A simple technique for impression taking of teeth and functionally generated paths
Article information
Abstract
The objective of this case report is to introduce a simple technique for simultaneously taking a closed-mouth impression and functionally generated path (FGP) for a full coverage crown restoration. A monolithic zirconia crown was the restoration of choice. An alginate impression of the abutment tooth was taken to fabricate a custom-made closed-mouth impression tray covering the abutment tooth and the adjacent teeth. The tray had an FGP table and an abutment tray in cameo and intaglio surfaces, respectively. The impression was taken with silicone impression material after adjusting the abutment tray and inscribing the FGP using self-curing acrylic resins. Plaster casts were made from the impression, and a zirconia crown was fabricated. The crown was cemented to the abutment tooth with minimal adjustments. This simple technique resulted in a well-fitting crown that accounted for mandibular movements. Using the custom closed-mouth impression tray incorporating an FGP table simultaneously aids in fabricating an accurately fitting restoration that incorporates harmonious mandibular movements using a single impression capture.
INTRODUCTION
Impression taking is an indispensable process in the fabrication of indirect restorations. The conventional technique requires 3 impressions, i.e., the prepared tooth, the opposing arch or quadrant, and the occlusal registration if required. Teeth move when occluded because of the periodontal ligaments deformation by the occlusal forces. Therefore, there is a difference between intra-oral occlusal contacts and the contacts on gypsum casts made by the conventional technique. Closed-mouth impression technique was reported to minimize the difference by capturing the information in one impression [12].
Studies have shown that the use of a custom tray for making impression provides a good fit of the restoration to the abutment. The custom tray minimizes the impression material volume which in turn polymerizes more uniformly, leading to the better accuracy of the impression [34].
Tooth restorations need to have anatomically and functionally proper shape. Functionally generated path (FGP) technique that records mandibular movement is an effective way to fabricate restorations possessing appropriate function [5].
The objective of this case report was to introduce a simple impression technique for tooth restoration that is capable of achieving the advantages of closed-mouth impression, custom abutment tray, and FGP technique simultaneously.
CASE REPORTS
The patient was 28-year-old male with a chief complaint of poor esthetics of a metal crown in tooth #46. Teeth #46 and #47 were guiding teeth for the mandibular lateral movements. The patient expected a tooth-colored restoration for the tooth. Four kinds of restorative materials were explained, which were porcelain, resin composite, lithium disilicate, and zirconia. Among them, porcelain and resin composite were likely to induce excessive wear in the opposing enamel or in itself. Comparing lithium disilicate to zirconia, the latter was more suitable for the restoration because the tooth was the guiding tooth [6]. A monolithic zirconia crown was selected as the replacement restoration, accordingly. After preparing the tooth (Figure 1A), impressions were taken using an alginate impression material (Aroma fine Plus, GC International, Tokyo, Japan) to make gypsum casts of the upper and lower teeth using a model stone (ISO Type 3, New Plastone II, GC International). A customized closed-mouth impression tray was made on the cast using a self-curing acrylic resin (Figure 1B and 1C, Unifast Lab, GC International). The tray was designed to include and adapt on the adjacent teeth for stabilization and to have a flat top (circled by yellow dashed line in Figure 1B) as an FGP table. The tray had a custom tray for abutment in the opposite side of the table (Figure 1C). After adjusting the abutment custom tray using a self-curing acrylic resin, the tray was verified to be stable, to be smoothly inserted and removed, and not to interfere in centric and eccentric mandibular movements (Figure 1D).
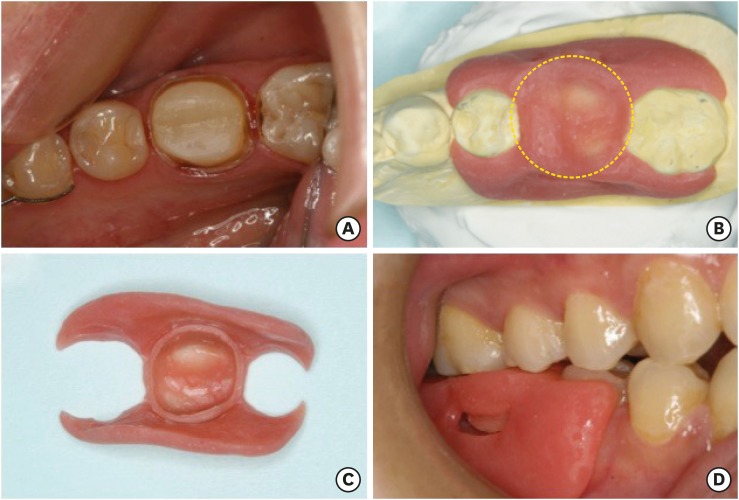
(A) Occlusal view of tooth #46 prepared for monolithic zirconia crown. (B) Customized closed-mouth tray made on the gypsum cast. Flat part circled is functionally generated path (FGP) table. (C) The tray has an individual tray for abutment tooth in the opposite side of the table. (D) Adjusting the tray so that it does not interfere in the mandibular movements.
