Dentinal defects induced by 6 different endodontic files when used for oval root canals: an in vitro comparative study
Article information

Abstract
Objectives
To compare the formation of dentinal defects using stainless-steel hand K-files (HFs), rotary files, reciprocating files, and Self-Adjusting File (SAF), when used for oval root canals.
Materials and Methods
One hundred and forty extracted human mandibular premolar with single root and oval canal were selected for this study. Oval canals were confirmed by exposing to mesio-distal and bucco-lingual radiographs. Teeth with open apices or anatomic irregularities were excluded. All selected teeth were de-coronated perpendicular to the long axis of the tooth, leaving roots segments approximately of 16 mm in length. Twenty teeth were left unprepared (control), and the remaining 120 teeth were divided into 6 groups (n = 20) and instrumented using HF (size 40/0.02), Revo-S (RS; size 40/0.06), ProTaper NEXT (PTN; size 40/0.06), WaveOne (WO; size 40/0.09), RECIPROC (RC; size 40/0.06), and the SAF (2 mm). Roots were then sectioned 3, 6, and 9 mm from the apex, and observed under stereomicroscope, for presence of dentinal defects. “No defect” was defined as root dentin that presented with no visible microcracks or fractures. “Defect” was defined by microcracks or fractures in the root dentin.
Results
The control, HF, and SAF did not exhibit any dentinal defects. In roots instrumented by RS, PTN, WO, and RC files exhibited microcracks (incomplete or complete) in 40%, 30%, 55%, and 50%, respectively.
Conclusions
The motor-driven root canal instrumentation with rotary and reciprocating files may create microcracks in radicular dentine, whereas the stainless-steel hand file instrumentation, and the SAF produce minimal or less cracks.
INTRODUCTION
The nickel-titanium (NiTi) files were introduced in 1998 for their use in endodontics and undergone various advances in their designs and use concepts for root canal instrumentation [1]. The super-elasticity of motorized NiTi instruments allows it to be used in root canal instrumentation with a decreased incidence of canal transportation and also requires less time to prepare canals [2]. However, Shemesh et al. [3] revealed that the efficiency of rotary instrumentation might also have a biomechanical effect on the radicular dentin by creating microcracks in it. This finding has been supported by several studies reported in literature [3456]. The mentioned studies used hand K-files (HFs; stainless-steel or NiTi), rotary files (multiple or single), and reciprocating files. These microcracks may propagate and lead to a full-thickness fracture into the radicular dentin, leading to a vertical root fracture, if the tooth is subjected to repeated stresses from endodontic procedures. Nevertheless, factors other than the endodontic files like; force of instrumentation and obturation; retreatment procedure and high concentration of hypochlorite may also be responsible for the formation of dentinal defects in different degrees [7].
The prevalence of oval canals in mandibular premolar teeth is high if a single canal is present. The currently used rotary/reciprocating NiTi endodontic files result in a circular preparation for irregularly shaped root canals [8]. A round canal preparation in an oval canal decreases the remaining dentin thickness and increases the susceptibility to fracture [9].
The present research was designed to compare the propagation of dentinal defects, that are caused by HFs and various motor-driven endodontic files in mandibular premolars; rotary files; Revo-S (RS; Micro-Mega, Besançon, France) and ProTaper NEXT (PTN; Dentsply Sirona, Ballaigues, Switzerland), reciprocating files WaveOne (WO; Dentsply Maillefer, Ballaigues, Switzerland) and RECIPROC (RC; VDW, Munich, Germany), and Self-Adjusting File (SAF; ReDent-Nova, Raanana, Israel).
