Endodontic management of central incisor associated with large periapical lesion and fused supernumerary root: a conservative approach
Article information

Abstract
Fusion and gemination are developmental anomalies of teeth that may require endodontic treatment. Fusion may cause various clinical problems related to esthetics, tooth spacing, and other periodontal complications. Additional diagnostic tools are required for the diagnosis and the treatment planning of fused tooth. The present case report describes a case of unilateral fusion of a supernumerary root to an upper permanent central incisor with large periapical lesion in which a conservative approach was used without extraction of supernumerary tooth and obturated with mineral trioxide aggregate to reach a favorable outcome.
INTRODUCTION
Developmental tooth anomalies are deviation from the normal appearance in color, shape, size and number of teeth. The anomaly of conjoined teeth ‘Connate’ was one of the first introduced terminologies by J. Tomes (1859) [1]. De Jonge (1955) proposed the terms ‘Synodontia’ for those formed by the inability of adjacent tooth germs to retain their individuality and ‘Schizodontia’ to describe teeth, which originate by partial division of tooth germ [2]. The term double teeth was suggested by Miles (1954) [1]. Tooth fusion or syndontia is defined as a union of 2 or more separately developing tooth germ yielding a single large tooth during osteogenesis before mineralization of crown [3]. Gemination occurs when the tooth bud of single tooth attempts to divide. The incidence of these anomalies is very rare: 0.1% in permanent and 0.5% in primary dentition [4567]. The union of a supernumerary tooth and a normal tooth is referred to as diphyodontic gemination [8]. Etiology for this anomaly is still unknown but the authors suggested that it may be caused by the influence of pressure of physical forces producing close contact [9], necrosis of intervening tissue between 2 close tooth germs [10], and genetic determination [11]. Other investigators considered a viral infection, use of thalidomide during pregnancy and hypervitaminosis A as a possible cause of the anomaly [1213]. Injuries to primary teeth also cause 12%–74% developmental disturbances in permanent teeth [14]. Incidence of union in permanent teeth is 2.9% when there is fusion in primary teeth [15]. Fusion may also be associated with some syndromes such as Wolf-Hirschhorn syndrome, osteopetrosis, achondroplasia, focal dermal hypoplasia, and chondroectodermal dysplasia [16].
Fusion may be partial or total depending on the stage of tooth development and calcification at the time of union [9]. The number of root canals also corresponds to this stage of union. If the contact occurs before the calcification stage, the teeth unite completely and form one large tooth. Incomplete fusion may be formed at root level if the contact and union occur after calcification of crown. In anterior region, fused teeth are esthetically unpleasant and may cause functional limitations. If such teeth show endodontic involvement, their treatment becomes a challenge to the clinician. In dental literature, various treatment considerations for fused teeth have been recommended. Conventional intraoral periapical radiographs are the most important diagnostic tool for assessing the root configurations. However, it is difficult to understand the complicated morphology of fused teeth. In such cases newer diagnostic tools like cone-beam computed tomography (CBCT) play an important role by producing three dimensional images.
The present case report describes the endodontic management of upper central incisor fused with supernumerary root by using CBCT as a diagnostic aid.
CASE REPORT
A 20-year-old male patient who complained of pain in upper anterior region since 15 days ago was reported to Department of Conservative Dentistry and Endodontics, VSPM’s Dental College and Research Center. Patient gave a history of dull intermittent pain on upper left central incisor (tooth #21) which had undergone a root canal treatment 7 days ago. Clinical examination revealed that tooth was normal in size and shape with slight discoloration and healthy periodontium (Figure 1A). Access cavity was seen in tooth #21 with distal cavity and labial perforation extending subgingivally (Figure 1B). The tooth was not sensitive to percussion. Patient's medical history was non-contributory. A preoperative intraoral periapical radiograph revealed a large periapical lesion on tooth #21 and a prepared access cavity (Figure 1C). Overlapping radiopacity was seen with the root of tooth #21. Because of this aberrant anatomy, CBCT was taken. CBCT images showed the presence of an extra root fused with the root of tooth #21 below the cervical line continuing till the apex (Figure 2). From clinical and radiograph findings, diagnosis of previously initiated root canal treatment with chronic apical periodontitis was made on tooth #21. Root canal treatment was planned for both roots. It was decided to treat the 2 canals separately. Root canal of tooth #21 was treated via the main access cavity and the root canal of supernumerary root was treated after elevation of full thickness periodontal flap. Treatment plan was explained to the patient and informed consent was taken.