A self-curing acrylic resin (Pattern Resin, GC International) was put on the FGP table, and the custom tray was placed on the prepared teeth. FGP was carved into the resin as it was setting by letting the patient move their mandible in protrusive, retrusive and lateral directions (Figure 2A). FGP record is shown in Figure 2B. An adhesive for impression material was applied to the tray except the surface of FGP record. The closed-mouth impression was taken using addition silicone impression material (Figure 2C, Imprinsis, Tokuyama Dental, Tokyo, Japan), which recorded the teeth position under occlusal force. The impression of the prepared side is shown in Figure 2D.
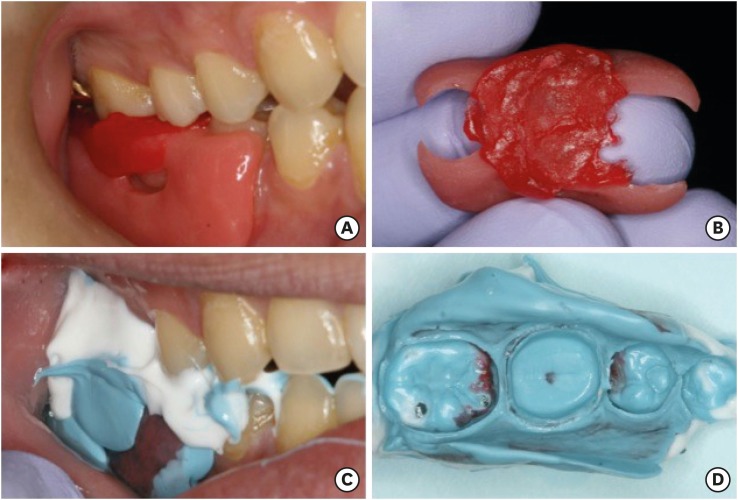
(A) Self-curing resin was put on the table and functionally generated path (FGP) was carved into the resin. (B) Recorded FGP. (C) Impression was taken using addition silicone impression material. (D) Impression of the abutment and adjacent teeth.
From the impression above, 3 casts were generated: a working cast (Figure 3A), an opposing dentition cast (Figure 3B), and the FGP functional core cast (Figure 3C). The plasters used were a die stone (ISO Type 4, New Fujirock IMP, GC International) for the working cast and the FGP cast, and a model stone (New Plastone II, GC International) for the opposing cast. The 3 casts were mounted to an articulator such as a twin stage occluder. Other hinge articulators whose bows include magnets for easier mounting/removal of casts, are also applicable instead of the twin stage occluder. The hinge articulator was used in this case. Procedure of the mounting was: 1) the plasters were poured into the impressions for the working and the opposing casts, 2) the working and the opposing casts were mounted on the lower and the upper bows, respectively, while keeping the casts in the impression, 3) the opposing cast was removed from the impression, and the impression material covering the FGP record was cut out, 4) the plaster was poured only on the record to obtain the FGP core, and 5) the core was mounted to the other upper bow of the twin stage occluder or with another attachment for the magnetic mounting. A wax pattern of the crown was conventionally fabricated on the model. Contour of the pattern was roughly carved with the normal opposing cast (Figure 3B), and occlusal contacts, in particular eccentric contacts, were adjusted with the FGP core. The pattern was scanned and a monolithic zirconia crown was fabricated according to the manufacturer's instructions (Figure 3D, Katana, Kuraray Noritake Dental, Tokyo, Japan) at an in-hospital dental laboratory of Tsurumi University Dental Hospital.
