Retreatability of two endodontic sealers, EndoSequence BC Sealer and AH Plus: a micro-computed tomographic comparison
Article information
Abstract
Objectives
Recently, bioceramic sealers like EndoSequence BC Sealer (BC Sealer) have been introduced and are being used in endodontic practice. However, this sealer has limited research related to its retreatability. Hence, the aim of this study was to evaluate the retreatability of two sealers, BC Sealer as compared with AH Plus using micro-computed tomographic (micro-CT) analysis.
Materials and Methods
Fifty-six extracted human maxillary incisors were instrumented and randomly divided into 4 groups of 14 teeth: 1A, gutta-percha, AH Plus retreated with chloroform; 1B, gutta-percha, AH Plus retreated without chloroform; 2A, gutta-percha, EndoSequence BC Sealer retreated with chloroform; 2B, gutta-percha, EndoSequence BC Sealer retreated without chloroform. Micro-CT scans were taken before and after obturation and retreatment and analyzed for the volume of residual material. The specimens were longitudinally sectioned and digitized images were taken with the dental operating microscope. Data was analyzed using an ANOVA and a post-hoc Tukey test. Fisher exact tests were performed to analyze the ability to regain patency.
Results
There was significantly less residual root canal filling material in the AH Plus groups retreated with chloroform as compared to the others. The BC Sealer samples retreated with chloroform had better results than those retreated without chloroform. Furthermore, patency could be re-established in only 14% of teeth in the BC Sealer without chloroform group.
Conclusion
The results of this study demonstrate that the BC Sealer group had significantly more residual filling material than the AH Plus group regardless of whether or not both sealers were retreated with chloroform.
Introduction
The success of nonsurgical endodontic therapy depends on the removal of necrotic and inflamed tissue, microorganisms, and debris from the root canal system and the prevention of recontamination.1 Four conditions which include pre-operative absence of periapical radiolucency, root filling with no voids, root filling extending to 2 mm within the radiographic apex, and satisfactory coronal restoration, were found to significantly improve the outcome of primary root canal treatment.2 However, endodontic failures do occur and the percentages of cases that fail to heal can range from 15 - 22%.3 Nonsurgical retreatment is the principal treatment of choice to manage post-treatment disease.4 Retreatment consists of the removal of existing obturation material to allow disinfection of the root canal system in order to provide an environment satisfactory for periradicular healing.5 Nevertheless, the myriad of retreatment techniques and studies consistently find residual root canal filling after removal is accomplished.6 Removing filling material from root canal systems is necessary because this material could potentially cause a mechanical barrier that hinders contact of irrigating solutions and intracanal dressings to the root canal walls.7 Furthermore, there maybe bacteria present in these areas that could be responsible for post treatment pathosis.8 For this purpose, it is imperative that the obturation material be completely removed in order to improve chances of success.
Gutta-percha (GP) in conjunction with sealers is the most common root canal filling material.9 Currently, many different sealers are being used in endodontics.1011 More recently, bioceramic sealers like EndoSequence BC Sealer (BC Sealer, Brasseler USA, Savannah, GA, USA) have been introduced and are being used in endodontic practice. BC Sealer is a premixed bioceramic endodontic sealer that is composed of zirconium oxide, calcium silicates, calcium phosphate (monobasic), calcium hydroxide, filler, and thickening agents.12 However, this sealer has a short history of use and limited research related to its retreatability. Previous studies on bioceramic sealers have evaluated their bond strength, sealing ability, root fracture resistance, setting properties, cytotoxicity, and antibacterial effects.1314151617 However, there are limited studies related to the retreatability of these sealers.18 On the contrary, AH Plus (Dentsply International Inc., York, PA, USA), an epoxy-resin-based endodontic sealer, has an extensive history of use and research studies13141719 which is why it has been used for many comparative studies.192021
The efficacy of removing the root filling materials during retreatment has been assessed by many different methods. However, most methodologies destroy the specimens. These methodologies include horizontal or vertical splitting of the examined teeth or clearing to render the teeth transparent.2223 Another method involves micro-computed tomography (micro-CT) analysis.8 This method has been used previously and provides detailed imaging of the root canal system without destroying the specimen.
It is important to understand if these newer sealers are retreatable, especially since these materials are being used routinely in endodontics and could affect periapical healing.24 Hence, the aim of this study was to evaluate the retreatability of BC Sealer as compared with AH Plus sealer using micro-CT analysis. The null hypothesis tested was that there were no differences in the retreatability of BC Sealer and AH Plus sealer.
