Effects of the endodontic access cavity on apical debris extrusion during root canal preparation using different single-file systems
Article information

Abstract
Objectives
This study was conducted to evaluate the effects of traditional and contracted endodontic cavity (TEC and CEC) preparation with the use of Reciproc Blue (RPC B) and One Curve (OC) single-file systems on the amount of apical debris extrusion in mandibular first molar root canals.
Materials and Methods
Eighty extracted mandibular first molar teeth were randomly assigned to 4 groups (n = 20) according to the endodontic access cavity shape and the single file system used for root canal preparation (reciprocating motion with the RCP B and rotary motion with the OC): TEC-RPC B, TEC-OC, CEC-RPC B, and CEC-OC. The apically extruded debris during preparation was collected in Eppendorf tubes. The amount of extruded debris was quantified by subtracting the weight of the empty tubes from the weight of the Eppendorf tubes containing the debris. Data were analyzed using 1-way analysis of variance with the Tukey post hoc test. The level of significance was set at p < 0.05.
Results
The CEC-RPC B group showed more apical debris extrusion than the TEC-OC and CEC-OC groups (p < 0.05). There were no statistically significant differences in the amount of apical debris extrusion among the TEC-OC, CEC-OC, and TEC-RPC B groups.
Conclusions
RPC B caused more apical debris extrusion in the CEC groups than did the OC single-file system. Therefore, it is suggested that the RPC B file should be used carefully in teeth with a CEC.
INTRODUCTION
Even when the working length is controlled during root canal preparation, the undesirable extrusion of dentin chips, pulpal residue, microorganisms, and irrigation solution into the periradicular tissue may occur. This extruded debris may cause inflammation, postoperative pain, flare-ups, and delayed periapical recovery [12]. The incidence of such complications has been reported to be between 1.4% and 16% in the literature [2]. All instrumentation techniques and file systems seem to force intracanal debris into the periapical tissues [34]. Most root canal instrumentation techniques involve nickel-titanium (NiTi) instruments because of their flexibility.
A straight access path with coronal flaring facilitates the early access of irrigants and allows rotary instruments to prepare the apical portion with less wall contact [5]. Therefore, increasing the coronal space for debris and creating a straight access path may reduce the amount of apically extruded debris. Access cavity preparation is one of the most important steps of root canal treatment [6]. In a traditional endodontic cavity (TEC) procedure, the aim is to have the pulpal chamber and pulpal horns in the access cavity to increase the efficiency of preparation, to establish a straight access path to the root canals, and to ensure effective preparation of coronal sections of root canals [578]. In a contracted endodontic cavity (CEC) procedure; however, the aim is to maintain the mechanical stability of the tooth. The latter was introduced as an alternative to the TEC procedure [910]. The CEC technique results in less dentin loss by protecting the pericervical dentin and by limiting the size of the cavity. Thus, this type of cavity positively contributes to the mechanical stability of the tooth [89].
In recent years, a number of NiTi single-file systems with different designs, alloy characteristics, heat treatments, and kinematics were developed for root canal preparation. The Reciproc Blue (RPC B; VDW, Munich, Germany) single-file system is an updated version of the Reciproc (RPC; VDW) single-file system. The RPC B has an S-shaped horizontal cross-section and 2 cutting edges, similar to the design properties of the RPC, and is used with a reciprocating motion. It is manufactured using a new heat treatment technology named the “blue treatment,” which was developed in order to increase the flexibility of the file's structure [1112]. Another single-file system, One Curve (OC; MicroMega, Besançon, France), was recently introduced to the market. OC files are made using C-wire heat-treated NiTi material and are used with a continuous rotary motion. The OC instruments have a variable cross-section along the blade for better centering ability and cutting efficiency.
Previous studies reported that all root canal preparation methods and file systems caused different levels of debris extrusion from the apical foramen [413]. These differences were attributed to variations in the file design (radial area, flute depth, taper, and cross-section), kinematics, and operational principles [13].
No study has yet investigated the effect of the shape of the access cavity on the amount of apical extrusion during canal shaping procedures. Thus, the present study aimed to evaluate the effects of the TEC and CEC preparation methods with the use of RPC B and OC single-file systems on the amount of apical extrusion in mandibular first molar root canals.
MATERIALS AND METHODS
Approval for this study was obtained from the Ethical Committee of Hatay Mustafa Kemal University, Hatay, Turkey (2018/181). Based on a similar study carried out previously [14], the sample size was calculated using G*Power 3.1 software (Heinrich Heine University, Dusseldorf, Germany), assuming α to be 0.05 and power to be 80%. The calculated sample size was 20 for each group.
