A cone-beam computed tomography study of the prevalence and location of the second mesiobuccal root canal in maxillary molars
Article information

Abstract
Objectives
This study aimed to investigate the incidence and location of the second mesiobuccal root (MB2) canal in maxillary molars with the aid of various measuring points and lines using cone-beam computed tomography (CT).
Materials and Methods
A total of 205 images of patients who underwent cone-beam CT examinations between 2011 and 2015 as part of their dental diagnosis and treatment were included. There were 76 images of the maxillary first molar and 135 images of the maxillary second molar. Canal orifices were detected at −1 mm from the top of the pulpal floor on cone-beam CT images. Image assessment was performed by 2 observers in reformatted image planes using software. Assessments included measurement of the distance between the MB1 and MB2 canals, and the angles between the lines connecting the MB1-MB2 and distobuccal (DB)-palatal (P) canals. The data were analyzed using the student's t-test.
Results
The prevalence of the MB2 canal was 86.8% in the first molar and 28.9% in the second molar. The angle between the lines connecting the MB1-MB2 and DB-P canals was 2.3° ± 5.7° in the first molar and −3.95° ± 7.73° in the second molar. The distance between the MB1 and MB2 canals was 2.1 ± 0.44 mm in the first molar and 1.98 ± 0.42 mm in the second molar.
Conclusions
The angles between the lines connecting the MB1-MB2 and DB-P canals was almost parallel. These findings may aid in the prediction of the location of the MB2 canal orifice.
INTRODUCTION
To achieve successful long-term endodontic treatment, the entire treatment process, beginning with appropriate access cavity preparation to shaping and cleaning in order to maximally remove organic tissues while maintaining the original anatomical shape and appropriate restoration to 3-dimensionally enclose the root canal and prevent microleakage, must be performed without error. Understanding the root canal system, particularly the complexity and structure of multirooted teeth, is the basis of endodontic treatment [1]. Maxillary molars feature a complex root canal morphology, and the second mesiobuccal root (MB2) canal is an important factor contributing to the failure of endodontic treatment [234]. Therefore, identification of the MB2 canal and its location is crucial for successful endodontic treatment of the maxillary molars.
Cone-beam computed tomography (CT) enables examination of the root canal morphology in vivo and offers relatively accurate 3-dimensional information to differentiate root canal morphology [567]. Although many studies have investigated the incidence of the MB2 canal in maxillary molars, studies on the location of the MB2 canal are still lacking. Some studies measured the distance between the MB1 and MB2 canals in order to predict the location of the MB2 canal, but none measured the angles between the canals for this purpose.
Thus, we aimed to examine the incidence of MB2 canals in the maxillary molars and measure the distances and angles between the canals by reconstructuring and analyzing cone-beam CT images of Korean patients, in an attempt to propose a simple method for locating MB2 canal orifices.
MATERIALS AND METHODS
Patients who underwent cone-beam CT (D-mode, voxel size 0.1 mm) of the maxillary molars due to a dental implant, facial trauma, impacted tooth, or periodontal disease at the Gangneung-Wonju National University Dental Hospital between January 2011 and May 2015 were enrolled. This study was approved by the institutional review board (IRB) at Gangneung-Wonju University Dental Hospital (IRB 2017-008), and the patients provided informed consent before inclusion into the study. For a more accurate reading, teeth that underwent wide-ranging restorative treatment or endodontic treatment, teeth with defects, and teeth with incomplete root formation or incomplete eruption were excluded, resulting in a total of 205 images for analysis [89]. The 205 images consisted of 76 images of the maxillary first molar and 135 images of the maxillary second molar. There were 125 men, and 80 women, with a mean age of 44.9 years (range, 18–74 years).
Alphard Vega (Asahi Roentgen Ind., Kyoto, Japan) cone-beam CT equipment was used and the images were restructured in 3 planes (axial, coronal, and sagittal) in 3-dimensional images and aligned such that the long axis of the tooth was perpendicular to the plane with reference to the cementoenamel junction (CEJ) using the Xelis Dental Program (Infinitt, Seoul, Korea). The incidence of MB2 canals was investigated using the images, and when the MB2 canal was present, 1 mm inferior to the pulpal floor to the root apex (−1 mm), it was set as the reference plane to perform various measurements and analyses using the MB1 canal, MB2 canal, distobuccal (DB) canal, and palatal (P) canal. Images were evaluated by 2 endodontists, and the mean values of the measurements were used for analysis. Separate analyses were performed for the maxillary first and second molars.
