Comparison of apical extrusion of intracanal bacteria by various glide-path establishing systems: an in vitro study
Article information

Abstract
Objectives
This study compared the amount of apically extruded bacteria during the glide-path preparation by using multi-file and single-file glide-path establishing nickel-titanium (NiTi) rotary systems.
Materials and Methods
Sixty mandibular first molar teeth were used to prepare the test apparatus. They were decoronated, blocked into glass vials, sterilized in ethylene oxide gas, infected with a pure culture of Enterococcus faecalis, randomly assigned to 5 experimental groups, and then prepared using manual stainless-steel files (group KF) and glide-path establishing NiTi rotary files (group PF with PathFiles, group GF with G-Files, group PG with ProGlider, and group OG with One G). At the end of canal preparation, 0.01 mL NaCl solution was taken from the experimental vials. The suspension was plated on brain heart infusion agar and colonies of bacteria were counted, and the results were given as number of colony-forming units (CFU).
Results
The manual instrumentation technique tested in group KF extruded the highest number of bacteria compared to the other 4 groups (p < 0.05). The 4 groups using rotary glide-path establishing instruments extruded similar amounts of bacteria.
Conclusions
All glide-path establishment instrument systems tested caused a measurable apical extrusion of bacteria. The manual glide-path preparation showed the highest number of bacteria extruded compared to the other NiTi glide-path establishing instruments.
INTRODUCTION
All instruments and techniques used for root canal preparation are associated with debris extrusion, which contains dentin chips, pulp tissue, microorganisms and/or irrigants, into the periradicular tissue [123]. This extrusion may potentially result in post-operative flare-ups [456] or lead to the development of ulcerative and tissue necrosis processes [789].
Various instrumentation techniques, whether they are engine driven or manual preparation, have been associated with different amounts of apical debris extrusion [1011]. Rotary instruments improve coronal evacuation of dentin chips out of the tooth rather than extruding them in an apical direction out of the root when compared to hand file preparation [12]. Assessing and evaluating apical debris extrusion as a result of canal shaping by different instrument systems and techniques were investigated previously [1314].
While full-sequence rotary instrumentation was reported to be associated with less debris extrusion compared with the use of reciprocating single-file systems, both of the WaveOne (Dentsply Maillefer, Ballaigues, Switzerland) and ProTaper rotary instruments (Dentsply Maillefer) produced significantly more debris compared with the Hyflex CM rotary instruments (Coltene/Whaledent, Altstätten, Switzerland) [15]. Regardless of the instrument types used for canal shaping, the glide-path preparation procedure may reduce the debris and/or bacterial extrusion [16].
Various nickel-titanium (NiTi) rotary glide-path instrument systems, such as G-File (Micro-Mega, Besançon, France), ScoutRace (FKG Dentaire SA, La Chaux-de-Fonds, Switzerland), PathFile (Dentsply Maillefer), One G (Micro-Mega), and ProGlider (Dentsply Maillefer), have been introduced. These systems comprise 1 to 3 sequential and multiple instruments. Some of these glide-path preparation instruments were compared for the efficiency and fracture resistances [1617]. The G-File rotary instruments and the PathFile system reduced the debris extrusion than the manual preparation using stainless steel instrument. The ProGlider system had lower debris extrusion than the PathFile and One G system [16].
Meanwhile, the claim on that the greater the extruded debris weight may increase the severity of the inflammatory response is not well rationalized as “it is likely that not only the quantity of debris but also the type and virulence of bacteria and the resistance of host tissue are important” [1819]. Therefore, considering the importance of this parameter and the biologic efficacy of glide-path establishing instrument during root canal preparation, the purpose of this in vitro study was to assess the amount of apically extruded bacteria during the glide-path preparation with a manual stainless-steel file and various rotary glide-path systems.
The hypotheses tested were 1) all the rotary glide-path systems will extrude less bacteria than the manual glide-path technique and 2) the single-file rotary glide-path systems will extrude less bacteria than the multi-file systems.
MATERIALS AND METHODS
Teeth selection
Sixty mandibular first molar teeth that meet the inclusion criteria were collected and used under the approval by the University of Pavia Institutional Review Board (UPAV201507). Radiograph of each tooth was taken, digitized, and stored electronically. Inclusion criteria were: moderately curved mesial roots with angles of curvature ranging between 10° and 20° and mesial root canals with an initial apical size equivalent to a size 10 K-file. The teeth were disinfected in 0.5% chloramine T solution, stored in distilled water at 4°C, and used within 6 months after extraction.