Materials and Methods
Specimen preparation
Fifty-six extracted human single-rooted maxillary anterior teeth with straight roots were selected. Roots with curvatures higher than twenty degrees were excluded. Only fully formed apices with a single root canal and a single apical foramen were included. The presence of a single canal was verified with buccal and proximal radiographs. Teeth were divided into 4 groups of 14 teeth each:
Group 1A: Canals obturated with GP/AH Plus and retreated using chloroform.
Group 1B: Canals obturated with GP/AH Plus and retreated without chloroform.
Group 2A: Canals obturated with GP/BC Sealer and retreated using chloroform.
Group 2B: Canals obturated with GP/BC Sealer and retreated without chloroform.
Teeth that had an initial apical file size of more than a size 25 were discarded. Teeth were decoronated with a diamond disk (Keystone industries, Gibbstown, NJ, USA) to standardize the lengths to 17 mm with the aid of calipers. After access, cavity preparation patency and working length were determined by introducing a size 10 Flexofile (Dentsply Maillefer, Tulsa, OK, USA) in the canal until it was visible at the apical foramen and by subtracting 1 mm from this measurement for a working length (WL) of 16 mm.
Instrumentation of teeth was performed by using a crown-down technique with Vortex Blue (Dentsply, Tulsa Dental Specialties, Tulsa, OK, USA) nickel titanium rotary instruments at 500 rpm to master apical file of size size 45/0.04 taper. Files were used to instrument 5 canals and then replaced. Each canal was filled with irrigant during instrumentation. Three mL of 6% NaOCl was used for irrigation after each file. A size 10 Flexofile was used to reconfirm patency. As a final rinse each canal was irrigated with 2 mL 17% EDTA, 2 mL NaOCl, followed by 2 mL of sterile saline, and then dried with paper points. All irrigating solutions were delivered with a 30 G Max-i-Probe irrigating needle (Dentsply-Rinn, Elgin, IL, USA) placed 1 mm short of the WL.
Micro-CT imaging, 3D rendering, and volume calculations
Specimens were numbered and scanned with a micro-CT (Skyscan 1076, Bruker microCT, Antwerp, Belgium). Each specimen was scanned three times: once following instrumentation to enable calculation of the root canal volume, once to confirm the homogeneity of root canal obturation, and the final time to determine the volume of remaining material. The scanning parameters for each scan were kept constant: 65 kV (10 W, 154 µA), a 0.5 mm aluminum filter, a 160 milllisecond exposure time and 0.70° rotation step, and isotropic voxel size of 35 µm. Raw scan data were reconstructed into multiplanar slice data using the computer program, NRecon V1.6.1.0 (Bruker microCT).
After reconstruction of the initial scan dataset, the degree of curvature of the root canals was re-evaluated from images rendered with the 3D volume exploration software, Drishti V2.4 (http://sf.anu.edu.au/Vizlab/drishti) and compared with the original determinations from the 2D radiographs. The curvatures were checked once again to ensure none had curvatures greater than 20 degrees. For calculation of the root canal volume following instrumentation, the canal was reverse filled by inverting the rendering settings (ie. transfer function) and using the getvolume function in Drishti.
To enable calculation of total remaining sealer after retreatment, rendering settings were applied that readily detected the radiopaque sealer (Figure 1). The same rendering settings were applied to both the second (obturated) and third (retreated) scan datasets and the volumes of sealer determined again using the getvolume function. For visualization purposes, the 3D renderings of each tooth was manually aligned and oriented in the same multi-dimensional space and different transfer functions applied to show both the surface of the root and the sealer (Figure 1, root, black; obturation material, orange). For subdivision of the root canal into thirds (apical, middle, and coronal), the rendered datasets were virtually cut in the horizontal plane such that each third consisted of the exact number of rendered slices. The volume of sealer remaining in each third was then determined using the getvolume function of Drishti as described above.
