Postoperative pain after endodontic treatment of necrotic teeth with large intentional foraminal enlargement
Article information

Abstract
Objectives
To evaluate postoperative pain after endodontic treatment of necrotic teeth using large intentional foraminal enlargement (LIFE).
Materials and Methods
The sample included 60 asymptomatic necrotic teeth (with or without chronic apical periodontitis), and a periodontal probing depth of 3 mm, previously accessed and referred to perform endodontic treatment. After previous procedures, the position and approximate size of the apical foramen (AF) were determined by using an apex locator and K flexo-files, respectively. The chemomechanical preparation was performed with Profile 04 files 2 mm beyond the AF to achieve the LIFE, using 2.5 mL of 2.5% NaOCl at each file change. The filling was performed by Tagger's hybrid technique and EndoFill sealer. Phone calls were made to all the patients at 24, 48 and 72 hours after treatment, to classify postoperative pain. Statistical analysis was performed by different tests with a significance level of 5%.
Results
Age, gender, periradicular status and tooth type did not influence postoperative pain (p > 0.05). Only 1 patient (1.66%) reported severe pain after 72 hours. Moderate pain was reported by 7, 4 and 3 patients after 24, 48 and 72 hours, respectively (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). Sealer extrusion did not influence the postoperative pain (p > 0.05).
Conclusions
Acute or moderate postoperative pain was uncommon after endodontic treatment of necrotic teeth with LIFE.
Trial Registration
The Brazilian Clinical Trials Registry Identifier: RBR-3r967t
INTRODUCTION
Endodontic treatment aims to maintain or reestablish the health of periapical tissues by cleaning and filling the root canals [12]. Biomechanical preparation and intracanal dressing (when used) are responsible for the disinfection process; however, they are not able to eliminate the content of the root canal system completely due to its anatomical and morphological complexity and to the resistance of some microorganisms involved in endodontic infection [34].
Molecular analysis has shown the presence of bacterial biofilms in apical foramen (AF) [567]. This is why the impact of intentional foraminal enlargement (IFE) on the success of endodontic treatment has been studied [8910].
IFE is based on the mechanical enlargement of the AF to reduce the bacterial load by excising the infected cementum and dentin from this area [910]. However, a study performed by Tinaz et al. [11] showed that IFE caused greater debris extrusion, which is one of the main reasons for postoperative pain after endodontic treatment of necrotic teeth [1213].
Several randomized clinical trials have evaluated postoperative pain after performing endodontic treatments of necrotic teeth using manual, rotary and reciprocating files to conduct IFE, and have found different results [141516]. Silva et al. [16] carried out endodontic treatments of necrotic anterior teeth with or without IFE using hand files. The authors reported similar levels of postoperative pain between these groups. Cruz Junior et al. [15] conducted a similar analysis in the single-rooted necrotic tooth using a reciprocating system. Patients from the IFE group reported more pain after 24 hours.
It is noteworthy to mention that the AF frequently has an oval shape [171819]. Therefore, it might be cleaned better with large IFE (LIFE) [1020]. To the best of our knowledge, no study has yet been made to evaluate postoperative pain after performing endodontic treatment with LIFE in necrotic teeth (with or without chronic apical periodontitis). Therefore, this was the purpose of this study.
MATERIALS AND METHODS
This study received approval from the Human Research Ethics Committee of the Pontifical University of Paraná – PUC/PR (CAAE. 12449019.6.0000.0020), is reported in accordance with the Consolidated Standards of Reporting Trials Statement (CONSORT, 2010), and is registered at The Brazilian Registry of Clinical Trials (ReBEC; RBR-3r967t).
Sample size calculation
The sample size to validate the results of this research was determined by conducting a pilot study that showed that less than 5% of the patients reported significant postoperative pain (acute or moderate) after treatment. The proportion-sampling method was used to determine the sample size, which was set at 60 teeth, considering a confidence level of 95% and a maximum margin of error of 5.5%.
Case selection
This study was conducted in patients ranging in age from 14 to 73 years, referred to the Centro de Especialidades Odontológicas de Navegantes, Santa Catarina, Brazil, to perform endodontic treatment, between September and October 2019. The patients were informed about the postoperative care, the clinical and radiographic examinations, and the available alternative treatment options. Information about the study and the treatment protocol were provided to all the patients or their caregivers (for patients under 18 years old), and written consent was obtained.
