Endodontic treatment of maxillary lateral incisors with anatomical variations
Article information
Abstract
Maxillary lateral incisors usually exhibit a single root with a single canal. However, maxillary lateral incisor teeth with unusual morphology of root canal system are frequently reported. These cases of variable root canal anatomy can be treated well by nonsurgical endodontic methods. A detailed description of root canal morphology is fundamental for successful endodontic treatment. Treatment using an operating microscope, radiographs from different angles, and cone-beam computerized tomography (CBCT) can produce more predictable endodontic outcomes.
Introduction
Endodontic treatment involves thorough mechanical and chemical cleansing of the entire pulp cavity and three-dimensional obturation with inert filling materials. In some cases, however, a root canal may be left untreated because of the failure to recognize its presence.1,2 Endodontic literature generally describes maxillary lateral incisors as a tooth with a single root and a single canal. This generalization is not completely true as reports describe maxillary lateral incisors with two roots or three canals.2,3 Many of these manifest clinically as germination, fusion, concrescence, or dens invaginatus, since maxillary lateral incisors are often located at the site of high embryological risk.4,5 Maxillary lateral incisors can have various configurations of root canals, especially in the Turkish population.6,7 Following are three treatment cases of maxillary lateral incisors with anatomical variations of root canal system.
Case reports
Case 1
A 26-year-old male in good health was referred to the endodontic clinic of Kyungpook National University Dental Hospital for root canal treatment of the maxillary right lateral incisor. The root canal treatment had been initiated by a general dentist, who opted for a referral after observing its unusual root canal morphology. Clinical examination revealed a sinus tract labially to the lateral incisor and swelling at this level. There was tenderness to palpation and percussion. Radiographically, a diffuse radiolucent area was noticed at the apices of roots of the maxillary right lateral incisor (Figure 1a). The sinus tract was traced with a gutta-percha cone to tooth #12 that showed a second root surrounded by a radiolucent area. The pulpal diagnosis was previous endodontic treatment and the periapical diagnosis was chronic apical abscess with sinus. There appeared to be two roots that had distinct root canal space.
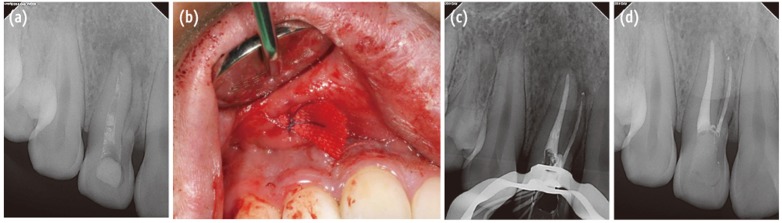
Right maxillary lateral incisor with two roots and two canals. (a) Preoperative periapical radiograph; (b) Intraoral photograph during incision and drainage; (c) Post-obturation periapical radiograph; (d) Periapical radiograph at the 6-month follow-up.
A rubber dam was applied, and temporary sealing material was removed. The principle canal was found easily but the second canal was not negotiated. At the following visit, because the second canal was not negotiated again while the patient had labial swelling with fever and pain, incision and drainage was performed at the labial swollen area (Figure 1b). At the third visit, the second canal was negotiated with ultrasonic instruments under an operating microscope. The second canal was located at the corresponding part of palatogingival groove in the pulpal chamber of the tooth. After removing dentin carefully with an ultrasonic device, an orifice was detected by using a size 10 stainless steel K-file (Mani, Tochigi, Japan). Both canals were cleaned and shaped with stainless steel K-files using the step-back technique. Radiograph revealed a narrow second canal, which was prepared with 2 mm increments per each size of file (.025 taper).
After preparation, the root canals were irrigated with 17% ethylenediaminetetraacetic acid (EDTA) followed by 5% sodium hypochlorite solution and dried with sterile paper points. The root canals were obturated with gutta-percha using cold lateral compaction technique with an epoxy resin sealer (AH Plus, Dentsply De Trey GmbH, Konstanz, Germany) (Figure 1c). After verifying that the root canal filling was complete with a radiograph, the crown was restored with a composite resin (Gradia PA2, GC, Alsip, IL, USA). At six month examination, the tooth was asymptomatic and there was no radiolucency around the root apex (Figure 1d).
