Effect of cooling water temperature on the temperature changes in pulp chamber and at handpiece head during high-speed tooth preparation
Article information

Abstract
Objectives
It was the aim of this study to evaluate the effect of cooling water temperature on the temperature changes in the pulp chamber and at the handpiece head during high-speed tooth preparation using an electric handpiece.
Materials and Methods
Twenty-eight intact human molars received a standardized occlusal preparation for 60 seconds using a diamond bur in an electric handpiece, and one of four treatments were applied that varied in the temperature of cooling water applied (control, with no cooling water, 10°C, 23°C, and 35°C). The temperature changes in the pulp chamber and at the handpiece head were recorded using K-type thermocouples connected to a digital thermometer.
Results
The average temperature changes within the pulp chamber and at the handpiece head during preparation increased substantially when no cooling water was applied (6.8°C and 11.0°C, respectively), but decreased significantly when cooling water was added. The most substantial drop in temperature occurred with 10°C water (−16.3°C and −10.2ºC), but reductions were also seen at 23°C (−8.6°C and −4.9°C). With 35°C cooling water, temperatures increased slightly, but still remained lower than the no cooling water group (1.6°C and 6.7ºC).
Conclusions
The temperature changes in the pulp chamber and at the handpiece head were above harmful thresholds when tooth preparation was performed without cooling water. However, cooling water of all temperatures prevented harmful critical temperature changes even though water at 35°C raised temperatures slightly above baseline.
INTRODUCTION
During tooth preparation with a high-speed handpiece, friction between the tooth structure and rotating bur creates excessive heat. As the handpiece rotates, the bur rotates at the speeds of 200,000–400,000 rpm, and can generate temperatures that reach up to 240°C at dentin-enamel junction during tooth preparation without cooling [1]. This heat can result in structural changes to the hard dental tissues and pathologic changes to the dental pulp. Therefore, there is consensus in the dental literature regarding the mandatory use of cooling water during tooth preparation with high-speed handpieces [234]. This cooling technique is considered simple and effective to prevent heat gain [5]. Moreover, water cooling allows for efficient cutting by preventing clogging of the rotary cutting instrument, and acts as a lubricant between the rotary cutting instrument and the tooth structure [67]. Theoretically, the major variables that affect the heat absorption capacity of cooling water are its flow rate and temperature [8]. Many previous reports [45678910] have concluded that flow rates of 30 to 50 mL/min are adequate for cooling, and the International Organization for Standardization has recommended a coolant flow rate of 50 mL/min [11]. This flow rate prevents thermal damage to the dentin-pulp complex without affecting the clinician's visibility during preparation [12]. However, few recent studies have examined the effect of cooling water temperatures on heat gain in the tooth, and those that did assess temperature change in the pulp chamber during tooth preparation did not take into consideration of the effect of cooling water temperature.
Recently, the electric handpieces became well known in dental clinics, and used more frequently in tooth preparation because it is more efficient cutter than the air-driven handpieces (also known as turbines), and the electric handpiece provides a steady load with a smooth and even cutting rate [131415]. In addition, it is more hygienic, produces less aerosol during use, and produces less noise [16]. High torque handpieces differ significantly in their components, driving power, and mechanisms compared to turbines [17]. Specifically, electric handpieces have an electric motor with rotating transmission gears instead of driving air through turbines. Therefore, high friction is created in the transmission bearings, and the lack of cooling caused by driving air results in a greater heat load that is conducted to the handpiece surface because of its metal components. This heat builds up in the handpiece body if not controlled by an efficient cooling mechanism, which can cause pain or soft tissue burn [1819]. Furthermore, the hot handpiece body heats the cooling water running through it [8], and may result in not sufficient cooling water temperature to prevent heat gain during tooth preparation. This is especially true if the water source comes from municipal supplies that already is at elevated temperatures.
There has been a lack of recent information available in the literature regarding the role of cooling water temperature on heat gain both in the pulp chamber and at the handpiece head during tooth preparation using an electric handpiece. Therefore, this study evaluated the effects of different cooling water temperatures on the temperature changes in the pulp chamber during tooth preparation using an electric handpiece. In addition, the temperature change at the electric handpiece head during tooth preparation was assessed at different cooling water temperatures.
