Differential diagnosis of periapical cyst using collagen birefringence pattern of the cyst wall
Article information

Abstract
Objectives
Periapical lesions, including periapical cyst (PC), periapical granuloma (PG), and periapical abscess (PA), are frequently affected by chemical/physical damage during root canal treatment or severe bacterial infection, and thus, the differential diagnosis of periapical lesions may be difficult due to the presence of severe inflammatory reaction. The aim of this study was to make differential diagnosis among PC, PG, and PA under polarizing microscope.
Materials and Methods
The collagen birefringence patterns of 319 cases of PC (n = 122), PG (n = 158), and PA (n = 39) obtained using a polarizing microscope were compared. In addition, 6 cases of periodontal fibroma (PF) were used as positive controls.
Results
Collagen birefringence was condensed with a thick, linear band-like pattern in PC, but was short and irregularly scattered in PG, and scarce or absent in PA. PF showed intense collagen birefringence with a short, palisading pattern but no continuous band-like pattern. The linear band-like birefringence in PC was ascribed to pre-existing expansile tensile stress of the cyst wall.
Conclusions
In this study all PCs (n = 122) were distinguishable from PGs and PAs by their characteristic birefringence, despite the absence of lining epithelium (n = 20). Therefore, the authors suggest that the presence of linear band-like collagen birefringence of the cyst wall aids the diagnostic differentiation of PC from PG and PA.
Introduction
The differential diagnosis of periapical cyst (PC), periapical granuloma (PG), and periapical abscess (PA) is sometimes difficult when etiologic cyst epithelium has completely degenerated and been replaced by an inflammatory granulomatous lesion. During endodontic treatment, therapeutic irrigation of a periapical lesion can destroy cystic epithelium due to the cytotoxic effects of sodium hypochlorite, ethylenediaminetetraacetic acid (EDTA), chlorhexidine, etc.123
However, without microscopic observation the differential diagnosis of PC, PG, and PA is sometimes difficult, although radiographic findings are helpful. Neither radiographic size nor presence of an associated radiopaque line alone is sufficient to determine lesion type, and histological examination is required in order to reach a definitive diagnosis.4
Cysts may be defined as a real or imagined lumen lined with stratified squamous epithelium.5 The histological diagnosis of PC is often viewed to be conditional on the presence of epithelium-lined lumen in a random or limited number of serial sections.6 However, this means some partially epithelialized PCs and PCs devoid of lining epithelium are misdiagnosed as PG. In fact, in a previous study, 52% of PCs (n = 256) were found to be epithelialized, and among PCs only 15% were correctly diagnosed.6
Collagen protein is composed of a triple helix, which generally consists of two identical chains (α1) and an additional chain that differs slightly in its chemical composition (α2). Furthermore, it is well known the polymerized structure of mature collagen triple helix exhibits characteristic birefringence (an optical property of a material with a refractive index that depends on the polarization and propagation direction of light) under polarizing microscope,7 and that this collagen birefringence can be used to investigate the stromal fibrous tissue of odontogenic cysts.78910
In histologic cross-sections of diaphysis of the equine third metacarpal bone, collagen fiber orientation under polarizing microscope could be an indicator of a diagnosis of osteoporosis.11 Longitudinal collage fiber orientation is regionally variable and contributes to modulus and strength, but not to fatigue life, and this fiber orientation is reduced by osteonal remodeling.11 These findings indicate that the collagen fiber orientation produced by mechanical stress remains for a long time in tissues, and that it can be detected under a polarizing microscope.
We hypothesized sclerosed collagen bundles exposed to tensile stress by cystic expansion would have higher birefringence than newly produced collagen bundles in PG and periodontal fibroma (PF). In this study, we aimed to examine the different features of the collagen birefringence of PCs, PGs, and PAs under a polarizing microscope.
Materials and Methods
The retained specimens of 325 cases of PC, PG, PA, and PF were used in this study, that is, 122 cases of PC, 158 cases of PG, 39 cases of PA, and 6 cases of PF. These specimens were selected from among those of patients treated in Gangneung-Wonju National University Dental Hospital (GWNUDH) using biopsy results obtained by the Department of Oral Pathology at GWNUDH. The use of biopsy specimens was approved by the institutional review board of GWNUDH (IRB2015-07).