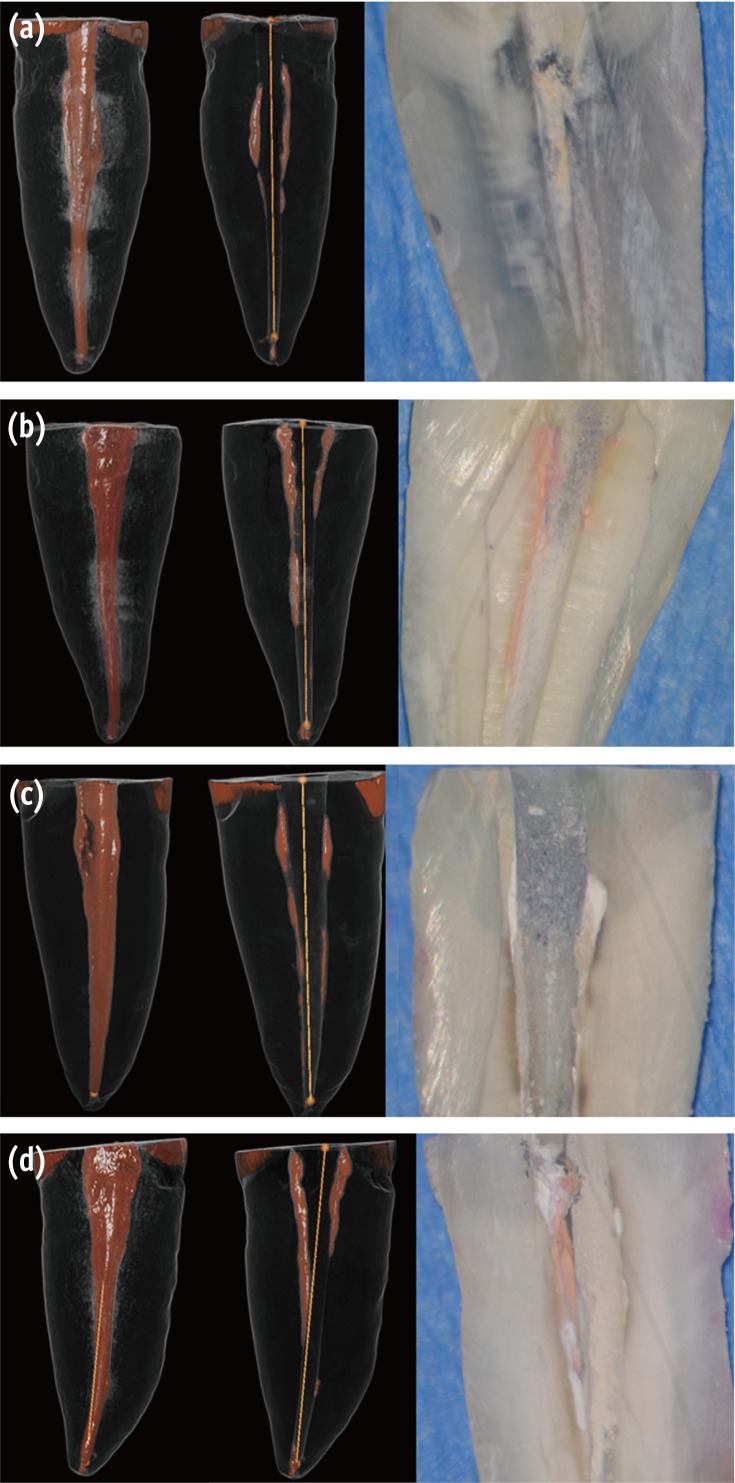
Visualization of residual sealer after retreatment. Micro-CT scans of obturated canals with (a) gutta-percha and AH Plus retreated with chloroform; (b) gutta-percha and AH Plus retreated without chloroform; (c) gutta-percha and BC Sealer retreated with chloroform; (d) gutta-percha and BC Sealer retreated without chloroform retreatment. The left-most images are representative 3D renderings of the filled canals, while the adjacent images are the same teeth following retreatment. Black, root surface; white and orange, obturation material. The right-most images are the corresponding longitudinal sections of these teeth. Micro-CT, micro-computed tomography; BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA); 3D, 3 dimensional.
Root canal obturation
The teeth were randomly divided into 2 groups (Groups 1 and 2) of 28 each. All canals were obturated by the continuous wave compaction technique. In Group 1, twenty-eight canals were obturated by coating EndoSequence gutta-percha (Brasseler USA) of size 45/0.04 with AH Plus sealer (Dentsply Maillefer) following the manufacturer's protocol. In Group 2, 28 canals were obturated with EndoSequence gutta-percha points and EndoSequence BC Sealer again following the manufacturer's protocol. The access preparations were sealed with Cavit (3M ESPE, St. Paul, MN, USA). The same volumes of sealer were used for both groups of teeth. The specimens were scanned a second time with the micro-CT using the same scanning parameters to confirm the homogeneity of root canal obturation. All samples were stored at 37℃ in 100% humidity for 30 days to allow the sealers to set completely. A single operator performed all the procedures.
