Effects of cavity configuration on bond strength and microleakage of composite restoration
Article information
I. INTRODUCTION
One of the inevitable characteristics of dental composites is the shrinkage during radical polymerization as monomer molecules are converted into a polymer network, reducing intermolecular spaces. This shrinkage produces contraction stress in a confined structure such as a tooth cavity. The performance of a composite restoration depends upon a complete bond with the surrounding tooth structure. During placement, the polymerization contraction of the composite produces stress which can lead to failure of this bond. The majority of the contraction stress of composite occurs during the initial polymerization period after gelation, and the stress development rate decreases gradually with time1,2,3). The internal stress generated in the restricted environment of a tooth cavity can exceed the adhesive bond strength and produce a delamination of the restoration interface4). In cases where higher bond strength is present, this stress may cause to fracture the marginal tooth substrate and/or the composite restorative itself5,6). Either case results in the formation of a marginal gap, allowing the possible ingress of oral fluids and bacteria through leakage though it is not easy to clinically detect leakage around the cavity wall immediately after placement. Furthermore, marginal leakage is associated with postoperative sensitivity, and may eventually produce discoloration of the margins and/or recurrent caries, and consequently may reduce the life of a restoration.
A number of factors contribute to the magnitude of the stress produced by a given composite compositionally and technically. The amount and type of resin phase presented determines the magnitude of the polymerization contraction which occurs7,8,9,10). The level of inorganic filler presented directly effects the elastic modulus, translating a given amount of contraction into varying levels of stress11). The other approach is performed technically and includes a modified application technique12,13,14), the use of a indirect restoration15), controlling the reaction rate by altering light energy16,17,18), and using flexible and lowviscosity intermediate adhesives2,19,20). Choi and others21) reported the effects of adhesive thickness on polymerization contraction stress. Contraction stress decreased significantly as the adhesive thickness was increased. This stress that contributes to early marginal leakage was absorbed and relieved by increasing thickness of low-stiffness adhesive. Despite these measures, the successful use of dental composite is still hindered by its inability to reliably form wellbonded margins. Therefore, it is difficult to guarantee a leakproof restoration.
As the resin bonds to the walls and floor of the cavity preparation, competition will develop between the opposing walls as the restorative resin shrinks during polymerization6). The magnitude of this phenomenon depends upon the configuration of the cavity and hence is called the cavity configuration22,23,24). Cavity configuration factor(C-factor) is the ratio of the bonded surface area to the unbonded or free surface area. This ratio becomes the largest in Class I and deep Class V, that is, box-like cavities.
A micro-tensile bond test introduced recently can evaluate the bond strength between inner cavity wall and composite contrary to conventional bonding methods such as a shear bond test or a tensile bond test25). This testing method using small surface areas for bonding has facilitated the determination of bond strengths to caries-affected dentin26), and dentin of cervical erosion/abrasion lesions27).
In experimental design, maximum contraction forces were inversely related to C-factor and directly related to composite volume in a non-rigid system which allowed compliance28). Also, Yoshikawa and others29) reported that the bond strength of several dentin adhesives fell as increasing C-factor by a three dimensional cavity preparation, but the difference was significant only with one adhesive system. However, there has not been reported the relationship between cavity configuration and bond strength of composite restoration directly. Therefore, the purpose of this study was to evaluate the effects of various cavity configurations on bond strength of composites and microleakage of composite restoration according to different types.
II. MATERIALS AND METHODS
1. Specimen preparation
The materials, components, manufacturers, and batch numbers used in this study listed in Table 1. Ninety-eight bovine incisors (40 for micro-tensile test and 58 for microleakage test) within one month of extraction were selected and the pulps were cleaned from the root canals.

The materials used in this study
2. Micro-tensile test
For control group (C=1), bovine teeth were ground with wet 600 grit SiC paper serially and exposed dentin surface. In experimental groups with high C-factor, cavities were prepared with a carbide steel bur(#245; Shofu Co., Japan) in bovine teeth. The depth of cavities was 2.0mm to make even curing degree and the ratio of bonded to unbonded surface area, or the C-factor(C=1+4h/d, in which d and h are the diameter and height of the cylindrical cavities, respectively), was controlled by the diameter of cavity (Table 2). The dimensions of the preparation were verified with an electronic caliper (Mitutoyo Corp., Japan).