Teeth preparation
The teeth were decoronated at 3 mm above the level of the cemento-enamel junction using a diamond bur under continuous saline irrigation. The crown was partially maintained to create a reservoir for infection of root canals. The root canal and apical foramen were explored with a size 10 K-file. Working length (WL) was measured by visualization under a dental-operating microscope at ×20 magnification (M320 Leica, Leica Microsystems, Wetzlar, Germany). Size 10 K-file was introduced beyond the apical foramen and 1 mm was subtracted from the length of apical foramen. After that, the length of all roots was standardized to have 13 mm of WL.
Test apparatus
Vials with rubber stopper were adjusted with a heated instrument to create a hole through the center. The prepared tooth was adapted under pressure into the rubber stopper and fixed with cyanoacrylate cement. Two coats of nail varnish were applied to the external surface of all roots to prevent bacterial microleakage through lateral canals. The rubber stopper with the tooth was fitted into the opening of the vial and sealed with Parafilm (Sigma-Aldrich Co., St. Louis, MO, USA). The apical part of the root was suspended within the vial. The vial was used as the collecting container for apical material extruded through the foramen of the root. A 27-gauge needle was inserted into the rubber stopper to equalize the air pressure inside and outside the vial. The entire model system was sterilized in ethylene oxide gas for a 12-hour cycle using an anprolene 74°C gas sterilizer (Andersen Products, Essex, UK) (Figure 1).
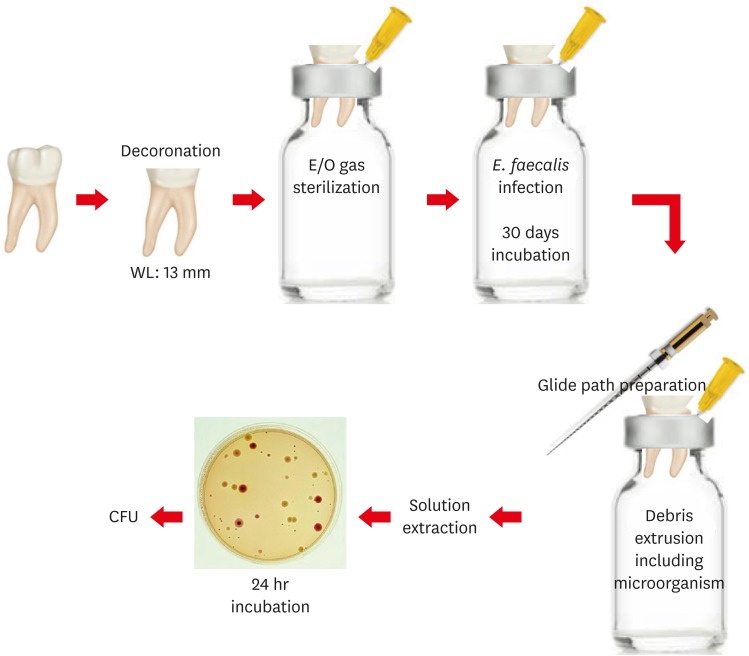
The schematic diagram of the methods used in this study.
WL, working length; E/O, ethylene oxide; CFU, colony-forming unit.
Infection with Enterococcus faecalis (E. faecalis)
A pure culture of E. faecalis (ATCC 29212) was used to infect root canals. A suspension was prepared by adding 1 mL of a pure culture of E. faecalis grown in brain heart infusion (BHI) broth for 24 hours to fresh BHI broth. The bacterial suspension was adjusted to a McFarland standard number 0.5 to ensure that the bacterial concentration would be 1.5 × 108 colony-forming units (CFU)/mL. Before infection of root canals, a sterile size 10 K-file was placed 1 mm beyond the foramen to create a hole in the nail varnish that covered the apical foramen. Each root canal was filled completely with the E. faecalis suspension using sterile micropipettes. A size 10 K-file was used to carry the bacteria down the length of the canals. The infected root canals were incubated at 37°C for 30 days to simulate chronic infection. To maintain the biofilm, the infected roots received new sterile BHI medium every other day. Glass vials were entirely filled with 0.9% NaCl solution. The tooth-rubber stopper-needle unit was fitted into the mouth of the vial.