Retreatment with or without chloroform
Each group was divided into two subgroups: Groups 1A and 2A were retreated using chloroform; Groups 1B and 2B were retreated without chloroform. Briefly, for Groups 1A and 2A, Cavit was removed and a total of 0.2 mL of chloroform was used for each tooth. Two drops of chloroform were introduced in the access preparations. ProFile ISO Rotary Files (Dentsply Maillefer) of size 45/0.04 taper at 300 rpm were used until WL was reached or resistance was met. If the WL was reached, crown-down instrumentation was performed using Vortex Blue size 45/0.04 at 500 rpm to WL to remove the remaining obturation material. If the WL was not reached, small hand files (C+ Files, and Flexofile sizes 6, 8, and 10) were used to reach WL. When WL was reached, the canal was instrumented to length with Vortex Blue size 50/0.04. The remaining volume of chloroform was introduced in the canals and any remaining gutta-percha was removed with paper points. As a final rinse, each canal was irrigated with 5 mL of 6% NaOCl, 5 mL of 17% EDTA, followed by 2 mL of sterile saline, and then dried with paper points. Files were used to instrument 5 canals and then replaced.
For Groups 1B and Group 2B, retreatment was done as stated above in the methods section with the similar rotary files but without chloroform. After retreatment of all samples, a third micro-CT scan was performed using the same parameters as the first two scans.
Longitudinal sections
The specimens were longitudinally sectioned and observed under the dental operating microscope (×20 magnification, Global Surgical Corp., St. Louis, MO, USA).14 Digitized images were taken for correlation with the results from the micro-CT imaging.
Statistical analysis
SigmaPlot 11.0 (Systat Software Inc., San Jose, CA, USA) was used for the statistical testing. The required sample size was calculated to be 14 samples per group. This gave at least 95% power to detect a maximum difference between group means. Data from the experiments were analyzed using an analysis of variance (ANOVA) to determine differences among the groups, with further pairwise multiple comparisons with a post hoc Tukey test. Fisher exact tests were performed to analyze the ability to regain patency. Differences with p < 0.05 were considered significant.
Results
Residual root canal filling material
The percentages of residual filling material was calculated based on an equation stated in a previous study.8 Analysis of the rendered micro-CT images showed significantly less residual root filling material in Group 1A when compared to Groups 1B, 2A, and 2B when the entire length of the root canal was analyzed (Figure 1). The BC Sealer group retreated with chloroform (Group 2A) showed significantly less sealer than the BC Sealer Group 2B (Figure 2). These results were verified and related closely with the longitudinal sections of the teeth (Figure 1). Group 1B showed less residual material compared to Group 2B, however, these results were not statistically significant. All teeth were scanned using micro-CT but only representative images have been shown in Figure 1.
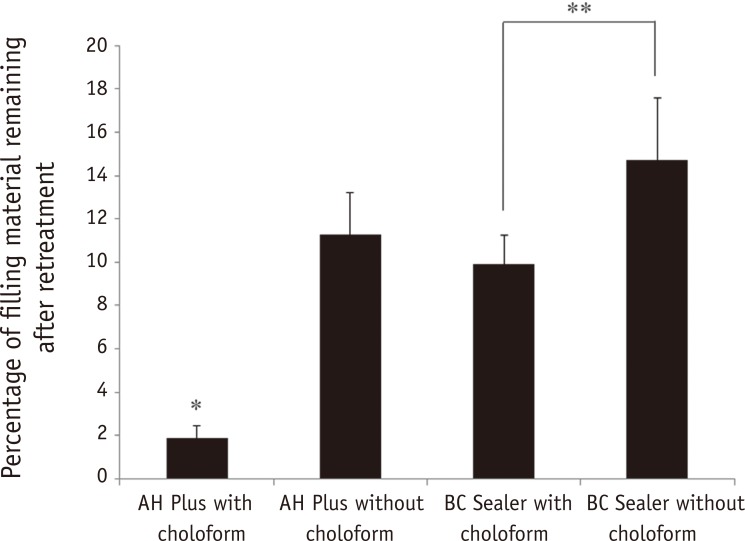
Percentage of residual filling material in the entire length of root canal. The differences in the percentage of residual root canal filling were statistically significant between the AH Plus with chloroform and the other groups (*p ≤ 0.05). The BC Sealer with chloroform group was significantly different from the BC Sealer without chloroform group (**p ≤ 0.05). BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA).