Sample selection
In total, 80 mature and intact mandibular first molar teeth extracted for periodontal reasons and having no caries were used. The teeth were all stored in physiological saline solution until use. All the teeth were checked using a stereomicroscope (Olympus BX43; Olympus Co., Tokyo, Japan) under ×20 magnification to determine whether there were any root fractures, cracks, or fusion in the mesial and distal roots. Periapical radiographs of each tooth were taken from the mesiodistal and buccolingual angles, digitized, and stored. The root canal curvature was determined based on the angle of curvature starting at the coronal aspect of the apical third of the root using Schneider's method (Figure 1) [1516]. Only roots with an angle of curvature ranging between 10° and 20° were selected. Teeth with 2 canals in the mesial root and a single canal in the distal root and with similar mesiodistal and buccolingual dimensions of the pulp chamber were selected for inclusion in the study. Teeth with a root canal treatment history, internal or external root resorption, or pulpal calcification were excluded. The crown-to-apical length of the teeth was measured using a digital caliper (Digimess, São Paulo, Brazil), and teeth with similar length (20 ± 1 mm) were chosen in order to ensure standardization. All residual soft and hard tissue on the teeth were mechanically removed.
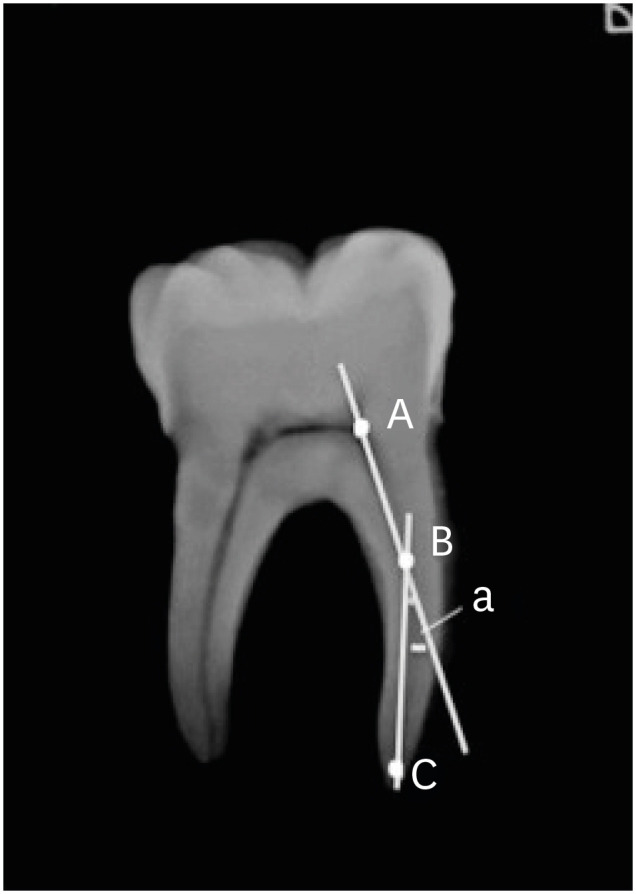
Diagrammatic representation of Schneider's method.
Groups and access cavity preparation
A single endodontist performed all the endodontic procedures in all groups. The teeth were randomly divided into the following 4 groups, with 20 teeth in each group: TEC-OC, CEC-OC, TEC-RPC B, and CEC-RPC B.
The access cavity was opened using an diamond bur with water cooling at high speed. The access cavities in the TEC group were prepared as described in previous studies [517] (Figure 2A). The access cavities of the teeth in the CEC group were opened at the mesial quarter of the central fossa by partially retaining and enlarging the roof of the pulp chamber in the apical and distal directions. In the CEC groups, a very small portion of dentin was removed from the mesiodistal, buccolingual, and circumferential pericervical areas, and part of the pulp chambers' roof was retained [7818]. The locations of the root canal orifices could be seen. In all cavities, the enamel was beveled using angle diameter burs (Figure 2B).