Experimental groups
A self-etching primer system (Clearfil SE Bond; Kuraray Co., Japan) was applied on surface and in cavities of all specimens according to the manufacturer's instruction. The composite resins that are a hybrid (Clearfil AP- X; Kuraray Co., Japan) and a microhybrid type (Esthet-X; Dentsply, USA) were placed as a series of thin layers on the flat control surface to minimize contraction, and the cavities were bulk-filled to maximize contraction(Fig. 1; Bc and Be). Composite was light-cured (Spectrum 800; Dentsply, USA) for 40sec in all of cases. Additional composite was built-up for mounting on the microtensile testing zig (Fig. 1; C).

Specimen preparation for tensile bonding test: A) cavity preparation for each C-factor, Bc) composite bonding on dentin surface for control group, Be) composite filling for experimental groups, C) additional composite build- up, D-E) vertical slices (1.0mm thick) cut perpendicular to the long axis of the tooth, and F) trimmed specimens into hour-glass shape with the narrowest portion.
All restored specimens were stored in water at 37℃ for 24hrs and then sliced serially to be 1.0mm thick perpendicular to the bonded surfaces with a low-speed diamond saw (Isomet; Buehler, USA) under copious water supply. Slices were trimmed into an hour-glass shape with the narrowest portion of approximately 1mm2 area located at the adhesivedentin interface using with a diamond point (#104, Shofu, Japan) in high -speed handpiece (Fig. 1-F). The trimmed specimens were mounted on a testing zig with cyanoacrylate adhesive (Zapit, MDS Products Co., Corona, USA)(Fig. 2), then stressed to failure in tension at 1mm/min in a universal testing machine (EZ test; Shimadzu, Japan).

Micro-tensile bond test.
The maximum tensile force was divided by the area of the specimen and the measured micro-tensile bond strength values were analysed using ANOVA/Tukey's test at a significance level of 0.05.
3. Microleakage Test
Each cavity was prepared and restored with composites as same manner in micro-tensile test, but control group was ruled out. All filled restorations were finished immediately using abrasive disks (Soflex, 3M, USA). After finishing, the teeth filled with composites were placed in 37℃ water for 1 day. The teeth were then coated with nail varnish 2.0mm short of the restoration margins after the apices were blocked with utility wax. These measures were taken to prevent staining from occurring through any route besides that provided by the presence of marginal defects.
As described in a previous study21), the teeth were stained by immersion in room temperature 3mol/L silver nitrate in amber vials for 24 hours in a dark room. They were then removed, rinsed with tap water, and placed in film developer (Eastman Kodak) under fluorescent light for 24 hours. The roots were cut off and embedded in epoxide resin (Buehler, USA) and allowed to set overnight before they were sectioned inciso-gingivally in the approximate center of the restoration with a low-speed saw. After the sectioned surface was ground with 400 and 600 grit SiC paper and polished with 3µm diamond compound (Buehler), both surfaces were examined under a stereomicroscope (Olympus, Japan) at x40 magnification by two examiners. Each examiner independently graded the dye penetration at the incisal and gingival margin using the following ordinal scale:
0 = no marginal leakage.
1 = silver nitrate penetration that extended less than or up to half the distance to the DEJ (dentino-enamel junction).
2 = penetration greater than half and up to, but not past, the DEJ.
3 = penetration past the DEJ, but not including the pulpal wall.
4 = penetration involving the pulpal wall.
Two examiners reevaluated all specimens if there were any discrepancies. The statistical analysis of the results of the staining measurement was done with the Kruskal-Wallis non-parametric independent analysis and the Mann-Whitney U test to evaluate differences between experimental groups at a significance level of 0.05.
III. RESULTS
1. Micro-tensile test
Micro-tensile bond strengths are summarized in Table 3, and those of each type composite are showed in Fig. 3 and 4. Mean micro-tensile bond strength was decreased with increasing C-factor in both types of composites. For hybrid composite, the tensile bond strength to flat dentin showed the greatest value of approximately 37MPa and was different significantly from experimental groups with higher C-factor statistically. And there was no significant difference among these groups. For microhybrid composite, tensile bond strengths were decreased with increasing C-factor though no difference statistically. Tensile bond strength between hybrid and microhybrid type composites with various C-factors is also compared in Fig. 5.

