Isthmuses, accessory canals, and the direction of root curvature in permanent mandibular first molars: an in vivo computed tomography study
Article information

Abstract
Objectives
This study was performed to assess the anatomy of mandibular first molars.
Materials and Methods
In this in vivo study, cone-beam computed tomography (CBCT) volumes of 312 bilateral intact first mandibular molars from 156 patients (79 men and 77 women; average age, 35.6 ± 11.2 years) were investigated in terms of the direction of each canal's curvature in the buccolingual and mesiodistal dimensions (direction of the position of the apex in relation to the longitudinal axis of the root), the presence of an isthmus (a narrow, ribbon-shaped communication between 2 root canals) in 3 segments (0–2, 2–4, and 4–6 mm) from the apex), and the presence and number of accessory canals (smaller canals besides the main root canals, connecting the pulp to the periodontium). Data were analyzed statistically (α = 0.05).
Results
Mesiolingual canals were mostly buccally and distally inclined, while mesiobuccal and distolingual canals were mostly distally curved. Isthmuses were more common in younger patients (χ2 test, p < 0.05). The average numbers of accessory canals in the apical, middle, and coronal segments were 9.9 ± 4.2, 6.9 ± 2.9, and 9.3 ± 3.0 canals per segment, respectively (analysis of variance, p < 0.001). Age and sex were not associated with the number of accessory canals (p > 0.05).
Conclusions
The complex anatomy of these teeth deserves attention during non-surgical or surgical endodontic treatment. Around the apex, isthmuses might be more prevalent in younger and female individuals.
INTRODUCTION
Proper outcomes of endodontic treatment rely on the practitioner's knowledge of root canal anatomy, appropriate visualization, and meticulous cleaning and shaping of root canals. Lack of knowledge of canal morphology, the presence of thick radicular walls around the canal, and anatomical variations might contribute to an increased risk of failure [123].
The morphological configuration of radicular canals depends greatly on ethnicity, which necessitates the establishment of various norms regarding the predominant configurations in each population [3]. A root canal isthmus (also called a lateral interconnection, corridor, or transverse anastomosis) is a narrow, ribbon-shaped communication between 2 root canals; this structure is of crucial clinical importance because it can contain necrotic pulp tissue, along with microbial populations and their byproducts [456]. Accessory root canals are smaller canals alongside the main root canals, which connect the pulp to the periodontium through other routes than the main canal, thereby potentially compromising periodontal health or endodontic success [78910].
Permanent mandibular first molars erupt very early and have rather convoluted surfaces. Therefore, they are prone to caries formation and hence are among the teeth that most commonly require endodontic treatment. This makes knowledge of their anatomic properties even more critical [231112]. Most of the time, 3 canals within 2 roots can be seen in these teeth, but ethnic and interindividual variations are frequent [231112].
This study was conducted because of the abovementioned importance of radicular anatomy and the inconsistent outcomes of the few studies that have been conducted on the Iranian population [123], because many studies on radicular anatomy have utilized conventional or 2-dimensional radiographic methods that might not be as accurate as 3-dimensional (3D) radiographic techniques [1314], and finally because many morphological characteristics have not been evaluated by many studies, either domestic or international [12]. This study aimed to evaluate certain aspects of the root and canal morphology of permanent mandibular first molars (i.e., root direction, the presence of isthmuses, and the presence of accessory canals) in a large sample of cone-beam computed tomography (CBCT) volumes.
