A micro-computed tomography evaluation of voids using calcium silicate-based materials in teeth with simulated internal root resorption
Article information

Abstract
Objectives
The obturation quality of MTA, Biodentine, Total Fill BC root canal sealer (RCS), and warm gutta-percha (WGP) in teeth with simulated internal root resorption (IRR) was evaluated by using micro-computed tomography.
Materials and Methods
Standardized IRR cavities were created using 40 extracted maxillary central incisor teeth and randomly assigned into 4 groups (n = 10). IRR cavities were filled with MTA, Biodentine, Total Fill BC RCS (bulk-fill form) and WGP + Total Fill BC RCS. Percentage of voids between resorptive cavity walls and obturation material (external void), and inside the filling materials (internal voids) were measured.
Results
Total Fill BC sealer in the bulk-fill form presented significantly highest values of external and internal void percentages (p < 0.05). Biodentine showed a significantly lowest external void percentage (p < 0.05). WGP + Total Fill BC RCS presented significantly lower values of internal void percentages than all groups (p < 0.05), except Biodentine (p > 0.05).
Conclusion
None of the filling materials were created void-free obturation in resorption cavities. Biodentine may favor its application in teeth with IRR over Angelus MTA and bulk-fill form of Total Fill BC.
INTRODUCTION
Internal root resorption (IRR) is a form of root resorption which breaks down hard tissues of root canal walls as a result of a clastic activity. IRR is commonly caused by trauma or root canal infection [1]. In IRR cases, the pulp tissue apical to the resorptive defect has a viable blood supply, whereas the coronal pulp tissue above the resorptive defect must be infected to provide the stimulation for the clastic activity [1]. If this infected necrotic pulp tissue is not removed by root canal treatment, the pulp tissue apical to resorptive defect also undergoes necrosis, bacteria may infect the whole of the root canal system and consequently apical periodontitis may develop. Therefore, to prevent developing apical periodontitis, endodontic treatment is necessary to remove the infected pulp tissue, disinfect and obturate root canal system and resorptive defect. However, the irregularly concave nature of resorptive defects makes them inaccessible to clean and obturate properly. During the obturation of the resorptive defect, it can be expected from an obturation material to be able to flow and provide an adequate 3-dimensional (3D) obturation.
Gutta-percha is most popular and widely regarded as the gold standard filling core material. It becomes flowable with the application of heat. However, it has some disadvantages such as lack of adhesion to dentin, and when heated shrinkage happens upon cooling. It is used in conjunction with a root canal sealer (RCS). Total Fill BC sealer (FKG, La Chaux-de-Fonds, Switzerland) is a novel premixed and hydrophilic calcium silicate-based sealer. Total Fill BC RCS forms hydroxyapatite upon setting and chemically bonds to dentine [2]. Calcium silicate-based materials are recommended due to their higher bond strength, which is attributed to their small particle size and excellent level of viscosity [3]. Less than 2 µm of particle size enhances its flow into dentinal tubules, lateral canals, and leading to improved adaptation and gap-free seal [4]. Recently, calcium silicate-based RCSs have been used as root canal filling materials without the use of a core material (bulk-fill form) [567]. In previous studies, RCSs, more specifically calcium silicate-based RCSs in bulk-filled form had shown higher bond strength values than in conjunction with a core material [567].
In cases of extensive IRR, the prognosis of endodontic treatment can be compromised due to the weakening of the remaining dental structure. Considering the thin and weakened tooth structure in IRR cases, a calcium silicate-based material might be needed to reinforce the tooth to enhance the prognosis of the tooth. However, to the authors' knowledge, no study exists that compared the obturation quality of these materials with gutta-percha/sealer conjunction in teeth with simulated IRR. Therefore, this in vitro study was conducted to investigate whether calcium silicate-based sealer (Total Fill BC) and calcium silicate-based cements (CSCs; MTA [Angelus, Londrina, PR, Brazil] and Biodentine [Septodont, Saint-Maur-des-Fossés, France]) may have shown enhanced obturation quality in IRR cases due to their extremely small particle size and level of viscosity. In order to evaluate the obturation quality of these materials, the percentage of voids between dentine walls of resorptive cavity and filling materials (external voids) and inside the filling materials (internal voids) were measured by using micro-computed tomography (µCT). The null hypothesis was that there was no significant difference between filling materials.