MATERIALS AND METHODS
Selection and preparation of specimens
The study protocol for this study was approved at the Institutional Review Board at the Nair Hospital Dental College (Mumbai, India). One hundred and forty extracted human mandibular premolar teeth with single root and oval canal were selected for this study. Oval canals were confirmed by exposing to mesio-distal and bucco-lingual radiographs. Teeth with open apices or anatomic irregularities were excluded from the current study. All selected teeth were de-coronated perpendicular to the long axis of the tooth by using a diamond-coated bur with water-cooling, leaving roots segments approximately of 16 mm in length. All roots were embedded in auto-polymerizing acrylic resin, and periodontal ligament simulation was performed using hydrophilic vinyl polysiloxane impression material (3M ESPE, Seefeld, Germany) as described previously [10].
Canal patency was established till a size 10 K-File (Dentsply Sirona) in canals. In the HF group the root canals were prepared till size 40 apical size (2% taper). For standard apical preparation, in the other groups the apical preparation were maintained by; rotary RS till file AS40 (size 40/0.06) and PTN till file X4 (size 40/0.06), reciprocating WO Large (size 40/0.08) and RC R40 (size 40/0.06). In the SAF group the samples were instrumented using 2 mm diameter file. For the HFs a balanced force technique and all the other files were used according to manufacturers' instructions for instrumentation of root canals.
Root canal instrumentation
1. Group HF using Stainless-steel HF
Stainless-steel HFs (2% taper) were used to enlarge the root canals to size 40 using the balanced force technique. Files were inserted by a quarter-turn clockwise (CW) rotation of 90° with no apical pressure and cutting was accomplished by counter-clockwise (CCW) rotation of 120° applying sufficient apical pressure. Then working length (WL) was incrementally reduced by 1 mm beginning from sizes 45 to 70 K-file instrument. Irrigation was performed with 5% sodium hypochlorite. For each canal, a new set of K-file was used.
2. Groups RS and PTN using rotary NiTi files
The samples in the group RS were instrumented using sequential RS rotary files. The root canal orifices were preflared using EndoFlare (Micro-Mega). The canals were instrumented at a rotational speed of 300 rpm at a torque of 2.5 Ncm using a torque-controlled endodontic motor (X-Smart Plus, Dentsply Sirona). The sequential files after orifice flaring were used in the following order: SC1 (size 25/0.06) was used until the two-third length of the root canal was reached, SC2 (size 25/0.04) and SU (size 25/0.06) files were used up to the full WL. After this, AS30 (size 30/0.06), AS35 (size 35/0.06), and AS40 (size 40/0.06) files were used till WL.
Before introducing each file, the root canal was irrigated with 5% NaOCl (Prime Dental, Mumbai, India), the canal was recapitulated, and the subsequent file was introduced in the aforementioned sequence. EDTA Gel (RC Help: Prime Dental) was used as lubricant for the file with every reinsertion of the file.
In this group PTN, the samples were instrumented by PTN instruments, used according to the manufacturer's instructions using a gentle in-and-out motion with the same endodontic motor at 300 rpm and a torque of 2.5 Ncm. The root canal orifice was flared using ‘SX’ file from the ProTaper Universal (Dentsply Sirona). This was followed by the use of X1 (size 20/0.04), X2 (size 25/0.06), X3 (size 30/0.06) and X4 (size 40/0.06) files. On meeting obstruction, the file was removed and the canal was irrigated, recapitulated, and the file was re-introduced into the canal again. The instrumentation was continued till the X1 and X2 both reached the WL.
3. Groups WO and RC using reciprocating NiTi files
Fifteen samples of this group were instrumented by single reciprocating file WO large (size 40/0.09) instrument, used in a pecking motion. A large file was selected according to the manufacturer's instructions (size 25 K-file reached the apex passively). The root canal orifice was flared using SX file from the ProTaper Universal. A pre-programmed reciprocating endodontic motor (X-Smart Plus) possessing the program for WO (small, primary, and large) files was used. The WO file was introduced in the canal with reciprocating and in-and-out pecking motion. On meeting an obstruction, the file was removed, the canal was irrigated, recapitulated, and the file was re-introduced into the canal again. The instrumentation was done till the WO large file reached the apex. The same EDTA Gel was used as lubricant. Instrumentation was continued in the aforementioned manner until the file reached the WL.
