Esthetic enhancement of a traumatized anterior tooth with a combination of forced eruption and tooth alignment: a case report
Article information

Abstract
Exposing sound structure of a subgingivally fractured tooth using orthodontic extrusion is considered to be a conservative way to re-establish biologic width without sacrificing esthetics or jeopardizing periodontal support of neighboring teeth. When a misaligned tooth is traumatically involved, a more comprehensive approach combining tooth extrusion and re-alignment may be necessary for a successful restorative outcome. This case report describes a successful esthetic management of a patient with complicated crown-root fracture on the maxillary right central incisor and pre-existing malocclusion in the maxillary anterior region. Forced eruption along with re-alignment of teeth by orthodontic movement seems to allow re-positioning of the fracture line to a favorable position and correction of crowding, providing a better esthetic result.
Introduction
Management of a complicated crown-root fracture of an anterior tooth is challenging and often requires multidisciplinary approaches for improving the functional and esthetic outcomes. A combination of endodontic, periodontal, orthodontic, and restorative procedures may be needed depending on the position of the fracture line, the type of occlusion, the condition of adjacent teeth, and the prognosis.12 Subgingival fracture calls for the re-positioning of the fracture margin supragingivally to provide a ferrule effect over sound dentin available for restorative needs. Neglecting periodontal tissue is a common mistake during restorative procedures, and is often the cause of failure. Hence, it is crucial to maintain a healthy periodontium and biologic width while restoring teeth. Among the suggested modalities for re-establishing biologic width such as orthodontic extrusion, surgical extrusion and crown lengthening, the use of orthodontic force allows the exposure of sound tooth structure without sacrificing the supporting bone or altering the position of the gingival margin.3
When misaligned teeth are traumatically fractured, a clinician can encounter a dilemma in choosing a proper treatment option for optimal esthetic results. Although a simple repair of the fracture may result in some degree of functional and esthetic recovery of the teeth, a more comprehensive approach may be required for a successful outcome and increased patient satisfaction. To improve esthetic appearance, correction of the misalignment should be also included in the treatment plan. In managing a misaligned tooth with a subgingival fracture line, therefore, a combination of forced eruption and tooth alignment using extended orthodontic appliances can be a better alternative to orthodontic extrusion used alone.
This clinical case reports a patient who had a fractured maxillary right central incisor and pre-existing malocclusion in the maxillary anterior region. The patient's esthetic expectations were successfully met through a comprehensive approach consisting of forced eruption and tooth alignment to extrude the traumatized tooth and correct the misalignment of crowded teeth simultaneously.
Case Report
A 37 year old male came to the Department of Conservative Dentistry, Kyungpook National University Dental Hospital, Daegu, Korea, requesting treatment for an injured maxillary right central incisor. The patient reported that he fell off a bicycle and injured the tooth 1 day previously. Clinical and radiographic examinations showed an oblique crown-root fracture with pulp exposure of the maxillary right central incisor. The fracture line extended approximately 6 mm below the cement-enamel junction at the mesiopalatal aspect after removing the coronal segment (Figure 1). The maxillary anterior teeth from the right canine to the left canine responded positively to a pulp vitality test including an electric pulp test and a cold test, with no tenderness to percussion. The maxillary right central incisor only had moderate mobility due to the fracture. The case was complicated because of esthetic problems in the maxillary anterior region, cross bite on the right lateral incisor, and crowding of the right central and lateral incisors. For facial analysis, irreversible hydrocolloid impressions of both arches were taken and a diagnostic cast was fabricated. The patient had skeletal class I malocclusion with bialveolar protrusion and dentoalveolar crowding of the maxillary anterior teeth (Figure 2). Based on the analysis of the model, full-mouth orthodontic treatment involving forced eruption of the fractured tooth for overall facial improvement was firstly considered. However, the patient declined the recommended option due to its high cost, long treatment period, reluctance to undergo tooth extraction and extensive orthodontic procedures. Thus, orthodontic extrusion of the fractured tooth and realignment of crowded anterior teeth were planned as an alternative option.