MATERIALS AND METHODS
This study was approved by the ethics committee of the Zonguldak Bulent Ecevit University (protocol number 2017-88-20/09). Forty extracted maxillary central incisor teeth with similar in mesiodistal and buccolingual size were selected for this in vitro study. Crown lengths were shortened using a high-speed diamond bur under water cooling to obtain a standard tooth length of 20 mm. Working length was established 0.5 mm short of the apical foramen with a size 10 K-file, and root canals were instrumented with ProTaper Next rotary instruments (Dentsply-Maillefer, Ballaigues, Switzerland) to a master apical size of X5. The root canals were copiously irrigated using 3 mL 2.5% sodium hypochlorite (NaOCl) during instrumentation. After the preparation was completed, each specimen was placed in Eppendorf tubes that filled with additional polyvinyl silicone impression material (Hydrorise Light, Zhermack, Badia Polesine, Italy) to create an individual mold and to mimic an alveolar socket for each specimen [8]. After polymerization of impression material, the roots were taken out. Teeth were split along their long axis in a buccolingual direction. The lengths of the halves were measured by a digital caliper (Liaoning MEC Group, Dalian, China), and the localizations of the resorptive cavity were determined with ensuring that cavities were simulated at the same site in both root segments. Internal semi-circular cavities were located 6 mm from the apex and were created with a size 8 round bur leaving a diameter of 2.3 mm on each half of the roots (Figure 1A). Then, root halves were reattached using a luting agent (Jota AG, Rüthi, Switzerland). Final irrigation was applied with 5 mL 2.5% NaOCI and 17% ethylenediaminetetraacetic acid (EDTA) Then root canals were rinsed with 5 mL distilled water and dried with paper points and put into their respective sockets in Eppendorf tubes (Figure 1B).
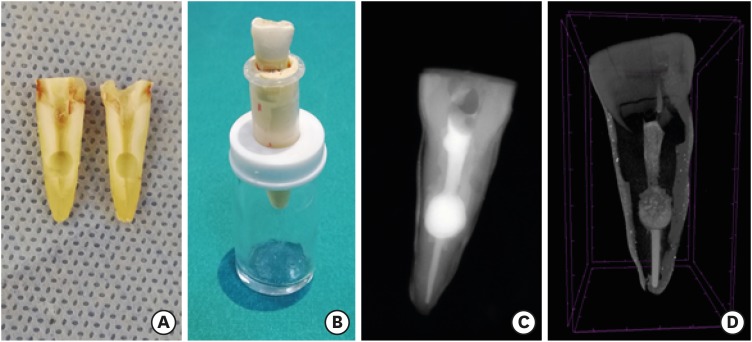
Experimental design. (A) Semi-circular cavities were created on each half of the roots; (B) Individual molds in Eppendorf tubes; (C) Periapical radiography; (D) Micro-computed tomography (µCT) images for obturation of resorption cavity.
Obturation of resorptive cavities
The apical part of 40 root canals (below resorptive cavity) were filled with Total Fill BC sealer (FKG) and X5 gutta-percha cones using single cone technique with taking care to avoid sealer extrusion into the resorptive cavity. The gutta-percha was partially removed with a heated plugger, leaving 6 mm of apical filling. Resorptive cavities were checked and cleaned. Then, specimens were randomly divided into 4 groups (n = 10) according to filling materials used as follows:
• Group Angelus MTA (White MTA, Angelus, Londrina, PR, Brazil): The powder of MTA was mixed with sterile water in a 3:1 powder/liquid ratio. Then, the cement was incrementally placed into the resorptive cavity and remained root canal (coronal to resorptive cavity) with MTA carrier (Medesy, Maniago, Italy) and was condensed by using a Buchanan hand plugger (SybronEndo Corp., Orange, CA, USA) (Figure 1C).
• Group Biodentine (Septodont, Saint-Maur-des-Fossés, France): According to the manufacturer's instructions, 5 drops of the liquid were poured into the powder-containing capsule. The capsule was triturated for 30 seconds on an amalgamator. Then, the cement was incrementally placed into the resorptive cavity and remained root canal as described previously.
• Group Total Fill BC (bulk-fill form): RCS, without a core material, was injected directly into the resorptive cavity and remained root canal.
• Group warm gutta-percha (WGP) +Total Fill BC sealer: A small amount of RCS was injected into resorptive cavity. Then, WGP was injected to resorptive cavity by using the DiaGun Obturation System (DiaDent, Burnaby, BC, Canada) with 25-G delivery needles. The endodontic heat gun was set to 200°C and each time 2- to 3-mm WGP segments were injected and vertically condensed with a hand plugger.
