Pulp revascularization with and without platelet-rich plasma in two anterior teeth with horizontal radicular fractures: a case report
Article information

Abstract
Pulp revascularization is an alternative treatment in immature traumatized teeth with necrotic pulp. However, this procedure has not been reported in horizontal root fractures. This is a case report of a 9-year-old patient with multiple horizontal root fractures in 2 upper central incisors that were successfully treated with pulp revascularization. The patient presented for treatment 2 years after the initial trauma, and revascularization was attempted after the initial treatment with calcium hydroxide had failed. Prior to pulp revascularization, cone-beam computed tomography and autoradiograms demonstrated multiple horizontal fractures in the middle and apical thirds of the roots of the 2 affected teeth. Revascularization was performed in both teeth; platelet-rich plasma (PRP) was used in one tooth (#11) and the conventional method (blood clot) was used in the other tooth (#21). Clinical and radiographic follow-up over 4 years demonstrated pulp calcification in the PRP-treated tooth. Neither of the 2 teeth were lost, and the root canal calcification of tooth #11 was greater than that of tooth #21. This case suggests that PRP-based pulp revascularization may be an alternative for horizontal root fractures.
INTRODUCTION
Pulp revascularization is a technique used in regenerative endodontics that aims to replace damaged structures and cells in the pulp-dentinal complex [1]. This procedure has been postulated as an alternative treatment for teeth presenting with pulp necrosis and open apices [2]. The conventional method for pulp revascularization entails the use of triple antibiotic paste for disinfection of the root canal system [3], along with the formation of a blood clot at the amelocemental junction. Mineral trioxide aggregate (MTA) can be used to seal the canal, providing a favorable environment for regeneration and repair of the tissues [245]. Pulp revascularization is a conservative treatment that induces maturation, increases root wall thickness, and promotes root development and closure [6]. However, this procedure has not been reported in horizontal root fractures.
The use of platelet-rich plasma (PRP) has been reported for bone augmentation [7], and it could potentially serve as an ideal matrix in regenerative endodontic treatments since it fulfills many of the characteristics of an adequate matrix. [8]. PRP is an autologous material that is easily reabsorbed and is rich in the growth factors contained in the alpha granules of platelets [91011]. In addition, PRP forms a 3-dimensional matrix that favors adhesion and cell migration, which assist in the proliferation of stem cells to induce repair and/or tissue regeneration [91011].
As described by Andreasen and Hjorting-Hansen [12], 4 healing modalities exist in cases of horizontal root fractures: 1) healing with calcified tissue, 2) interposition of connective tissue, 3) interposition of bone and connective tissue, and 4) interposition of granulomatous tissue. The latter is the most unfavorable [12], and is the one found in this case report.
The objective of this case report is to describe, for the first time, the induction of the healing process of 2 horizontal root fractures in 2 upper central incisors with a revascularization protocol performed at the level of the fractures. For this procedure, PRP was used in one tooth and the conventional method (blood clot) in the other tooth.
CASE REPORT
A 9-year-old male patient was evaluated at the endodontic clinic of the National University, School of Dentistry, Bogota, Colombia, on March 19, 2014. The patient had no prior medical or dental history. The trauma to his upper front teeth occurred 2 years previously (May 2012), and the initial autoradiogram revealed multiple root fractures at the level of teeth #11 and #21 (Figure 1A). One week after the first appointment, a flexible splint was placed between these 2 teeth, which remained present for approximately 7 months, based on the rationale that the teeth were very mobile and could be lost at any time. The parents were then informed that the prognosis of the case was poor and that extraction was recommended. They decided to request a second opinion (private practice); the splint was removed and endodontic treatment was started using intracanal medication, with calcium hydroxide paste placed on the fracture line in both teeth. This treatment was continued for approximately 1 year; however, the patient continued to have a sinus tract and pain in response to the percussion test, likely associated with necrosis of a coronal fragment, regardless of whether the apical fragment remained vital, which could be assumed due to the continuous apical growth of the teeth (Figure 1B and 1C). Given the lack of positive response to treatment, the patient was referred to our endodontic clinic.