Micro-tensile bond strength (MPa SD)
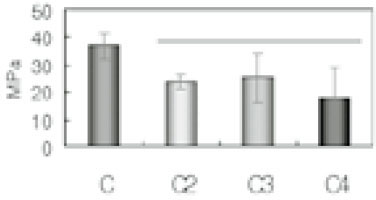
Micro-tensile bond strength of hybrid type composite according to C-factors.
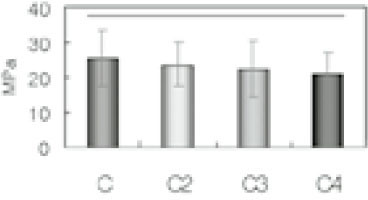
Micro-tensile bond strength of microhybrid type composite according to C-factors.
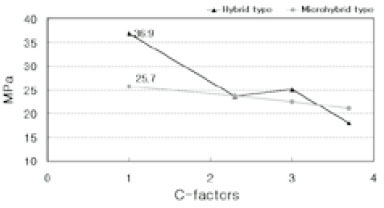
Comparison of micro-tensile bond strength between hybrid and microhybrid type composites.
2. Microleakage test
Microleakage scores of all experimental groups are shown in Table 4. No specimens ranked zero in the microleakage experiment. Microleakage scores of hybrid composite restoration were generally higher than those of microhybrid at both incisal and gingival margin (p>0.05). In all experimental groups, microleakage scores were increased with higher C-factors, and those of gingival margin were higher than incisal margin though there were no difference significantly(p>0.05). Figure 6 showed the microleakage at each score mentioned previously.

Microleakage scores of experimental groups
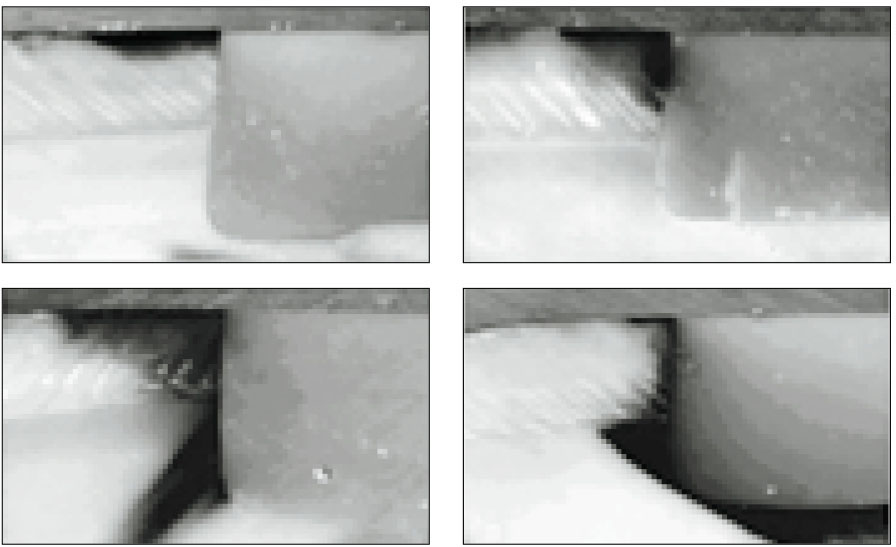
Degree of microleakage. (a); degree 1, (b); degree 2, (c); degree 3, (d); degree 4.
IV. DISCUSSION
Though the use of composite restoration is increasing continuously and most dentists select composites as their main esthetic alternatives to amalgam for posterior teeth, approximately 70% continue to use amalgam as their primary posterior restorative30). Composites are more difficult to place and their longevity is inferior to that of amalgams in general practice31). Secondary or recurrent caries that is regarded as a main cause of failure is primarily related to technical difficulties in placing restorations with sealed margins due to the excessive polymerization contraction of composites. Many factors influence marginal leakage in composite restorations, including polymerization contraction and differences in thermal expansion characteristics32). Either can produce stress within the composite when it is restrained from shrinking freely. Anything that increase the capacity of the resin to flow and relieve stress, such as large unbonded surfaces, slow curing rates, or porosity, results in less contraction stress1,6,23,33).
