Shaping ability and apical debris extrusion after root canal preparation with rotary or reciprocating instruments: a micro-CT study
Article information

Abstract
Objectives
The aim of this study was to evaluate the shaping ability of the TruShape and Reciproc Blue systems and the apical extrusion of debris after root canal instrumentation. The ProTaper Universal system was used as a reference for comparison.
Materials and Methods
Thirty-three mandibular premolars with a single canal were scanned using micro-computed tomography and were matched into 3 groups (n = 11) according to the instrumentation system: TruShape, Reciproc Blue and ProTaper Universal. The teeth were accessed and mounted in an apparatus with agarose gel, which simulated apical resistance provided by the periapical tissue and enabled the collection of apically extruded debris. During root canal preparation, 2.5% sodium hypochlorite was used as an irrigant. The samples were scanned again after instrumentation. The percentage of unprepared area, removed dentin, and volume of apically extruded debris were analyzed. The data were analyzed using 1-way analysis of variance and the Tukey test for multiple comparisons at a 5% significance level.
Results
No significant differences in the percentage of unprepared area were observed among the systems (p > 0.05). ProTaper Universal presented a higher percentage of dentin removal than the TruShape and Reciproc Blue systems (p < 0.05). The systems produced similar volumes of apically extruded debris (p > 0.05).
Conclusions
All systems caused apically extruded debris, without any significant differences among them. TruShape, Reciproc Blue, and ProTaper Universal presented similar percentages of unprepared area after root canal instrumentation; however, ProTaper Universal was associated with higher dentin removal than the other systems.
INTRODUCTION
During root canal preparation, organic and inorganic debris, bacteria, and irrigants may extrude into the periapical tissues [12]. This extrusion may result in undesirable consequences, such as postoperative pain and flare-ups, as well as the induction of local inflammation [3]. Flare-ups have been reported to occur in 1.4% to 16% of cases [4]. Thus, preventing the apical extrusion of debris is essential for reducing the incidence of those complications [5].
Some studies have reported that all root canal preparation techniques were associated with apical extrusion of debris, however, the amount of extruded debris varies among the different instrumentation systems [267]. The design of the instrument, cross-section, taper, the number of files employed, and cutting efficiency can influence the amount of debris or bacteria extrusion [891011].
Several laboratory studies have evaluated the amount of extruded debris after root canal preparation [6712]. However, a major limitation of these studies is that the resistance to extrusion offered by periapical tissues was not simulated. To overcome this problem, Alves et al. [13] recently proposed a new method for the assessment of apically extruded debris. This method consists of a quantitative analysis of the extruded debris volume, in an apparatus of agarose gel, through micro-computed tomography (micro-CT) scanning. Using this method, it is possible to simulate the resistance offered by periapical tissues and the use of sodium hypochlorite (NaOCl) as an irrigant during the experimental procedures, allowing a better simulation of clinical conditions than is possible with other methods commonly used in apical extrusion studies. Moreover, due to the non-destructive nature of micro-CT technology, it is possible to evaluate other shaping outcomes in combination with debris extrusion evaluation. However, only 2 single-file nickel-titanium instruments, the XP-endo Shaper (FKG Dentaire, La Chaux-de-Fonds, Switzerland) and Reciproc (VDW, Munich, Germany), have been evaluated with this new method.
Recently, a novel heat-treated NiTi rotary system, TruShape 3D Conforming Files (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA), was introduced to the endodontic market. This system has a characteristic longitudinal S-shaped design and a 0.06 regressive taper. According to the manufacturer, this innovative design enables a larger contact surface with the walls of the canals, while promoting the preservation of dentin during the shaping of the root canal, conserving the integrity of the root structure [14]. Reciproc Blue (VDW) is the new generation of Reciproc instruments. It presents the same cutting S-shaped cross-section as the Reciproc files, however, it is manufactured with a proprietary thermal treatment that results in the deposition of a blue titanium oxide layer on its surface, which significantly improves flexibility and reduces the risk of fracture in comparison to the M-wire Reciproc file [15161718].