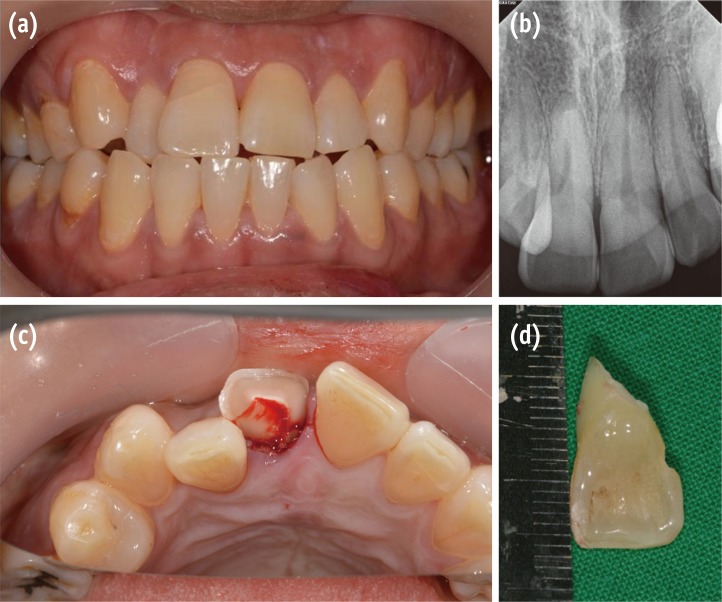
Preoperative views. (a) Intraoral photograph; (b) Periapical radiograph; (c) Clinical view showing complicated crown-root fracture on the maxillary right central incisor after removal of the coronal fragment; (d) The deepest fracture site, approximately 6 mm below the cement-enamel junction at the mesiopalatal aspect.
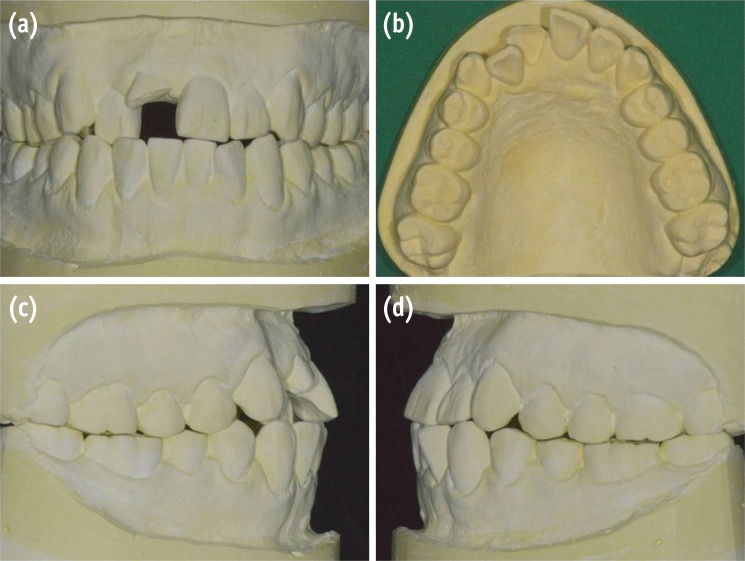
Diagnostic cast. (a) Frontal view; (b) Occlusal view; (c) Right side view; (d) Left side view. The patient showed skeletal class I malocclusion with bialveolar protrusion and dentoalveolar crowding on the maxillary anterior region.
On the first visit, emergency pulp extirpation and splinting of the tooth fragment to adjacent teeth using a bonding procedure were carried out to control pain and the esthetic problem. To re-align the palatally erupted maxillary right lateral incisor, labial movement of the tooth using removable orthodontic appliances such as a finger spring or a clear aligner may be used. However, removable orthodontic appliances apply force to the crown of a tooth through the palatally positioned spring or the elasticity of the material, resulting in a gradual tipping movement of the tooth.4 A large degree of inclination of the tooth axis during tipping can lead to unaesthetic results. Moreover, orthodontic extrusion of a tooth does not seem to be feasible with a clear aligner. Therefore, application of a fixed orthodontic appliance on the maxillary anterior area was planned to bodily move the tooth. A set-up model including a diagnostic wax-up was created to calculate the exact amount of tooth movement necessary and to predict the treatment results. As large overjet on the maxillary right central incisor was expected after re-alignment, space opening through interproximal reduction was also needed (Figures 3a and 3b). To measure the amount of space required to arrange the teeth ideally, the discrepancy of the maxillary anterior arch was calculated according to the following formula:5
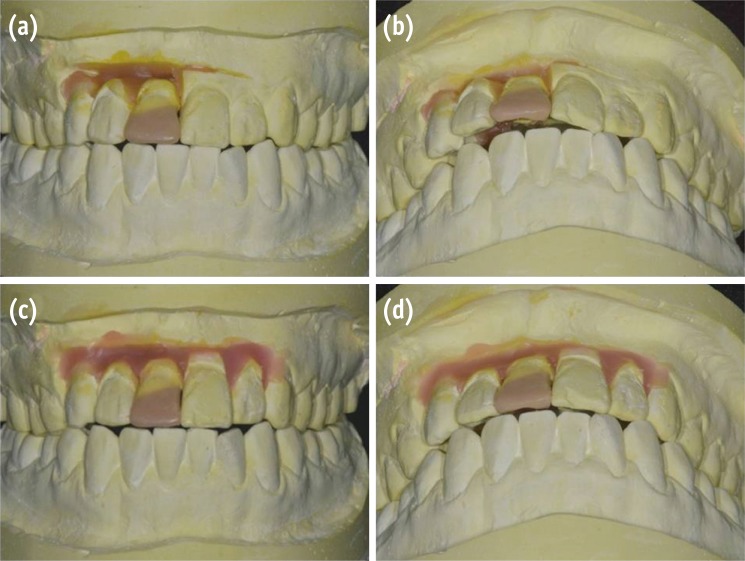
Set-up models with diagnostic wax-ups. (a) Frontal view, the maxillary right central and lateral incisors were re-aligned; (b) 45 degree occlusal view, large overjet was shown on the maxillary right central incisor due to the lack of space after re-alignment; (c) Frontal view, esthetic teeth alignment was acquired with interproximal reduction of the maxillary left central and both lateral incisors; (d) 45 degree occlusal view showing decreased overjet by re-aligning the teeth after space gaining.
Arch-length discrepancy in the maxillary anterior region = (arch length from distal plane of the maxillary right second premolar to that of left second premolar) – (sum of the width of an individual tooth), where the width of an individual tooth is the largest mesiodistal distance perpendicular to the long axis of the tooth.
The calculated discrepancy was -2.0 mm. Stripping of interproximal surfaces of the maxillary left central and both lateral incisors had to be done by removing 0.5 mm and 0.25 mm, respectively, thereby gaining 2.0 mm of space. When the teeth were re-aligned in the set-up model after interproximal reduction, decreased overjet and esthetic teeth alignment were achieved (Figures 3c and 3d). According to the pre-operative analyses, the final treatment plan was designed: orthodontic extrusion followed by all-ceramic crown restoration of the maxillary right central incisor and orthodontic alignment combined with interproximal reduction of the crowded maxillary anterior teeth.