Incidence of MB2 canals in the maxillary molars
The incidence of MB2 canal orifices was investigated by navigating the restructured image (based on the CEJ) from the pulpal floor plane to the root apex.
Locations of the MB2 canal orifices in the maxillary molars
1. Angles of the lines connecting the MB1 and MB2 canals and those connecting the DB and P canals
The angles of the lines connecting the MB1 and MB2 canals and those connecting the DB and P canals were defined α and measured (Figure 1). The angle was defined as positive when the MB2 canal was more mesial than the hypothetical line parallel to the line connecting the DB and P canals passing through MB1, and negative when the MB2 canal was more distal than the hypothetical line.
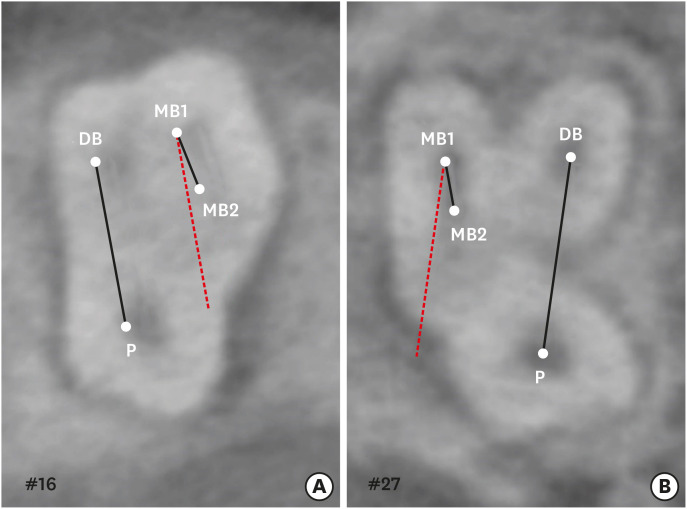
Measurement of the angle between the line connecting the MB1-MB2 and that connecting the DB-P canals in a maxillary molar. (A) Positive angle; (B) Negative angle.
MB1, first mesiobuccal root; MB2, second mesiobuccal root; DB, distobuccal; P, palatal.
2. Distance between the MB1 and MB2 canal orifices
The distance (mm) between the MB1 and MB2 canal orifices was measured, the average distance was calculated for maxillary first molars and second molars, respectively.
3. Distribution of MB2 canal locations
To analyze the distribution of the MB2 canal orifice, an individual graph was drawn for every tooth by using the ‘α’ value and the distance between the MB1 and MB2 canals (Figure 2). The y-axis was defined as a hypothetical line passing MB1, which was parallel to the line connecting DB and P canals. The x-axis was drawn perpendicular to the y-axis, while the y-value is set to be the average distance between the MB1 and MB2 canals corresponding to tooth type (either maxillary first molar or maxillary second molar). If the orifice of the MB2 canal of a certain tooth is located on the y-axis, i.e., the ‘α’ is 0, the x-value is 0. And the coordinate value (0, 0) means that the line connecting DB, P orifices and the line connecting MB1, MB2-orifices are parallel (α = 0), and the distance between MB1 and MB2 orifices is equal to the average distance. For every tooth, the x- and y-coordinates were determined using the following equation and plotted for the maxillary first molars and second molars, respectively.
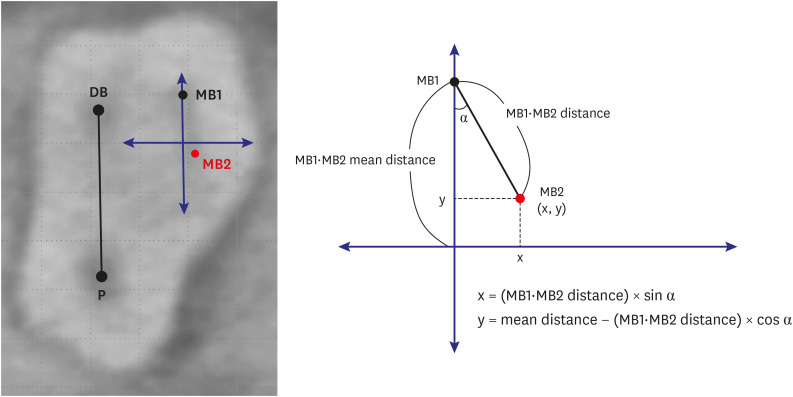
Measurement of the mean distance between the MB1 and MB2 canals in a maxillary molar. The hypothetical line that passes through the MB1 and is parallel to the line connecting the DB and P canals (mm) is the y-axis. The maximum value of the y-axis and the 0 point are assumed to be the mean distance between the MB1 and MB2 canals.
