Periodontal healing following non-surgical repair of an old perforation with pocket formation and oral communication
Article information

Abstract
Iatrogenic perforations negatively impact the outcome of endodontic treatments. Studies on prognostic factors showed that perforations in the coronal third of the root with periodontal pocket formation have an unfavorable prognosis. A 36-year-old female was referred for endodontic evaluation of tooth #13 with a history of an iatrogenic perforation, happened 3 years ago. There was a sinus tract associated with perforation, 10 mm probing on the mesial and mesio-palatal, bleeding on probing, radiolucent lesion adjacent to the perforation and complete resorption of the interdental bone between teeth #13 and #12. After the treatment options were discussed, she chose to save the tooth. The tooth was accessed under rubber dam isolation, the perforation site was cleaned and disinfected using 0.5% sodium hypochlorite and sealed with calcium-enriched mixture cement. Eighteen months after treatment the tooth was functional and asymptomatic. The probing depths were normal without bleeding on probing. Radiographically, the interdental crestal bone formed between teeth #13 and #12. Despite all negative prognostic factors in this case (i.e., perforations in the coronal third, pocket formation, and radiolucent lesion), healing was unexpectedly achieved via non-surgical repair of the perforation. Further research on biological aspects of healing in the periodontium following iatrogenic perforations are recommended.
INTRODUCTION
Root perforation is defined as an iatrogenic or pathological communication between root canal system and the external tooth/root surface. Iatrogenic root perforations mainly occur during root canal treatment or restoration of the root canal treated teeth. A study on 5,048 root canal treated teeth showed a prevalence of approximately 2.3% for root perforations [1]. The incidence of root perforations during root canal treatments were predicted to be 2%–12% [2]. Despite these low figures, perforations have detrimental effects on the outcome of root canal treatments. Presence of pre-operative perforations was correlated with increased failure rate in non-surgical retreatment procedures [3]. In other words, root perforations are negative predictors for the outcome of non-surgical root canal treatments. Long lasting break down in the periodontium is the main reason for failure of the root canal treatment in teeth with iatrogenic or pathologic root perforations [14].
Orthograde perforation repair can be challenging for clinicians. The visualization of the perforation area itself can be problematic because bleeding/exudation often makes access to the perforation area difficult [2]. Different materials have been used for perforation repair [5]. An ideal material for perforation repair should be biocompatible, should seal the perforation against bacterial ingress, and should induce healing in periodontal tissues [2]. Mineral trioxide aggregate (MTA) has shown reliable and successful outcomes in perforation repair. MTA is biocompatible, osteoinductive and produces a long-lasting seal at the perforation area [6]. Retrospective examination of orthograde perforation repair using MTA showed a success rate of 86% [7]. Another retrospective study on the outcome of perforation repair using MTA showed a success rate of 73.3% during a follow up period of up to 10 years [4].
Calcium-enriched mixture (CEM) cement is a bioactive calcium silicate based cement with the capability of producing hydroxyapatite crystals on its surface when in contact with tissue fluids [8]. CEM cement induced periodontal regeneration when used as perforation repair material [9] or root-end filling material [10] in dogs. Also, CEM cement was successfully used as a perforation repair material in iatrogenic [11] and pathologic [12] root perforations. CEM is a white tooth-colored cement which makes it a favorable choice for perforation repair in anterior teeth [13]. CEM cement sets faster than ProRoot MTA [14] and causes significantly less crown discoloration in long-term (5 months) [13]. The major components of the CEM cement powder are CaO, SO3, P2O5 and SiO2, with small amounts of Al2O3, Na2O, MgO, Cl. The cement is alkaline (pH > 10.5) and releases CH during and after setting [14]. This article presents successful non-surgical repair of an old perforation in the coronal third of a maxillary canine which caused extensive periodontal damage, pocket formation, and communication with the oral cavity. CEM cement was used as the perforation repair material.
CASE REPORT
A 36-year-old female was referred by her prosthodontist to an oral surgeon for the extraction of tooth #13. The patient did not want to extract her tooth and asked for further evaluations. The prosthodontist referred the patient to an endodontist. The referral letter stated that tooth #13 has an old perforation repaired with zinc-oxide eugenol paste. The perforation happened about 3 years ago during a restorative procedure. The patient has recently developed an ‘infection’ in the area and the tooth has an unfavorable periodontal prognosis.