Considering the advantages of the new proposed method and the limited number of studies that have investigated this issue using the new methodology, it is evident that this topic needs to be better explored. Thereby, this study evaluated the shaping ability, measuring surface area, volume before and after instrumentation, and unprepared root canal area, as well as the volume of apically extruded debris, after TruShape and Reciproc Blue root canal instrumentation using micro-CT, with an agarose gel apparatus simulating the periodontal tissues. The ProTaper Universal system was used as a reference for comparison. The null hypotheses tested were that there would be no significant differences among the tested instruments in terms of 1) their shaping ability and 2) the amount of apically extruded debris.
MATERIALS AND METHODS
Sample size estimation
Based on a previous study, a power calculation was performed using G*Power 3.1 software (Heinrich Heine University, Dusseldorf, Germany) with an effect size of 2.06, power (β) = 80%, and α = 5% entered into an F-test family for 1-way analysis [19]. The calculation indicated that the minimum sample size for each group was 9 teeth. Two additional specimens per group were added to compensate for possible sample loss.
Sample selection
This study was approved by the Juiz de Fora Federal University Ethics Committee (number 2.001.443). Thirty-three mandibular premolars with a fully formed apex, no fractures, no previous endodontic treatment, and 1 root canal were selected. The specimens were scanned in a micro-CT device (SkyScan 1174, Bruker, Kontich, Belgium) using the following parameters: 50 kV and 800 mA, an isotropic resolution of 22 µm, 180º rotation around the vertical axis, a rotation step of 1 and a 0.5-mm-thick aluminum filter. The images were reconstructed with NRecon software (Bruker) using a 26% beam hardening correction, a smoothing of 7, and a ring artifact correction of 3. After reconstruction of the images, the teeth used in the ProTaper Universal, TruShape and Reciproc Blue groups were matched to create 11 groups of 3, based on similar surface area, volume, and 3-dimensional (3D) configuration, obtained by the software programs CTAn (v. 1.6.6.0, Bruker MicroCT N.V., Kontich, Belgium) and CTvol (Bruker MicroCT N.V.), respectively. Only premolars with a Vertucci type I classification were selected [20]. Moreover, the diameter of root canals 1 mm above the foramen was evaluated (CTAn software, Bruker MicroCT N.V.) and only teeth with similar diameters were selected for the experiment (from 0.20 to 0.25 mm). Teeth not matching this last criterion were excluded. Each single specimen of each trio was assigned into one of the 3 experimental groups (n = 11) according to the system applied to the root canal instrumentation.
Coronal access was made with a 1014HL round diamond bur (KG Sorensen, Cotia, SP, Brazil) and an Endo-Z bur (Dentsply Sirona, York, PA, USA). Apical patency was confirmed by inserting a size 10 K-file into the root canal until its tip was visible at the apical foramen, and the working length (WL) was set 1.0 mm short of this measurement.
Apparatus to collect extruded debris
An apparatus previously described was adopted in this study to collect extruded debris [19]. Each specimen was fixed on the lid of an Eppendorf tube, through a previously custom-made hole in such a way that the apical 5-mm segment of the specimen was inside the tube and its coronal portion was outside. The space between the specimen and Eppendorf tube was sealed with Top Dam (FGM, Joinville, SC, Brazil).
Subsequently, the Eppendorf tube was flipped upside down and the bottom part was cut off, creating an opening where 1.5% agarose gel was poured until the apical root was completely covered. The apparatus remained in the same position until the gel solidified (Figure 1). The apparatus with agarose gel was necessary for the quantification of extruded debris using micro-CT because it provided a matrix to collect debris. In addition, agarose gel simulated the resistance offered by the periapical tissues [19].