In previous pilot study, we have used the sandblasted and silanated pyrex tube to make simulated cavity on dentin surface instead of tooth cavity in this study. However, there was no significant difference with increasing the C-factors. It was difficult to get the attachment between tube and dentin surface and the pyrex tube was too flexible to keep constant configuration. This is why the previous study was failed. In virtue of microtensile testing method, we can evaluate the bond strength on irregular tooth surface as well as on inner surface of cavity wall, which could not be conducted with the conventional testing method that was mainly shear bond test. Moreover, microtensile test has some other advantages that can evaluate more adhesive failures, means and variances can be calculated for single tooth, permits measurements of regional bond strengths on very small areas, and facilitates SEM examination of the failed bonds. On the other hand, there are some disadvantages that is labor-intensive, technically demanding, difficult to measure bond strength under 5MPa and require special equipment34).
Mean tensile bond strength of hybrid composite was decreased so much in lower C-factor, but that of microhybrid was slightly decreased with C-factors. This result suggests that the bond strength of a stiffer composite is more affected and impaired by the cavity configuration. Most of hybrid composites have the higher elastic modulus, that is, high stiffness as a result of a higher filler load than a microhybrid35). For hybrid composite, the tensile bond strength of a control group to flat dentin surface was the highest value because there was no or less impairment by contraction stress for polymerization.
Another reason that we can suppose, which the composite with higher physical properties is generally showed the higher bond strength to tooth substrate. Miyazaki et al36) reported that filler content was one of the important factors influencing the physical properties of composites in the study of bond strength to bovine dentin. Another researches informed us that mechanical properties of dental composites were most highly correlated with bond strengths to the tooth dentin/ or enamel37,38).
Stresses large enough to exceed the adhesive forces between the tooth and the composite are relieved as gaps formed at the margins6,32). Because the bonding of resin to dentin is more variable than to enamel in vivo, cavities with margins in dentin are most at risk39). Optimization of these margins depends on reducing contraction or relieving contraction stresses. In this study, microleakage scores of hybrid composite restoration were generally higher than those of microhybrid at both incisal and gingival margin though there were no significant differences. In all experimental groups, microleakage scores were increased with higher C-factors, and those of gingival margin were higher than incisal margin though there was no significant difference. Similar microleakage test according to various C-factors was performed by Choi et al21) previously. Although the clinical results are unpredictable under the environment that C-factor is less than 1, microleakage at the increased C-factors showed a relative high scores in this study.
Beside of this study, we have performed another research40) having a hypothesis that contraction stress may affect the properties of composite restoration itself. The properties of hybrid composite were more deteriorated with increasing C-factor than that of microhybrid type. There was performed another study that C-factor had no influence on the cavity adaptation for compomer restorations41). This might be due to reduced stress generation at the bonding interface caused by relatively low mechanical properties immediately after curing, less elasticity, and water absorption in compomers.
Hybrid composite with higher filler contents and elastic modulus showed more sensitive results than microhybrid according to increasing C-factor. These results suggest that the adequate selection of materials as well as the control of polymerization contraction stress is so important factors for successful composite restoration. We have a plan to study continuously on human teeth with same protocol instead of bovine teeth in the future and need to evaluate the correlation between these vitro studies and clinical situations through the examination of practical restorations in oral cavity of the followed patient up for long time.
V. CONCLUSION AND SIGNIFICANCE
Polymerization contraction depends upon the type of dental composites and the cavity configuration that plays an important role on the development of its stresses. The purpose of this study was to evaluate the effects of various cavity configurations on bond strength of composites and microleakage of composite restoration according to different resin types.
Micro-tensile bond strength of hybrid composite to flat dentin surface was significantly higher than that of microhybrid type(p<0.05), but there was no significant difference between experimental groups of two type composites.
Micro-tensile bond strength was decreased with increasing C-factor in both types of composite. For hybrid composite, the tensile bond strength to flat dentin showed significantly different from experimental groups with higher C-factor. And there was no significant difference in microhybrid composite.
Microleakage scores of hybrid composite restoration were generally higher than those of microhybrid at both incisal and gingival margin(p>0.05).
In all experimental groups, microleakage scores were increased with higher C-factors, and those of gingival margin were higher than incisal margin though there was no significant difference(p>0.05).
Hybrid composite with higher filler contents and elastic modulus showed more sensitive results than microhybrid with increasing C-factor. These results suggest that the adequate selection of materials as well as the control of polymerization contraction stress are so important factors for successful composite restoration.