The samples in this group RC were instrumented using RC R40 (size 40/0.09) files, with the same endodontic motor. The R40 was selected according to the manufacturer's instruction (size 25 K-file reached the apex passively). The RC file was introduced in the canal with a reciprocating and pecking (in-and-out) motion, similar to that used in group 4 and was continued till WL. The same EDTA Gel was used as lubricant.
4. Group SAF using SAF system
The samples were instrumented using 2.0 mm SAF with transline motion (in-and-out). The file was operated with in-and-out pecking motion till the WL at 5000 vibrations/min using the EndoStation endodontic system (ReDent-Nova). The file was operated for 4 minutes with continuous irrigation with 5% NaOCl at a flow rate of 4 mL/min (as recommended by the manufacture). The irrigation solution was applied through the hollow file using a built-in peristaltic pump. This was followed by the removal of smear layer with 5 mL of 17% aqueous EDTA (Dent Wash, Prime Dental) for 1 minute and a final rinse with 5 mL of distilled water.
Sectioning and microscopic examination
All roots were sectioned perpendicular to their long axes at 3, 6, and 9 mm from the apex using a diamond-coated saw (Isomet 1000 precision saw, Bueller, Lake Bluff, IL, USA) under a continuous water stream. Each specimen was then checked for the presence of dentinal defects/microcracks. Two observers who were blinded to the group to which a given sample belonged and who were initially checked for inter-observer reproducibility checked the specimens independently. The examination was performed using a stereomicroscope (Olympus, Tokyo, Japan) at ×20 magnification. The entire periphery of the root slice was examined for dentinal microcracks or complete, full-thickness fractures. “No defect” was defined as root dentin that presented with no visible microcracks or fractures. “Defect” was defined by microcracks or complete fractures in the root dentin. A tooth with a microcrack or fracture in one or more of its segments was defined as a tooth with defects.
Digital images of sections with defects were captured using a digital camera (Sony Alpha NEX-7, Sony, Tokyo, Japan) attached to the microscope. A total of 60 segments were examined in each group for a total of 420 root segments. The results were expressed as the number and percentage of teeth with defects or cracks out of the total number of teeth in each group.
Statistical analysis
The results were numerically expressed and as percentages of cracks in each group, followed by analyzing the data with χ2 test with the significance level set at p < 0.05.
RESURTS
Incidence of microcracks after instrumentation
The unprepared canals (control group), the HF group, and the SAF group presented no defects. Defects were found in rotary file (RS and PTN), and reciprocating file (WO and RC) groups. The percentages of roots with defects in each group are shown in Figure 1. There was a statistically significant difference between the rotary/reciprocating file groups and the control/hand file/SAF file groups, which presented no defects (Table 1, p < 0.0001).
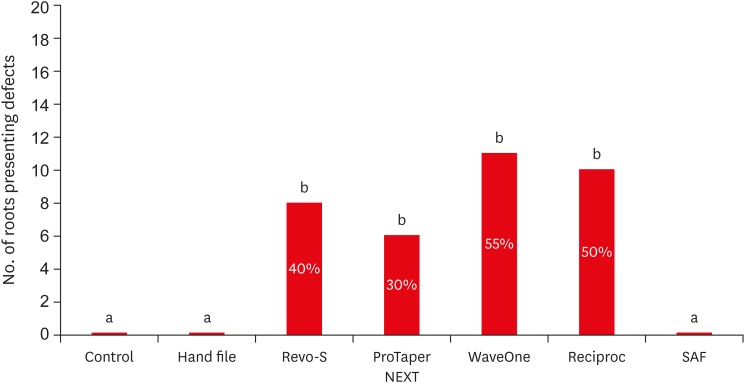
Percentages and number of roots presenting dentinal defects (a, b: Significant differences between groups with the different alphabets).