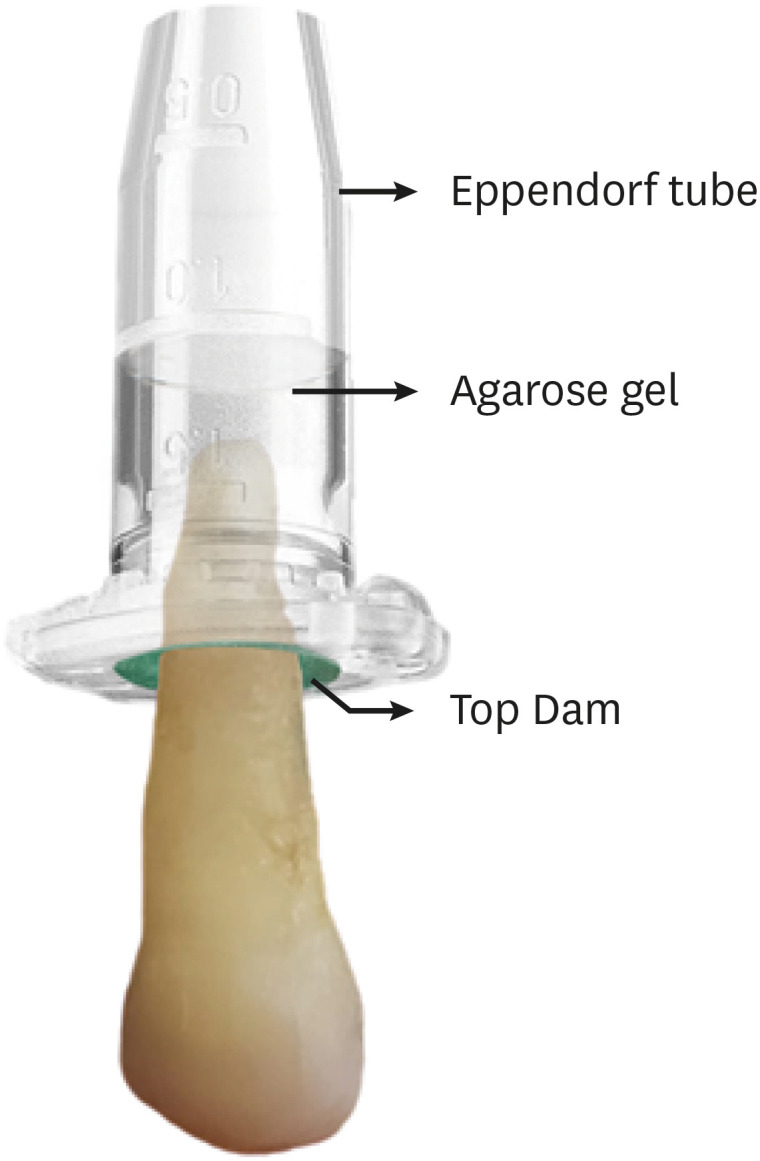
Eppendorf tube and agarose gel apparatus with a tooth fixed. The visible line indicates the agarose gel level inside the tube.
Root canal preparation
1. ProTaper Universal group
The instruments were operated with a VDW Silver motor (VDW GmbH, Munich, Germany) at 250 rpm and 3.5 N·cm according to the instructions provided by the manufacturer. Initially, the root canal was rinsed with 2 mL of 2.5% NaOCl, a glide path was prepared with a size 15 K-file, and the root canal was once again irrigated with 2 mL of 2.5% NaOCl. The root canals were instrumented with a gentle in-and-out pecking motion using the ProTaper Universal system (Dentsply Maillefer, Ballaigues, Switzerland) in the following sequence: S1 (18/0.02), S2 (20/0.04), F1 (20/0.07), F2 (25/0.08), F3 (30/0.09) and F4 (40/0.06). S1 and S2 were used with a brushing outstroke motion until the WL, and F1–F4 was used without a brushing outstroke motion at the WL.