Patient's medical history was non-contributory, and she was not taking any medications at the time of examination. The chief complaint was presence of a ‘bump’ on the gingival tissue between teeth #13 and #12 with a localized discomfort. Clinical examination of the area showed that tooth #13 had a large class 4 (distal-facial-palatal-incisal) resin restoration. Tooth #13 was not tender to percussion or palpation at the periapex. The mobility was within normal limits (< 1 mm labio-palatally). The probing depth was 10 mm on mesial and mesio-palatal of tooth #13 with bleeding on probing. The probing depths were within normal limits (i.e., ≤ 3 mm) on other areas of tooth #13 and on adjacent teeth. A sinus tract and a parulis were present on the attached gingiva between teeth #13 and #12. The sinus tract was not patent for tracing at the time of evaluation. Radiographic examinations showed tooth #13 was previously treated with normal periapical tissues. The prior root canal filling was 2 mm short of the radiographic apex. The outline of the access cavity suggested an iatrogenic perforation on the mesial side 7 mm apical to the cemento-enamel junction (CEJ). There was crater-shaped interproximal alveolar bone loss between teeth #6 and #7 (Figure 1A). This mesial interproximal bone loss and 10 mm periodontal pocket was determined to be associated with the iatrogenic perforation. Considering the time lapse since occurrence of the perforation (about 3 years), location of the perforation, pocket formation, and extensive interproximal alveolar bone loss, the prognosis of the perforation repair was deemed unfavorable. The patient was informed about these findings. The treatment options presented to the patient were no treatment, extraction (as recommended by the referring dentist), and perforation repair. It was explained that perforation repair had an unfavorable prognosis with a very high failure rate [4]. She was advised to proceed with the recommendation of referring prosthodontist for extraction of tooth #13 followed by a dental implnat #13. However, the patient wanted to save the tooth. She elected to repair the perforation. Written informed consent was obtained.
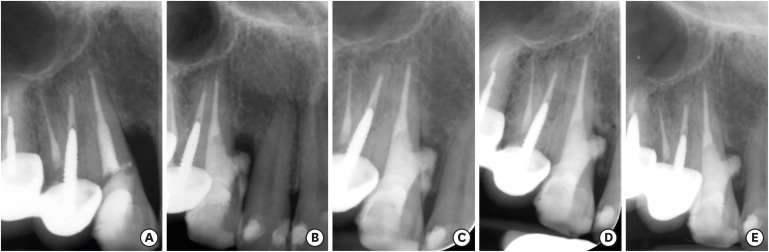
(A) Pre-operative radiograph of tooth #13 showing a crater-shape bone loss on the mesial and a possible iatrogenic perforation on the coronal third of the root below cemento-enamel junction. There are 10 mm pockets on the mesial and mesio-palatal; (B) Immediately after perforation repair with calcium-enriched mixture (CEM) cement. Part of the material is extruded into the mesial periodontal pocket; (C) 6-month follow up; (D) 12-month follow up; (E) 18-month follow up. Note the formation of the interdental alveolar bone and partial resorption of the extruded CEM cement. The tooth is functional with normal probing.
After local anesthesia using labial and palatal infiltration of 1.7 mL 2% lidocaine with 1/100,000 epinephrine (Novocol Pharmaceutical, Cambridge, Canada), the tooth was isolated with a rubber dam. An access cavity was prepared through the coronal resin restoration using a fissure diamond bur (Endo Access Round-end Taper, Diatech, Heerbrugg, Switzerland). The gutta-percha in the coronal third was removed using a gates glidden drill size #4. Then the access cavity was extended towards mesial and mesio-palatal, and the old perforation repair material was removed to uncover the perforation. Profuse bleeding started after the perforation was uncovered. The access cavity was gently irrigated with 10 mL of 0.5% sodium hypochlorite. Care was taken to keep the tip pf the needle away from the perforation during irrigation. The solution was left in the access cavity for 10 minutes to control the bleeding and disinfect the perforation site. CEM cement powder and liquid (BioniqueDent, Tehran, Iran) was mixed to a putty consistency and carried into the access cavity using an amalgam carrier. CEM cement was gently adapted apically towards the root canal filling material and laterally on the dentinal walls around the perforation site using a saline-moistened cotton pellet. The procedure was continued until the entire access cavity was filled with CEM cement. The tooth was then restored with a base of glass ionomer cement (Fuji II, GC Corporation, Tokyo, Japan) and composite resin (3M ESPE, St. Paul, MN, USA). The rubber dam was removed, and a final periapical radiograph was taken to check the quality of perforation repair (Figure 1B). The radiograph showed extrusion of the CEM cement through the perforation site. Part of the extruded CEM cement that was visible clinically was removed using a curved explorer. The patient was informed about the extruded material and the added risk of failure due to possible interference with periodontal healing.
The patient was recalled at 6, 12, and 18 months after the initial visit. At all recalls, tooth #13 was asymptomatic and functional. Clinically, there was no percussion or palpation sensitivity, no sinus tract or parulis, probing depths were ≤ 3 mm with no bleeding, and the mobility was normal. Radiographic examination at 6 months (Figure 1C) showed osseous healing apical to the perforation site and mesial to the extruded CEM cement. The 12- and 18-month radiographs (Figure 1D and 1E) showed that the extruded CEM cement coronal to the perforation site was replaced with newly-formed bone. The 18-month radiograph (Figure 1E) showed continued regeneration of the interdental crestal bone between teeth #13 and #12.