Case 2
A 12-year-old male was referred from the Department of Pediatric Dentistry for root canal treatment of the maxillary left lateral incisor. Upon clinical examination, the upper left lateral incisor showed mild tenderness to percussion and palpation. The tooth did not respond to electric and thermal pulp sensibility test while the adjacent teeth responded within normal limits. The periapical radiograph suggested two root canals in a bulbous root and a diffuse apical lesion (Figure 2a). From the clinical and radiographic findings, the maxillary lateral incisor was diagnosed as pulp necrosis and chronic apical abscess without sinus, for which root canal treatment was planned.
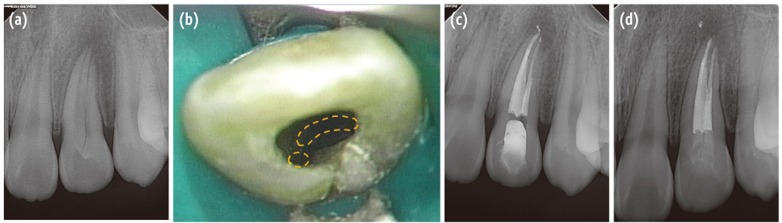
Left maxillary lateral incisor with one root and two canals. (a) Preoperative periapical radiograph; (b) Intraoral photograph of access cavity and canal orifices; (c) Post-obturation periapical radiograph; (d) Periapical radiograph at the 6-month follow-up.
An access opening was made after rubber dam isolation. The main canal was wider and C-shaped. Another narrower canal was seen running towards palate under an operating microscope (Figure 2b). Along the dentinal map, the second canal was detected easily by extending the access cavity palatally. Working lengths were determined with an apex locator (Root ZX, Morita, Tokyo, Japan) and confirmed radiographically. Under copious irrigation with 5% sodium hypochlorite and 17% EDTA, the root canals were cleaned and shaped up to a size 35 with stainless steel K-files using the step-back technique and the circumferential filing technique. Obturation of the root canal was performed by cold lateral compaction of gutta-percha using an epoxy resin sealer (AH Plus) (Figure 2c). The access cavity was restored with composite resin (Filtek Z350 XT, 3M ESPE, St. Paul, MN, USA) and a postoperative radiograph was taken. The tooth was asymptomatic and the periapical lesion resolved over the subsequent six months (Figure 2d).
Case 3
A 17-year-old male patient was referred for endodontic treatment of his upper left lateral incisor. Two years earlier, he had received root canal treatment for a severe pain in the same region. He reported swelling, pain and discharge of pus at the mucosal area in the lateral incisor for one week. His medical history was noncontributory. An intraoral examination revealed a sinus tract on the labial gingiva associated with the lateral incisor. The tooth was sensitive to percussion and palpation. A periapical radiograph demonstrated a diffuse radiolucency at the apex of the lateral incisor (Figure 3a). The pulp diagnosis was previous endodontic treatment, and the periapical diagnosis was periapical abscess with sinus.
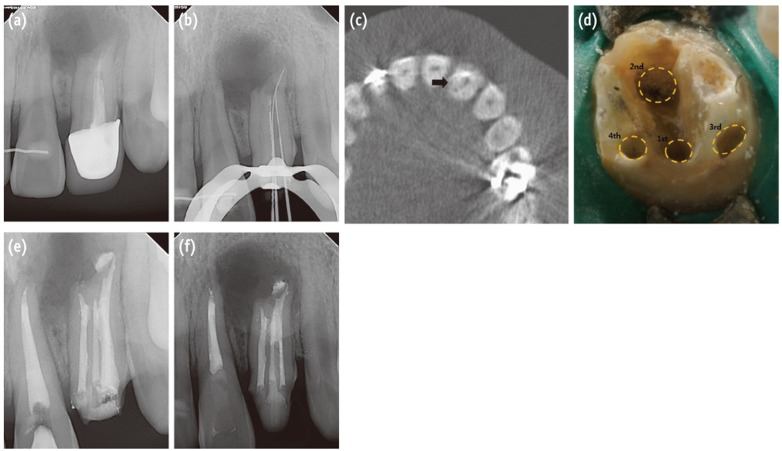
Left maxillary lateral incisor with one root and four canals. (a) Preoperative periapical radiograph; (b) Working length files of the first, second and third canals of the left maxillary lateral incisor; (c) Axial CBCT section of the tooth. Black arrow indicates the fourth canal; (d) Intraoral photograph of access cavity and canal orifices; (e) Postobturation periapical radiograph; (f) Periapical radiograph at the 4-month follow-up.