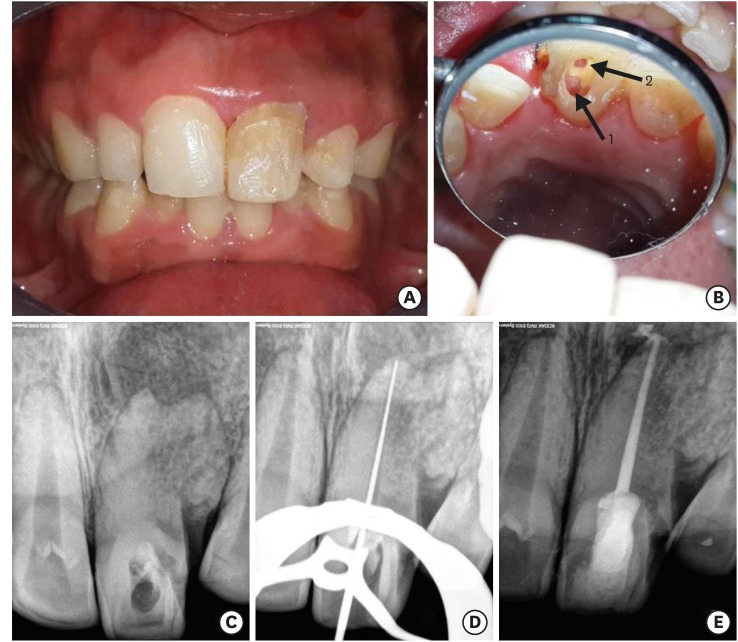
(A) Initial clinical photograph shows discoloration of tooth #21. (B) Canal orifice (1) and labial perforation area extended subgingivally (2) (C) Intraoral radiograph of tooth #21 with periapical lesion and lateral radiopaque shadow. (D) Working length determination radiograph. (E) Post-obturation radiograph of tooth #21.
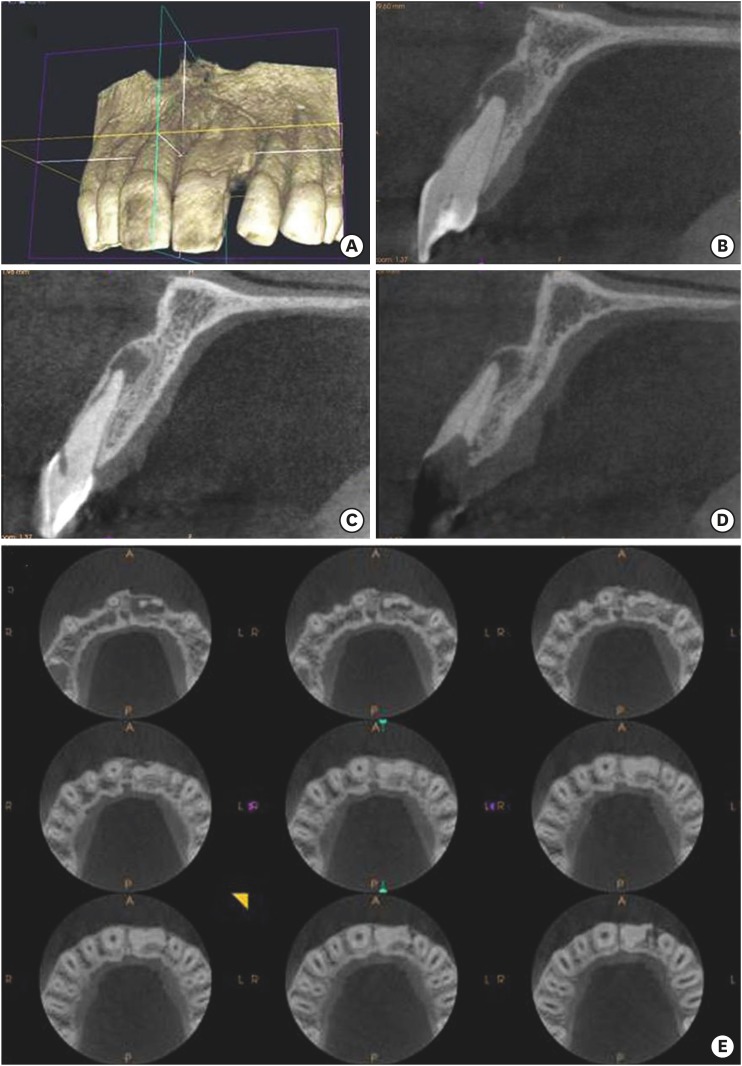
CBCT images showed the presence of extra root fused with the root of tooth #21 bellow cervical line continuing till the apex. (B) Periapical lesion of tooth #21. (C) Perforation area extended to labial surface. (D) Presence of canal in supernumerary root.
