Oral manifestation and root canal therapy of the patient with mucopolysaccharidosis
Article information

Abstract
Mucopolysaccharidosis (MPS) is an inherited metabolic disorder caused by a deficiency in enzymes that participate in the degradation of glycosaminoglycans (GAGs) such as heparin sulfate and dermatan sulfate. Left untreated, patients show progressive mental and physical deterioration due to deposition of GAGs in organs. Death often occurs due to cardiac or respiratory failure before patients reach their early twenties. MPS has several oral and dental manifestations. An enlarged head, short neck, and open mouth associated with a large tongue are major characteristics of MPS patients. Dental complications can be severe, including unerupted dentition, dentigerous cyst-like follicles, malocclusions, condylar defects, and gingival hyperplasia. A 21-year-old female patient with MPS was described in this article, with special emphasis on oral manifestations and dental treatment.
INTRODUCTION
Mucopolysaccharidosis (MPS) is a heterogeneous innate disease induced by lysosomal storage of glycosaminoglycans (GAGs) characterized by the absence of enzymes responsible for breakdown of GAGs [1]. Progressive accumulation of GAGs such as dermatan sulfate and heparin sulfate in organs will lead to musculoskeletal abnormalities, joint stiffness, severe growth deficit, coarse facial features, mental retardation, and enlarged organs [234].
There are 7 distinct types of MPS: I (Hurler), II (Hunter), III (Sanfilippo), IV (Morquio), VI (Maroteaux-Lamy), VII (Sly), and IX (Natowicz). The incidence of MPS has been estimated to be ranging from 1:25,000 to 1:100,000 [56]. Children with MPS look nearly normal at birth. However, if untreated, they show gradual mental and physical deterioration. Death usually occurs before they reach their early twenties [7]. Usually, death is a result of either respiratory tract infection or cardiac valvular disease, a major systemic factor caused by deposition of mucopolysaccharides [8]. However, patients with mild forms have relatively normal life expectancy [9].
Oral and dental findings of MPS are characteristically present, making it important to know from clinical and radiographic findings. They include flattened alveolar ridges with hyperplastic gingiva, macroglossia, high-arched palate, and short mandibular rami with abnormal condyles. Peg-shaped teeth, delayed dental eruption, malocclusions, and localized dentigerous cyst-like radiolucencies are frequently observed [10111213].
Bone marrow transplantation is considered one of long-term therapies for inversing the deposition of excess GAGs in tissues. In this procedure, the patient's unhealthy bone marrow is destroyed by chemotherapy or radiotherapy ahead of the infusion of healthy marrow into the blood stream. Successful transplantation leads the new bone marrow to migrate to cavities of the large bone and engrafts to produce normal blood cells. Thereafter, hematopoietic-origin donor cells will help remove GAGs from host organs [14].
Hematopoietic stem-cell transplantation is a treatment with minimal or no central nervous syndrome damage for children diagnosed with MPS. Treatment can increase patient's life expectancy, resolve hepatosplenomegaly, stabilize cardiac disease, and improve airway disease, hearing, and range of motion of joints. Hematopoietic stem-cell transplantation can be as successful as bone marrow transplantation [15161718]. The present study aims to present oral health conditions and oral features of a patient with MPS and introduce dental treatment procedure.
CASE REPORT
A 21-year-old female attended the Department of Conservative Dentistry, Chonnam National University Dental Hospital, Gwangju, Republic of Korea. She was referred from the Department of Oral and Maxillofacial Surgery for evaluation and the treatment of the tooth #45. All diagnosis and treatment procedures were conducted following informed consent. She was a type I MPS patient with mitral and aortic regurgitation. Her sisters were also MPS patients. First, she visited the Department of Oral and Maxillofacial Surgery and complained ectopic eruption of tooth #15 and tooth #25. She wanted to extract both teeth. In panographic radiograph findings, supernumerary tooth between the root of tooth #21 and tooth #22, abnormal mandibular condyles, and shortened ramus were identified (Figure 1A).