2. TruShape group
Each instrument was operated using a VDW Silver motor (VDW GmbH) at 300 rpm and 3 N·cm, according to the instructions provided by the manufacturer. After irrigation with 1 mL of 2.5% NaOCl, a glide path was prepared with a size 15 K-file. Subsequently, another 1 mL of 2.5% NaOCl was used and the canal was instrumented up to the WL by the sequential use of TruShape instruments (Dentsply Sirona) 20/0.06, 25/0.06, 30/0.06, and 40/0.06. A gentle in-and-out pecking motion of about 2–3 mm in amplitude with light apical pressure was applied to each instrument until it reached the WL.
3. Reciproc Blue group
The Reciproc Blue R40 (40/0.06v) (VDW) instruments were driven with the VDW Silver motor (VDW GmbH) in “Reciproc All” mode, according to the instructions provided by the manufacturer. The canal was rinsed with 2 mL of 2.5% NaOCl and a glide path was prepared with a size 15 K-file. Another round of irrigation with 2 mL of 2.5% NaOCl was performed, and the Reciproc R40 instrument was used at the coronal, middle, and apical thirds.
After use or insertion, each instrument was removed from the root canal and cleaned with sterile gauze. The teeth were irrigated with 2.5% NaOCl after the use of each instrument and the patency was checked using a size 15 K-file at the apical foramen after the use of each instrument. In all groups, the root canals were irrigated with a total of 10 mL of 2.5% NaOCl with 30-G Endo-Eze needles (Ultradent Products Inc., South Jordan, UT, USA) inserted 3 mm up from the apical foramen. The final irrigation was performed with 2 mL of NaOCl followed by 2 mL of 17% ethylenediaminetetraacetic acid for 1 minute and 2 mL of NaOCl. The canals were then subjected to micro-CT scanning.
All root canal instrumentations were performed by a single operator, specialized in endodontics with 6 years of experience. Each instrument was used for a single tooth and then discarded.
Micro-CT analysis
The specimens were rescanned using micro-CT (Skyscan 1173, Bruker) with the same parameters described previously.
1. Shaping ability
The images acquired before and after the root canal instrumentation were coregistered using an affine algorithm of the 3D Slicer [21]. ImageJ (National Institutes of Health, Bethesda, MD, USA) was used to calculate the volume (mm3) and surface area (mm2) before and after root canal instrumentation. The percentage of unprepared area were calculated as the number of static voxels (voxels present in the same position on the canal surface before and after instrumentation) divided by the total number of voxels present on the canal surface, according the following formula [22]:

The volume of dentin removed after root canal preparation was quantified by subtracting pre-and post-segmented root dentin using morphological operations (ImageJ) [23].
2. Extruded debris
The 3D quantitative analysis of the extruded debris volume was performed using CTAn software (Bruker MicroCT) through the binary selection tool. The histogram values were defined for all specimens (40-255) and the region of interest was defined for each specimen. The extruded debris was then quantified using the morphometry plug-in.
Statistical analysis
The normal distribution of data was confirmed by the Shapiro-Wilk test (p > 0.05). The volume (mm3) and surface area (mm2) of the root canal before instrumentation were compared to confirm the hypothesis of similar anatomical conditions between the groups. One-way analysis of variance was used to compare the results among the groups. A post hoc analysis was performed using the Tukey test for multiple comparisons. The Fisher exact test was used to compare the volume of apically extruded debris among the groups. The level of significance was set at α = 5%. SPSS version 17 (SPSS Inc., Chicago, IL, USA) was used to perform the statistical analysis.