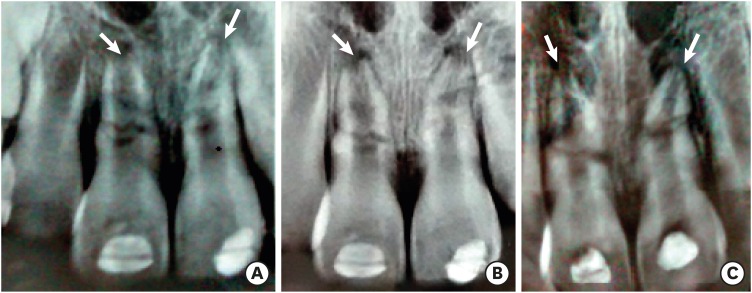
(A) Radiographs taken on July 21, 2012 in which multiple fractures are shown in teeth #11 and #21, as well as 2 radiopaque areas in the crowns of these teeth that are compatible with the restorative material used to hold the splint. (B) Autoradiogram taken on August 27, 2012 at a follow-up visit. (C) Autoradiogram taken on February 4, 2013 in which 2 radiopaque areas are observed in the crowns of both teeth, which are compatible with the material used to seal the pulp chambers after handling the intracanal medication. The progression of root formation in the apical third can be seen, likely because the apical fragment remained vital (white arrows).
First appointment
The first appointment occurred on March 19, 2014. The patient's clinical appearance can be seen in Figure 2A. Both teeth showed a mobility grade of 3, with no periodontal pockets or pain to horizontal or vertical percussion. Sinus tracts were present in both teeth. The pulp vitality, vertical percussion, and horizontal percussion tests were negative.
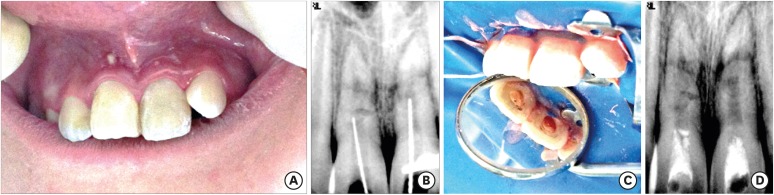
(A) Initial picture on March 19, 2014. (B) Root-length radiography was taken with a large file extending to the fracture lines. (C) Platelet-rich plasma was placed on tooth #11 and a blood clot on tooth #21. (D) Autoradiogram taken after completing the procedure, in which the mineral trioxide aggregate level can be observed at the entrance of the canals and the pulp chamber (April 9, 2014).
Radiographically, multiple fracture lines were observed at the cervical and middle levels of the root, as well as an increase in the periodontal ligament space, a periradicular lesion, and inflammatory external root resorption. These clinical and radiographic findings confirmed the diagnosis of horizontal root fracture with chronic apical abscesses in teeth #11 and #21. Considering the poor prognosis for both teeth, an informed consent form was signed, and a revascularization treatment protocol was initiated using autologous PRP in tooth #11 and conventional revascularization treatment with a blood clot in tooth #21.
Local anesthesia was administered with the infiltration technique, using 2% lidocaine with 1:100,000 epinephrine, temporary cement was removed from both teeth, proper isolation and access to the root canals were ensured, and the working length of each tooth was extended up to the fracture line with an apex locator (Root ZX, Morita, Tokyo, Japan) and confirmed with a periapical radiograph (Figure 2B). Profuse irrigation was performed for each tooth with 10 mL of 1.25% sodium hypochlorite (NaOCl) using Endo-Eze Irrigator Tips (Ultradent Products Inc., South Jordan, Utah, USA) without instrumentation. After drying the canals with sterile paper points, a triple antibiotic paste consisting of amoxicillin (500 mg), metronidazole (500 mg), and ciprofloxacin (500 mg) (triturated and mixed in a 1:1:1 ratio with sterile water to obtain a paste-like consistency) was introduced into the canal using a 4 Lentulo Spiral 25 mm (Dentsply Maillefer, Tulsa, OK, USA). After condensing the paste on the orifice of the canal, the access cavity was temporarily restored with a glass ionomer (Ketac Molar Easymix; 3M ESPE, St. Paul, MN, USA).