Comparison of apical, middle, and coronal one-thirds for residual root canal filling material
The teeth were further analyzed after micro-CT analysis for residual filling material in the coronal, middle, and apical thirds of the canal. There was significantly less residual root canal filling material in all the areas of Group 1A compared to those one-thirds of Groups 1B, 2A, and 2B (Figure 3). Furthermore, the BC Sealer group that was retreated without chloroform (Group 2B) showed significantly more sealer in the coronal 1/3 of the root as compared to those teeth that were retreated with chloroform (Group 2A).
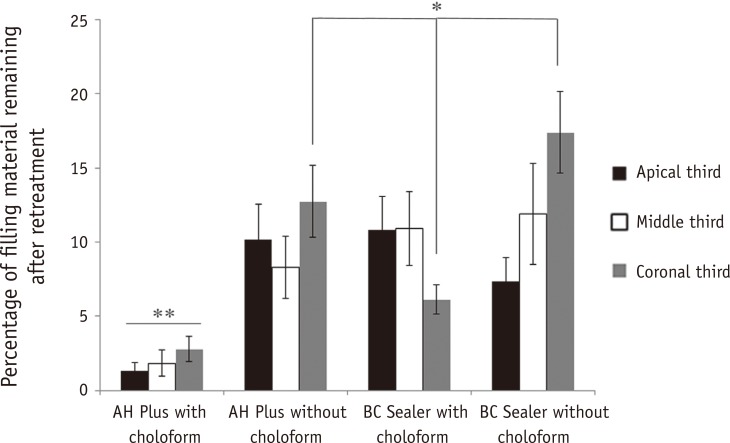
Percentage of residual filling material of apical third compared with middle and coronal third of canals. The differences in the percentage of residual root canal filling were statistically significant between the AH Plus with chloroform and the other groups (**p ≤ 0.05) and between the BC Sealer group retreated with chloroform and the AH Plus and BC Sealer groups that were not retreated with chloroform (*p ≤ 0.05). BC Sealer, EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA).
Re-establishing working length and patency
Establishing patency and WL in retreatment cases has been shown to significantly improve periapical healing rates.24 Hence these two factors were considered in this study when evaluating all the groups. Patency and WL were reestablished in all the teeth (100%) in the AH Plus groups (Groups 1A and 1B). WL and patency were re-established in 93% of teeth in Group 2A. In contrast, although WL was re-established in 93% of Group 2B teeth, patency could only be re-established in 14% of the cases, which was significantly different from the other groups (p < 0.0001, Table 1).

Ability to regain patency and re-establish working length during retreatment for the different groups
Discussion
Root canal failures occur due to persistent periapical disease after treatment.24 There are a number of causes that could lead to failure to heal which include necrotic tissue, bacterial biofilms, coronal leakage, recurrent caries, and tooth fractures.2526 In order to establish adequate periapical healing, these etiological factors must be removed. Hence, it is imperative that the root canal system be adequately cleaned which would entail removing the entire existing root canal filling. Furthermore, establishing patency and WL in retreatment cases has been shown to significantly improve periapical healing rates.24 However, this is not always possible due to various factors, which include root canal anatomy.27
Many new sealers have been introduced in the market; however, the retreatability of some of these sealers is still unknown. Hence, this study evaluated the retreatability of the relatively new BC Sealer compared to the more commonly used AH Plus sealer. Previous studies have shown that AH Plus is soluble in chloroform to about 99% which is why it was used for this comparative study.2829 Our results demonstrate that BC Sealer left significantly more residual filling material in the root canal as compared to AH Plus whether or not they were retreated with chloroform, although when treatment was performed with chloroform the differences were even more marked. Nevertheless, when treated with chloroform, the BC Sealer group left less residual material when compared to the group without chloroform (Figure 2). This notable difference between the sealers could be attributed to the fact that BC Sealer has the potential to adhere to the dentin.20 Another explanation for this finding could be related to the tag-like structures that were of calcium and phosphate materials, suggesting intratubular precipitation and this may be responsible for the sealing ability and dentine bonding of this material.3031 Some previous studies have inferred that BC Sealer and AH Plus had comparable remaining filling material.1832 However, retreatment methods and the techniques used in these studies were different and so firm conclusions are not possible. In this study, we employed non-destructive, quantitative high resolution micro-CT-based imaging to assess the percentage of residual filling material of EndoSequence BC Sealer compared to AH Plus with or without the use of chloroform. This methodology, which has been successfully used in other studies, allows stepwise assessment by repeated scans of the same root specimen.1133