Test groups
The groups were randomly distributed using a computer algorithm (http://www.random.org). Teeth were assigned to one of the experimental groups (n = 10) as the following:
In group KF, manual K-files size 10, 15, and 20 (Micro-Mega) were introduced sequentially into the canal to the WL using the balanced force movement. As experimental groups, 4 rotary glide-path preparation files were used with Endo Mate (Endo Mate DT, NSK, Tochigi, Japan) according to the manufacturer's instructions. In group PF, PathFile system composed of 3 instruments with 0.02 taper and tip size 13 (PathFile #1), 16 (PathFile #2), and 19 (PathFile #3) was sequentially introduced into the canal using the motor adjusted to 300 rpm and 5 Ncm. In group GF, G-File system composed of 2 instruments with 0.03 taper and size 12 (G1) and 17 (G2) was introduced with the motor set at 300 rpm and 1.2 Ncm. In group PG, ProGlider (Dentsply Maillefer) of single-file rotary glide-path system with a variable taper and tip size 16 was used at 300 rpm and 5 Ncm. In group OG, another single-file rotary glide-path system One G (Micro-Mega) with 0.03 taper and tip size 14 was used at 300 rpm and 1.2 Ncm. The teeth for the positive and negative control groups were composed of 5 specimens for each, and the specimens in the positive control were infected but were not instrumented. Teeth in the negative control were not infected but instrumented with one of the 5 systems for each specimen respectively. One instrument (set) was used for only one tooth.
The teeth were instrumented to get the debris into the collection containers. One operator, using aseptic techniques, carried out canal preparation and sampling procedures on each specimen under a class I laminar airflow cabinet to prevent airborne bacterial contamination. A total volume of 6 mL 0.9% NaCl solution was used for each root canal as an irrigant because of the different number of files in the 3 groups. The irrigants were delivered using syringes with a disposable 30-gauge stainless steel endodontic irrigation needle placed passively down the canal, up to 3 mm from the apical foramen without binding.
At the end of canal preparation, 0.01 mL NaCl solution was taken from the experimental vials. The suspension was plated on BHI agar. The plates were incubated at 37°C for 24 hours. Colonies of bacteria were counted, and the results were given as the number of CFU.
Statistical analysis
Statistical analysis was carried out using non-parametric Kruskal-Wallis analysis and post hoc Mann-Whitney U test. Significance was set at 95%.
RESULTS
Data regarding the number of bacteria extruded are presented in Table 1. The results indicated that all instrumentation techniques tested caused a measurable apical extrusion of bacteria. The manual instrumentation technique tested in group KF extruded the highest number of bacteria compared to the 4 other groups (p < 0.05). The other 4 groups using rotary glide-path establishing instruments extruded a similar quantity of bacteria as shown in Figure 2.

Descriptive statistics of colony forming units for each group tested
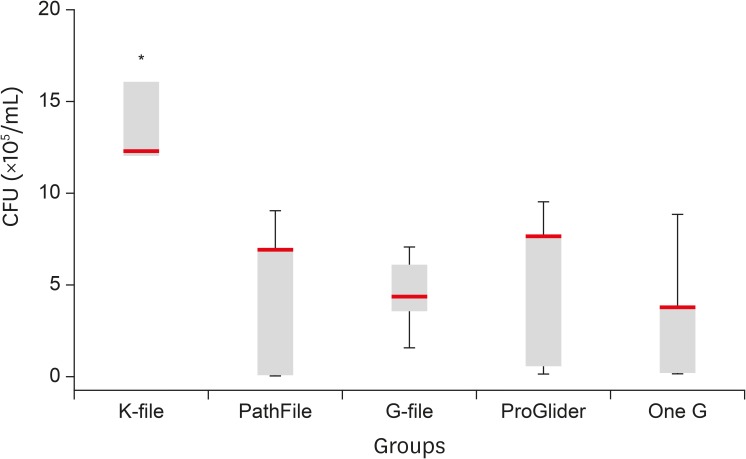
The manual instrumentation technique tested in K-file extruded the highest number of bacteria compared to the other groups.
CFU, colony-forming unit.
*It means significant differences from other groups, p < 0.05.
DISCUSSION
The main goal of root canal preparation is to clean and shape the root canal while maintaining the original canal configuration [20]. In the early stages of root canal preparation, a glide-path preparation is highly recommended to make a minimal space for NiTi rotary instruments to enlarge the canals [212223]. Compared to manual glide-path preparation with stainless steel files, NiTi rotary instruments are faster, maintain the original canal anatomy better, and result in lesser modification of canal curvatures leading to fewer canal aberrations [24]. Creating a glide-path may also increase the lifespan of the rotary instrument by reducing torsional stress during instrumentation [23]. From the results of the present study, while the stainless steel manual instruments showed significantly greater bacterial extrusion than the rotary files, there was no significant difference between rotary instrument groups.