Second appointment (3 weeks after the first appointment)
The patient remained asymptomatic, and the intraoral sinus drainage had disappeared. Therefore, we conducted the second part of the revascularization protocol. PRP was obtained by drawing blood from the patient into sterile tubes with 3.8% sodium citrate that were centrifuged for 10 minutes at a speed of 3,000 rpm in a standard laboratory centrifuge (ROTOFIX 32; Andreas Hettich GmbH & Co., Tuttlingen, Germany). Subsequently, in a laminar flow chamber, the obtained fractions were carefully separated with a 500 μL sterile pipette to isolate the PRP in the middle of the tube, distinct from the red blood cells at the bottom and the platelet-poor plasma at the top of the tube. The PRP obtained was then transferred to a 10 mL hypodermic syringe to be prepared for injection into the canal. Following local anesthesia (2% lidocaine without a vasoconstrictor), and rubber dam isolation, the root canals were accessed and irrigated with 5 mL of 5.25% NaOCl to remove the antibiotic paste and then irrigated with 5 mL of sterile saline solution. Both canals were dried with sterile paper points, and the final Irrigation was carried out with 17% ethylenediaminetetraacetic acid for 1 minute in each tooth and then dried again [13]. We used a size 60 K-file to extend the working length until bleeding was achieved at the cementoenamel junction, and then waited for 20 minutes until hemostasis occurred and the fibrin clot stabilized. We only applied PRP on tooth #11, leaving the blood clot in place in tooth #21 with no further treatment (Figure 2C). Finally, the entrance of both canals was sealed with a 3-mm-thick layer of MTA Pro Root (Dentsply Maillefer) mixed according to the manufacturer's instructions. The MTA coronal barrier was sealed with a temporary filling glass ionomer (Ketac Molar Easymix; 3M ESPE). After completing the revascularization protocol, the patient was scheduled for periodic follow-ups. An autoradiogram at the end of this appointment was taken to verify the location of the coronal seal (Figure 2D).
First follow-up visit (3 months after the first appointment)
This visit took place on June 27, 2014. An autoradiogram did not show any changes in relation to the initial autoradiogram (Figure 3A). Cone-beam computed tomography (CBCT) showed a seal with MTA in both upper central incisors. Figure 4A shows the axial view, Figure 4B shows the coronal view, Figure 4C shows the sagittal view of tooth #11 (PRP), and Figure 4D shows the sagittal view of tooth #21 (blood clot). The final restoration was performed with a composite (Filtek Z 250, 3M ESPE) at this time.
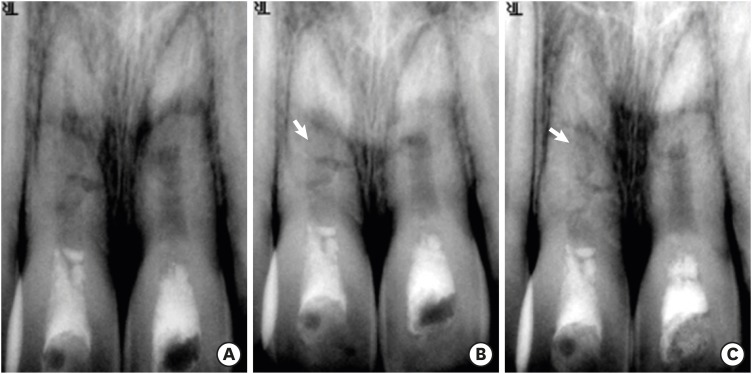
(A) Autoradiograms after treatment for teeth #11 (platelet-rich plasma) and #21 (blood clot) at 3 months (June 27, 2014), (B) 8 months (October 10, 2014), and (C) 1 year (March 19, 2015). White arrows show areas of calcification.