RESULTS
The preliminary assessment regarding volume and surface area within the canals showed similar results among the groups at baseline (p > 0.05). There was no significant difference in the surface area after root canal preparation or in the final volume between groups (p > 0.05). No significant differences were observed in the percentage of unprepared area according to the instrument used (p > 0.05) (Figure 2). ProTaper Universal demonstrated higher percentages of removed dentin than the TruShape and Reciproc Blue instruments (p < 0.05) (Table 1). The evaluated instruments produced similar volumes of apically extruded debris (p > 0.05). Debris extrusion was detected in 4 (36%), 8 (73%), and 7 (64%) canals in the ProTaper Universal, TruShape, and Reciproc Blue groups, respectively, which also was not a statistically significant difference (Figure 3).
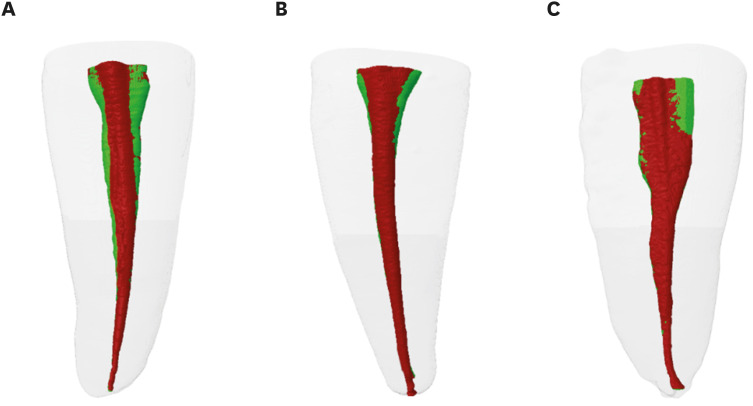
Representative 3-dimensional images of the root canals before (green) and after instrumentation (red) with (A) ProTaper, (B) TruShape, and (C) Reciproc Blue.

Root canal parameters before and after preparation, percentage of unprepared area, and amount of extruded debris of each experimental group

Micro-computed tomography 3-dimensional reconstruction of extruded debris in the (A) ProTaper, (B) TruShape, and (C) Reciproc Blue groups.
DISCUSSION
Micro-CT is a non-destructive method that allows a 3D visualization of the root canal anatomy and the unprepared area after root canal preparation [24]. In addition, micro-CT scanning makes it possible to determine the presence, location, and quantity of the volume of hard tissue debris accumulated inside the root canal system after preparation and, within the newly proposed method, the debris extruded via the apical foramen [13]. Thus, this study evaluated the instrumentation efficacy and the apical extrusion of debris after root canal instrumentation with the ProTaper Universal, TruShape, and Reciproc Blue systems through a micro-CT analysis. To this date, no studies have analyzed the shaping ability and debris extrusion of the aforementioned instruments using micro-CT.
The vast majority of previous studies regarding debris extrusion calculated extruded debris by weight, but this method does not simulate the resistance offered by periapical tissues. In this study, the collection of extruded debris was performed with an agarose apparatus, in a similar manner as described in a previous study [19]. The 1.5% agarose gel simulated the resistance offered by the periapical tissues and provided a matrix to collect and quantify the apically extruded debris, by means of micro-CT analysis [25].
NaOCl was used as an irrigating solution to simulate clinical conditions. The possibility of crystallization of NaOCl does not compromise the results because the extruded debris was evaluated by micro-CT analysis and not by weight. In addition, a previous study demonstrated that there was no interaction between NaOCl and agarose gel, meaning that this system is suitable for the analysis of extruded debris [26].
For the standardization of specimens, the 3D configuration, area, initial volume, and apical diameter were calculated, and the teeth were divided into 3 homogeneous groups. In addition, apical preparation was finished at the WL by using instruments with the same apical size and taper (40/0.06), allowing a better comparison between groups. ProTaper Universal was used as a comparison system since it is a multi-file rotary system that has been widely studied in the literature and because it has the same tip size and taper as the TruShape and Reciproc Blue systems (40/0.06) [27282930].