MB1, first mesiobuccal root; MB2, second mesiobuccal root; DB, distobuccal; P, palatal.
Statistical analysis
The means and standard deviations of the measured angles and distances were computed. The measurements for the maxillary first molars and second molars were compared using the student's t-test at 95% statistical significance using the SPSS software (version 23.0, IBM Crop., Armonk, NY, USA) software.
RESULTS
Incidence of MB2 canals in the maxillary molars
The incidence of MB2 canals was 86.8% (66/76) in the maxillary first molars and 28.9% (39/135) in the maxillary second molars.
Locations of MB2 canal orifices in the maxillary molars
1. Angles between the lines connecting the MB1 and MB2 canals and those connecting the DB and P canals
The angles between the lines connecting the MB1 and MB2 canals and those connecting the DB and P canals were 2.30° ± 5.70° in the first molar and −3.95° ± 7.73° in the second molar (Table 1), with a significant difference between the 2 groups (p < 0.05). The angles between the lines were within ± 15°, and with reference to the hypothetical line parallel to the line connecting the DB and P canals and passing through MB1, MB2 canals were predominantly mesial in the first molars and distal in the second molars.

Angles between the line connecting the MB1 and MB2 canals and the line connecting the DB and P canals, as well as the distances between the MB1 and MB2 canals, in the first and second maxillary molars
2. Distances between the MB1 and MB2 canal orifices
The distances between the MB1 and MB2 canal orifices were 2.10 ± 0.44 mm in the first molars and 1.98 ± 0.42 mm in the second molars, with no significant differences between the 2 groups (Table 1) (p > 0.05).
3. Distribution of the MB2 canal locations
The MB2 canal locations were plotted based on the angles between the lines connecting the DB and P canals and those connecting the MB1 and MB2 canals as well as the distances between the MB1 and MB2 canals. The percentage of cases in which the MB2 canal was located within a circle with a radius of 0.5 mm was 68.2% (45/66) in the first molars and 69.2% (27/39) in the second molars (Figure 3).
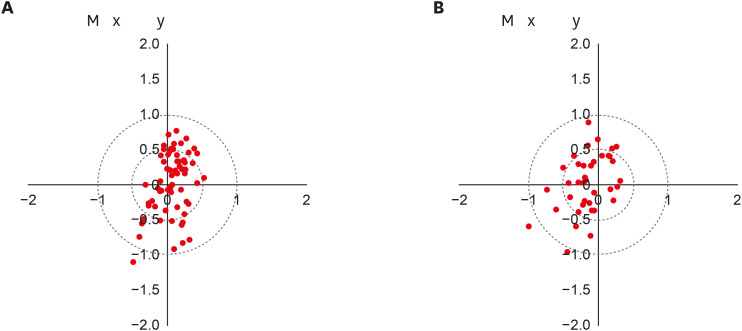
Distribution of the second mesiobuccal root canal in the maxillary first and second molars. (A) Maxillary first molar; (B) Maxillary second molar.
DISCUSSION
This study was based on the idea that the line connecting MB1 and MB2 and the line connecting DB and P appear parallel, according to the clinical experience of Dr. Sung-Ho La (personal communication). If the above assumption can be proven, it will be easier to predict the location of MB2. Therefore, this study examined the incidence of MB2 canal orifices in maxillary molars and attempted to predict MB2 locations based on various measurements in Korean patients by analyzing cone-beam CT images acquired for various purposes.
Some studies investigating the incidence of MB2 canals in the maxillary molars have utilized periapical radiographs or extracted teeth for microscopic analysis. However, periapical radiographs have reduced accuracy due to image distortions or superimposition of anatomical structures, and it is difficult to collect good samples with extracted teeth because teeth are commonly fractured due to curved roots [10]. Cone-beam CT enables a more precise analysis of the various shapes of the root canal system while addressing these limitations [11]. This study was particularly useful in that it identified the presence of MB2 canals in maxillary molars using existing images and more accurate measurements were made based on various points and lines.