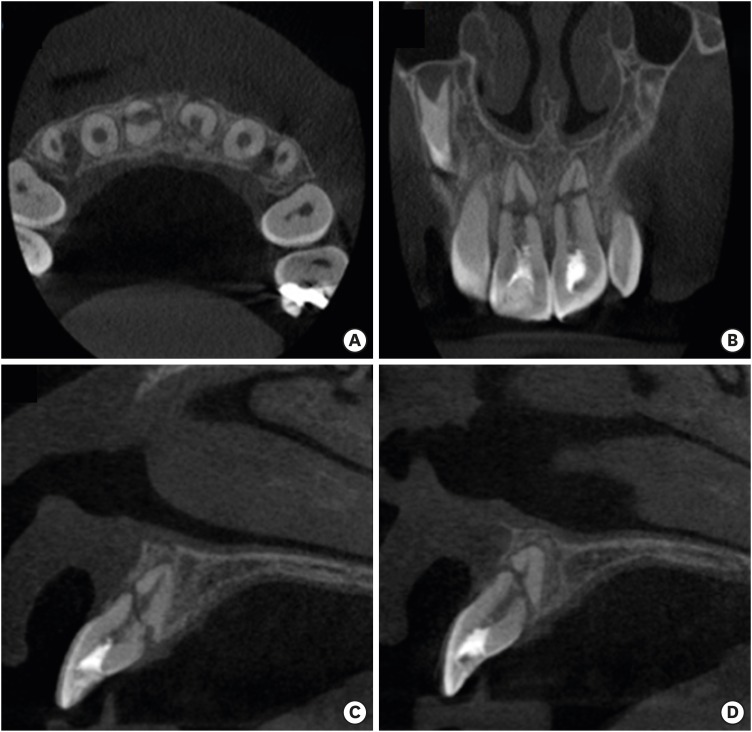
Cone-beam computed tomography images taken on June 27, 2014. (A) Axial view, (B) coronal view, (C) sagittal view of tooth #11 (platelet-rich plasma), (D) sagittal view of tooth #21 (blood clot). No significant changes in the fractures were seen radiographically.
Second follow-up visit (7 months after the first appointment)
This appointment was on October 10, 2014. An autoradiogram showed apparent mineralization in the distal wall of the canal of tooth #11 (Figure 3B); unfortunately, no more autoradiograms were taken at that time to confirm the aforementioned mineralization. There were no symptoms or signs of inflammation, infection, or sinus tract. Cold tests were performed, and the patient reported a delayed stimulus in tooth #21.
Third follow-up visit (1 year after the first appointment)
On March 19, 2015, an autoradiogram of tooth #11 showed greater calcification in the root canal space and the fracture lines at the middle third (Figure 3C). There was no presence of periodontal pockets or sinus tracts. Cold tests gave a delayed response in teeth #11 and #21.
Fourth follow-up visit (3 years after the first appointment)
On April 20, 2017, periapical radiography was taken in the orthoradial position for teeth #11 and #21. This image demonstrated calcification of the canal space of tooth #11 (PRP-treated). Preservation of the crestal alveolar bone of both teeth and the process of healing with interposition of calcified tissue in the fracture line of tooth #21 were observed (Figure 5A). There were no periodontal pockets and no presence of sinus tracts. The response to the cold test was positive in tooth #11 and negative in tooth #21. A CBCT scan was taken, on which it was possible to clearly observe the seal with MTA and the calcification that had occurred in the root canal space of both the coronal (Figure 5B) and the apical fragments of tooth #11 (Figure 5C and 5D). In tooth #21, the apical fragment had been mineralized, and the coronal fragment still had a defined root canal space (Figure 5E), but there was no evidence of periapical pathology (Figure 5B-5E).
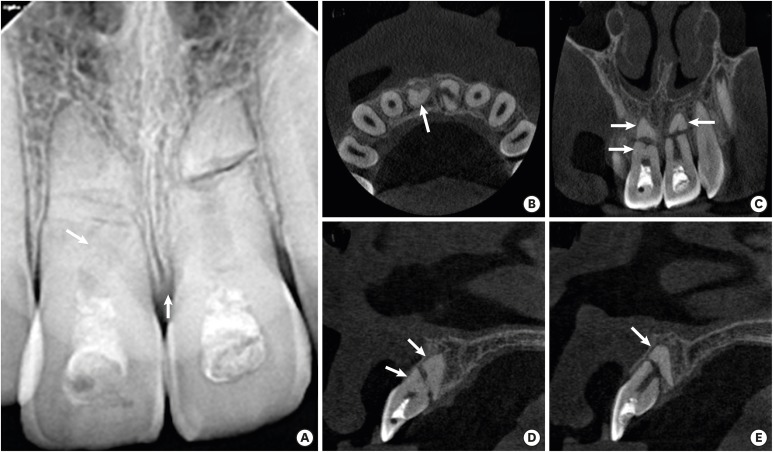
Follow-up imaging at 3 years after the procedure: autoradiogram and cone-beam computed tomography (CBCT) (April 20, 2017). (A) Autoradiogram with orthoradial angulation for teeth #11 (platelet-rich plasma [PRP]) and #21 (blood clot). White arrows show areas of calcification and crestal alveolar bone. CBCT images showing the (B) axial view, (C) coronal view, (D) sagittal view of tooth #11 (PRP), and (E) sagittal view of tooth #21 (blood clot). White arrows show areas of calcification in the apical and coronal fragments of tooth #11 and only in the apical fragment of tooth #21.