Postoperative pain and swelling are mainly associated with the preparation procedures. They involve the host immune response against extruded debris containing microorganisms, over-instrumentation, or the obturation material [426]. Extruded debris containing microorganisms, dentin particles, or necrotic pulp tissue remnants may trigger inflammatory reaction in the periapical region and subsequent postoperative pain and swelling [425]. Therefore, in the present study, the microbial extrusion by glide-path establishing instruments was quantitatively compared. The results showed that the motor driven glide-path establishing instruments may have lower microbial extrusion than the manual preparation. It may implicate that motor driven NiTi glide-path files would be much proper instruments than stainless steel instruments. Ha et al. [16] also reported that the rotary glide-path establishing instruments (One G, ProGlider, ScoutRace) have significantly lower extrusion of debris than the manual stainless steel group. Also, the ProGlider had the least extrusion of debris among the other rotary NiTi instrument groups. They analysed the geometric differences resulted in the difference of debris extrusion.
However, the main factor to decide the clinical relevance should be microorganisms. During the root canal preparation and irrigation, intra-canal contents are forced to extrude as debris such as dentin particles, necrotic pulp tissue remnants, or microorganisms [425]. These may trigger the inflammation reactions in the periapical region. By establishing a glide-path prior to the root canal preparation, debris extrusion could be decreased, and it would reduce postoperative pain [426]. Many previous studies have been conducted regarding debris extrusion using the NiTi root canal shaping instruments, especially for minimising debris extrusion during reciprocating preparation [1926]. Pasqualini et al. [24] reported that the NiTi rotary glide-path files induced less postoperative pain than the stainless steel manual files. Based on this and previous studies, recently introduced convenient and highly efficient NiTi rotary instruments for the glide-path preparation have sufficient benefit to reduce the toxic extrusion of microbiological and non-biological debris.
In the present study, mandibular molar in which the size 10 K-file hardly reached the apical foramen were selected, and the size 10 K-file was used prior to using 4 glide-path establishing files. This step in the method was important to compare the file systems fairly. To mimic the clinical situation and to exclude a potential effect of different WLs on the debris removal or bacterial extrusion, the coronal structure of each tooth was removed and flattened as a reference point for a consistent study condition. Further, the WL was adjusted to 13 mm to standardize the depth of shaping and the penetration of irrigation. Although a physical back-pressure provided by the periapical tissues could not be simulated, the generally accepted method of Myers and Montgomery allowed the comparison of the file systems [27].
The test results of present study are in accordance with the previous studies that rotary NiTi instrumentation showed less debris extrusion than hand instrumentation [1628]. The stainless steel instruments extruded much more bacterial organism than all the other instruments used in this study. The stiffness and push-pull motion with minimal rotation would be the main reasons for this phenomenon [16]. Although the statistical significance is not implacable, the difference of geometries and number of instruments of the glide-path establishing system may have some effect on the debris or bacterial extrusion tendency.
Although the glide-path preparation is an adjunctive procedure prior to the main instrumentation, it was observed that the methodological difference of glide-path preparation prior to the main instrumentation resulted in significantly decreased postoperative pain [4]. This result may have resulted from the amount of bacterial extrusion. Therefore, present study paid attention to the bacterial extrusion during glide-path establishing procedure. Although the amount would be very low, the initially extruded debris may have higher toxic potency than the debris extruded later by shaping instrument [42528]. Future studies focused on the aspect of extrusion as calcitonin gene-related peptide and substance P expression in the periodontal ligament caused by glide-path instrument would help us better understand the influence of the glide-path instruments on the inter-appointment pain and discomfort [16].
This study may prove clinically implacable effects from glide-path preparation procedure and potential effects of debris and bacterial extrusion. The debris extrusion during glide-path preparation would be clinically important due to the fact of bacterial extrusion.
CONCLUSIONS
Within the limitations of this in vitro study, data indicated that all instrumentation techniques tested caused a measurable apical extrusion of bacteria. Manual instrumentation technique showed the higher number of bacteria extruded compared to the other NiTi rotary glide-path instrumentation groups.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Dagna A, El Abed R.
Data curation: Bertoglio F, Beltrami R.
Formal analysis: Beltrami R.
Funding acquisition: Dagna A, El Abed R.
Investigation: Dagna A, El Abed R, Poggio C.
Methodology: Dagna A, Poggio C, Visai L, Bertoglio F, Bosco F.
Project administration: Dagna A, Poggio C, Visai L.
Resources: Dagna A, Poggio C, Visai L, Bertoglio F.
Software: Poggio C, Beltrami R.
Supervision: Dagna A, Kim HC.
Validation: Dagna A, El Abed R, Hussain S, Abu-Tahun IH, Visai L, Bertoglio F, Bosco F, Beltrami R, Poggio C.
Visualization: Dagna A, El Abed R, Hussain S, Abu-Tahun IH, Visai L, Bertoglio F, Bosco F, Beltrami R, Poggio C.
Writing - original draft: Dagna A, El Abed R.
Writing - review & editing: Kim HC.
