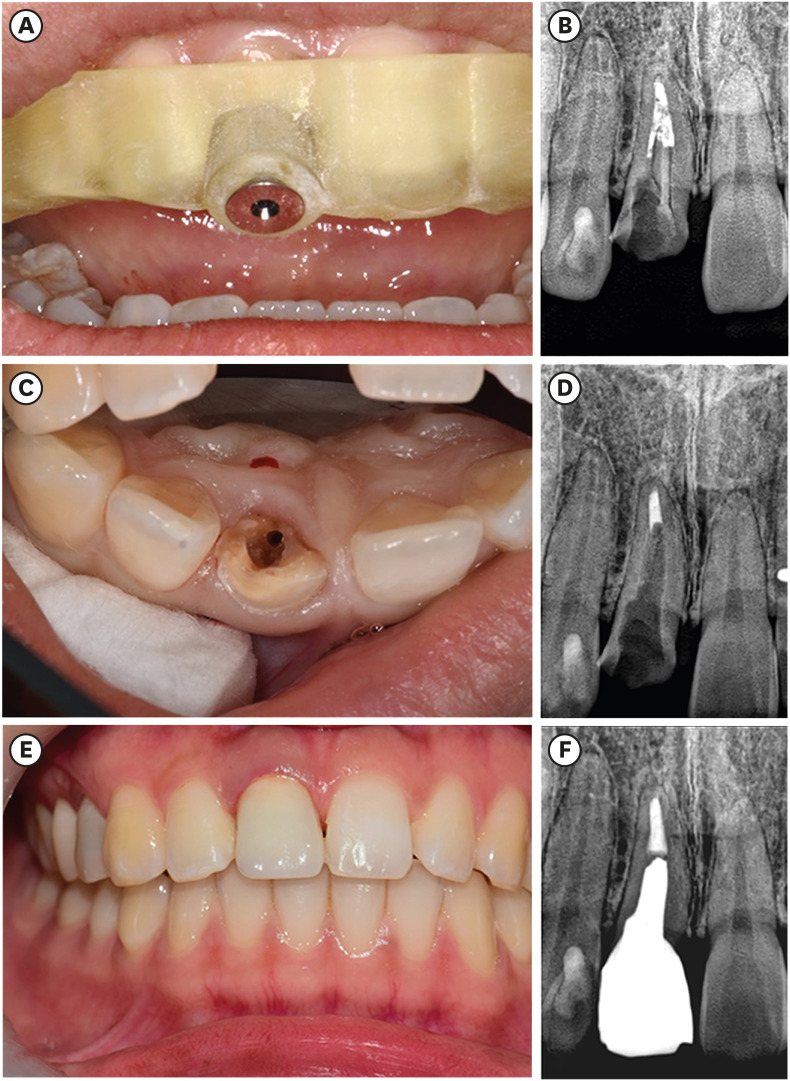
(A) The stent is positioned in the mouth. (B) After 8.0 mm apical advancement of the guide drill. (C) After removing the remaining fiber-reinforced composite post-resin core under the dental operating microscope. (D) Radiographic verification of post removal. (E) After seating cast post and core and full veneer crown. (F) Radiography of completed case.
Thereafter, a rubber dam was placed, and the remaining FRC post-resin core was removed using an ultrasonic tip (Start-X #3, Dentsply Sirona, Ballaigues, Switzerland) under the dental operating microscope (Figure 3C and 3D). A part of the FRC post-resin core was removed using a guide drill; therefore, the remnant of FRC post-resin core was easily distinguishable from the root dentin. There was no sign of contamination inside the root canal and no periapical changes. Thus, the existing gutta-percha filling was left in place. Then, the restoration was completed with a metal (Ni-Cr alloy) cast post and core full veneer zirconia crown (Figure 3E and 3F).
Case 2
1. Patient evaluation
A 13-year-old girl was referred from a local dental clinic because of multiple periapical radiolucent lesions around the upper maxillary (right) central incisor, upper maxillary (left) central incisor, upper maxillary (left) lateral incisor (Figure 4A). The teeth were endodontically treated 1 year ago. and showed a distinct radiolucent area with loss of lamina dura (PAI score 3) [11]. There was tenderness on percussion and openings of the sinus tract. The teeth were diagnosed as previously endodontic treated and chronic apical periodontitis. Nonsurgical root canal treatment was planned because we suspected the presence of accessory canals canal was suspected and poorly condensed canal space to improper shaping, cleansing, and filling. The FRC posts cemented in the 3 teeth needed to be removed. The interface between FRC post and gutta-percha could be identified depending on the difference of radiopacity in the periapical radiographs. For the upper maxillary (left) lateral incisor, the FRC post was removed with an ultrasonic tip (Start-X #3) under the dental operating microscope (OPMI pico) (Figure 4B). It took a long time, and was a tedious task for the pediatric patient and the operator. Thus, for the upper maxillary (right and left) central incisors, we decided to use the guided endodontics technique for removing the FRC posts.