All 325 samples were routinely prepared for histological microsection (4 µm thick) and stained with hematoxylin and eosin. Pathological examinations had been performed from year 2012 to 2015 (Table 1). The sections were routinely embedded for the observation of mid-line main lesions. All microsections were observed under a polarizing microscope (U-POT, Olympus, Tokyo, Japan) for birefringence in the cystic fibrous wall, granulomatous inflammation, abscess, and collagen bundles. Periapical lesions were carefully confirmed by clinico-pathological diagnosis, and re-examined under the polarizing microscope to determine collagen birefringence.

Cases examined in this study and collagen birefringence in periapical lesions
Patterns of collagenous fibrous tissue birefringence were classified according to the intensity of birefringence under a polarizing microscope, as follows: no birefringence (-), rare birefringence (±), mild birefringence (+), moderate birefringence (++), and severe birefringence (+++). The collagen birefringence of periapical and periodontal lesions were captured using a digital camera (DP-70, Olympus) and compared histologically.
Results
Clinical cases showed relatively even gender distribution, and mean ages in the PC, PG, PA, and PF groups were in the fifth decade (Table 1). According to this classification system, PF showed the strongest birefringence (++ ~ +++) followed by PC (+ ~ +++), PG (± ~ +), and PA (- ~ +) (Table 1).
The cyst walls of PCs usually consisted of thick fibrous collagenous bundles that were aligned parallel to the cyst wall. The collagen bundles of PCs exhibited characteristic birefringence patterns which were linearly arranged and densely segmented, while the diffuse collagen bundles of PGs showed irregular birefringence that was usually scattered and rudimentary (Figures 1, 2, 3).
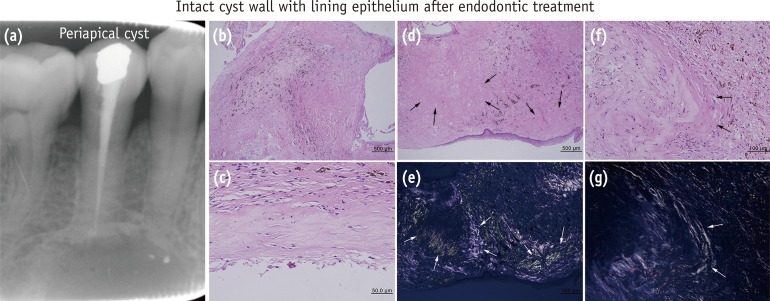
Periapical cyst with lining epithelium after endodontic treatment, noted the linear band-like birefringence in collagen bundles (arrows) encircling the cyst wall. (e) and (g), polarized views of (d) and (f), respectively.
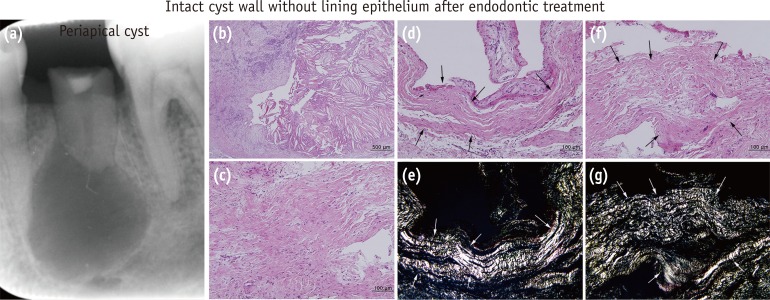
Periapical cyst with no lining epithelium after endodontic treatment, noted strong linear band-like birefringence parallel to the cyst wall in collagen bundles (arrows). (e) and (g), polarized views of (d) and (f), respectively.
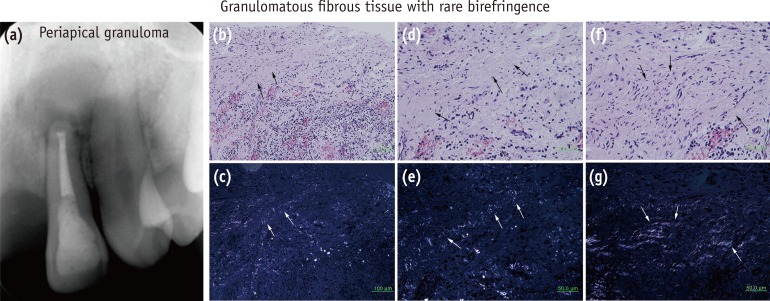
Periapical granuloma, note the weak and rudimentary birefringence in degenerating collagen bundles (arrows) of this granulomatous lesion. (c), (e), and (g), polarized views of (b), (d), and (f), respectively.