MATERIALS AND METHODS
Specimen preparation
This study was conducted in full accordance with the World Medical Association Declaration of Helsinki, and ethical approval was obtained as per the university's protocols by the ethics committee at the College of Dentistry of Qassim University (DEC/ST/25/2017). Twenty-eight freshly extracted intact human maxillary first molar teeth were used in this study. These teeth all were extracted for periodontal reasons and were maintained in distilled water at room temperature until use. The root of each sample was sectioned perpendicular to the long axis of the tooth at 1 mm below the cemento-enamel junction using a diamond disc with a water spray coolant. The pulp tissue then was removed using an excavator, and the pulp chamber was cleaned thoroughly by rinsing with 5.25% sodium hypochlorite followed by normal saline. Irregularities of the pulp chamber were removed by a large flat end tapered finishing carbide bur with a water spray coolant.
To facilitate tooth manipulation and fastening to a slider's mini vice, the remaining 1 mm of the root was notched horizontally for retention to an acrylic resin and then embedded in a cold-cure acrylic resin (Duralay, Reliance Dental Mfg., Worth, IL, USA) using a standardized rectangle silicone mold (19 × 10 × 3 mm). To prevent the acrylic resin from entering the pulp chamber, the entrance was covered with a small piece of adhesive tape.
After complete polymerization of acrylic resin, each tooth's occlusal surface was prepared to remove the enamel using a rotary diamond-cutting instrument with a high-speed handpiece and the water spray coolant. Then an abrasive tip mounted in a low-speed handpiece was used to prepare the dentine to make a flat dentine surface. During this procedure, a backhause type caliper was used to standardize the dentine thickness at 2.5 mm. Teeth with abnormally large pulp chambers with thin dentin less than 2.5 mm thickness remaining after preparing the flat dentin surface were excluded from the study. The flat, exposed dentin surface was polished with fine (24 μm) aluminum oxide polishing disks (Sof-lex, 3M ESPE, St. Paul, MN, USA). The adhesive tape covering the pulp chamber entrance was removed using tweezers, and two K-type thermocouple probes were inserted into the pulp chamber so that their non-insulated tips were touching the roof of the chamber. Radiographs were taken to confirm the position of thermocouples (Figure 1). Following conformation, a high-conductivity thermal compound (Arctic MX-4, Arctic, Braunshweig, Germany) was injected into the pulp chamber to facilitate heat conduction from the chamber walls to the thermocouples, and the thermocouples were secured in position by fold-back clip. Then, the apical portion of the pulp chamber was sealed using glue pads (UHU GmbH, Bühl, Germany). The assembly was attached to a custom-made motorized precision linear slider table programmed to move in 2 mm forward and backward increments (Figure 2).

Radiograph showing thermocouples inside pulp chamber.

Schematic diagram of test apparatus.
Tooth preparation assembly
An ELECTROtorque plus dental electric motor system with INTRA LUX KL 701 micromotor and INTRAmatic 25 CH electric handpiece (KaVo Dental Corp., Biberach, Germany) were used in this study. The system was attached to an A-dec stationary simulator (A-dec Inc., Newberg, OR, USA) with a self-contained water bottle. This simulator has two handpiece tubes (4-way hoses), one that was connected to the back of the electric handpiece control unit and the other was used to verify cooling water temperature prior to each specimen preparation (Figure 2). The temperature of the water was measured by collection at the end of the 1.6 mm coolant water tube that was disconnected from the 4-way connector. The cooling water temperature was adjusted (increased or decreased) in the self-contained water bottle until the water exiting from the 1.6 mm tube at the end of the hose reached the desired temperature (± 2°C). The measured water temperature just prior to entering the electric handpiece system was used to standardize the water temperature (water temperature may change while it runs from the self-contained water bottle through the simulator's tubes and valves) and to exclude the warming effect of the handpiece body on the cooling water temperature.
To measure the handpiece head temperature, two K-type thermocouple probes were attached to the handpiece using rubber band, and their non-insulated tips touched the head were fixed in position with cyanoacrylate adhesive. The electric handpiece system was set to run the 1:5 electric handpiece at its highest speed (200,000 rpm) with a 2.7 N·cm torque. The cooling water rate from the handpiece's three-jet cooling water spray holes was set to 50 mL/min. To measure the rate of coolant water, the handpiece ran for 1 minute and the cooling water was collected in a graduated tube. The coolant water control knob was adjusted on the side of the simulator and the back of the electric micro-motor until a 50 mL/min flow rate was achieved. To standardize the load applied during tooth preparation, the handpiece was clamped to the vertical arm of a dental surveyor. A 30 g weight was attached to the head of the surveyor arm. With the addition of a micro-motor and handpiece weights and the spring tension of the surveyor, the net applied load during preparation was 50 g, which was measured using an electronic weight scale. Teeth were prepared only with this low load, which was applied to avoid the clogging that may stop slider movement and reduce bur advancement to maintain at least a 0.5 mm residual dentin thickness after completion of the preparation step.