MATERIALS AND METHODS
This in vivo cross-sectional analytical study was done on CBCT volumes obtained retrospectively from patients aged 20 to 60 years old who had visited 2 centers in Tehran (a private radiology center and the oral radiology department). All CBCT volumes had been taken solely for clinical purposes, and there was no risk of any extra X-ray exposure to patients for the sake of this research. The protocol received ethical approval from the research committee of Azad University of Medical Sciences, Dental Branch, Tehran, Iran (thesis No. 14859) [12].
The inclusion criteria comprised complete patient information; the presence of both mandibular first molars; the absence of resorption, agenesis, fractures, open apices, or any pathology; and no history of any previous endodontic treatment. All included CBCT scans were obtained using the same device and settings (NewTom, GiANO, Verona, Italy; field of view, 8 × 5 cm; focal size, 0.3 mm; 12 mA; 85 kVp; 0.4 seconds) [12].
The collected sample consisted of 312 teeth in 156 patients, including 79 men and 77 women with a mean age of 35.58 ± 11.17 years [12]. Of the subjects, 101 (64.7%) were between 20 and 39 years old, and 55 were between 40 and 60 years old. CBCT slices were investigated in the sagittal, coronal, and axial planes. All assessments were performed using NNT software (version 4.5, NewTom) by a dentist who had been trained by a maxillofacial radiologist [12]. The sample size was determined to be twice as large as the sample size of a previous study [15]. Specimens were collected randomly from an archive of CBCT scans until 156 patients with bilateral mandibular first molars who satisfied the other inclusion criteria were identified.
The evaluated anatomical parameters comprised the direction of each canal’s curvature in the buccolingual and mesiodistal dimensions (defined as the direction in which the root apex was positioned in relation to the longitudinal axis of the root); the presence of an isthmus (according to the criteria presented by Hsu and Kim [416]) in 3 segments defined in terms of distance from the apex (0–2 mm, 2–4 mm, and 4–6 mm); and the presence and number of accessory canals (Figure 1).
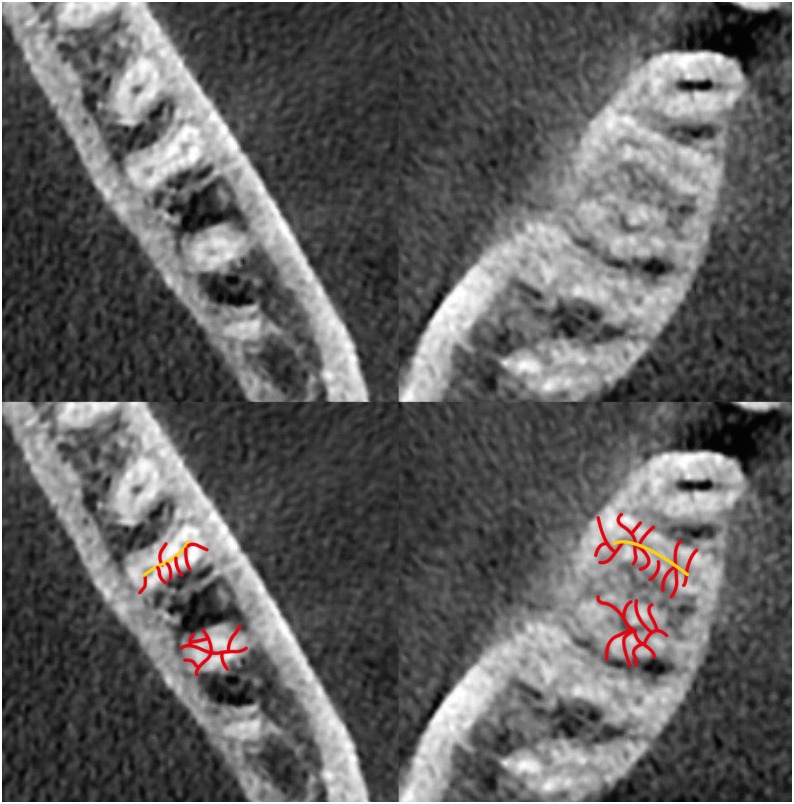
An example of accessory canals. In the bottom image, the main (yellow) and accessory (red) canals are marked.
Descriptive statistics were calculated for the parameters. The χ2 test was used to compare the groups. Correlations were evaluated using the Spearman correlation coefficient. Accessory canal counts were compared using the paired t-test, analysis of variance (ANOVA), and least significant difference (LSD) tests in SPSS version 24 (IBM Corp., Armonk, NY, USA). The level of significance was set at p ≤ 0.05.
RESULTS
As detailed in an earlier report [12], 16 bilateral teeth in 8 patients had 3 roots (the third root was distolingual in all of those cases). The remaining teeth had 2 roots. The mesial roots of 271 teeth had 2 canals, while in 42 mesial roots, there were 3 canals. Of the distal roots, 136, 165, and 11 had 1, 2, and 3 canals, respectively. There were 16 distolingual roots, each having 1 canal [12].
Canal curvatures
The results for canal curvature are summarized in Table 1. The mesiobuccal canals were mostly not inclined toward the buccal or lingual sides, but were instead distally inclined. The mesiolingual canals were mostly buccally and distally inclined. The distolingual canals were distally oriented, and mostly showed no inclination toward the buccal or lingual sides.