Fifth follow-up visit (4 years after the first appointment)
On April 19, 2018, periapical radiography was taken in the orthoradial position (Figure 6A). The pattern of calcification into the root canal space of tooth #11 (PRP-treated) was still observed (Figure 6A), and it was also possible to see the displacement of the apical fragment of tooth #21 (Figure 6A). It is noteworthy that periodontal ligament formation was observed in the apical zone of the coronal fragment of tooth #21, as well as preservation of the level of the crestal alveolar bone of both teeth. The mobility of both teeth was grade 3. CBCT was again performed, showing that the calcification process continued in both fragments of tooth #11 (Figures 6B-6D). In tooth #21, displacement of the apical fragment was confirmed (Figure 6E). Finally, at this follow-up there was no presence of periapical pathology in either tooth (Figure 6B-6E).
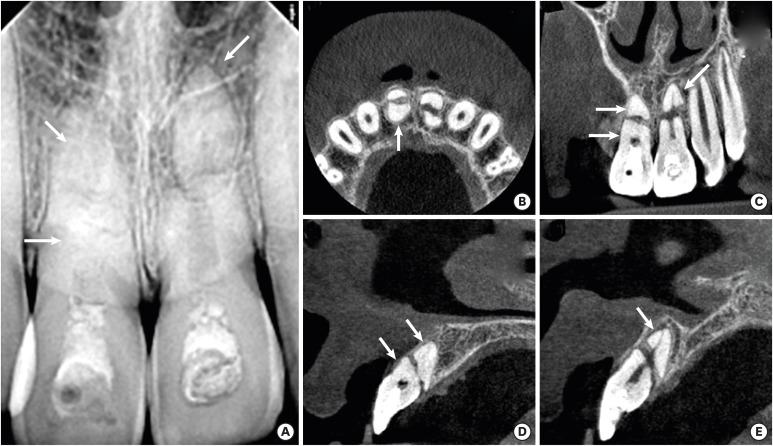
Follow-up imaging at 4 years after the procedure: autoradiogram and cone-beam computed tomography (CBCT) (April 19, 2018). (A) Autoradiogram with orthoradial angulation for tooth #11 (platelet-rich plasma). and #21 (blood clot).White arrows show clear calcification in the apical and coronal fragments of tooth #11 and calcification in the apical fragment of tooth #21. CBCT images showing the (B) axial view, (C) coronal view, (D) sagittal view of tooth #11 (PRP), and (E) sagittal view of tooth #21 (blood clot). In all views, white arrows show clear calcification in the apical and coronal fragments of tooth #11.
DISCUSSION
In endodontics, revascularization is a set of procedures based on molecular and cellular biology that seek to promote healing, root maturogenesis, and tissue replacement of the dentinopulpar complex to restore the physiological functions of the dental pulp [14]. Angiogenesis plays a fundamental role in the success of the treatment because cells migrating to the root canal require nutrients and oxygen to survive. For this reason, revascularization is possible in any tooth with an open foramen, and an even better prognosis is possible if the apical diameter is greater than 1 mm [15].
Although in the present case report, we showed a slightly better result for revascularization with PRP than with a blood clot, it is necessary to perform clinical trials that complement our findings, since the use of PRP vs. a blood clot remains controversial.