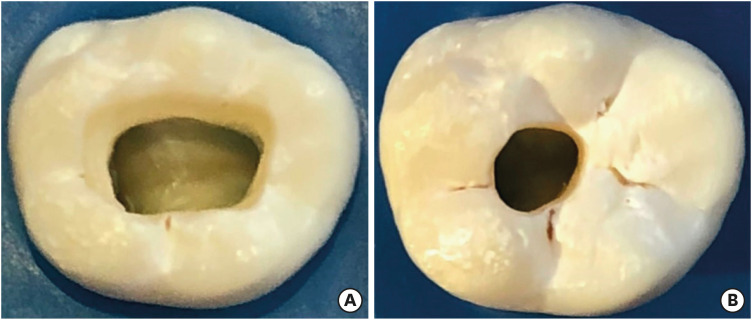
Photographs of mandibular first molars showing access outlines. (A) TEC. (B) CEC.
TEC, traditional endodontic cavity; CEC, contracted endodontic cavity.
After opening the access cavity, the apical patency of the root canal was checked using a size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). Teeth with a root canal greater than size 15 were discarded. The size 10 K-file was pushed forward until it could be seen from the major apical foramen, and the working length was determined to be 1 mm shorter than this length.
Assessment of apical debris
The method described by Bürklein et al. [19] was used to assess apical debris extrusion in all groups (Figure 3). The teeth were placed in a rubber stopper and fixed with cyanoacrylate cement. Eppendorf tubes, in which the teeth were placed at the cementoenamel junction point, were placed in a glass bottle. Prior to placing each tooth in the tube, the weight of each tube was measured 3 times using an electronic scale (Pioneer, Ohaus Corp., Parsippany, NJ, USA) with 10−4 g sensitivity, and the average value of these measurements was calculated. A 25-gauge syringe was added to the rubber stopper in the bottle to equalize the internal and external air pressures.
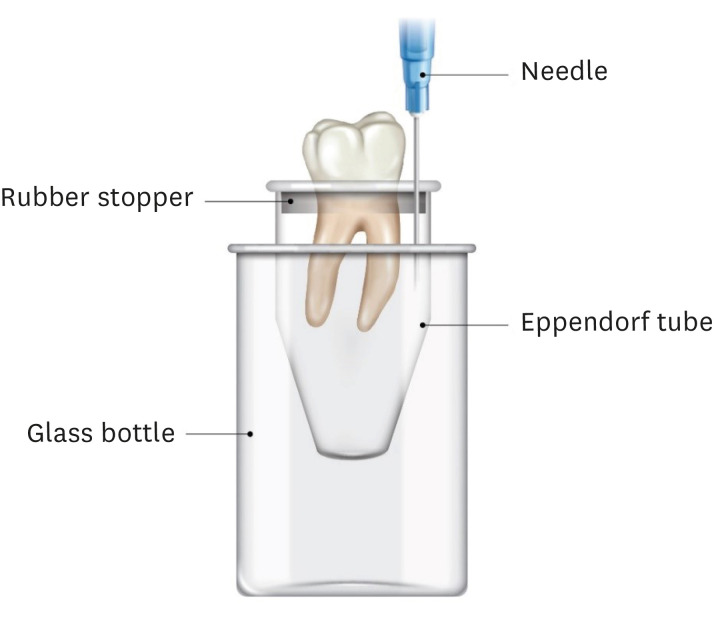
A schematic presentation of the test model.
In order to prevent the operator from viewing the debris extrusion during the preparation, the Eppendorf tubes were wrapped with aluminum foil. The debris that was extruded from the apex while shaping the root canal was collected in the Eppendorf tubes.
Root canal preparation
The root canal preparation procedures of the teeth in the TEC-OC and CEC-OC groups were performed using an OC file (size 25/0.06) and an endodontic motor (X-Smart Plus; Dentsply Maillefer) with a continuous rotation motion at 300 rpm and 2.5 N·cm of torque.
The canals in the TEC-RPC B and CEC-RPC B groups were prepared using an RPC B R25 (size 25/0.08) file in the Reciproc All mode with a Silver Reciproc endodontic motor (VDW).
In root canal preparation, all files were used with an in-and-out pecking motion at a 3-mm amplitude limit, with slow and light movements. The files were removed from the canal and checked after every 3 pecking motions. The grooves of the file were cleaned, and the preparation was continued until the working length in the root canal was reached.
The canals of the teeth in all the groups were irrigated using a total of 20 mL of distilled water by a side-vented needle (#27 gauge) during root canal preparation. Each file was used to prepare the root canals of only 1 tooth.
Evaluation of apically extruded debris
After completing the root canal preparation, the Eppendorf tubes were removed from the glass bottle. Before taking the teeth out of the tubes, the roots of the teeth were washed inside the Eppendorf tube with 1 mL of distilled water in order to collect the debris residue on the outer surface of the apex. Before weighing the extruded debris, the tubes were kept in an incubator at 70°C for 5 days in order to vaporize the distilled water in the tube [13].