Before orthodontic extrusion was initiated, the root canal treatment was completed. The root canal was prepared up to an apical file size of 55/0.06 taper with ProFile nickel-titanium rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland). The enlargement procedure was followed by irrigation with 2.5% sodium hypochlorite. The prepared canal was filled with gutta-percha using a continuous wave compaction technique (B&L SuperEndo α2·β, B&L Biotech Co., Ltd., Ansan, Korea) and AH Plus sealer (Dentsply DeTrey, Konstanz, Germany). The access cavity was then temporarily sealed with resin-modified glass ionomer cement (Ionoseal, Voco GmbH, Cuxhaven, Germany). Prior to orthodontic treatment, the condition of the injured tooth and adjacent teeth was periodically monitored using clinical and radiographic examinations for three months due to the potential root resorption and vitality loss of the traumatized teeth.6
Minor tooth movement from the right first premolar to the left first premolar was scheduled to obtain the anchorage necessary to move the maxillary incisors. For orthodontic extrusion, a lingual button was attached to the labial surface of the maxillary right central incisor and 0.022 inch fixed pre-adjusted edgewise appliances (Victory metal bracket Roth, 3M Unitek, Monrovia, CA, USA) were bonded to the rest of the teeth involved in orthodontic movement. A 0.014 inch nickel-titanium archwire (SE Nickel Titanium Trueform, G&H Orthodontics, Franklin, IN, USA) was then placed for leveling and alignment of the teeth (Figure 4a). Extrusion of the central incisor and labial movement of the lateral incisor were done with elastic threads (Square Thread, Dentos Inc., Daegu, Korea) exerting a force of approximately 60 g, which were replaced every 4 weeks (Figure 4b). After 4 weeks, a 0.016 inch nickel-titanium archwire (SE Nickel Titanium Trueform, G&H Orthodontics) was used, and then exchanged for a 0.016 × 0.022 inch betatitanium alloy archwire (TMA Low Friction, Ormco Co., Glendora, CA, USA) after 8 weeks. After 12 weeks of orthodontic treatment, approximately 4 mm of extrusion had been achieved, exposing a good substrate for restoration. In addition, the palatally positioned right lateral incisor was labially re-aligned (Figures 4c and 4d). To open space for the maxillary right central incisor, interproximal reduction was performed using an orthostrip (Intensiv Ortho Strips, Intensiv SA, Montagnola, Switzerland, Figure 5a) and a metal strip (Separating Strips, Dentaurum, Pforzheim, Germany, Figure 5b) on the maxillary left central and both lateral incisors. The stripped enamel surface was smoothed using Sof-Lex Tooth Polishing Strips (3M ESPE, St. Paul, MN, USA), and then treated with 5% sodium fluoride varnish (CavityShield, 3M ESPE). An open coil spring was inserted between the right lateral incisor and the left central incisor to shift the left central incisor and both lateral incisors distally over 4 weeks. While moving the adjacent teeth, the extruded tooth remained in place for stabilization at the new position.