For the rotary-cutting instruments, a new and unused medium-grit round-end tapered diamond bur (TF-13, Mani, Tochigi, Japan) was fitted in the handpiece to prepare each tooth. Then the tooth-linear slider table assembly was placed on the surveyor's platform with the long axis of the bur parallel to the facio-lingual tooth axes, and the entire cutting surface of the bur was engaged on the middle of the flat occlusal dentin surface. The assembly was placed in an incubator at (37°C ± 1°C). All thermocouples (the two pulp chamber thermocouples and the two handpiece thermocouples) were connected to a 4-channel digital thermometer (SD 947, REED Instruments, Wilmington, NC, USA) that had an auto datalogging function to measure temperature and time information.
Tooth preparation and temperature measurements
The 28 samples were assigned randomly into four groups with seven specimens each. The first group was the control group and did not use cooling water. The other three groups were prepared at different cooling water temperatures (10°C, 23°C, and 35°C; ± 2°C). The desired cooling water temperature was achieved by increasing or decreasing the water temperature in the self-contained water source until the chip water from 1.6 mm coolant water tube reached the desired temperatures. Each preparation consisted of one uninterrupted step for standardization, as follows: the slider motor was activated so the tooth moved under the handpiece 2 mm in each direction then the handpiece was used by fully depressing the foot pedal for 60 seconds at its full speed to start the tooth preparation. The temperature of both the pulp chamber and the handpiece head was recorded continually every 2 seconds by the thermometer during the whole tooth preparation interval. At the end of each cutting interval, the thermocouples where removed from the first specimen and inserted to the next specimen. The highest temperature (Tmax) and change in temperature (ΔT = change from baseline temperature to the highest or lowest temperature) for both the head of the handpiece and the pulp chamber were determined as the average of the temperature recorded from the two thermocouple readings for all 28 specimens in the four groups.
Statistical analysis
Data were analyzed using descriptive statistics and one-way multivariate analysis of variance (MANOVA) tests. Post hoc Tukey's test was used to determine statistically significant differences among groups. The level of significance was p < 0.05. The statistical analysis was performed with Statistical Package for the Social Sciences (SPSS) 20.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
Temperature versus time curve for pulp chamber and for an electric handpiece head are shown in Figures 3 and 4. Average change in temperature (∆T) and standard deviations for the groups are presented in Table 1. For groups without water cooling, the average temperature increase within the pulp chamber and at the handpiece head was 6.8°C and 11.0°C, respectively. When refrigerated cooling water (10°C) and room temperature water (23°C) were used, temperature decreased in the pulp chamber by 16.3°C and 8.6°C, respectively. For the handpiece head, the decreases were 10.2°C and 4.9°C, respectively. With the warm water (35°C), temperature increased slightly for the pulp chamber (1.6°C) and more substantially for the headpiece (6.7°C).
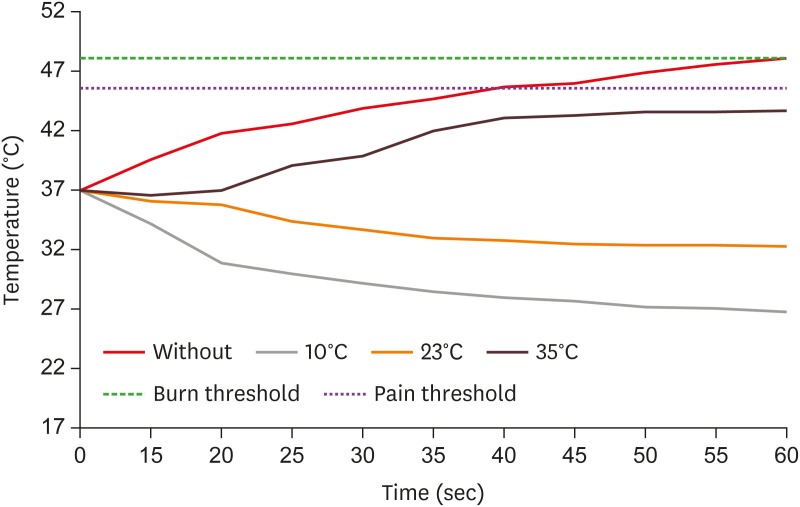
Temperature versus time curve at the handpiece head during teeth preparation for the 4 tested groups. The effect of different conditions of water cooling temperature is illustrated.