Each of the tubes was weighed 3 times consecutively using an electronic scale, and the average values were recorded. The amount of extruded debris was calculated by subtracting the empty weight of the tube from the value measured after root canal preparation. A second independent operator measured the apical debris extrusion and the 2 sets of measurements were compared.
Statistical analysis
The statistical analyses were performed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). After statistically analyzing the amount of debris extruded from the apical foramen using 1-way analysis of variance, Tukey's post hoc test for multiple comparisons was performed. The level of significance was set at p < 0.05.
RESULTS
The minimum, maximum, and mean values with standard deviations of apical debris extrusion are presented in Table 1. No statistically significant difference was found in the amount of apical debris extrusion among the TEC-OC, CEC-OC, and TEC-RPC B groups. However, there was a statistically significant difference between the CEC-RPC B group and the TEC-OC groups and CEC-OC groups (p < 0.05).

The median, minimum, and maximum values of apically extruded debris in grams
DISCUSSION
The debris extruded from the apical foramen during the root canal preparation may initiate an inflammatory reaction in the periapical region. As a result, postoperative pain and swelling may occur, both of which may have negative effects on the prognosis of root canal treatment [20]. In a previous study, the authors reported an association between the severity of inflammatory reactions during root canal preparation and the amount of apical debris extrusion, with more severe reactions occurring in the presence of greater amounts of debris extrusion [21].
Various factors affect the amount of apical extrusion, including the apical size, curvature length, and degree of the root canal of a prepared tooth, in addition to the tip size, taper, movement kinematics, design of the file used in root canal preparation, irrigation solution, and amount of irrigation solution [22]. A correctly opened access cavity offers many advantages, such as optimal preparation and sufficient irrigation of the root canal system, both of which may have positive effects on the success of root canal treatment [23].
The TEC preparation is a method in which the root canal orifices can be clearly located when looking from the occlusal side, and the cavity can be opened in a way that provides a straight path to the root canals [24]. The CEC method was developed as an alternative to the TEC. It is a modern operative approach, which aims to remove less dentin than in the TEC approach, thereby minimizing the effects of the procedure on the tooth's mechanical resistance and ensuring optimal preparation. Despite its advantages, the CEC method has some disadvantages, including the difficulty in locating the root canals and challenges during root canal preparation and cleaning [25]. Based on a literature search, no study has yet compared the amount of apical debris extrusion in teeth according to the shape of the access cavity (i.e., TEC vs. CEC). Thus, the present study compared the amount of apical debris extrusion during root canal preparation of mandibular first molar teeth according to whether a TEC or CEC procedure was performed.
The results of the present study showed that both the OC rotary single-file system and the RPC B reciprocating single-file system caused apical debris extrusion. There was no statistically significant difference among the TEC-OC, CEC-OC, and TEC-RPC B groups in terms of apical debris extrusion values. However, there was a statistically significant difference between the apical debris extrusion values of the CEC-RPC B group and those of the TEC-OC and CEC-OC groups. In the literature, there are no similar studies with which the results the present study can be directly compared.