Types of microcracks
The stereomicroscopic images of no crack, incomplete crack; external (red arrow), internal (black arrow) and a higher magnification of a fracture are presented in Figure 2. The PTN group had the lowest number of defects (6/20 roots) 30%; RS (8/20) 40%, reciprocating, RC (10/20) 50% and WO had the highest incidence of defects (11/20) 55%. However, no significant difference was detected among these groups (p > 0.05, Figure 1).
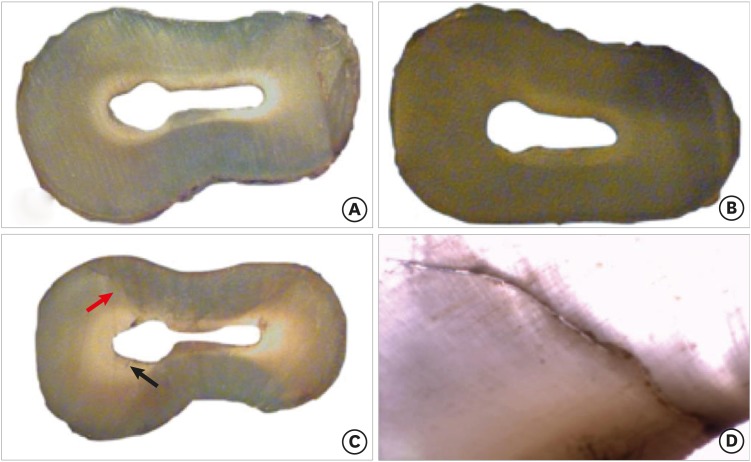
Representative images of dentinal defects. (A, B) No cracks (seen for hand K-file and Self-Adjusting File groups). (C) Incomplete cracks: red arrow, external surface; and black arrow, internal surface. (D) High magnification of a fracture (from lumen of the canal to the external surface).
Type and location of the defects
In the WO group 1 roots (5%), and RC group 2 roots (10%) presented with a full thickness fracture, while the remaining 31 defects found in all the groups were defined as microcracks (Table 1). These microcracks were seen originating either from the internal surface (22/31), or the external surface (9/31) of the roots (Table 1). The number of dentinal defects seen at 3 mm, 6 mm, and 9 mm are tabulated in Table 2. There was a significant higher incidence of microcracks at the 6 mm and 9 mm levels of roots in the rotary/reciprocating file groups (p < 0.05).

Occurrence of dentinal defects
DISCUSSION
Root canal preparation with different rotary NiTi endodontic instruments may cause stress and strain, which can lead to micro cracks or craze line formation in root dentin [3]. The current study aimed to investigate and compare the effect of endodontic files using different kinematic motions (rotary, reciprocating, and vibratory) on the formation of dentinal microcracks. The total volume of dentin removed from root canals is significantly greater with NiTi engine driven systems may contribute for the formation of the defects [3]. A reciprocal motion has shown various advantages like; extended durability, resistance to cyclic fatigue, and centered root canal preparation [11]. Also, this motion is associated with CW and CCW rotation consequently and repeatedly, aiding the release of file when it is engaged in the radicular dentin during the preparation process [12]. Nevertheless, Bürklein and Schäfer [13] reported high debris transportation toward the apex enhances with reciprocal motion, increasing torsional forces.
Resistance to tooth fracture is an important aim in endodontics as they may decrease the long-term survival rate. Previous experimental studies have shown that excessive removal of dentin during root canal preparation may create fractures in teeth [34]. In the current study, 3 complete fractures were seen (1 in WO, 2 in RC), and it seems that the reason of fracture was the weakening of the tooth structure that may have been caused by the excessive removal of dentin (size 40/0.09 and size 40/0.06). Various degrees of fracture rates have been reported, when obturation and retreatment procedures were included [3514]. The present study did not test the effects of obturation or retreatment; therefore, the results showed a relatively low fracture rate.