The inclusion criteria for this study were asymptomatic necrotic teeth (with and without chronic apical periodontitis), and a periodontal probing depth of 3 mm at most, as previously accessed at the Public Basic Health Units of the aforementioned city. The exclusion criteria were consumption of anti-inflammatories, analgesics of any type, or antibiotics within the last 10 days before treatment, presence of root resorption, sinus tracts, trismus, periodontal probing greater than 3 mm, systemic diseases, history of trauma, pregnancy, severe malocclusion associated with traumatic occlusion, lack of patient compliance and history of intolerance to nonsteroidal anti-inflammatory drugs.
Treatment protocol
After clinical and radiographic examination of the patients, and evaluation of their health status, the teeth were anesthetized using 2% mepivacaine with epinephrine 1:100,000 (Mepiadre; DFL Indústria e Comércio S.A., Rio de Janeiro, RJ, Brazil). After rubber dam placement and disinfection, the temporary restoration was removed using a 1014 or 1016 HL bur (KG Sorensen, Barueri, SP, Brazil). When reaching the pulp chamber, copious irrigation was performed with 5 mL 2.5% sodium hypochlorite (NaOCl) (Fórmula & Ação, São Paulo, SP, Brazil), and the canals were flooded continuously with irrigation solution from a NaviTip 31 G needle (Ultradent, South Jordan, UT, USA). Initial exploration was performed with a size 15 K Flexo-File (Dentsply-Maillefer, Ballaigues, Switzerland). Cervical and middle thirds were prepared with Orifice Shapers (Dentsply-Maillefer) driven by an X-Smart Plus motor (Dentsply-Maillefer). Afterward, the position of the AF was established by size 10 or larger K Flexo-Files (Dentsply-Maillefer) coupled to an apex locator (Root ZX II, J Morita, Kyoto, Japan), and confirmed by radiographs. The approximate size of the AF was determined by using K Flexo-Files size 10, 15, 20, 25 or 30 (Dentsply-Maillefer). This strategy was crucial for the instrumentation planning of similar LIFE procedures performed to treat different teeth (Table 1).

Instrumentation planning for similar large intentional foraminal enlargement (LIFE) to treat different teeth
Chemomechanical preparation was performed by using Profile 04 files (Dentsply-Maillefer) driven by the same motor mentioned above, using a crown-down approach. A 2.5 mL aliquot of 2.5% NaOCl was used as an irrigating solution at each file change, applied with a NaviTip 31 G (Ultradent) needle up to 5 mm short of the AF, as established by rubber stops. All the teeth received the same amount of irrigant.
After instrumentation, the canals were flooded with 3 mL of 17% ethylenediaminetetraacetic acid (Fórmula & Ação) for 3 minutes. A final flush with 5 mL of saline solution was performed, and the canals were dried with absorbent paper points (Dentsply-Maillefer). For each canal, the main cone corresponding to the last instrument used during chemomechanical preparation was calibrated and stabilized to approximately 1.5 mm from the AF to avoid overextension. After radiographic analysis of the level of the main cone, the root canal filling was performed by Tagger's hybrid technique and Endofill sealer (Dentsply-Maillefer), and the temporary restoration, with Cavitec (Caitech, São José dos Pinhais, PR, Brazil) or Cimpat (Septodont, São Paulo, SP, Brazil). A final radiograph was taken after occlusal adjustment (Figure 1), after which the patients were referred back to the Public Basic Health Unit of origin to receive the definitive restorations. No medication was prescribed, and the patient was instructed to take either paracetamol (750 mg every 6 hours) or ibuprofen (600 mg every 6 hours) if feeling pain [15]. All the treatments were performed by a single and experienced operator (R.M).