DISCUSSION
A recent Editorial in the Journal of Dental Research has made a call to action to revisit the long history of success of tooth maintenance to preserve the natural dentition without the rush to extract teeth and replace with implants [15]. In the presented case, the recommendation to extract the tooth was based on evidence showing that old perforations with periodontal pocket formation and oral communication generally have an unfavorable prognosis [45]. However, the clinical and radiographic outcome of the treatment proved that even in such compromised situations, it is possible to achieve long-term success using a non-surgical repair procedure, which is a more conservative and less expensive treatment compared to extraction and implant placement.
Perforations in the coronal third of the root adjacent to the crestal alveolar bone have the worst prognosis compared to perforations in the other areas of the root [4]. If left untreated, apical migration of the periodontal attachment (i.e., pocket formation) happens relatively quickly. Once the pocket is formed, persistent inflammation of the area is expected due to continuous bacterial ingress through the pocket [2]. At this stage, repair of the perforation has an unfavorable treatment prognosis from periodontal aspect. Clinical research shows that presence of a radiolucent lesion adjacent to the perforation, periodontal breakdown at the perforation site (in the form of deep probing, recession, etc.), and presence of communication between perforation and oral cavity are negative prognostic factors for the outcome of perforation repair [1457]. Failure rate following repair of perforations in the coronal third of the root with pocket formation is reported to be 100% [4]. Another study showed that teeth with deep probing and periodontal pocket formation adjacent to the perforation showed 21 times higher risk of failure and continued inflammation compared to the perforated teeth with normal probing [16].
Despite all these negative prognostic factors in the presented case, periodontal healing occurred following non-surgical repair with CEM cement. Even the extruded material did not interfere with the healing process and no surgical intervention was required. A recent clinical study raised questions about our knowledge of the prognosis of perforation repair [16]. They suggested that the classic negative prognostic factors might not be applicable if a bioactive cement is used for perforation repair [16]. A systematic review and meta-analysis of the clinical outcomes of perforation repair showed that the type of repair material is in fact an important prognostic factor [5]. The study showed that the overall success rate of perforation repair was 72.5%, but it increased to 80.9% when MTA was used as the repair material. Other studies have shown that the outcome of perforation repair is affected by operator experience. When the perforation repair was done by endodontic specialists the success rate was higher [716] and the outcome was more predictable [1718].
Calcium silicate-based cements, like MTA, are bioactive. Hydroxyapatite crystals are formed on the surface of the set bioactive cements in contact with tissue fluids [1920]. This bioactivity is the basis for biocompatibility and hard tissue induction potential of calcium silicate-based cements. Osteogenic, dentinogenic, and cementogenic potential of MTA has been documented in several different studies [6]. Like MTA, CEM cement is a calcium silicate-based bioactive cement. CEM cement has been successfully used as capping material in vital pulp therapies [212223], as root-end filling material in root-end surgeries [24], as perforation repair material in diverse types of perforation repairs [111225], as obturation material and apical plug in immature teeth [2627], and as a coronal plug in regenerative endodontic treatments [2829]. Osteogenic [10], dentinogenic [30], and cementogenic [9] potential of CEM cement has been documented.
Osseous healing adjacent to the extruded CEM cement and partial replacement of the extruded material with the newly-formed bone shows a possible biological integration at the material-bone interface. Previous studies showed bone formation adjacent to extruded MTA [313233] and resorption of extruded MTA over time [3133]. Case reports showed that complete absorption of extruded bioactive cements can happened over extended periods of time (4 to 7 years) [3133]. Nevertheless, extrusion of the root canal filling materials (including perforation repair materials) into the periodontium should be prevented using biocompatible sterile barriers like collagen [2]. CEM cement is white and does not discolor teeth [13], which makes it a superior option for perforation repair in anterior teeth compared to MTA.
CONCLUSIONS
In conclusion, this case report shows the possibility of periodontal healing following non-surgical repair of perforations in the coronal third with pocket formation and radiolucent lesion. Therefore, the classic negative prognostic factors for perforation repair might not be applicable if a bioactive material is used for repair. Further investigations on mechanisms of healing of the bone and periodontium following iatrogenic perforations are recommended. Clinical studies with larger sample size, longer follow ups and three-dimensional imaging documentation are recommended.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Asgary S, Verma P, Nosrat A.
Investigation: Asgary S, Verma P, Nosrat A.
Methodology: Asgary S, Nosrat A.
Writing - original draft: Nosrat A.
Writing - review & editing: Asgary S, Verma P.