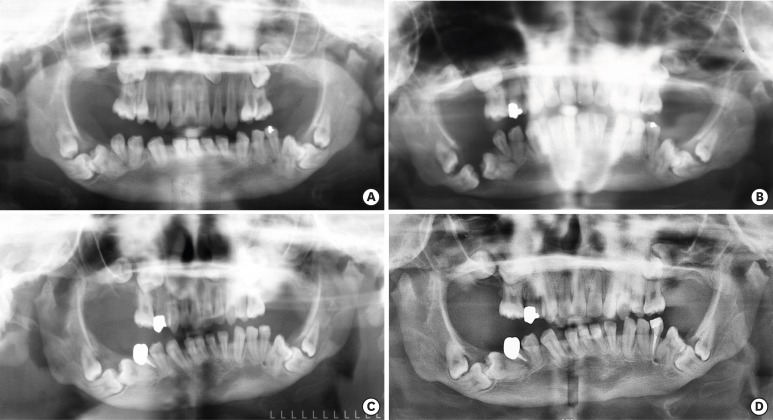
A preoperative panoramic view (A). A panoramic view of 2nd visit (B). A panoramic view after marsupialization of dentigerous cyst on teeth #46 and #47 (C). A panoramic view after 6 years of marsupialization on teeth #46 and #47 (D).
After 1 year, she came back because of swelling and pain on the lower right jaw. In clinical examination, swelling and fluctuation on buccal gingiva of tooth #46 area were observed. Destruction of alveolar ridge was identified on area of both unerupted upper and lower posterior teeth (Figure 1B). The patient was diagnosed with dentigerous cyst on tooth #46 and tooth #47. Thus, marsupialization was done (Figure 1C) and periodic examination was performed for 6 years (Figure 1D).
After another year, she complained pain of the tooth #35 and tooth #45. Spacing, severe labioversion, and gingival inflammation on both tooth #35 and tooth #45 were observed (Figure 2). Responses to Electric pulp test and cold test were positive. The tooth #45 was decayed. It was sensitive to percussion with slight mobility (Figure 3A). The tooth #45 was diagnosed with caries of dentin. Thus, caries removal and resin filling were planned. Before the next appointment, the patient suffered from severe spontaneous pain on tooth #45. It was diagnosed with irreversible pulpitis, and conventional root canal treatment was performed. Under rubber dam isolation, the access opening was prepared. The pulp tissue was extirpated and the working length was determined using an electronic apex locator (DentaPort ZX, J Morita Corp., Osaka, Japan) with periapical radiograph (Figure 3B). Nickel-titanium rotary instrument (ProTaper universial, Dentsply Tulsa Dental, Tulsa, OK, USA) with crown-down technique was used for instrumentation. The canal was enlarged to size F2. During instrumentation, the canal was irrigated copiously with 5.25% sodium hypochlorite solution and sterile saline. Sterile paper points were used to dry the canal and intracanal medication with calcium hydroxide was applied. The access cavity was temporarily sealed with Caviton (GC, Tokyo, Japan). After 2 weeks, the pain disappeared, and the canal was obturated with gutta-percha and AH26 plus sealer (Dentsply DeTrey, Konstanz, Germany) using a continuous wave technique (Figure 3C). Crown restoration was performed (Figure 3D). Tooth #35 treated with amalgam previously showed positive percussion sensibility, uncomplicated crown fracture, and secondary caries. For tooth #35, fractured amalgam and caries were removed and composite resin restoration was done (Figure 3E).

A preoperative clinical photograph.
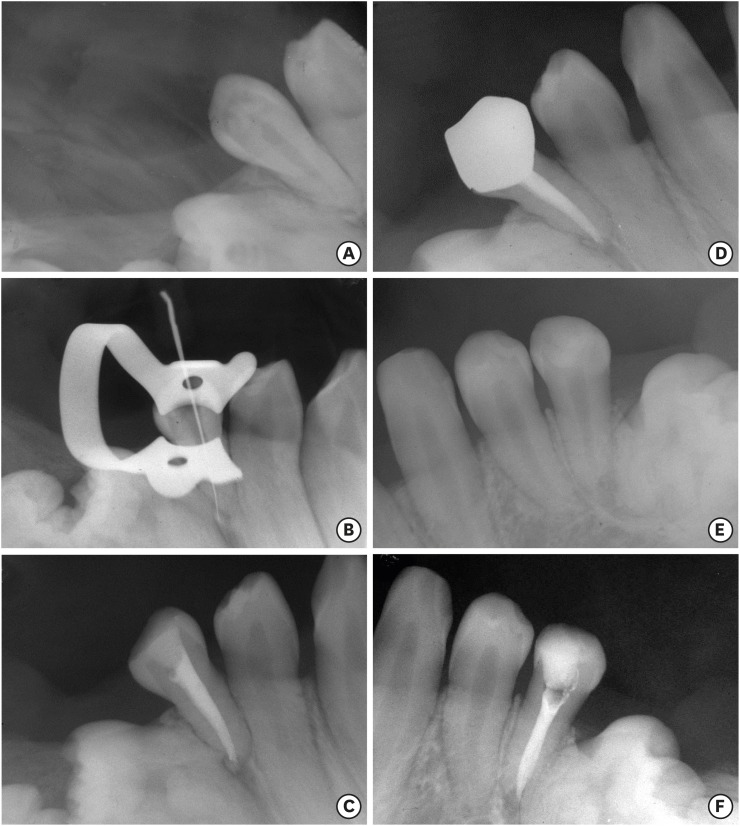
A preoperative radiograph of the tooth #45 (A). A radiograph of the tooth #45 with initial apical file (B). A radiograph of the tooth #45 after filling (C). One year and 5 months follow-up radiograph of the tooth #45 (D). A preoperative radiograph of the tooth #35 (E). A radiograph of the tooth #35 after filling (F).