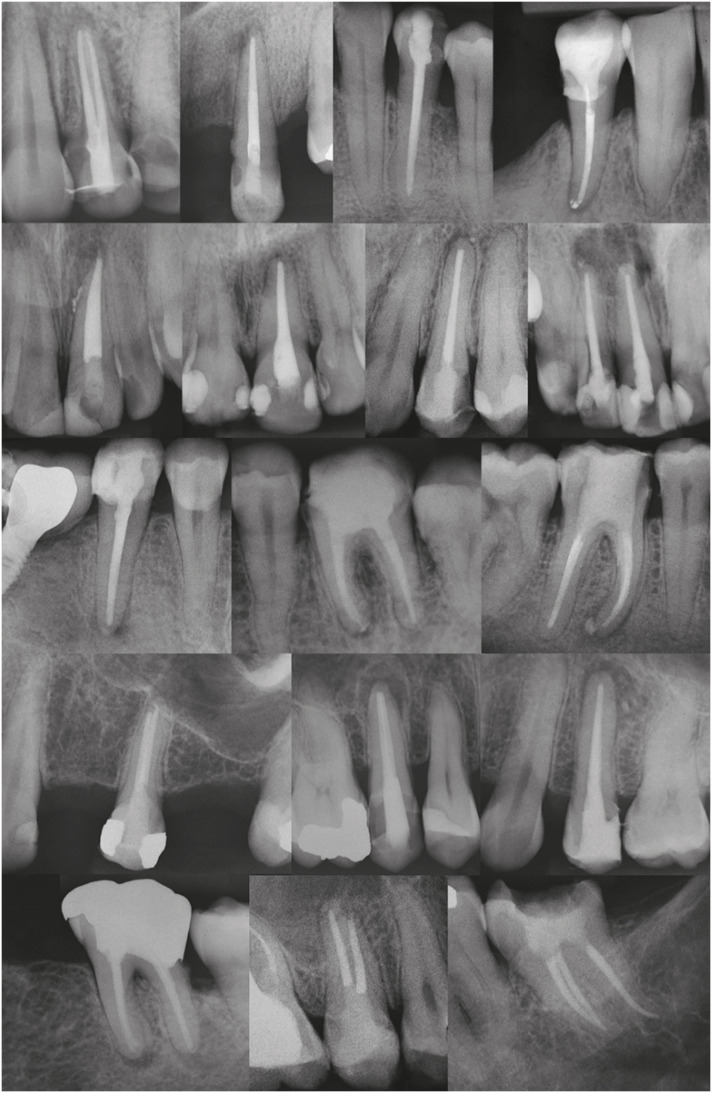
Examples of final radiographs.
Analysis of postoperative pain and statistical analysis
The assessment of postoperative pain was conducted at 24, 48 and 72 hours after the treatments, as outlined below. Phone calls were made for all the patients to inquire into their pain. The postoperative pain was classified according to a score based on a verbal categorization (Table 2) [1621].

Scores and features of the pain
The findings were recorded on an Excel spreadsheet (Microsoft Corp., Redmond, WA, USA) for statistical evaluation with SPSS software version 25.0 (IBM Corp., Armonk, NY, USA). Kolmogorov-Smirnov's test was used to evaluate the normality of data. Kruskal-Wallis, Mann-Whitney U, χ2, Friedman's analysis of variance and Friedman's multiple 2 to 2 comparison tests were used to determine significant any difference among the variables (p < 0.05).
RESULTS
Demographic data are being shown in Table 3. General incidence and levels of postoperative pain at the time points are shown in Figure 2. There was a tendency for the postoperative pain to decrease over time (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). Age, gender, periradicular status, tooth type and sealer extrusion did not influence the postoperative pain, regardless of time (p > 0.05) (Tables 4, 5, 6).

Demographic data
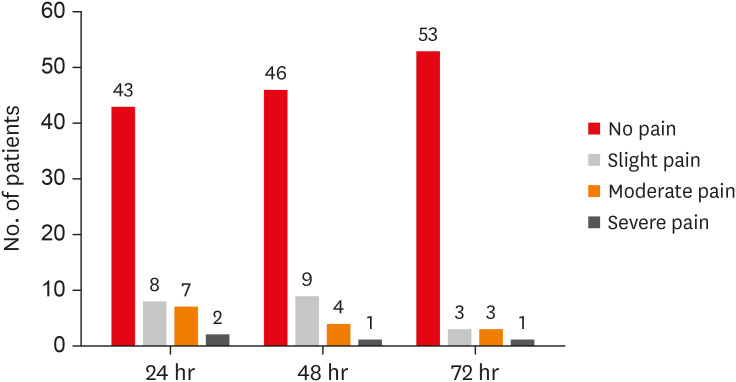
Incidence and levels of postoperative pain after 24, 48 and 72 hours.