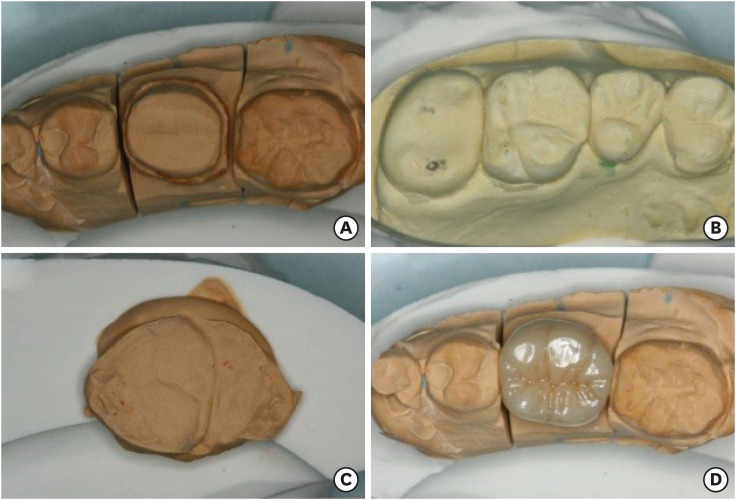
(A) Working cast made from the impression. (B) Opposing dentition cast. (C) Functionally generated path (FGP) functional core. (D) Monolithic zirconia crown.
The crown fitted the abutment well without the proximal contact adjustments (Figure 4A and 4B). Figure 4A demonstrates occlusal contacts at initial placement before occlusal adjustment. Red and blue points indicate centric and eccentric contacts, respectively. The contacts were verified on both teeth #46 and #47. The eccentric contacts were applied in the artificial facets of the crown. Following minimal occlusal adjustment, the crown was cemented to the abutment using a resin cement containing an adhesive monomer, 10-methacryloyloxydecyl phosphate (Figure 4C, Panavia V5, Kuraray Noritake Dental).
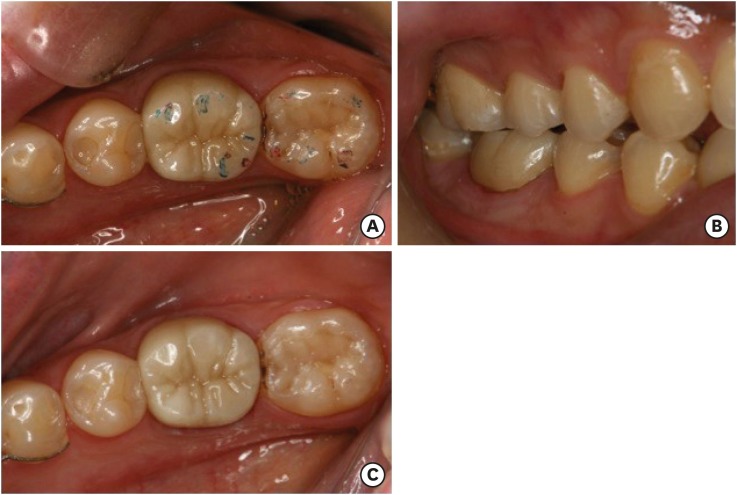
(A) State of occlusion at initial placement. Red, centric contact; Blue, eccentric contact. (B) Buccal view of the crown. (C) The crown as cemented using a resin composite cement containing 10-methacryloyloxydecyl dihydrogen phosphate (MDP).
DISCUSSION
Recently, digital impression techniques are gaining popularity in dental practices owing to advances in CAD/CAM technology. None of the CAD/CAM systems, however, offers digital recording of mandibular movement that can be applied to crown fabrication in a sophisticated manner. The design software algorithm doesn't differentiate between group function and mutually protected occlusion and therefore cannot be manipulated when the patient has an unusual occlusion. We believe FGP technique is still a simple and predictable method for recording mandibular movements. The technique presented here is surely suitable for restoring the guiding teeth in a group function situation.
Another advantage of this technique, compared to the conventional closed-mouth impression using a dual-arch tray, is that the modified custom tray supplies a more accurate occlusal registration because the custom tray does not have the intermediate mesh between the upper and lower dentitions. Contrarily, disadvantage of this technique compared to the conventional CAD/CAM procedures, is the total number of steps in chair-side and laboratory procedures. This technique includes more steps of impression taking, plaster-modeling, and mounting of models than the CAD/CAM restorations, which may indicate more occasions to make errors.
Intra-oral scanning seems to be well accepted by patients compared to conventional impression methods in terms of the amount of discomfort [4]. In the future, a combination of an FGP record and intra-oral scanning could contribute to an improvement in occlusal details of full coverage restorations requiring little or no adjustments especially in situation where the teeth are guiding teeth in group function or when the patient has some occlusal disharmony.
CONCLUSIONS
A customized closed-mouth impression tray with FGP table fulfills the fabrication requirement of restorations that are in harmony with the patient's mandibular movements with a single impression technique.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Abe M.
Methodology: Yamamoto T, Sato Y, Abe M, Ohkubo C.
Supervision: Watanabe H, Punj A, Momoi Y, Ohkubo C.
Writing - original draft: Yamamoto T, Sato Y.
Writing - review & editing: Watanabe H, Punj A, Abe M, Momoi Y, Ohkubo C.