After obturation was completed the samples were wrapped in wet gauze, and allowed to set for 1 week to allow complete setting of filling materials. To evaluate the obturation quality, the volume of voids within the obturation materials (internal) and at their interface with dentin walls (external) were measured for each specimen by using µCT (Figure 1D).
µCT analyses
The samples were scanned with µCT imaging (SkyScan 1172, Bruker microCT, Kontich, Belgium). The scanning conditions were 100 kV, 100 µA, and a pixel size of 13.74 µm. Scanning was performed by 360° rotation around vertical axis, a camera exposure time of 1,500 ms. Nrecon v.1.6.5.2 (SkyScan, Brucker-microCT) and CTAn v.1.14.4.1 (Skyscan, Bruker microCT) softwares were used to reconstructing, and volumetric analyzing, respectively. Reconstructed images were transferred to CTAn v.1.14.4.1 software to make 3D quantitative measurements of the samples as described in a previous report [9]. After determining the region of interest, the original grayscale images were processed to calculate of the voids in the resorptive cavity. An automatic segmentation threshold was used to subtract dentin from filling materials and voids (Figure 2A-2C). All images were examined by a single evaluator who was blinded to data regarding the groups. The volume of the filling materials and the voids was calculated (in mm3) with CTVox software (version 3.2.0, Bruker microCT). Then, the ratio of these 2 measurements was calculated as the percentage of voids (in %) (Table 1).
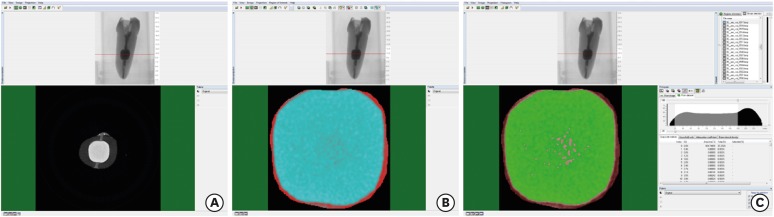
Micro-computed tomography (µCT) analysis stages. (A) Measurement of percentage voids on CTAn software (Bruker microCT); (B). Selection of the region of interest; (C) Threshold selection from gray-level histogram.

Median and range percentage values of experimental groups (%)
Statistical analyses
Statistical analysis was performed using SPSS version 22 (IBM Corp, Armonk, NY, USA). Shapiro Wilk test was used to check the normality of data. Differences among groups were compared using Kruskal-Wallis test. Mann Whitney U test was used for intragroup comparison. The threshold for statistical significance was set at p < 0.05.
RESULTS
Significant differences were found among groups in terms of external and internal void percentages (p < 0.05). Mean values of external void highest to lowest were found as follows: Total Fill BC (bulk-fill form) > WGP + Total Fill BC > MTA > Biodentine. The significantly highest value for external void percentage was found in Total Fill BC (bulk-fill form) (p < 0.05), whereas the lowest was found in Biodentine (p < 0.05).
Mean values of internal void highest to lowest were found as follows: Total Fill BC (bulk-fill form) > MTA > Biodentine > WGP + Total Fill BC. The significantly highest value for internal void percentage was found in Total Fill BC (bulk-fill form) (p < 0.05). WGP + Total Fill BC sealer presented significantly lower values of internal void percentages than all groups, except Biodentine (p < 0.05).
DISCUSSION
Teeth with extensive IRR may become more brittle due to the loss of dental structure. Therefore, materials that were suggested to have reinforcing capacity should be preferred for filling these teeth to prevent fractures [10]. CSCs such as MTA or Biodentine may be considered the material of choice to repair the extensive resorption defects. In addition to that, the selected material can also prevent the spread of a bacterial infection with the lower values of gap size between cement and dentin interface with adequate sealing. However, due to the nature of irregular concave cavity of IRR, the obturation quality of CSCs is unknown. Therefore, this in vitro study was conducted to evaluate the obturation quality of MTA, Biodentine, and Total Fill BC sealer (bulk fill form) in teeth with simulated IRR. Voids along the dentin walls of the resorptive cavity and inside the tested materials were evaluated by using µCT.
In the present study, IRR cavities were simulated on each root halves by using round burs to obtain standardization. This technique may not replicate a real irregular resorptive cavity. However, standardizing the cavity dimensions make it possible to compare. MTA and Biodentine were placed into resorption cavities with hand condensation. In a previous µCT study, El-Ma'aita et al. [11] observed fewer voids with hand condensation of MTA root filling than with indirect ultrasonic activation. Sisli and Ozbas [12] and Küçükkaya Eren et al. [13] reported that placement techniques did not affect the obturation quality of CSCs. Based on these results of previous report findings, the supplementary placement technique did not use in the present study.