Postoperative pain considering time and age, gender, periradicular status, and tooth type

Postoperative pain considering time frame

Postoperative pain considering sealer extrusion
DISCUSSION
The root canal system of necrotic teeth is contaminated, including the AF. Considering that the recommended treatment involves removing the cause of the disease, IFE could promote better cleaning by improving the condition for tissue repair [10]. However, it has been suggested that even small patency files used through the apex may cause an acute periapical inflammatory response and severe postoperative pain [22]. Therefore, a common concern regarding IFE is the postoperative pain related to physical iatrogenic trauma in the periapical region [14151623]. However, the AF in most dental groups is oval-shaped; consequently, better cleaning of this region could be achieved with LIFE [1017181920]. Up to now, the incidence and levels of postoperative pain have been evaluated only after performing endodontic treatments of necrotic teeth with IFE [141516]. Hence, the aim of this study was to perform the same analysis with LIFE.
Assessment of the incidence and levels of postoperative pain after performing endodontic treatment is a challenge due to the complexity of the intervention [13242526]. Assuming preoperative pain is a strong predictor of postoperative pain, only symptom-free patients were included in this study. Single-visit endodontic treatments have led to the same postoperative pain and healing of periapical tissues as 2-visit treatments [2728293031]. Therefore, all treatments were completed in a single visit, to minimize the number of procedures and variations of intracanal medication used [141529]. However, endodontic accesses had already been performed in previous appointments. Finally, it has been considered that operator experience may influence the incidence of postoperative pain [32]. For this reason, all treatments were performed by the same operator [141524].
Different methods have been used to assess pain after endodontic therapy, such as visual analog scales (VAS), scores based on verbal categorizations or both [15333435363738]. The design of the method is crucial and must ensure that the questions will be fully understood by the patients and easily interpreted by the researchers [1639]. In the present study, a score was used to classify postoperative pain, based on verbal categorizations, as follows: no, slight, moderate, and severe/acute pain. These categories were understood straightforwardly by patients. A similar strategy was used in other studies [1634353640].
Our results pointed out that age did not influence postoperative pain, thus corroborating the findings by Ng et al. [41] and Polycarpou et al. [42]. On the other hand, Ali et al. [40] showed a higher postoperative pain in older (41 to 65 years) compared with younger (15 to 40 years) patients. The probable reasons could be lower pain tolerance, less blood flow, and delayed healing. However, a direct comparison between our results and those obtained by the 3 previously cited studies [404142] should be made with caution. The age difference between the upper and lower limits of the age groupings of the cited studies [404142] was 10 years and 25 years. Herein, the limit was about 15 years. In addition, the number of patients in the study groups was very discrepant. In the study by Ng et al. [41] for example, 119 (28.7%) of the 415 patients were ≥ 40 and < 50 years old, and 8 (1.9%) were ≥ 80 years old. In the present study, 21 patients were < 30 years old, 21 patients were ≥ 30 and ≤ 50 years old, and 18 patients were > 50 years old, that is, a similar distribution of patients occurred herein regarding age.
Several studies have shown a higher prevalence of postoperative pain in females than males [133440]. The biological discrepancy between men and women could explain why [4344]. Moreover, comparing the difference between male and female reproductive and pelvic anatomies, females have an additional portal of entry of infection, thereby leading to possible local and distant hyperalgesia. Moreover, fluctuating female hormonal levels might be associated with changing levels of serotonin and noradrenaline, thus leading to increased pain prevalence in females during the menstrual period, and when receiving hormonal replacement therapy or taking oral contraceptives [134041]. However, our results pointed to no gender-related difference in postoperative pain. A plausible explanation is that a similar number of men and women (28/32) having similar ages (37.86 ± 18.55/38.38 ± 15.29, respectively) were treated herein. Healthy middle-aged women are likely to be less subject to the side effects associated with the above physical factors, and may therefore have responses to pain corresponding to those of men [4142].
The nature of the pulp and periapical status could modulate postoperative pain in endodontics. Teeth with nonvital pulps associated with periapical lesions are densely contaminated, and have an 83.2% prevalence of foraminal resorption [45]. In addition, disruption of the apical constriction by IFE causes greater debris extrusion, which is an important factor associated with postoperative pain [1117]. Nevertheless, our results showed that postoperative pain was not influenced by periradicular status. Marshall and Liesinger [46] observed that patients with periapical lesions that could not be detected by radiograph had more postoperative pain than those who had such lesions detected by radiograph. Ng et al. [41] indicated that postoperative pain was less in teeth having large periapical lesions (> 3 mm), compared with teeth having smaller or no periapical lesions. Genet et al. [47] showed that postoperative pain was greater in teeth with periapical radiolucency greater than 5 mm in diameter. A periapical lesion from an endodontic infection might exist without being visible in the radiograph [48]. It can be detected radiographically only when it attains nearly 30%–50% of the bone mineral loss [4950]. Other conditions, such as apical morphologic variations, surrounding bone density, X-ray angulations and radiographic contrast, also influence radiographic interpretation [51]. These factors may explain the conflicting results of the studies cited above and also the present findings [414647].