Distribution of apical foramen locations in mesiobuccal, mesiolingual, distobuccal, and distolingual canals
Internal communications (isthmuses)
In the spans farther from the apex, the probability of observing an isthmus increased. Isthmuses were more common in subjects aged between 20 and 40 years old than in those aged between 40 and 60 years old (χ2 test, p < 0.05, Table 2). In the segment 0–2 mm away from the apex of mesial roots, 36.4% of women and 24.1% of men showed isthmuses, and this difference was significant (p = 0.018). In the segment 2–4 mm away from the apex of mesial roots, 56.5% of women and 45.6% of men showed isthmuses (p = 0.054). Non-significant differences were seen in the segment 4–6 mm away from the mesial root apex (64.9% of women and 59.9% of men, p = 0.322). Similar results were observed in the segment 0–2 mm away from the distal root (22.1% of women and 16.5% of men, p = 0.208). The only segment with a higher prevalence of isthmuses in men than in women was 2–4 mm away from the apex of distal roots (33.5% in men and 25.3% in women), although this difference was not significant (p = 0.111). Non-significant differences were seen in the segment 4–6 mm away from the distal root (40.9% of women and 33.5% of men, p = 0.178).

Distribution of isthmuses in each root segment
Accessory canals
The average numbers of accessory canals in the apical, middle, and coronal segments were 9.9 ± 4.2, 6.9 ± 2.9, and 9.3 ± 3.0 canals per segment. The fewest accessory canals were seen in the middle third of roots (ANOVA, p < 0.001, Table 3). Post hoc comparisons between sections were all significant (LSD test, p < 0.005). The average numbers of accessory canals in the mesial and distal roots were 14.1 ± 5.1 and 11.9 ± 4.3, respectively. Accessory canals were more prevalent in mesial roots than in distal roots according to the paired t-test (p < 0.001). No significant association was found between age and the number of accessory canals according to the χ2 and Spearman tests (p > 0.05). Sex was not associated with the number of accessory canals (Spearman test, p > 0.05).

Number of accessory canals per root segment
DISCUSSION
In the present study, the mesiolingual canals usually had a distobuccal orientation, while the mesiobuccal, distobuccal, and distolingual canals had a distal orientation. In many previous studies on the curvature of mandibular first molar root canals, the curvature of the roots was assessed, but not the direction of canal curvature. Some studies have evaluated canal curvature using various methods such as the Schneider technique [21718] (Table 4); however, no studies have evaluated the direction of canal curvature. Rocha et al. [19] performed an in vitro study using the clearing technique to assess root curvature in 232 teeth and reported a 73% proportion of distal inclinations (and 17% straight roots) in mesial roots, while among distal roots, 8% showed distal inclinations, 12% had mesial inclinations, and 78% were straight. Schäfer et al. [18] conducted an in vitro CBCT study on 50 teeth and reported that 58% to 76% of canals were curved, with angles of 33° to 48°. Estrela et al. [17] performed an in vivo CBCT study on 200 teeth and observed a 92.7% proportion of curvature in the apical third and a 73.2% proportion of curvature in the cervical third (Table 4). Curved canals can jeopardize the outcome of endodontic treatment, and should be dealt with through various techniques, such as flaring of the cervical portion and the use of more advanced imaging technologies such as 3D radiography [17].

Summary of reports on root and canal curvature
de Pablo et al. [20] reviewed previous articles and stated that internal communications are mostly seen in the middle parts of the root. In the segment 4–6 mm away from the apex, isthmuses were observed in 79.5% of mesial roots and 57.5% of distal roots in this study. Previous studies have shown a wide range of results; for example, Zafar and Alrahabi [21], Arjmand et al. [22], and Masoudi et al. [23] reported a low prevalence of isthmuses, while many other studies reported higher prevalence rates (10%, 30%, 37.3%, 44.6%, 61%, 62%, 69.2%, 77.4%, 81%, 85, and 88.5% in mesial roots [468910242526], and 5%, 8%, 9.2%, 10%, 11.3%, 12%, 13%, and 27.3% in distal roots [24678910202425272829]) (Table 5). These discrepancies can be attributed to ethnic and methodological differences. Previous studies agree that internal communications may be more common in mesial roots than in distal roots, which might be due to the greater development and complexity of mesial roots. According to Villas-Bôas et al. [25], the mesial roots of molars do not follow a fixed pattern, and isthmuses are quite frequent in the apical third. Gu et al. [24] suggested that like other pulp structures, isthmuses might become narrower with age and hence disappear if they were originally narrow enough. Peiris et al. [10] also found age to be an important factor affecting the prevalence of isthmuses and concluded that during the fourth decade of life, canal development increases considerably, which is why internal communications become considerably less common after 40 years of age. Consistently, in this study, isthmuses were about 2 times more frequent in younger patients than in older ones. Inconsistencies in statistics on the prevalence of isthmuses may be due to ethnic and methodological differences, such as variation in the age ranges of patients. In younger patients, the internal structures of the dental pulp are not yet completed [10], and in older people, internal structures have become narrowed or in some areas have completely collapsed. We also obtained the novel finding that in areas close to the apex, isthmuses might be more prevalent in females. We could not find any other studies assessing this issue.