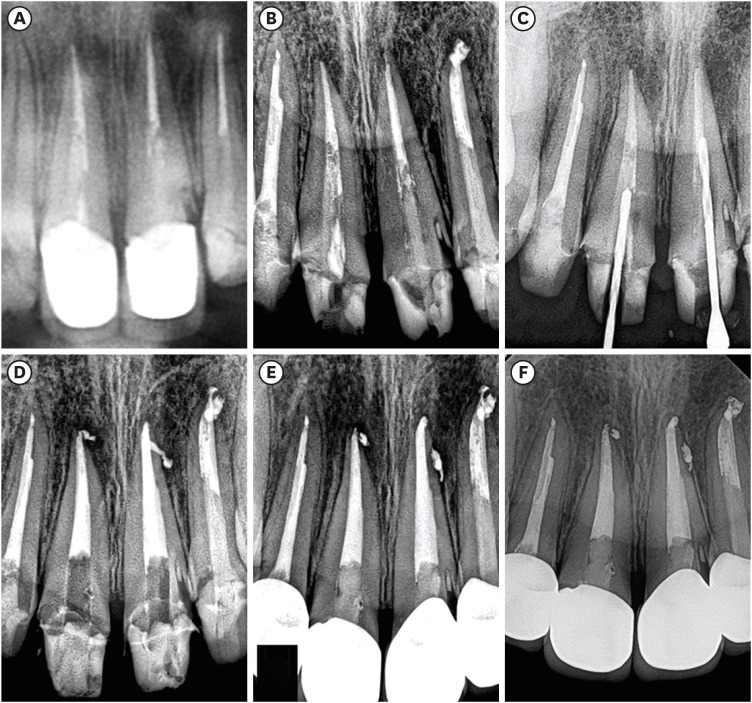
(A) Preoperative radiography shows preinstalled fiber-reinforced composite (FRC) posts and periapical lesions in the upper maxillary (right) central incisor, upper maxillary (left) central incisor, and upper maxillary (left) lateral incisor. (B) For the upper maxillary (left) lateral incisor, the FRC post was removed with a conventional method, and nonsurgical root canal treatment was completed. (C) For upper maxillary (right) and (left) central incisors, guided endodontics was used for removing the FRC posts. Periapical radiography shows the direction of the guide drill. (D) After removing the remaining FRC post with an ultrasonic tip, the root canal was obturated nonsurgically. (E) One-month follow-up radiograph. (F) The periapical lesion was resolved after 1-year follow-up.
2. Treatment using a customized stent
The procedure for making a customized stent and drilling procedure was the same as in case 1. Gutta-percha was visible after approximately 14.5 mm of apical advancement in the upper maxillary (right) central incisor and 15.0 mm of advancement in the upper maxillary (left) central incisor (Figure 4C). A part of the root dentin around the apex of the FRC post was shown to be removed, although the amount of removal was limited.
Then, a rubber dam (Dental Dam, Coltene/Whaledent, Altstätten, Switzerland) was placed, and the remaining FRC post-resin core was removed using an ultrasonic tip, Start-X #3, under the dental operating microscope. Thereafter, routine conventional nonsurgical root canal retreatment was initiated. Previously filled gutta-percha was removed with k-file and h-file. Using an electronic apex locator (iRoot, Meta Biomed, Cheongju, Korea) and a dental radiograph, the working length was determined to be 22.5 mm and 23.0 mm in the upper maxillary (right) and (left) central incisors individually. The root canals were as shaped using ProTaper Next (Dentsply Sirona) X1, X2, X3, X4, and X5 with copious 2.5% sodium hypochlorite irrigation. Master apical file size was #60 for the upper maxillary (right) central incisor and #80 for the upper maxillary (left) central incisor. The shaped root canal was obturated with gutta-percha and AH-plus sealer (Dentsply Sirona) using a combination of cold lateral compaction and continuous wave compaction techniques (Figure 4D). The access cavity was sealed with a composite resin (Gradia Direct, GC Corporation). Full veneer crowns were completed for the teeth after 1 month (Figure 4E). On 1-year follow-up radiograph, the periapical lesion was resolved (PAI score 0), and the patient did not present any discomfort regarding the treated teeth (Figure 4F).