Upper left central incisor was isolated with rubber dam and access cavity was refined. Patency of the main canal was checked with ISO size 15 K-file. The working length was determined with an apex locator (Root ZX, Morita, Tokyo, Japan) and confirmed with working length radiograph (Figure 1D). Cleaning and shaping were performed using nickel titanium (NiTi) rotary ProTaper files (Dentsply Maillefer, Konstanz, Germany) with crown down technique. Canal was enlarged with ProTaper F3 file. Root canal was frequently irrigated with 5.25% sodium hypochlorite (Prime Dental Products, Thane, India), normal saline, 17% ethylene diamine tetraacetic acid (EDTA, Pulpdent Corporation, Watertown, MA, USA), and 2% chlorhexidine gluconate (Endo-CHX, Prime Dental Product, Thane, India) as the final irrigant. Canal was dried with absorbent points (Dentsply Maillefer). Calcium hydroxide (RC Cal, Prime Dental Products) intracanal medicament was placed and the access cavity and distal perforation area of crown was sealed with intermediate restorative material (IRM) cement (Dentsply DeTrey GmbH, Konstanz, Germany). Patient was recalled after 3 weeks. At the second appointment, IRM cement was removed and canal was irrigated with normal saline, 17% EDTA, and Endo-CHX. Canal was dried with absorbent paper points (Dentsply Maillefer) and obturated with the single cone technique using the corresponding gutta-percha point (Dentsply Maillefer) and AH-Plus sealer (Dentsply Maillefer, Figure 1E). The access cavity was sealed with resin modified glass ionomer cement (GC Fuji PLUS, GC Corporation, Tokyo, Japan). Tooth was anesthetized with 1.8 mL 2% Lignocaine (LOX 2%, Neon Laboratories Ltd., East Mumbai, India) in the same appointment for the sealing of labial perforation and root canal treatment of supernumerary root. A full thickness periodontal buccal flap was raised. Perforation area was identified on labial surface of main root and canal was located in supernumerary root (Figure 3A and 3B). The working length was determined with an apex locator (Root ZX, Morita). Canal was enlarged with a ProTaper F2 file and frequently irrigated with normal saline, and Endo-CHX as the final irrigant. Canal was dried with absorbent paper points (Dentsply Maillefer) and obturated apico-coronally with MTA (ProRoot MTA, Dentsply India Pvt Ltd., Mumbai, India, Figures 3C and 4A). Labial perforation present on upper central incisor was also sealed with MTA (Figure 3C). Distal cavity was sealed with resin modified glass ionomer cement (GC Fuji PLUS, GC Corporation, Figure 3D). Flap was repositioned with sutures and patient was recalled after seven days for suture removal. Patient had started orthodontic treatment for protrusion of anterior teeth. After 1 year follow-up, healing of periapical lesion was seen with normal color and consistency of gingival tissue (Figure 4B and 4C). Periodontal pocket was within the normal range with tooth #21. Slight discoloration was present with tooth #21. Thus, the patient was advised to have full coverage porcelain crown on tooth #21 after completion of orthodontic treatment.