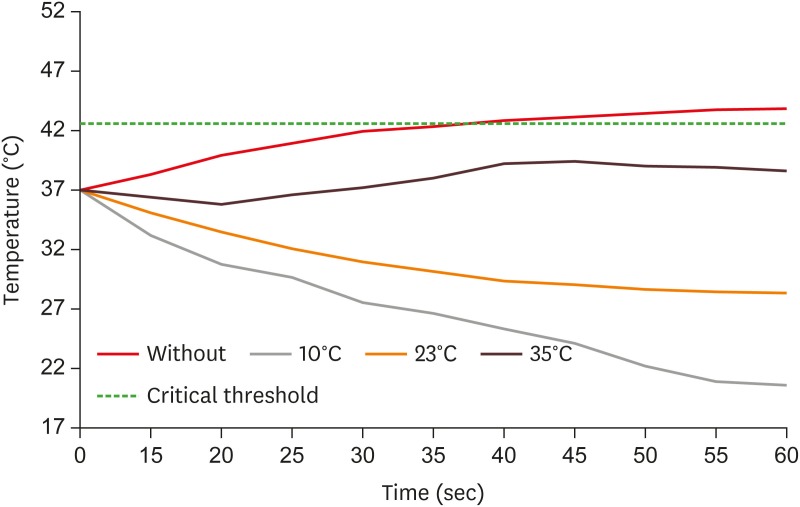
Temperature versus time curve in the pulp chamber during teeth preparation for the 4 tested groups. The effect of different conditions of water cooling temperature is illustrated.

Temperature changes (ΔT) in pulp chamber and handpiece head for the 4 test groups
One-way MANOVA was used to determine the effect of cooling water temperature on the temperature within the pulp chamber and at the handpiece head. The three groups with water cooling were used in the final statistical analysis, and no water group was eliminated from the final analysis because the variances between this group and the other three groups with water cooling for the dependent variable (ΔT in pulp chamber) were not equal as Levene's test was statistically significant p < 0.05. There were no univariate outliers in the data of the three groups with water cooling, as assessed by inspection of a boxplot. Data were normally distributed (Shapiro-Wilk test, p > 0.05), and there was homogeneity of variance-covariance matrices (Box's M test, p = 0.414) of equality of covariance matrices. The differences between cooling water temperatures on the combined dependent variables were statistically significant (F4,34 = 114.302, p < 0.001; Wilks' Λ = 0.005; partial η2 = 0.931). Follow-up univariate ANOVAs showed that both pulp chamber temperature (F2,18 = 569.125, p < 0.001; partial η2 = 0.984) and hand piece head temperature (F2,18 = 437.258, p < 0.001; partial η2 = 0.980) differed significantly among the different cooling water temperatures (Bonferroni adjusted, p < 0.025). The Tukey's post hoc test revealed that there were significant differences (p < 0.05) in the temperature changes in both pulp chamber and at the handpiece head among the three groups with different cooling temperatures (p < 0.001).
DISCUSSION
To assess the potential risk of pulp and soft tissue thermal injury, this study tested the effects of cooling water temperature on both the pulp chamber temperature and handpiece head temperature during tooth preparation using an electric motor handpiece system. Therefore, it is important to determine the critical temperature at which pulp and soft tissue injury may occur. An increase in pulp chamber temperature to 42.4°C has been considered by many previous reports as the critical threshold, above which, irreversible damage to the pulp may occur [20]. However, there are few reports in the dental literature that determined the critical threshold for thermal pain of oral soft tissue. Green reported a pain threshold for the most sensitive part of the oral-facial region (vermilion lip) at 45.6°C [21]. The American Dental Association (ADA), when evaluating the electric handpiece temperatures and the associated risk of burns, determined that serious soft tissue burns occurred if tissue contacted a heat source of 48°C for five minutes [18]. Therefore, 45.6°C was considered as the critical thermal threshold for heat pain and 48°C for burn in this study.
Consistent with other studies, this study used a custom-made apparatus to simulate intra-oral tooth preparation to ensure standardization and reproducibility of all variables that may affect the amount of heat generated and conducted to the pulp chamber and handpiece head surface during tooth preparation. These included the handpiece torque and speed, bur design and coarseness, bur contact area with tooth structure, speed of movement, load used during cavity preparation, and residual dentin thickness [582223].
When data from the control groups (no water cooling) was examined in light of critical thresholds, it was found that the average increase in pulp chamber temperature was 6.8°C, which was above the critical temperature for pulp. Furthermore, the average temperature of the handpiece head was 48°C, which would induce pain and could cause serious tissue damage if it contacted tissue for 5 minutes. These results emphasize the thermal risk of running an electric handpiece at its full speed without water cooling to both the pulp and oral soft tissue.