Analysis of the apical, middle, and coronal one-thirds of the canals of retreated teeth indicated that AH Plus with the use chloroform had significantly less residual filling material compared to all one-thirds from all the other groups (Figure 3). The longitudinal sections of the teeth corroborated the findings from the micro-CT scans (Figure 1). An interesting observation was the coronal 1/3 of both the Groups 1B and 2B, which demonstrated more filling material remaining. This could be attributed to tooth anatomy and the fact that no chloroform was used in these groups and maybe a solvent is necessary to clean the coronal 1/3 of the canal more efficiently. Most sections showed only residual sealer, however, there were a few specimens in all the groups that did show some residual gutta percha with sealer (Figure 1). This is an important finding as it correlates to some earlier studies that mention that no technique or solvent was effective in completely cleaning the root canal system during retreatment procedures.1834
Another important factor to consider is the concern related to the toxicity of chloroform. In 1976, the U.S. Food and Drug Administration (FDA) banned the use of chloroform in drugs and cosmetics due to toxicity concerns.35 However, there is no available data related to the toxicity of chloroform in endodontics and previous studies have demonstrated that chloroform is safe to be used in endodontics.363738 Furthermore, chloroform has been shown to efficiently soften gutta percha along with having some antimicrobial activity against E. faecalis during retreatment procedures.3940 Hence, based on previous research chloroform was used in this study.
Our study focused on single rooted teeth based on previous studies and the fact that we wanted to demonstrate differences in less complex anatomy.33 It is a possibility that more complex anatomy like mesial roots of mandibular molars could demonstrate even more significant differences between the two sealer groups. Another important aspect that was taken into consideration was the volume of sealer and the quantity of chloroform used in the study. The quantity of chloroform was standardized between Groups 1A and 2A, and the same volume of sealer was used for all the groups. Both these aspects of this study are important as these could have been potential variables when analyzing the results of the study.
Hess et al. evaluated the retreatability of BC Sealer and AH Plus related to patency and loss of WL using the scanning electron microscope.41 This study reported that BC Sealer was impenetrable to small hand files when it remained in the apical foramen. In this study, we had similar results. We demonstrated that while WL and patency could be re-established in 100% of AH Plus samples, these could not be re-established in every tooth in the BC Sealer groups. With the use of chloroform, WL and patency was regained in 93% of BC Sealer samples. Without the use of chloroform WL was re-established in 93% of cases, with patency in only 14% of the BC Sealer samples, which was significantly different from the other groups (Table 1). This is an important factor to consider especially during retreatments as this could affect periapical healing.24
Koch and Brave published a series of three review articles that included retreatment techniques for the removal of gutta-percha and EndoSequence BC Sealer.42 In the reviews, they recommended that retreatment techniques include the use of rotary, hand files, ultrasonics, and solvents (i.e. chloroform), which is why rotary files were used this study. A recent study suggested the use of solvents during retreatments as this technique reduced the amount of debris extruded apically and also reduced the time taken to retreat teeth.43 Furthermore, chloroform has been shown to have a superior ability over other solvents in dissolving canal sealing materials.44 Chloroform did prove to be effective when used with BC Sealer as it increased the likelihood of regaining patency in these samples (Table 1). However, we believe that it may be necessary to develop a solvent that has superior effect on bioceramic sealers to improve its retreatability.
Conclusion
The results of this in vitro study show that conventional retreatment techniques are not always able to fully remove all the filling material from the canal; however, the AH Plus group retreated with chloroform had significantly less material remaining than BC Sealer whether or not chloroform was used. Moreover, the use of chloroform increased the likelihood of regaining patency in a few of the BC Sealer samples but could not be achieved in 100% of the cases. We believe this information is important for practitioners especially when they are retreating teeth that have been previously obturated with BC Sealer.
Acknowledgement
This research was supported by the AAE Foundation Resident Research Grant.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