In the current study, no dentinal defect was observed in the control, HF, and SAF groups. In these groups, rotational movement was not applied; instead, Ingle's standardized preparation technique was used with HFs, and transline in-and-out oscillation motion was used for SAF. The hand file has 2% of taper and which is smaller than other rotary files with 4% or bigger taper. Thus, the tensile force generated from the hand files would be smaller than those from the rotary files, especially at the mid and coronal root canal area. The SAF is a hollow file that compresses into the unprepared canal and then attempts to regain its original shape/dimensions, applying a constant delicate pressure on the canal walls, allowing uniform removal of dentin along the whole perimeter of the root canal cross-section [15]. Also, this reactionary stress generated by the SAF is very minimal compared to the rotary files, which may increase the chance of preservation of root dentin integrity with a reduced risk of dentinal defects [1617]. It might be the reason why SAF did not create any defects in experimental samples.
The rotary and reciprocating files create microcracks in the radicular dentin ranging from 15% to 60% [8]. PTN, WO and RC were made of M-wire and it was known to have softer characteristic than the conventional NiTi wire and stainless-steel. However, they have shown much higher incidences of crack formation. It seemed due to the fact that these files possess a solid metal core with flutes and blades for increased cutting. Also, the large-sized taper of these files result in excessive, unnecessary removal of the dentin, thus weakening the root, and such aggressively cutting the dentin may contribute to microcrack formation [9151617]. The PTN and RS files work in a continuous rotation motion and caused 30% and 40% cracks in the current study. The WO and RC that are used in reciprocating motion, however, caused higher number of microcracks in the roots; 55% and 50%, respectively.
During root canal instrumentation, the canal is enlarged as a result of contact between endodontic file and dentin walls. These contacts result in momentary stress concentrations in the radicular dentin. Such stress concentrations result in initiation of dentinal defects. Contact stress levels are determined by the mechanical behavior of files, which is determined by their cross-sectional and longitudinal design [18].
The rotary files with higher tapers tend to generate more stresses into the radicular dentine when used for instrumentation, hence contributing as one of the factor for crack formation in root dentin [1519]. In the current study micro cracks occurred in 30% to 55% of the roots. Some studies are not in accordance with these results as they have reported less percentages of dentinal defects occurrence [3]. However, our study is in accordance with the studies of Wilcox et al. [14], Shemesh et al. [7], Yoldas et al. [4], and Gergi et al. [19].
RC was reported to cause more complete cracks than WO [19]. In the current study also 2 roots instrumented by RC complete fracture whereas only 1 root instrumented by WO exhibited a complete fracture. RC files exhibit a S-shaped geometry with a double cutting edge while WO has a modified triangular cross section with radial lands at the tip and a convex triangular cross section in the middle and coronal portion of the instrument. The WO cross-section results in lower cutting efficiency [192021].
Recently introduced instrument systems are made of different alloys with different heat treatments. Some of them are special characterized with a non-linear shape or shape change in the root canal by the temperature during shaping. All these characteristics may bring a different effect on root dentin integrity during instrumentation. Therefore, future studies using these new systems would be helpful for clinician to understand and select an efficient instrument system.
CONCLUSIONS
Under the study limitations, the motor-driven root canal instrumentation with rotary and reciprocating files may create microcracks in radicular dentine, whereas the stainless-steel hand file instrumentation, and the SAF produce minimal or less cracks.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Pawar AM, Kim HC.
Data curation: Pawar AM, Thakur B.
Formal analysis: Pawar AM, Kim HC.
Investigation: Pawar AM, Thakur B, Kfir A.
Methodology: Pawar AM, Kim HC, Kfir A.
Project administration: Pawar AM.
Resources: Pawar AM.
Software: Kfir A.
Supervision: Kim HC.
Validation: Pawar AM, Kim HC.
Visualization: Pawar AM.
Writing - original draft: Pawar AM.
Writing - review & editing: Kim HC.