Cooling water had a significant effect on the temperature changes both in the pulp chamber and at the handpiece head. However, none of the three treatment groups with different water cooling temperature reached the harmful critical temperature limits for both the pulp chamber and handpiece head. The use of 10°C cooling water produced a significant decrease of the temperature in the pulp chamber and at the handpiece head compared to baseline temperatures. However, this low cooling water temperature had the highest heat absorption capacity, which kept both the pulp chamber and the head of the handpiece at their lowest temperature. Moreover, this low temperature resulted in the pulp chamber temperature falling below 21°C, which may lead to reductions in pulp blood flow that could affect the pulp's ability to clear toxins or waste products, increasing the risk of pulp injury [2425]. Furthermore, this refrigerated water may be uncomfortable to the patient's mouth and the operator's hand.
The use of room temperature cooling water was also effective at maintaining appropriate temperatures for the pulp chamber and the head of the handpiece. The decrease in pulp chamber temperature was 8.6°C, which was similar to the results from Ercoli et al. [17], where a decrease of the simulated pulp chamber temperature was between 6.6°C and 8°C. Furthermore, this finding is consistent with many previous reports that recommend the use of room temperature water at a rate of 25–50 mL/min to suppress increases in pulp chamber temperature even in extreme conditions [57]. A reduction in temperature at the head of the handpiece was also detected, which contradicts an ADA report of a 3.4°C increase in the head with the use of a similar electric handpiece system [18]. However, their study involved the use of slightly worn handpieces at higher load, and their experiment was conducted at ambient conditions and not in an incubator, which may have affected the results.
When 35°C cooling temperature was used, there was a slight increase in temperature in the pulp chamber temperature and at the electric handpiece head. However, these temperature changes present no significant risk for pulp thermal injury or soft tissue pain or burn. Theoretically, when the rate of cooling water is sufficiently high, the pulp should not exceed the cooling water temperature. However, in this and similar studies, the recorded pulp chamber temperatures were higher than the cooling water temperature when using an electric handpiece. This is due to the warming of cooling water when passing through the shaft of the hot handpiece. Lauer et al. [8] used a nearby cooling water temperature (32°C ± 2°C) in the electric handpiece and found a slight drop (0°C to 2.7°C) in pulp chamber temperature. That study used intermittent cutting with pause intervals, which allowed temperature to drop, and a lower torque of the micro-motor (2 N·cm), which was less than the torque used in our study. The rise in the temperature both in the pulp chamber and at the handpiece head in this study suggests that this warm cooling temperature provides borderline protection that may not be effective in extreme conditions with higher load, longer cutting time, and closer proximity to the pulp.
Finally, when preparing vital teeth in real clinical situations, numerous factors will lead to heat dissipation and reduce the damaging effects of heat on dental tissue. For example, the presence of high water content in vital pulp tissue, dynamic changes in pulp blood flow, the dentinal fluid flow, release of heat shock protein-70, and thermoregulatory defense mechanisms all can mitigate the high temperatures that were generated in our simulated experimental setup [252627]. Furthermore, some studies have reported that pulp can withstand intra-pulpal temperature increases up to 11°C without any clinical or histologic changes [28]. However, it is important to note that pulp tissue damage is cumulative, especially in crown preparation in fixed prosthodontics, where long procedures and large preparation areas can lead to pulpal inflammation and necrosis. In addition, succeeding insults such as large number of exposed dentinal tubules, desiccation, vibration, chemical irritation during impression making, provisional fabrication, and biological irritation due to microleakage during the provisionalization period may reduce the ability of the pulp to withstand and may induce pathologic changes when added with thermal injuries [25]. This is supported by reports that revealed a high percentage (18%–54%) of pulp necrosis in teeth following fixed dental prosthesis [2930]. Even though this study cannot replicate the complexities of actual biological systems and real clinical situations, results of this study highlight the importance of cooling water temperature during high-speed tooth preparation using an electric handpiece to prevent potential thermal injury, pain, and burns to both the pulp and oral soft tissues. Moreover, this study suggests the need for a water supply for the water system in a dental unit that originates from a temperature-controlled self-contained water reservoir or a dedicated temperature-controlled piped supply which are ideal for keeping the dental unit cooling water at room temperature.
CONCLUSIONS
Within the limitations of this study, the critical threshold for thermal injury for the pulp and soft tissue was always reached for the group without water cooling. On the other hand, none of the three groups of different water cooling temperatures (10°C, 23°C, and 35°C) reached the harmful critical temperature. However, when 35°C was used, there were an increase in both the temperatures in the pulp chamber and at the handpiece head, which may suggest borderline protection of this warm cooling water when using electric handpieces.
ACKNOWLEDGMENTS
The author gratefully acknowledge Qassim University, represented by the Deanship of Scientific Research, on the material support for this research under the number "dent-2016-1-12-s-1561" during the academic year 2016.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