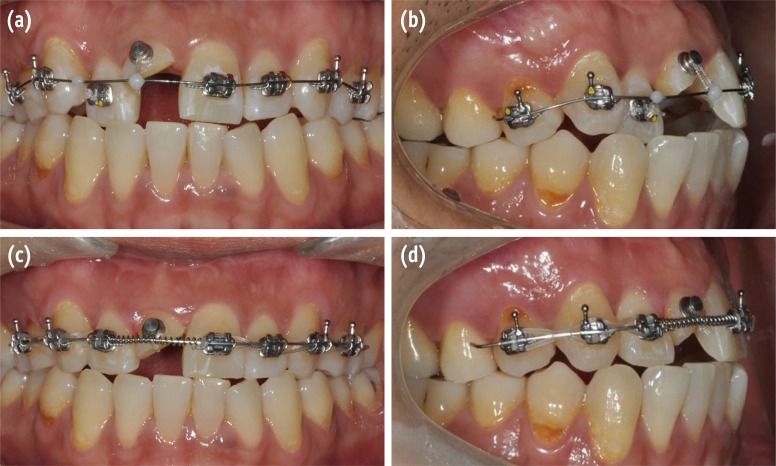
Orthodontic movement. (a, b) For extrusion, a lingual button was attached to the labial surface of the maxillary right central incisor and 0.022 inch fixed pre-adjusted edgewise appliances were bonded to the rest of the teeth involved in orthodontic movement. A 0.014 inch nickel-titanium archwire was then placed for leveling and alignment of the teeth. Extrusion of the central incisor and labial movement of the lateral incisor were done with elastic threads; (c, d) After 12 weeks, approximately 4 mm of extrusion had been achieved with a good substrate for restoration, and the palatally positioned right lateral incisor was labially re-aligned. However, to open space for the maxillary right central incisor, interproximal reduction on the maxillary left central and both lateral incisors seems to be necessary.
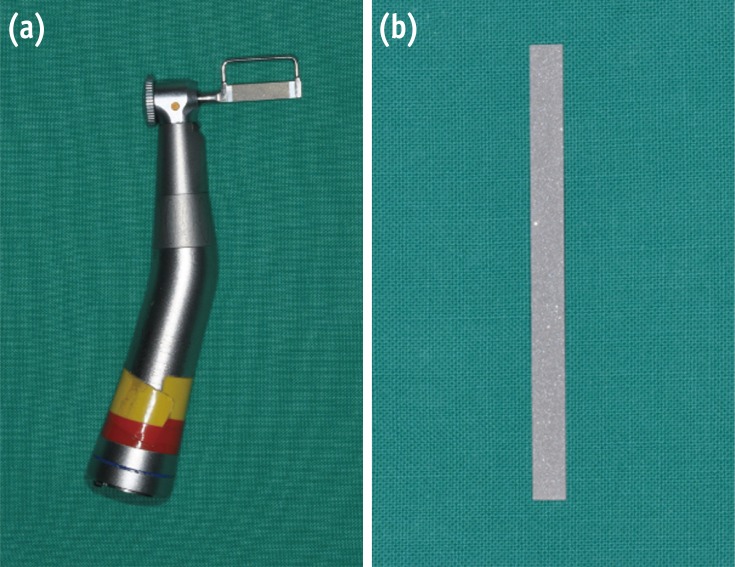
Interproximal stripping instruments. (a) An orthostrip operated in a low speed handpiece; (b) A metal strip.