The present study results revealed that there was a statistically significant difference in the quality of the root canal fillings in terms of their ability to fill a resorption cavity. Total Fill BC sealer in the bulk-fill form (without a core) showed significantly higher external and internal void percentages among experimental groups. Total Fill BC sealer is a premixed, hydrophilic single syringe that contains calcium silicate with small particle size and excellent level of viscosity, which could minimize the risk of void formation in the RCSs [9]. In previous reports, Nagas et al. [7] and Huffman et al. [5] reported that calcium silicate-based sealers in bulk fill form showed higher resistance to dislocation than used with a core material. Considering these advantages, in the present study Total Fill BC sealer in bulk-fill form was preferred due to its flowability and expected to fill the simulated resorptive cavity via direct injection. However, bulk-fill form showed the worst results for both percentages of external and internal voids. This apparent problem was probably caused by difficulty in any lack of condensing after injecting sealer into the resorption cavity and entrapment of air voids during taking out the syringe in some of the specimens might have been affected the measured results.
According to the results of the present study, Biodentine showed a lower external and internal void percentage than MTA. The external void percentage value for Biodentine was found 0.80% in the present study. This result was similar to a recent study in which a percentage of 0.86% was found for Biodentine when it was tested as an intracoronal barrier [14]. Biodentine has some features which are superior to MTA; such as its handling characteristics and consistency [15]. In a previous study, it was reported that the size of the particle of Angelus MTA was inhomogeneous, and it was surface looks more irregular than Biodentine [16]. In that study, the differences in the chemical composition of calcium silicate cements were reported to affect their clinical performances. Angelus MTA particles vary in size and have low circularity [17]. Therefore, due to these aforementioned reasons, Angelus MTA might have been shown more external and internal voids than Biodentine. This result is consistent with a previous study which revealed that Biodentine showed the lowest volume of the gap between the material and the root canal dentin compared to MTA [18]. On the contrary, a µCT study [13] reported that no difference in obturation quality exists between MM-MTA (Micro-Mega, Besançon, France) and Biodentine. These controversial results may have been related to the differences in the study designs and the type of materials used.
Filling artificial resorptive cavities with vertical condensation of WGP was found significantly better in previous reports [1920]. However, to authors' knowledge until now, no study is available that compared the obturation quality of WGP techniques with CSCs. According to the results of the present study, external void percentages for WGP were significantly higher than MTA and Biodentine. However, its internal void percentage value was lower than those of 2 CSCs. It is known that the thermoplasticized gutta-percha shrinks upon cooling [21]. Therefore, the shrinkage might be the reason for more external voids compared to MTA and Biodentine.
In the present study, the obturation quality was evaluated by measuring external and internal void percentages, separately. The incidence of these voids of root canal fillings can be influenced by several factors, such as the clinician's experience, the selected obturation technique, and the physical properties of the selected materials [22]. The presence of external voids along the dentine walls is an indicator for the assessment of the marginal adaptation of root canal fillings. It has a significant relationship with the outcome of root canal treatment [23]. However, the amount of voids within root canal fillings (internal void) to cause failure in treatment is unclear. Bogen and Kuttler [24] reported that the voids in a calcium silicate-based obturation material do not seem to affect biologic mechanisms necessary for favorable healing. However, it is important to keep in mind that the purpose of the obturation procedures of endodontic treatment is to provide a 3D obturation (without any void) of the whole root canal system to prevent microleakage and reinfection [25]. Further investigations are required in order to evaluate the effect of voids inside the root canal fillings in resorptive cavities obturated with different CSCs on the clinical success of root canal treatment.
CONCLUSIONS
In the present study, none of the filling materials showed void-free obturation. However, a lower void percentage in the Biodentine, both at the dentin/cement interface and inside the material, may favor its application in IRR over Angelus MTA, bulk-fill form of Total Fill BC.
Notes
Funding: This study was supported by the funds of Zonguldak Bülent Ecevit University (grant number: 2017-27194235-01)
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Aktemur Türker S.
Data curation: Tek V.
Formal analysis: Tek V.
Investigation: Aktemur Türker S.
Methodology: Aktemur Türker S.
Supervision: Aktemur Türker S.
Writing - original draft: Tek V, Aktemur Türker S.
Writing - review & editing: Aktemur Türker S.