Basically the arrangement of collagenous bundles among PCs, PGs, and PFs were different. The fibrous walls of PCs contained thickened collagen bundles arranged in parallel and showed the collagen bundles were condensed parallel. These collagen bundles exhibited strong birefringence (Figures 1 and 2). The fibrous stroma and outer zone of PGs showed relatively irregular arrangements of collagen bundles, which had partly degenerated presumably due to the presence of chronic inflammation. The scattered and partly encapsulated collagen bundles of PG exhibited short, irregular birefringence, which were diffusely dispersed throughout the lesions. On the other hand, the collagen bundles of PF (the positive control) exhibited a dominant interlacing arrangement of collagen bundles and did not form parallel or zonal arrangements. These collagen bundles showed prominent birefringence, which was mostly short, grouped, and diffusely scattered, but no linear band-like pattern was observed in any samples.
Periapical cyst
Among the 122 cases of PC, 21 cases showed no lining epithelium in their luminal surfaces. Histological examination showed cyst walls were lined with odontogenic epithelium (n = 101) and relatively well preserved with thick collagenous fibrous tissue, while cyst walls devoid of lining epithelium (n = 21) showed chronic granulomatous inflammation and their fibrous collagenous walls were partly distorted (Table 2).

Characteristic findings in periapical cyst for differential diagnosis
The histological features of PCs varied considerably from an intact fibrous cyst wall with/without lining epithelium to a severe granulomatous cyst wall with/without lining epithelium. Of the 122 PCs, among 101 cyst walls lined with odontogenic epithelium 69 involved endodontic treatment, and among remaining 21 cyst walls devoid of lining epithelium 16 cases received endodontic treatment. Twenty-three cases of the 122 PCs had almost intact cyst walls with mild inflammatory reaction, and 99 cases had a granulomatous cyst wall with severe inflammatory reaction. Sixty-nine cases out of the 99 degenerated cyst walls involved endodontic treatment, and 15 of 23 intact cyst walls involved endodontic treatment.
Granulomatous inflammation was found in 116 out of 122 PCs, and resulted in marked degradation of collagen bundles in cyst walls. Nevertheless, sclerosed collagen bundles parallel to the cyst wall remained, and these collagen bundles showed strong birefringence with a conspicuous band-like pattern. Furthermore, PCs with a granulomatous cyst wall with/without lining epithelium, like PCs with an intact cyst wall with/without lining epithelium, exhibited the same characteristic birefringence of collagen bundles with a linear band-like pattern (Figures 1 and 2).
Periapical granuloma
All 158 PG cases had a chronic granulomatous lesion without cyst lining epithelium but contained a thin fibrous band encapsulating the granuloma. Ninety-five cases out of the 158 PGs received endodontic treatment. Only 7 cases showed odontogenic epithelial cell rests of Malassez, but had not transformed into odontogenic cysts. Depending on the severity of granuloma inflammation the outer encapsulating fibrous tissue was preserved or partly degenerated, but the collagenous fibrous tissue showed weak birefringence under the polarizing microscope. Collagen bundles were sparsely condensed and loosely arranged in granulomatous stroma, so that their birefringence were relatively weak and rudimentary (Figure 3).
Periapical abscess
Thirty-nine cases of PA were heavily infiltrated with acute/subacute inflammatory cells, polymorphonuclear leukocytes (PMNs), and macrophages, and showed severe degeneration of stromal fibrous tissue. These lesions were usually exacerbated and poorly encapsulated by fibrous tissue. However, inflammatory exudative tissues showed no birefringence under the polarizing microscope, and some collagen bundles remaining in the stromal tissue had degenerated and showed rare birefringence (Figure 4).
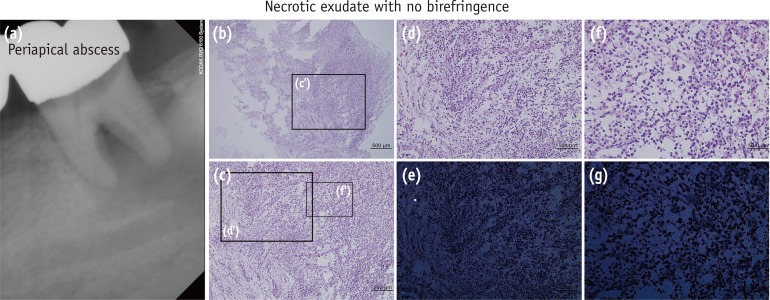
Periapical abscess, note almost no birefringence in the necrotic exudate. (e) and (g), polarized views of (d) and (f), respectively.