After 16 weeks, an appropriate space for the maxillary right central incisor had been made and a coronal restoration was performed. A fiber post (#0.5 D.T. Light-Post, Bisco Inc., Schaumburg, IL, USA) was placed using dual-cured resin cement (Duo-Link, Bisco Inc.) and a composite core was built up (Gradia Direct, GC, Tokyo, Japan; Shade PA1, Figure 6). However, it was found that additional interproximal stripping would be necessary to clear more space for the right central incisor because of a size discrepancy between both central incisors. After the interproximal reduction and the additional 4 week tooth movement, tooth alignment was completed at 20 weeks of orthodontic treatment. To prevent any relapse, the teeth were stabilized for 4 weeks using the same fixed orthodontic appliances. After the retention period, all the brackets and wire were removed (Figure 7).
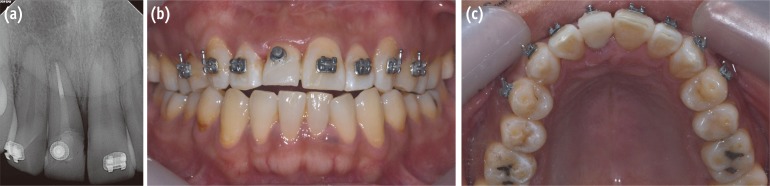
After 16 weeks of orthodontic treatment, coronal restoration with post placement and core build-up was performed on the maxillary right central incisor. (a) Periapical radiographs; (b) Photograph, frontal view; (c) Photograph, occlusal view.
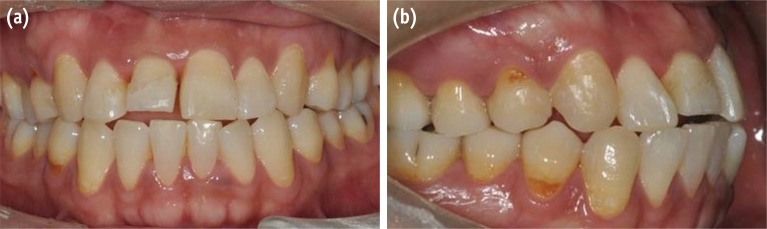
After 20 weeks of orthodontic treatment and 4 week retention period, all brackets and a wire were removed. A minor discrepancy of the gingival level between the maxillary central incisors was observed, probably due to the coronal migration of connective tissue during orthodontic extrusion. (a) Frontal view; (b) Right side view.
Before final restoration of the maxillary right central incisor, a provisional crown with an additive contour at the facial gingival level was used for 1 month after crown preparation to correct a minor discrepancy of the gingival level between the 2 maxillary central incisors. A porcelain-fused-to-zirconia crown was finally constructed over the fractured tooth with the crown margin on the sound tooth structure (Figure 8). Additional retention of the re-aligned teeth has been carried out with an invisible retainer. At the 5 month checkup following treatment, good esthetic, a stable crown position, and healthy periodontal tissues were observed. Neither vitality loss of the adjacent teeth nor pathologic signs from the injured tooth were present on follow-up clinical and radiographic examinations (Figure 9).
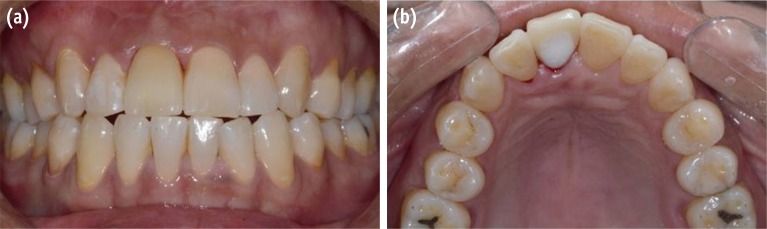
A porcelain-fused-to-zirconia crown was constructed over the fractured tooth. An optimal soft tissue profile at the facial gingival level of the maxillary right central incisor was obtained by using a provisional crown for 1 month before final restoration. (a) Frontal view; (b) Occlusal view.

At the 5 month check-up following treatment, good esthetic, a stable crown position, and healthy periodontal tissues were observed. Neither vitality loss of the adjacent teeth nor pathologic signs from the injured tooth were present on follow-up clinical and radiographic examinations.