Summary of reports on isthmus prevalence and locations (all reported values are percentages)
In this study, the prevalence of accessory canals was not influenced by sex or age. However, accessory canals were more prevalent in the apical and coronal segments than in the middle segments, and in mesial roots than in distal roots. The average number of accessory canals seen in mesial roots was 5, 4, and 5.5, respectively, in the coronal, middle, and apical segments, while in distal roots, the average number of accessory canals was 4.5, 3, and 4.5, respectively, in the coronal, middle, and apical segments. As Table 6 summarizes, very few studies have evaluated the presence of accessory canals in mandibular molar roots, and the studies that have done so used only conventional clearing, staining, and observation methods, which can account for the observed differences. Al-Qudah and Awawdeh [7] assessed 330 teeth, and reported a 1% prevalence of accessory canals in mesial roots (0.6% in the middle third, 0.3% in the apical third) and a 3% prevalence in distal roots (all in the apical third). Ahmed et al. [8] evaluated 100 teeth and observed accessory canals in 52% of mesial roots. Gulabivala et al. [9] assessed 139 teeth and reported an 11% prevalence of accessory canals in the apical third. Peiris et al. [10] investigated 177 first and second molars and determined the prevalence of accessory canals to be 45.2% in the apical third and 29.4% in the apical third. As for isthmuses, ethnicity and age may be sources of differences, as canals might be wider in younger teeth and therefore easier to detect or stain, while in older teeth, canals might have been narrowed or even obstructed by dentin deposition. CBCT scans can be obtained in various 3D planes without any damage to the root, which allows the researcher to check the results from other points of view. Moreover, CBCT assessments are not dependent on dyeing and dye viscosity. In contrast, conventional techniques rely on the staining of accessory canals, which depends on dye viscosity and therefore might fail in narrow accessory canals. Furthermore, in conventional techniques, it is impossible to section the tooth without losing it.

Summary of reports on the prevalence and location of accessory canals (all reported values are percentages)
Different views exist regarding the superiority of digital or conventional assessments. Some studies have recommended the traditional clearing technique over radiography [230]. According to Neelakantan et al. [31], CBCT might be as accurate as in vitro techniques. Nevertheless, according to other authors, 3D radiography techniques might be more accurate than clearing and dyeing [213]. It should be noted that CBCT might expose the patient to X-ray radiation in unnecessary areas; therefore, the as low as reasonably achievable (ALARA) principle should be taken into account. However, in this retrospective study, only archived CBCT scans were used; therefore, no additional X-ray exposure occurred in any patients for the sake of this research. In other words, the dosage and field of view of the X-rays were determined exclusively based on patients' clinical needs in accordance with the ALARA principle.
Since permanent mandibular first molars are among the most frequent teeth that need root canal therapy, knowledge of their anatomy is of clinical importance [231112]. For instance, such anatomical information may be useful for the 3-mm cutting and 3-mm retrofilling used to obtain a hermetic seal of the roots of diseased mandibular first molars during surgical endodontic procedures.
CONCLUSIONS
Mesiolingual canals were mostly buccally and distally inclined, while mesiobuccal and distolingual canals were mostly distally curved. Isthmuses might be more frequent in younger individuals and in women (especially in areas closer to the apex). In the apical, middle, and coronal segments of roots, there might be about 10, 7, and 9 accessory canals per segment, with the middle third generally having the fewest such canals. Accessory canals may be more frequent in mesial roots; in mesial and distal roots, there might be about 14 and 12 accessory canals, respectively. The number of accessory canals appears not to be influenced by age or sex. Based on the results of this study, mandibular first molars have a complicated root canal system, with widespread isthmuses and anatomical variations, and therefore require more attention during access cavity preparation and root canal therapy.
ACKNOWLEDGEMENTS
The authors wish to thank Dr. Zohre Khalilak, Dr. Nahid Akhlaghi, and Dr. Ladan Hafezi for their assistance with this research.
Notes
Conflict of Interest: The authors declare that they do not have any conflict of interest.
Author Contributions:
Conceptualization: Chuppani Dastgerdi A.
Data curation: Chuppani Dastgerdi A.
Formal analysis: Rakhshan V.
Funding acquisition: Navabi M.
Investigation: Chuppani Dastgerdi A, Navabi M, Rakhshan V.
Methodology: Chuppani Dastgerdi A, Navabi M.
Project administration: Chuppani Dastgerdi A, Navabi M, Rakhshan V.
Resources: Chuppani Dastgerdi A.
Software: Chuppani Dastgerdi A, Rakhshan V.
Supervision: Navabi M.
Validation: Chuppani Dastgerdi A, Navabi M, Rakhshan V.
Visualization: Chuppani Dastgerdi A, Rakhshan V.
Writing - original draft: Chuppani Dastgerdi A, Navabi M, Rakhshan V.
Writing - review & editing: Chuppani Dastgerdi A, Navabi M, Rakhshan V.