Some studies showed that postoperative pain was more frequent and higher in posterior teeth [133341]. This could be attributed to their more complex root canal anatomy [36]. Conversely, other studies pointed out that postoperative pain was not influenced by the tooth type [285253]. In this study, tooth type also did not influence postoperative pain. As mentioned previously, an experienced operator (R.M) performed all the treatments. This could have decreased the impact of the root canal anatomy, thus contributing to the low incidence and levels of postoperative pain.
Overall, mean pain scores were low, and just one patient reported severe/acute pain after 72 hours (1.66%). Similar results were obtained by Relvas et al. [35] in the group where the chemomechanical preparation was performed by a rotary system (ProTaper Universal). We believe that the low incidence and levels of postoperative pain observed in our study are probably related to the same reasons found by Relvas et al. [35] namely: a) only teeth with asymptomatic pulp necrosis were treated; b) all teeth suffered occlusal adjustment after the treatment; and c) in regard to the irrigation protocol, the same volume of irrigant was used, and the needle was inserted at a distance far enough from the apex to prevent extrusion.
Moderate pain was reported by 7, 4 and 3 patients after 24, 48 and 72 hours, respectively, implying that there was a tendency for pain to decrease over time (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). These results are in line with those obtained by a prospective, randomized, double-blind clinical trial performed by Shokraneh et al. [54] and a systematic review and meta-analysis conducted by Pak and White [55]. Nonetheless, Yaylali et al. [14] observed more pain in the 48-hour post-treatment period. This contradictory result may be attributed to the different methodological designs between the last cited study [14] and the current research. In the study by Yaylali et al. [14] only necrotic molars with radiographically visualized periradicular lesions were treated. Chemomechanical preparation was performed by using ProTaper Next files after establishing the working length (WL) at the AF. The irrigation consisted of 2.5% NaOCl using a Max-i-Probe needle up to 2 mm short of the WL, and the postoperative pain was evaluated by VAS. The authors did not report the approximate size of the AF. In our clinical protocol, the WL was determined at 2 mm beyond the AF. After measuring the approximate size of the AF with manual files, chemomechanical preparation was performed by using Profile 04 files to conduct the LIFE. Irrigation was performed with 2.5% NaOCl using a NaviTip needle up to 5 mm short of the AF, and the postoperative pain was evaluated with a score based on a verbal categorization.
Oxidative stress and, more specifically, reactive oxygen species (ROS) have been found to be linked to inflammatory pain in vivo [5657]. A recent study showed that the production of ROS increased 4- to 7-fold when the human pulp cells were treated with root canal sealers in vitro [58]. This led the authors of the present study to evaluate the relationship between postoperative pain and sealer extrusion; however, no correlation was observed. According to Sadaf and Ahmad [28], clinical symptoms are associated with the composition and amount of the extruded sealer. Cintra et al. [59] showed that Endofill had the least favorable characteristics regarding cell viability, compared with Sealer Plus, AH Plus, Endofill, and SimpliSeal. Furthermore, in the histologic analysis, severe inflammation was observed at 7 days, characterized by multinucleated giant cells, and most specimens presented severe inflammation even after 30 days. These results can be explained by the presence of eugenol, which was also responsible for the strong antimicrobial action of this sealer [60]. Endofill was used in the present study, but only slight sealer extrusion occurred in 24 cases, and did not have a significant influence on postoperative pain over time (p > 0.05) [28].
CONCLUSIONS
The incidence and levels of postoperative pain after performing endodontic treatments in necrotic teeth with LIFE were low and not influenced by gender, age, tooth type, periradicular status or sealer extrusion. When postoperative pain did occur, it tended to decrease over time.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Machado R.
Data curation: Machado R, Comparin D.
Formal analysis: Ignácio SA.
Funding acquisition: Machado R.
Investigation: Machado R.
Methodology: Machado R.
Project administration: Silva Neto UX.
Resources: Machado R.
Software: Machado R, Ignácio SA.
Supervision: Silva Neto UX.
Validation: Ignácio SA.
Visualization: Machado R.
Writing - original draft: Machado R, Comparin D.
Writing - review & editing: Silva Neto UX.