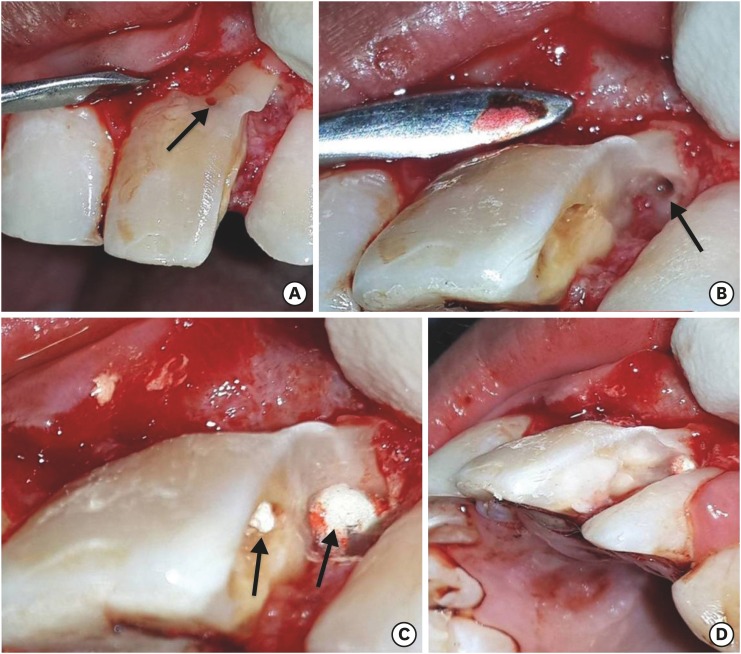
(A) Perforation area was identified on labial surface after flap reflection. (B) Canal found in supernumerary root. (C) Sealed labial perforation area (arrow) and obturated supernumerary root canal with MTA (arrow). (D) Distal access cavity was sealed with resin modified glass ionomer cement.
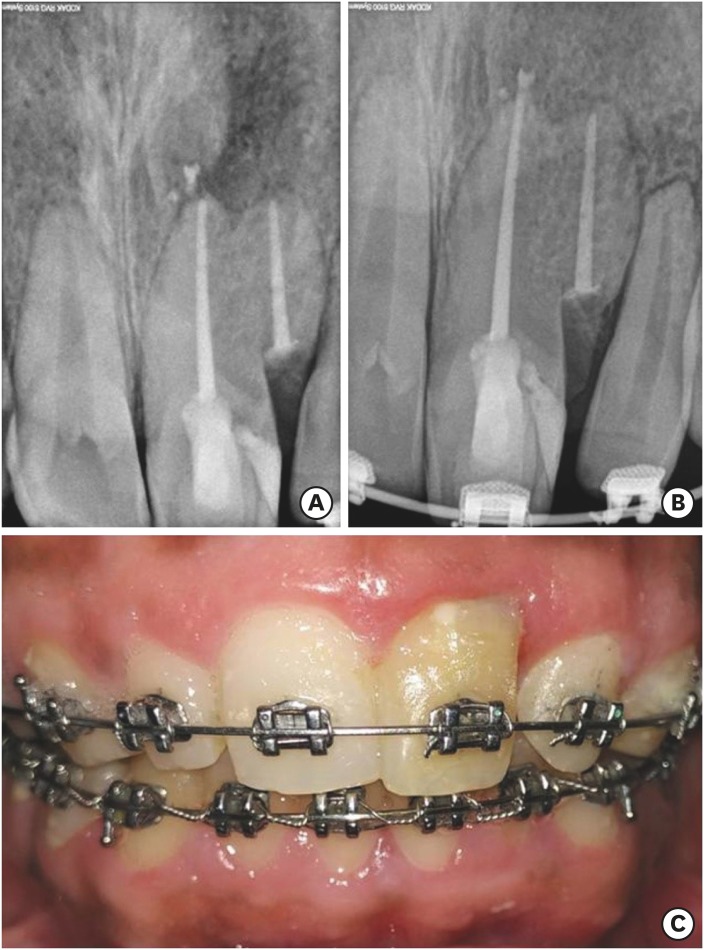
(A) Post treatment radiograph. (B) One year follow-up radiograph. (C) One year follow-up clinical photograph.
DISCUSSION
Clinically fusion and gemination are difficult to differentiate, and it is common to refer these anomalies as ‘double teeth’ [17]. Differential diagnosis of gemination and fusion can be possible on the basis of number of teeth present in the arch. Gemination shows normal number of teeth while fusion shows less number of teeth unless fusion occurs with supernumerary tooth [1518]. An exception to this rule is a union between normal and supernumerary tooth germ, congenitally missing tooth, fusion and gemination occurs concurrently, and history of extraction and exfoliation [15]. In the present case it was fusion of central incisor with a supernumerary root.