An access opening was made after removal of the prosthesis and rubber dam isolation. Old gutta-percha was removed from the first and second canals with a size 25 stainless steel H-file (Mani). The canals were irrigated with 5% sodium hypochlorite. At the following visit, the third canal running into the second canal was negotiated under the operating microscope (Figure 3b). To ascertain the location of the fourth canal, a cone-beam computerized tomography (CBCT, Mercuray, Hitachi, Tokyo, Japan) was taken. The fourth canal was negotiated by cutting the overlying dentin of the expected site with a pointed tip of an ultrasonic device under the microscope, considering the locations of the first and the second canals in CBCT axial section images (Figure 3c). The orifice of the fourth canal was located on the mesiopalatal side at the external wall of the prepared tooth (Figure 3d). All canals were cleaned and shaped using K-files with the step-back technique and copious irrigation with 5% sodium hypochlorite solution. The root canals were obturated by cold lateral compaction of gutta-percha using an epoxy resin sealer (AH Plus, Figure 3e). The access cavity was restored with composite resin (Filtek Z350 XT) and a post-obturation radiograph was taken. The patient returned for review four months later at which time he remained symptomless. On inspection, neither swelling nor sinus tract was seen. The tooth was not tender to percussion or palpation (Figure 3f).
Discussion
Maxillary lateral incisor teeth are generally single-rooted teeth with a single canal. Independent studies consistently report that maxillary lateral incisors have single root canals.1,8 However, there are reports of maxillary lateral incisors with two or three canals.2,3,9,10 These are thought to be the result of abnormal development of the tooth and root.
The possibility of multiple canals in the maxillary lateral incisor results from its location of high embryological risk4. During the fourth and sixth weeks of human embryonic development, the upper jaw, from which the lateral incisors originate, forms by fusion of the paired medial nasal processes (MNP) and maxillary processes (MP). As the MNP fuse with each other, they form the premaxilla, including the medial portion of the upper lip (philtrum) and the primary palate.11 Exact origin of the maxillary lateral incisor relative to the MNP/MP fusion area and the location of the premaxillary/maxillary suture in the human is an open question. The MNP/MP fusion area may be medial to the lateral incisor or at the medial or middle one-third of the lateral incisor. The premaxillary/maxillary suture may be between the lateral incisor and canine or at the middle third of the canine.12-14 For these reasons, maxillary lateral incisors may show various root canal morphology.15,16
Conventional intraoral periapical radiographs have been used to examine root canal morphology in vivo. However, these radiographs produce only two-dimensional images of three-dimensional objects, resulting in distortion and superimposition of structures. In comparison, more recently developed CBCT scans have significantly improved the understanding of three-dimensional root canal morphology.5,17 CBCT scans can be useful diagnostic tools in endodontic practice since it could help to speculate the location of the canal by referring anatomical structures.18
Given that morphological variations exist in these teeth, when a patient presents with persistent pain or sensitivity to hot and cold after root canal treatment, the clinician must suspect the presence of missed canals. Judicious use of high-end diagnostic aids such as radiographs with varying angles, CBCT, and an operating microscope should also be considered in such complicated situations. For successful endodontic therapy, the dentist should be aware of the possibility of variations in the root canal morphology.
Conclusions
The clinical significance of the present cases is that maxillary lateral incisors may have two or more canals. Use of operating microscope and CBCT are helpful in identifying the anatomic complexity of the pulpal spaces.
Notes
No potential conflict of interest relevant to this article was reported.