DISCUSSION
The FRC post should be removed for successful nonsurgical root canal retreatment or new restoration. Although various techniques have been used to remove FRC posts, the procedure remains challenging for clinicians. The FRC post could be removed by grinding away with a round bur or special ultrasonic tips, such as Start-X or SoniFlex Endo (Kavo, Biberach, Germany) [6]. This technique is very simple; however, it is hard to distinguish an FRC post from root dentin in the deep root area even with the use of a dental operative microscope. Otherwise, FRC post could be removed with pilot drilling for creating an initial hole and following by a bur to drilling out the entire post [45]. In compromised or severely angulated tooth, it might be difficult to estimate the orientation of the FRC post installed. Therefore, the orientation of initial pilot drilling might be improper, potentially resulting in root perforation.
Guided endodontics using a CAD/CAM stent was introduced for gaining access to the calcified canal and surgical root canal treatment [8910]. This newly proposed method was proven safe, effective, and operator-independent in several clinical and experimental studies [8]. Regarding FRC post as calcified canal, guided endodontics could provide a way to remove a FRC post safely and efficiently.
In this case report, the guided endodontics technique was successfully utilized for removing FRC post. The tooth in case 1 had a compromised coronal structure. Therefore, an alternative approach for removing FRC post was needed to minimize the loss of the remaining tooth structure that is essential for a favorable long-term prognosis in case 1.
In case 2, FRC post in upper maxillary (left) lateral incisor was removed using the conventional method under a dental operating microscope; however, it was a tedious task for the pediatric patient. Patient management would be difficult if the traditional method is used for FRC post removal in the other 2 teeth. Therefore, a fast and safe method for removing the FRC post was required. Thus, we decided to use the guided endodontics technique for case 2.
In the present cases, it took < 5 minutes to complete FRC post removal, and there was no perforation. With the guided endodontics technique, the chair time and risk of root perforation are lower, irrespective of patient cooperation. The precise fit between the metal sleeve and drill shank helped the operator maintain the axis of drilling precisely to the target point. It is capable of generating considerable heat and the lubricating gel was employed. In order to minimize thermal damage to the tooth structure during drilling, copious irrigation was used after each increment of movement.
Previous studies have shown that drilling precision decreased when a drill with a small diameter was used and selection of guide drill diameter should correlate with post diameter [121314]. In contrast, a drill with a large diameter could cause more heat generation. Considering thermal damage and accuracy, clinicians should select the proper drill as per the case. In the present cases, a 1.0-mm diameter drill was selected because it is the smallest-diameter commercially available drill, and the installed post size is larger than that of the selected drill.
Although the procedure was performed very carefully, a discrepancy between the planned and actual drilling path was observed (Figure 4B). Several ex vivo studies were performed to evaluate the accuracy of guided endodontics which presented a small numerical error in the deviation of the tip of the drill and angle deviation [15161718]. As the drill must go deeper in the root to remove the cemented post, the accumulated discrepancy could be larger. In addition, the experimental condition, ex vivo, was different from that in our clinical cases in terms of the use of implant planning software, different optical scanning method, and different CBCT settings. Therefore, further research is necessary on the method of improving the accuracy of guided endodontics and evaluating the accuracy of guided endodontics, depending on various factors.
It is advisable to use a dental operating microscope for removing the FRC post even with the use of guided endodontics. There was a discrepancy between the actual and planned drilling path; therefore, it is necessary to check the drilling axis with the use of a dental operative microscope as in our cases. As the dimension of the guide drill cannot be identical to the prepared post space, the remaining FRC post and cement must be removed using an ultrasonic tip or small round bur safely under an operative microscope.
CONCLUSIONS
In these cases, and the FRC post was removed quickly and safely with minimizing the loss of the remaining tooth structure and providing a less stressful treatment for both the clinician and patient. The guided endodontics is a useful option for FRC post removal.
Notes
Funding: This research was supported by Kyungpook National University Research Fund, 2019.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Ha JH.
Data curation: Cho C, Jo HJ.
Formal analysis: Jo HJ.
Funding acquisition: Ha JH.
Investigation: Cho C.
Methodology: Cho C.
Project administration: Ha JH.
Resources: Ha JH.
Software: Ha JH.
Supervision: Ha JH.
Validation: Jo HJ.
Visualization: Cho C.
Writing - original draft: Cho C.
Writing - review & editing: Jo HJ, Ha JH.