Zhang et al. [16] conducted a study in beagle dogs where a histological comparison was made between the use of PRP and the conventional blood clotting-based therapy [2] in endodontic regeneration procedures. They concluded that there were no significant differences in the healing of periapical lesions, apical closure, and thickening of the root canal walls. Taking into account that Zhang et al. [16] carried out an experimental study, while we are only reporting a clinical case, we can say that their results do not fully agree with what was observed in our clinical case, in which calcification with possible biomineralization [1718] was observed in the root canal of the tooth treated with PRP, but not in the tooth revascularized using blood clotting only. This difference might have been due to the fact that in our case, the revascularization procedure was not performed through the open apex, but by stimulating the tissue present in the fracture lines. In contrast, Jadhav et al. [9] compared revascularization in non-vital immature anterior teeth using blood clotting only vs. blood clotting and PRP. After 6–12 months, they found that in all cases, regardless of the protocol used, patients were asymptomatic and without inflammation or sinus tracts. However, although all the cases were successful, the group with the traditional protocol (blood clot only) showed lower grades of improvement (ranging between “satisfactory” and “good”), whereas the protocol with PRP and blood clot obtained better scores (“good” and “excellent”). In our clinical case, we used the 2 types of protocols proposed by Jadhav et al. [9], but compared them in the same individual. Overall, the outcome of our case agrees with their study because both teeth were successfully treated, but there was slightly better outcome for the tooth treated with PRP.
Dianat et al. [19], in a study conducted in immature teeth of dogs, compared the blood clot protocol vs. the use of plasma rich in growth factors, but the results did not have significant clinical or histological differences, since an apical closure of 53.33% was found radiographically in teeth with the blood clot protocol, whereas it was 60% in the group that received plasma rich in growth factors. Furthermore, histological confirmation of new tissue formation was found in 60% of the cases in both groups. Based on the aforementioned evidence, they concluded that the use of plasma rich in growth factors was not superior to the use of blood clots in terms of apical closure and new tissue formation; these results do not coincide with what was observed in the present clinical case. Discrepancies in the results are probably due to differences in plasma extraction and preparation protocols, as these factors influence the platelet concentration and the type of clot activator. Chaniotis et al. [20] reported the management of a patient with root fractures in the upper central incisors by mixing MTA with blood and introducing it into the canal to promote the formation of hard scar tissue in multiple horizontal root fractures. They concluded that this mixture created a favorable environment for tissue regeneration. From a purely comparative perspective, their procedure was very different from the one used in our present clinical case (we used conventional revascularization and PRP), and in both cases the MTA was used only to seal the coronal third, and was not mixed with the blood clot. However, we think that the favorable environment for mineralization provided by the MTA may have contributed to the success in our clinical case as well.
Our case also highlights the advantages of CBCT in the evaluation of root fractures. While a CBCT scan provides a 3-dimensional image, periapical radiography only presents a view in 2 dimensions. Periapical radiographs are also more likely to have errors of interpretation because the positioning of the radiographic plate and the X-ray tube can influence the obtained image. As a result, in complex cases, several periapical autoradiograms at different angulations are needed to make an accurate diagnosis. In contrast, a single CBCT image provides an exact 3-dimensional tomographic image of the dental region [2122].
CONCLUSION
In conclusion, our case suggests that biologic endodontic therapy performed with PRP is a safe procedure that can be successfully used in cases of horizontal root fracture with necrosis of the coronal fragment, obtaining healing with calcified tissue according to clinical and radiographic criteria.
It is necessary to carry out clinical studies with more cases to support the procedure performed in the present clinical case.
ACKNOWLEDGEMENT
The authors would like to thank Dra Magdalena Moreno for the assistance provided during the preparation of this manuscript.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Arango-Gómez E, Sossa-Rojas H, Jordan F, Nino-Barrera JL.
Data curation: Arango-Gómez E.
Formal analysis: Arango-Gómez E, Sossa-Rojas H.
Funding acquisition: Sossa-Rojas H.
Investigation: Nino-Barrera JL, Nino G.
Methodology: Arango-Gómez E, Sossa-Rojas H.
Project administration: Arango-Gómez E, Sossa-Rojas H.
Resources: Sossa-Rojas H.
Software: Arango-Gómez E.
Supervision: Nino-Barrera JL.
Validation: Nino-Barrera JL, Nino G.
Visualization: Nino-Barrera JL.
Writing - original draft: Nino G, Nino-Barrera JL.
Writing - review & editing: Nino-Barrera JL, Nino G.