In a study of mandibular incisors, Topçuoğlu et al. [26] compared the amount of apical debris extrusion using RPC, WaveOne (WO, Dentsply Maillefer), and One Shape (OS, MicroMega) files. They reported that the least amount of apical debris extrusion occurred in the OS rotary file group, and there was no statistically significant difference in the amount of apical debris extrusion between the RPC and WO groups. The authors attributed this result to the fact that rotary single-file systems transport more debris in the coronal direction in the canal than reciprocating single-file systems do. De-Deus et al. [27] applied the TEC procedure to mandibular molar teeth and compared the amounts of apical debris extrusion generated using 3 rotary file systems(RPC, WO, ProTaper) and a manual file (Flexo Files, Dentsply Maillefer) in mesial canals. The most apical debris extrusion was found in the manual file group, and the ProTaper conventional multifile system caused more apical debris extrusion than the RPC and WO file systems did. The authors attributed their findings to the following factors: single-file systems have fewer instruments than conventional multifile systems, single-file systems are made from advanced alloys, and the cutting efficiency of single-file systems is better than that of the conventional files. In the present study, there was no significant difference in the amount of apical debris extrusion between the rotary and reciprocating file systems in the TEC groups, whereas there was a significant difference between the 2 CEC groups. In the literature, many studies have reported different results regarding this issue. Some researchers reported that rotational movement caused more extrusion, while others reported that reciprocating movement caused more extrusion [2627]. We believe that this discrepancy is due to the different alloy and design properties of the files tested, as well as tooth selection, the shape of the cavity, and coronal flaring in their methodologies. The amount of apical debris extrusion in the CEC groups in the present study was greater than that in the TEC groups in both the OC and RPC B groups, but the difference was not statistically significant. In their micro-computed tomography (CT) study of mandibular molar teeth, Marchesan et al. [28] prepared 2 types of access cavities (TEC and CEC] and then compared the integrity of the original canal curvature and the total preparation time using Profile Vortex files (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) in mesial canals. The authors reported differences between the radii and angle values of the canal curvatures of the 2 groups. Furthermore, the total preparation time was longer in the CEC group than in the TEC group. They attributed these differences to having direct access to the canals in the TEC group and the requirement of a higher number of pecking motions in the CEC group for the files to reach the apical foramen, which extended the preparation time. In another micro-CT study on mandibular molar teeth, Krishan et al. [18] compared the total volume of dentin removed after canal preparation in groups in which a TEC and CEC were prepared using the WO system. They reported that much higher volumes of dentin were removed in the TEC group than in the CEC group. In the present study, in both the CEC-OC and CEC-RPC B groups, higher numbers of pecking motions were required to reach the apex. However, the volume of debris extruded from the apical foramen in both CEC groups was not as high as expected. We think that the reason for this difference related to the flexibility of the files that we used and the ability to release debris from the coronal part of the tooth.
In the present study, the RPC B single-file system caused more debris extrusion from the apical foramen in the CEC groups than did the OC single-file system. This may be because the OC single-file system is manufactured using C-wire heat treatment technology, which offers enhanced flexibility and easier access to canals. Additional factors that may explain the amount of debris extrusion using the single-file systems in the present study are the controlled memory alloy used in their production and their pre-bendability when compared to earlier versions of the files. However, since there is no study in the literature comparing C-wire and Blue Wire technologies in terms of a comprehensive range of metallurgical properties, further studies are needed to make a definitive judgment. In addition, due to the different taper of the files (RPC B, 0.08; OC, 0.06) used in our study, it is possible that the amount of debris formed during root canal preparation may be different, potentially affecting the amount of apical extrusion.
Changing the access cavity shape for both the RPC B and OC files did not result in a statistically significant increase in the amount of apical debris extrusion caused by these files. The reason for this is that the amount of extruded debris from the apex may be very low, which may have been affected by the sample size in the study. However, it is more likely that the alloy properties of the files can tolerate a disadvantageous cavity shape. In previous studies on apical debris extrusion, similar sample sizes were used based on the results of power analysis [2627].
The highest incidence of caries is seen in molar teeth, and the molar teeth are the reason for most patients’ first visit to a clinic for endodontic treatment [29]. As reported in similar studies in the literature, if sodium hypochlorite is used as a root canal irrigation solution, then the sodium crystals that form after vaporization cannot be distinguished from the extruded debris [2130]. This can make it difficult to determine the amount of apical debris extrusion accurately. Thus, distilled water was used as an irrigation solution in the present study.
Hülsmann and Hahn [31] reported that a file used with apical pressure in root canal shaping could cause debris extrusion from the apical foramen. Single- or multiple-file systems can be used in root canal preparation, as well as files with different movement kinematics (e.g., rotation or reciprocation). Thus, the present study compared the effects of OC and RPC B files with different kinematics on apical debris extrusion.
Finally, the cavity shape and the file system used are not the only factors affecting the amount of apical debris extrusion. Clinicians should consider all relevant factors in order to decrease apical debris extrusion.
CONCLUSIONS
Within the limitations of the present study, the RPC B and OC single-file systems tested using mandibular first molar teeth caused apical extrusion in all groups, and the RPC B system caused more apical extrusion in the CEC groups than did the OC single-file system. Therefore, it is suggested to use the RPC B file carefully in teeth with a CEC.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Yılmaz K.
Data curation: Tüfenkçi P.
Formal analysis: Adıgüzel M.
Funding acquisition: Yılmaz K.
Investigation: Tüfenkçi P.
Methodology: Yılmaz K.
Supervision: Yılmaz K.
Validation: Tüfenkçi P.
Writing - original draft: Yılmaz K.
Writing - review & editing: Tüfenkçi P, Yılmaz K, Adıgüzel M.