In this study, we reconstructed the images such that the plane passing the CEJ was perpendicular to the long axis of the tooth and set the plane 1 mm inferior to the horizontal plane passing the pulpal floor as the reference plane for observation. Using the CEJ as the reference for image restructuring is beneficial in that, this allows easy recognition and high reproducibility, and information can be more readily obtained from the pulpal floor considering that this is the location at which a clinician recognizes the root canal orifice after access cavity preparation [1213].
Our results indicated that MB2 canals were present in 86.8% of 76 maxillary first molars and in 28.9% of 135 maxillary second molars. In maxillary first molars, Degerness et al. [14] reported an incidence of 79.8% and another study reported an incidence of 73.8% [15]. The previous studies also included Korean patients. Lee et al. [16] reported a 76.5% incidence of MB2 canals in the maxillary first molars, and the current study showed a similar incidence. The incidence is lower in the maxillary second molars, ranging from 20% to 51.1% [17]. In another study on Korean patients, a 42.2% incidence in the maxillary second molars was reported [18]. The results of this study on maxillary second molars are also within the above-mentioned approximate range. The differences in the incidences found in the current and previous studies may be attributed to differences in race, sample size, voxel size, experimental methods, MB2 definition, and reference plane settings [19].
The large gap in the incidence of MB2 canals between the first molars and second molars in this study seems to be intimately related to tooth morphology. Kim et al. [20] reported that 97.91% of maxillary first molars were classified as 3-rooted, while only 74.9% of maxillary second molars were 3-rooted. The percentage of mesiobuccal roots classified as Vertucci type 1, that is, 1 root canal per root, was greater among maxillary second molars than among maxillary first molars. In a study in a Chinese population, second molars were reported with a more diverse morphology than first molars [21]. Therefore, the lower incidence of MB2 canals among maxillary second molars than first molars seems to be attributable to these morphological differences.
In a study on the distances between the MB1 and MB2 canals, Kulild et al. [22] reported a distance of 1.82 mm. In another study, the distance was reported to be 2.68 mm in the maxillary first molars and 2.41–2.2 mm in the maxillary second molars [23]. In a study in Korean patients, Lee et al. [16] observed a distance of 1.91 mm in the maxillary molars.
With reference to the hypothetical line parallel to the line connecting the DB and P canals and passing through MB1, the MB2 canal was present within ± 15° of the P side of the MB1, mesially in the first molars and distally in the second molars. This may be due to the fact that the crowns of maxillary first molars are generally square-shaped, but those of second molars taper towards the P side, and the location of the MB2 canal may vary according to the shape of the occlusal plane. However, Tuncer et al. [24] reported that the MB2 canal is generally located distally from the MB1, but this seems to be attributable to an error in the analysis of results.
In this study, the sample size was limited because only patients with D-mode cone-beam CT with a relatively high resolution were examined, and thus additional studies are needed to more objectively substantiate the results of this study. Furthermore, although D-mode, which has a relatively high resolution, was used, errors may have occurred when measurements were taken with reference to the midpoint of the root canal; we had 2 researchers take these measurements to minimize this error. Moreover, in this study, the number of samples of the maxillary first molar was smaller than that of maxillary second molar owing to more CBCT for cases of implants with the extraction of the maxillary first molar. As a limitation of this study, only Korean patients were investigated, so further extensive research is needed to include findings from individuals of various ethnic backgrounds.
When performing endodontic treatment on maxillary molars, clinicians need to accurately recognize MB2 canals and possess an understanding of tooth morphology. The finding that the line connecting the MB1 and MB2 canals and that connecting the DB and P canals are nearly parallel, and that the MB2 canal is located within 2 mm of the MB1 would serve as a more accurate standard for predicting the location of the MB2 canals and would have practical applications to access cavity preparation.
CONCLUSIONS
Based on the findings of the present study, the angles between the lines connecting the MB1-MB2 and DB-P canals were almost parallel. These findings may aid in the prediction of the location of the MB2 canal orifice.
ACKNOWLEDGEMENTS
We express our sincere gratitude to Dr. Sung-Ho La, who provided the inspiration for the idea of finding the second mesiobuccal root (MB2) canal.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Kim JW.
Data curation: Lee SJ.
Formal analysis: Kim JW, Cho KM, Park SH.
Funding acquisition: Kim JW.
Investigation: Lee SJ.
Methodology: Kim JW.
Project administration: Park SH.
Resources: Lee SJ.
Software: Lee SJ, Lee EH.
Supervision: Kim JW.
Validation: Park SH.
Visualization: Lee SJ.
Writing - original draft: Lee SJ.
Writing - review & editing: Kim JW, Cho KM, Park SH.