Dental fusion is more common in primary dentition than in permanent. Fusion occurs particularly in incisors and canines. Incidence of fusion in permanent and supernumerary teeth is 0.1% and unilateral incidence is 0.5% in primary dentition while 0.1% in permanent dentition [19202122]. The prevalence of double primary teeth is 1.55% to 3.0% in Asian children while in permanent teeth the frequency varied from 0.2% to 0.72% [15]. The frequency of fused teeth ranges from 0.1% to 0.85% and gemination of 0.08% to 2.5% [15].
Fusion with normal tooth germ causes diastema and fusion with supernumerary tooth germ causes crowding. Both these conditions cause esthetic problems, malocclusion, periodontal and periapical lesions. Treatment options available for the treatment of fusion are extraction, separation in two single teeth, and extraction of one half, auto transplantation after hemisection and reshaping of crown [23242526]. These treatment options depend on several factors, such as the type of abnormalities, the location of the connecting area, root development, patient age and compliance, and the pulp chamber and canal morphology. Morphology of fused teeth varies greatly so the treatment must be planned on an individual basis.
In fused teeth when the supernumerary tooth or both teeth have pulpal pathology only nonsurgical root canal is the choice of treatment. If the fusion is causing esthetic problem, the supernumerary tooth may be surgically removed as far as the level of fusion permits. Although this may be a feasible option in some cases, the long-term periodontal prognosis may be guarded [21]. In the case of fusion to decide most favorable treatment plan additional diagnostic tools are required along with intraoral periapical radiograph. The newer 3-dimensional system, CBCT imaging, was introduced to endodontics in 1990 [27]. CBCT becoming the powerful tool in the dental diagnosis and provide valuable information [282930]. In the present case CBCT scan revealed the supernumerary root was completely fused with the root central incisor from coronal third to apically. Surgical removal of this supernumerary root may cause more bone destruction and post-operative periodontal pocket formation so only root canal treatment with both the root was decided. Supernumerary root has remained as submerged root after treatment. Bjorn was the first person to publish a report of root submersions [31]. In 1960 Helsham in a survey of 2,000 patients with retained roots found that 1,676 patients were without symptoms or pathosis [32]. Rodd et al. [33] reported a 90% clinical success rate among 29 nonvital and 24 vital permanent incisor roots after more than 2 years of follow up, that were intentionally retained following a crown-root fracture. A submerged root underneath an old three-unit fixed dental prosthesis preserved the surrounding periodontium for 5 years without any periapical pathology [34]. Reames et al. [35] in their study concluded that bone will form coronal to amputated endodontically treated roots.
Root canal of supernumerary root was obturated completely with MTA as the root was below the alveolar crest and completely covered by gingival tissue. MTA has the potential to provide an effective seal, even in the presence of blood and moisture [3637]. The pH of MTA increased from 10 to 12.5 three hours after mixing. At this high pH calcium released from MTA reacts with phosphate in tissue fluid to form hydroxyapatite providing favorable sealing and biocompatibility [3738]. When used as root end filling material, MTA support the healing of periapical lesion and regeneration of periradicular periodontium [39]. Fresh as well as set MTA both caused cementum deposition when used after apical surgery [40]. In the present case 1 year follow-up radiograph showed the healing of periapical lesion showing favorable outcome to conservative treatment of fused roots.
CONCLUSION
Complexities of fused supernumerary teeth make it challenging for the clinician to deliver better treatment outcome. The clinician should be cautious of every detail of fusion including type and position of supernumerary tooth and its potential effect on adjacent tooth. CBCT helped in revealing complex tooth anatomy and level of fusion of supernumerary tooth which was not visible in radiograph. It hence paved a way for conservative treatment free of endodontic mishaps. As the mishaps could cause permanent damage and tooth loss. Newer biomimetic materials like MTA have most favorable outcome in periapical healing.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Badole GP.
Data curation: Badole GP, Parlikar A.
Formal analysis: Badole GP, Parlikar A.
Investigation: Shenoi PR, Badole GP, Parlikar A.
Methodology: Shenoi PR, Badole GP, Parlikar A.
Project administration: Shenoi PR.
Supervision: Shenoi PR, Badole GP.
Validation: Shenoi PR, Badole GP.
Writing - original draft: Badole GP.
Writing - review & editing: Shenoi PR, Badole GP, Parlikar A.