Discussion
When restoration of a subgingivally fractured tooth is indicated, maintenance of a healthy periodontal attachment and biologic width is required for good esthetics and a positive long-term prognosis. Although orthodontic extrusion is a costly and time-consuming procedure compared to surgical crown lengthening, it may be preferable because removal of the supporting alveolar bone and apical shifting of gingival margin compromise esthetics. Moreover, in clinical cases wherein pre-existing malocclusion may jeopardize the esthetic outcome of treatment, the use of extended orthodontic appliances seems to be a proper treatment option as a comprehensive approach to solve the overall esthetic problem. In the present case, orthodontic tooth movement combining forced eruption and tooth alignment was used for extrusion of the traumatized tooth and correction of anterior teeth crowding to achieve an optimal esthetic result.
As there was inadequate space in the maxillary anterior region due to cross-bite and crowding, interproximal stripping of the maxillary central and lateral incisors was attempted to gain enough space for re-alignment of the teeth. Rossouw and Tortorella7 reported that approximately 50% of the interproximal enamel can be safely removed when enamel reduction is needed in orthodontic treatment. After calculating the discrepancy between the arch length and the total widths of the teeth, stripping of interproximal surfaces of maxillary left central and both lateral incisors was done by 0.5 mm and 0.25 mm, respectively. Considering that enamel thickness of the maxillary central and lateral incisors are approximately 1.015 mm and 1.002 mm, respectively,8 the amount of the reduction in this case seems clinically acceptable. The patient did not complain of tooth sensitivity after the interproximal reduction. However, since the roughened enamel surface after stripping might be susceptible to demineralization,9 polishing the stripped surface with subsequent topical fluoride application was performed to make the tooth surface more resistant to caries attack.1011
After 12 weeks of controlled extrusion, 4 mm of sound tooth structure was exposed with a speed of 1 mm per 3 weeks. The general rule for forced eruption is to allow approximately 1 to 1.5 weeks for each millimeter of extrusion.12 Normally, 4 mm of orthodontic extrusion requires 1 to 1.5 months. In this case, however, the eruption was completed in about 3 months. The increase in the treatment duration can be attributed to the intentionally designed atraumatic eruption, in which initial traction force was strong enough to actively extrude the tooth for the first week and became weaker over time due to the loss of elasticity of the elastic threads.13 As the elastic threads were changed every 4 weeks in this case, the relaxation period beginning the second week might offer the supporting periodontal tissue an opportunity to adjust to and re-organize in the new position. In addition, because a periodic wire change for orthodontic movement of the adjacent teeth was scheduled every 4 weeks, it was possible to perform the regular checkups and elastic changes at the same recall interval for the patient's convenience.
Upon completion of the extrusion, a minor discrepancy of the gingival level between the maxillary central incisors was observed, probably due to the coronal migration of connective tissue during orthodontic extrusion. Soft tissue conditioning can be performed restoratively by adding or subtracting the restorative provisional materials,1415 and/or surgically.16 However, in this case, surgical re-contouring such as gingivectomy was not planned to correct the discrepancy. Instead, the selective pressure technique using a provisional crown with an additive contour at the facial gingival level was applied to obtain an optimal soft tissue profile before final restoration.
For rapid orthodontic extrusion, higher forces of 50 - 60 g are required, compared to slow extrusion with 20 - 30 g of force. When stronger traction forces are exerted, coronal shift of marginal bone through bone remodeling is less pronounced because the rapid movement exceeds the capacity for physiologic adaptation.17 However, coronal migration of the gingival margin can be stimulated under extrusive force.18 Although supracrestal fiberotomy is indicated to prevent movement of the gingival tissue,1819 its result may be unpredictable since it fails to prevent coronal displacement of the gingival attachment.20 In addition, periodontal surgery usually leads to recession of the gingival margin, compromising esthetics.20 Hence, in the present case, rapid extrusion was not associated with fiberotomy. Taken together, 12 weeks of stabilization was performed with the help of the orthodontic appliance itself to alleviate relapse. For retention of the re-aligned teeth, an invisible retainer was used. It is reported that about half of total observed relapses occur within the first 2 years after treatment.21 Therefore, at least 2 year retention seems to be necessary for good stability. Although a relatively long treatment time, long retention period, and use of fixed orthodontic appliances required motivation from the patient, a better esthetic result was obtained using a careful treatment plan for the subgingivally fractured, misaligned tooth.
Conclusions
The multidisciplinary approach combining endodontic, orthodontic, and restorative procedures described in this case report successfully recovered the function and esthetics of the misaligned tooth with complicated crown-root fracture. Forced eruption and simultaneous tooth alignment by orthodontic movement provided the exposure of sound tooth structure for restoration and the correction of crowding for esthetic improvement.
Acknowledgement
This case study was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2013R1A1A2012382).
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.