Periodontal fibroma
The 6 representative cases of PF were selected as positive controls for collagen birefringence. They were benign periodontal lesions and were almost entirely composed of collagenous fibrous tissue with rich vascular channels. Collagen bundles were short, partly grouped in interlacing arrangement, and showed strong birefringence under the polarizing microscope. Their birefringence patterns were short and irregular, and they did not exhibit the linear band-like pattern of PCs (Figure 5).
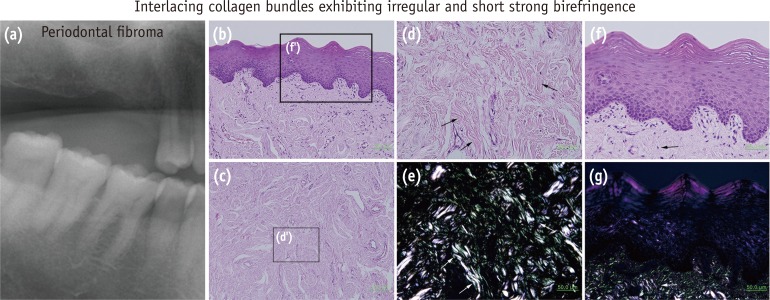
Periodontal fibroma, note strong birefringence with a short and irregularly scattered pattern (arrows). (e) and (g), polarized views of (d) and (f), respectively.
Discussion
PGs and PCs were the most common periapical lesions of endodontic origin associated with persistent periapical pathology. The presence of endodontic materials in a high proportion of periapical lesions suggests a cause-effect association and infers clinicians should employ canal preparation techniques that limit the apical extrusion of materials.1213
It has been reported that in dentigerous cysts, odontogenic keratocysts, and odontogenic tumors, the predominant color of collagen fiber birefringence was orange/red, whereas in radicular cysts collagen fibers were green colored.7 The similar birefringence patterns of collagen fibers in dentigerous cysts, odontogenic keratocysts and odontogenic tumors may indicate that these lesions have a common histogenesis, broad spectrum in biological behavior, and are developmental from a same origin. The different birefringence patterns of radicular cysts suggest different biological behaviors and that inflammation plays a role in the determination of the polarization color of collagen fibers.7
Because the birefringence of collagen fibers in polarized light depends on fiber orientation, viewing sections under polarized light provides a means of determining the variability of collagen fiber orientation within lamellar structures.11 It has been reported longitudinal collagen fiber orientation, as determined by quantifying birefringence under plane-polarized light, is an important predictor of tensile strength in bovine cortical bone.14 Similar results were obtained for the bending strengths and elastic moduli of bovine cortical bone.15 Furthermore, regions of the human femoral diaphysis, which are considered to be subjected to more longitudinal compression in vivo, were found to be more birefringent than regions on the tensile side of the neutral bending axis.11
As compared with the thin collagen fibers in normal connective tissues, thick collagen fibers showed a gradual birefringence change from predominantly yellow/orange to green/yellow during the advancing stages of desmoplastic connective tissue epithelial dysplasia. These changes in birefringence colors and arrangements of collagen fibers may imply impending neoplastic stress in oral submucous fibrosis.16
Many authors have investigated collagen birefringence in various tissues, including arterial walls,17 intestine submucosae,1819 uterine tubes,20 ligaments,21 and bones.142223 It appears these collagen bundles in different organs have characteristic birefringence, because they were partly sclerosed due to the effects of expansile tensile stresses. A similar condition might occur in PCs, as fibrous collagen bundles encircling the cystic cavity became sclerosed due to increasing tensile stress associated with continuous expansion. This explanation would supply why the linear band-like birefringence of PC collagen bundles were more prominent than those of PG and PA, which were basically proteolytic and degenerative lesions with less internal pressure.
In this study, we investigated the birefringence of collagen bundles in PC and compared these with those of other periapical lesions. Statistical analysis of the appearances of 325 periapical lesions observed under a polarizing microscope resulted in a pathogenetic classification of characteristic collagen birefringence, that is, a linear band-like pattern in PCs (n = 122), short, rudimentary birefringence in PGs (n = 158), and rare or no birefringence in PAs (n = 39). These findings are useful for the differential diagnosis of periapical lesions, particularly in the cases of PC with no epithelial lining caused by severe inflammation or endodontic treatment.
Conclusions
Because the collagen bundles of PC, contrary to those of PG and PA, are exposed continuously to tensile stress resulting from internal cystic pressure, they become rapidly sclerosed and produce characteristic collagen birefringence with a linear band-like pattern parallel to the cyst wall. This finding indicates the linear band-like collagen birefringence of PCs is characteristic and applicable to the differential diagnosis of PC with respect to distinguishing from PG and PA.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.