On 1-year follow-up, the patient felt spontaneous pain on tooth #35 again. Conventional root canal treatment was performed as describe previously (Figure 3F). In following check-ups, no symptoms were identified.
DISCUSSION
MPS and other diseases can be distinguished by oral findings. Multiple rosettes in the cavity of dental follicles found in radiographic images are conditions suggesting differential diagnosis of MPS [19] in relation to Gorlin's syndrome [2021] which presents several cystic lesions in upper and lower maxillas as well as permanent and supernumerary teeth inserted into alveolar bones [20]. Progressive accumulation of mucopolysaccharides in the soft tissues causes systemic complications such as cardiac failure and bronchopneumonia, resulting in the death of MPS patients before twenties [22].
In case of dental treatment with MPS patient, there are many consideration factors. First, degree of mental retardation should be considered. In the present case, the patient had slight mental retardation. However, she had no difficulty in communication. Second, the presence of a seizure disorder should be considered. For the treatment of this patient, we used rubber dam in all cases to prevent aspiration, and prepared an oxygen tank and mouth prop. The patient in the present study showed no significant seizure disorder. Third, joint stiffness should be considered. The patient moved with wheelchair because of restriction of knee joint’s extension, making it difficult to take x-rays. Sedation and general anesthesia during dental treatment should also be considered. In case of MPS, accumulation of mucopolysaccharides in the tunica intima of coronary arteries and heart valves contributes to cardiac valve disease [23]. The patient in this case had mitral regurgitation and aortic regurgitation. As a high-risk group patient of infective endocarditis, the patient took Amoxicillin 2.0 g as an antimicrobial prophylaxis one hour before the treatment. Due to mouth opening limitation caused by abnormal condyle, it was difficult to take x-ray pictures or clinical photographs, and instrumentation was hard to be done as well. In addition, the cumulation of GAG causes labioversioned teeth. Therefore, cautions should be made during access opening or crown preparation.
There is little information on dental treatment guidelines for patients with MPS. In the literature, a preventive care protocol including pit and fissure sealant, fluoride application, tooth brushing instruction, and diet counseling should be conducted based on patient’s needs. Regular visit to the clinic for check-up is necessary [24].
CONCLUSIONS
Patients with MPS show prevalence of clinical oral manifestations such as delayed eruption/retention of teeth, thickness of alveolar process, thick lip, peg-shaped teeth, and also prevalence of radiographic oral manifestations such as condylar defect, short mandibular ramus, dentigerous cyst-like radiolucencies, and delayed eruption of teeth. Understanding these typical oral manifestations of MPS patients can help clinicians set up differential diagnosis, early treatment intervention, prevention, and education of both patients and parents or caregivers. Although MPS is not encountered routinely in dental practice, MPS patients can maintain their oral and general health for the remainder of their lives if they are properly managed.
Notes
Funding: This study was supported by a grant (CRI 18029-1) of Chonnam National University Hospital Biomedical Research Institute and a grant (2016R1C1B1012703) of the National Research Foundation of Korea (NRF) funded by Ministry of Science, ICT and Future Planning (MSIP), Republic of Korea.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Oh WM.
Data curation: Yoon JH, Lee HI.
Formal analysis: Lee BN.
Funding acquisition: Lee BN.
Investigation: Choi SH.
Methodology: Chang HS.
Project administration: Hwang YC.
Resources: Hwang IN.
Software: Yoon JH, Lee BN.
Supervision: Oh WM, Lee BN.
Validation: Jang JH.
Visualization: Yoon JH, Lee HI.
Writing - original draft: Yoon JH, Lee HI.
Writing - review & editing: Lee BN, Oh WM.