Unprepared canal areas can compromise the disinfection of the root canal system and allow maintenance of the infectious process, as these areas can be colonized by biofilms, which in turn may cause endodontic failure [31]. In this study, no significant differences in the percentage of unprepared area were observed among the ProTaper Universal, TruShape and Reciproc Blue systems; thus, the first null hypothesis was accepted. The present results are corroborated by a previous study that demonstrated similar shaping abilities among ProTaper Next, Reciproc, Reciproc Blue, and TruShape [32]. However, the results of this study partially contradict those of Guimarães et al. [33], who compared the percentage of unprepared area between TruShape and Reciproc instruments in oval canals and showed that TruShape resulted in a smaller unprepared area in the full canal length than Reciproc. This difference could be explained by the fact that in this study, the Reciproc Blue instrument was used. These instruments undergo a blue heat treatment in the manufacturing process that increases their flexibility when compared to the M-wire Reciproc instrument [16]. This extra flexibility may potentially lead to better preparation results.
Regarding the removal of dentin, in this study, ProTaper Universal showed higher percentages of removed dentin than the other groups. These results are in line with the study of Serefoglu and Piskin [34], which showed that ProTaper Universal removed a greater amount of dentin than self-adjusting file instruments, designed to adapt 3-dimensionally to the cross-sectional shape of the canal. This result can be explained by the differences in design and kinematics among the tested instruments [35], and the fact that ProTaper Universal has a multi-tapered design and a good cutting efficiency, which results in a greater removal of dentin [36]. Zuolo et al. [35] also found no statistically significant differences regarding the removal of dentin between TruShape and Reciproc, which is corroborated by the results of this study.
In this study, all tested rotary (ProTaper Universal and TruShape) and reciprocating (Reciproc Blue) instruments showed apically extruded debris, similar to previous studies which demonstrated that, regardless of the type of movement, all instruments resulted in some degree of apical debris extrusion [121537]. ProTaper Universal, TruShape and Reciproc Blue produced a similar volume of apically extruded debris (p > 0.05), with no significant differences between the reciprocating and rotary instruments. Thus, the second null hypothesis was accepted. This result agrees with previous studies that evaluated other instruments and did not find differences among them [61938]. However, a reduced amount of apically extruded debris associated with reciprocating systems has been reported sporadically [1237]. The results in the literature are still inconsistent, reflecting differences among studies in factors such as the design of instruments, number of files, irrigation protocols, and type of teeth used.
The study by Alves et al. [13] was the only study to evaluate extruded debris through micro-CT analysis and verified similar amounts of extruded dentinal debris during instrumentation with Reciproc and XP-endo Shaper. In the present study, ProTaper Universal, Reciproc Blue, and TruShape were evaluated. Despite the differences in the tested instruments, neither study found significant differences in debris extrusion using the micro-CT methodology.
Previous studies demonstrated that ProTaper Universal showed a higher amount of apically extruded debris than single-file reciprocating systems, which contradicts the results of this study [2839]. This difference can be explained due to methodological discrepancies. While previous studies assessed data on debris by weight, the present study assessed the amount of using micro-CT images. In addition, a distinctive factor of this study is the use of agarose gel, which acted as a barrier and may have provided more resistance to extruded debris [19].
CONCLUSIONS
ProTaper Universal, TruShape, and Reciproc Blue instruments showed similar shaping abilities. ProTaper Universal resulted in a greater volume of removed dentin. All instruments generated apical extrusion of debris, without statistically significant differences in volume among the groups.
Notes
Funding: This study was partially funded by FAPERJ and CNPq.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Silva EJNL, Sassone LM.
Formal analysis: Silva EJNL.
Investigation: Barbosa AFA, Lacerda MFLS.
Methodology: Moura SG, Misael WF.
Project administration: Lima CO, Barbosa AFA.
Resources: Sassone LM, Silva EJNL.
Software: Lima CO, Barbosa AFA.
Supervision: Sassone LM.
Writing - original draft: Lima CO, Barbosa AFA.
Writing - review & editing: Lacerda MFLS, Silva EJNL.
